
A Serious Game for the Prevention of Obesity in School Children–Impact of Parent’s Involvement: A Randomized Controlled Trial

 ,
,  ,
,
Abstract
:1. Introduction
Objective and Hypothesis
2. Materials and Methods
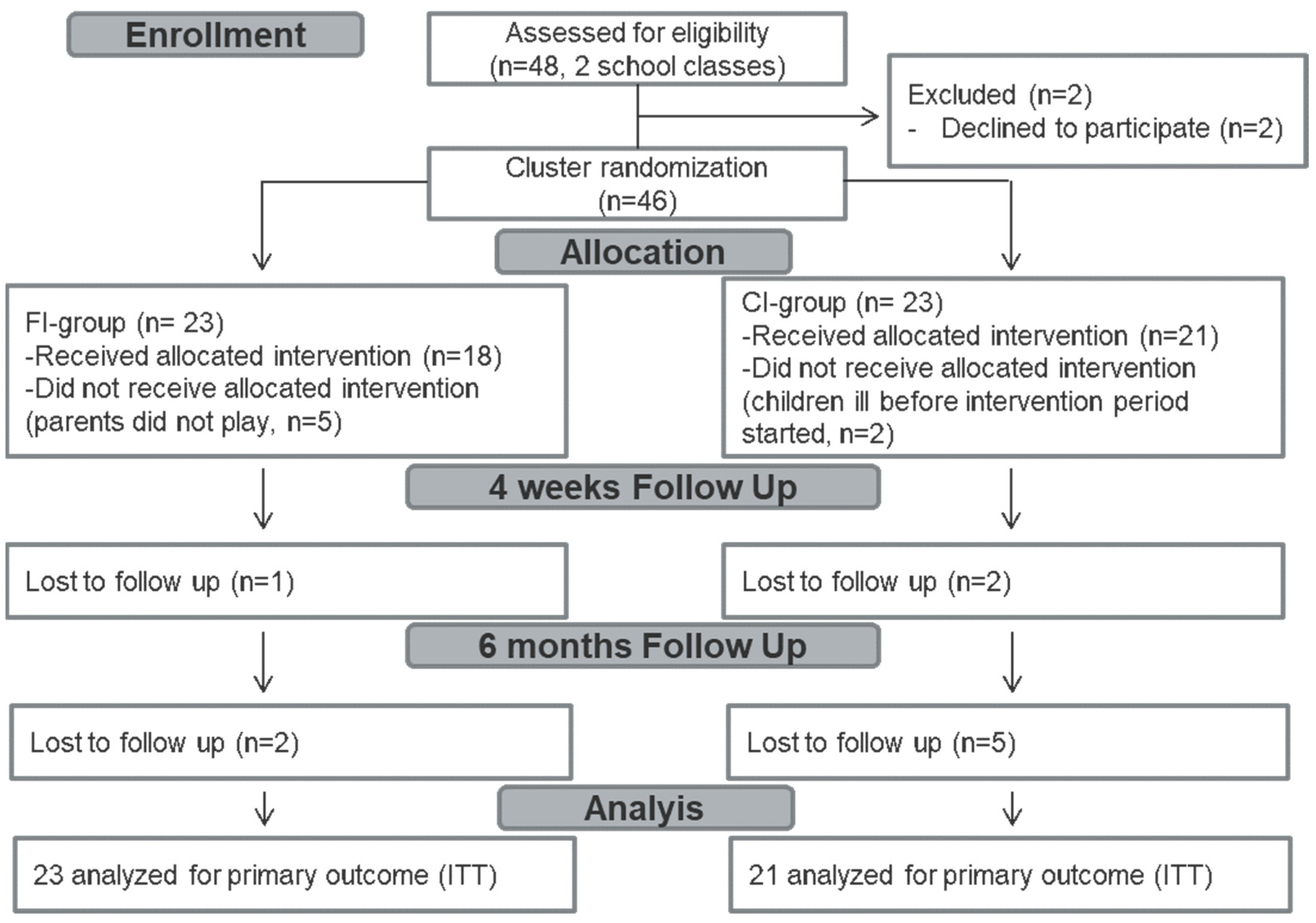
2.1. Study Design and Participants
2.2. Treatments
2.3. Outcome Measures
2.4. Sample Size
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Outcomes
3.2.1. Primary Outcome
3.2.2. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lobstein, T.; Jackson-Leach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.; Wang, Y.; McPherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef] [Green Version]
- Gallus, S.; Lugo, A.; Murisic, B.; Bosetti, C.; Boffetta, P.; La Vecchia, C. Overweight and obesity in 16 European countries. Eur. J. Nutr. 2015, 54, 679–689. [Google Scholar] [CrossRef]
- Wijnhoven, T.M.; van Raaij, J.M.; Spinelli, A.; Starc, G.; Hassapidou, M.; Spiroski, I.; Rutter, H.; Martos, E.; Rito, A.I.; Hovengen, R.; et al. WHO European Childhood Obesity Surveillance Initiative: Body mass index and level of overweight among 6–9-year-old children from school year 2007/2008 to school year 2009/2010. BMC Public Health 2014, 14, 806. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Methven, E.; McDowell, Z.C.; Hacking, B.; Alexander, D.; Stewart, L.; Kelnar, C.J. Health consequences of obesity. Arch. Dis. Child. 2003, 88, 748–752. [Google Scholar] [CrossRef]
- Weiland, A.; Nannette, K.L.; Zipfel, S.; Ehehalt, S.; Ziser, K.; Junne, F.; Mack, I. Predictors of Weight Loss and Weight Loss Maintenance in Children and Adolescents with Obesity after Behavioral Weight Loss Intervention. Front. Public Health 2022, 10, 813822. [Google Scholar] [CrossRef]
- Barlow, S.E.; Dietz, W.H. Obesity evaluation and treatment: Expert Committee recommendations. The Maternal and Child Health Bureau, Health Resources and Services Administration and the Department of Health and Human Services. Pediatrics 1998, 102, E29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prowse, R.; Carsley, S. Digital Interventions to Promote Healthy Eating in Children: Umbrella Review. JMIR Pediatr. Parent 2021, 4, e30160. [Google Scholar] [CrossRef] [PubMed]
- Cifuentes, L.; Camilleri, M.; Acosta, A. Gastric Sensory and Motor Functions and Energy Intake in Health and Obesity-Therapeutic Implications. Nutrients 2021, 13, 1158. [Google Scholar] [CrossRef] [PubMed]
- Stelmach-Mardas, M.; Rodacki, T.; Dobrowolska-Iwanek, J.; Brzozowska, A.; Walkowiak, J.; Wojtanowska-Krosniak, A.; Zagrodzki, P.; Bechthold, A.; Mardas, M.; Boeing, H. Link between Food Energy Density and Body Weight Changes in Obese Adults. Nutrients 2016, 8, 229. [Google Scholar] [CrossRef] [PubMed]
- Mack, I.; Reiband, N.; Etges, C.; Eichhorn, S.; Schaeffeler, N.; Zurstiege, G.; Gawrilow, C.; Weimer, K.; Peeraully, R.; Teufel, M.; et al. The Kids Obesity Prevention Program: Cluster Randomized Controlled Trial to Evaluate a Serious Game for the Prevention and Treatment of Childhood Obesity. J. Med. Internet Res. 2020, 22, e15725. [Google Scholar] [CrossRef] [Green Version]
- Mack, I.; Bayer, C.; Schaffeler, N.; Reiband, N.; Brolz, E.; Zurstiege, G.; Fernandez-Aranda, F.; Gawrilow, C.; Zipfel, S. Chances and Limitations of Video Games in the Fight against Childhood Obesity-A Systematic Review. Eur. Eat Disord. Rev. 2017, 25, 237–267. [Google Scholar] [CrossRef] [PubMed]
- Suleiman-Martos, N.; García-Lara, R.A.; Martos-Cabrera, M.B.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De la Fuente, G.A.; Gómez-Urquiza, J.L. Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2478. [Google Scholar] [CrossRef]
- Warsinsky, S.; Schmidt-Kraepelin, M.; Rank, S.; Thiebes, S.; Sunyaev, A. Conceptual Ambiguity Surrounding Gamification and Serious Games in Health Care: Literature Review and Development of Game-Based Intervention Reporting Guidelines (GAMING). J. Med. Internet Res. 2021, 23, e30390. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T.; Abdelsamad, D.; Baranowski, J.; O’Connor, T.M.; Thompson, D.; Barnett, A.; Cerin, E.; Chen, T.A. Impact of an active video game on healthy children’s physical activity. Pediatrics 2012, 129, e636–e642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Truthmann, J.; Mensink, G.B.; Richter, A. Relative validation of the KiGGS Food Frequency Questionnaire among adolescents in Germany. Nutr. J. 2011, 10, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleiser, C.M.G.; Karth, B.M.; Neuhauser, H.; Schenk, L. Semantic Scholar. Ernährungsverhalten von Kindern und Jugendlichen mit Migrationshintergrund? KiGGS-Migrantenauswertung—Endbericht (Nutrition Behaviour of Children and Adolescents with a Migration Background—Data from the KIGGS-Study). 2007. Available online: https://edoc.rki.de/handle/176904/553 (accessed on 2 February 2022).
- Bayer, O.; Jarczok, M.; Fischer, J.; von Kries, R.; De Bock, F. Validation and extension of a simple questionnaire to assess physical activity in pre-school children. Public Health Nutr. 2012, 15, 1611–1619. [Google Scholar] [CrossRef] [Green Version]
- Manz, K.; Schlack, R.; Poethko-Müller, C.; Mensink, G.; Finger, J.; Lampert, T.; KiGGS Study Group. Physical activity and electronic media use in children and adolescents: Results of the KiGGS study: First follow-up (KiGGS wave 1). Bundesgesundheitsblatt Gesundh. Gesundh. 2014, 57, 840–848. [Google Scholar] [CrossRef] [Green Version]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Mon. Kinderheilkd. 2001, 149, 807–818. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Freeman, G.H.; Halton, J.H. Note on an exact treatment of contingency, goodness of fit and other problems of significance. Biometrika 1951, 38, 141–149. [Google Scholar] [CrossRef]
- Vink, G.; Frank, L.; Pannekoek, J.; van Buuren, S. Predictive mean matching imputation of semicontinuous variables. Stat. Neerl. 2014, 68, 61–90. [Google Scholar] [CrossRef]
- Rubin, D. Statistical matching using file concatenation with adjusted weights and multiple imputations. J. Bus. Econ. Stat. 1986, 4, 87–94. [Google Scholar] [CrossRef]
- Kleinke, K. Multiple imputation by predictive mean matching when sample size is small. Methodology 2018, 14, 3–15. [Google Scholar] [CrossRef]
- Willson, V.L.; Putnam, R. A Meta-analysis of Pretest Sensitization Effects in Experimental Design. Am. Educ. Res. J. 1982, 19, 249–258. [Google Scholar] [CrossRef]
- Kostecka, M. The Effect of the “Colorful Eating Is Healthy Eating” Long-Term Nutrition Education Program for 3- to 6-Year-Olds on Eating Habits in the Family and Parental Nutrition Knowledge. Int. J. Environ. Res. Public Health 2022, 19, 1981. [Google Scholar] [CrossRef]
- Ebbinghaus, H. Über das Gedächtnis—Untersuchungen zur Experimentellen Psychologie; Verlag von Duncke&Humblot: Leipzig, Germany, 1985. [Google Scholar]
- Murre, J.M.; Dros, J. Replication and Analysis of Ebbinghaus’ Forgetting Curve. PLoS ONE 2015, 10, e0120644. [Google Scholar] [CrossRef]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F. Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef]
- Kostenius, C.; Hallberg, J.; Lindqvist, A.K. Gamification of health education: Schoolchildren’s participation in the development of a serious game to promote health and learning. Health Educ. 2018, 118, 354–368. [Google Scholar] [CrossRef] [Green Version]
- Kurtzman, G.W.; Day, S.C.; Small, D.S.; Lynch, M.; Zhu, J.; Wang, W.; Rareshide, C.A.L.; Patel, M.S. Social Incentives and Gamification to Promote Weight Loss: The LOSE IT Randomized, Controlled Trial. J. Gen. Intern. Med. 2018, 33, 1669–1675. [Google Scholar] [CrossRef] [Green Version]
- Rendon, A.A.; Lohman, E.B.; Thorpe, D.; Johnson, E.G.; Medina, E.; Bradley, B. The effect of virtual reality gaming on dynamic balance in older adults. Age Ageing 2012, 41, 549–552. [Google Scholar] [CrossRef] [Green Version]
- Hammersley, M.L.; Jones, R.A.; Okely, A.D. Parent-Focused Childhood and Adolescent Overweight and Obesity eHealth Interventions: A Systematic Review and Meta-Analysis. J. Med. Internet Res. 2016, 18, e203. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Children’s Characteristics | FI-Group (n = 23) | CI-Group (n = 21) | p-Value |
|---|---|---|---|
| Age (years), median, M (SD), (range) | 9.5, 9.67 (0.6) (9–11) | 9.5, 9.67 (0.33) (9–10) | 0.842 |
| Sex m; f n (%) | 9 (39.1); 14 (60.9) | 9 (42.9); 12 (57.1) | 0.802 |
| Weight (kg), M (SD), (range) | 37.05 (9.32), (21–67) | 36.05 (6.6), (27–56) | 0.687 |
| Height (cm), M (SD), (range) | 143.73 (9.03) (128–164) | 143.89 (5.27) (128–164) | 0.834 |
| BMI z-score, M (SD), (range) | 17.84 (4), (12.82–32.76) | 17.32 (2.98), (13.50–26.27) | 0.648 |
| Normal Weight n (%) | 15 (68%) | 15 (79%) | - |
| Thinness n (%) | 3 (14%) | 2 (11%) | |
| Overweight n (%) | 3 (14%) | 1 (5%) | |
| Obesity n (%) | 1 (4%) | 1 (5%) | |
| Knowledge score M (SD) % | |||
| Total score (max 60) | 26.68 (5.08) 45% | 27 (7.02) 45% | 0.944 |
| Food pyramid score (max 26) | 13.07 (2.85) 50% | 13.81 (3.25) 53% | 0.902 |
| Energy density score (max 15) | 6.39 (2.68) 43% | 5.71 (3.18) 38% | 0.448 |
| Stress score (max 15) | 6.11 (2.35) 41% | 6.69 (1.69) 45% | 0.759 |
| HNI parent report M (SD) | 9 (1.60) | 10.18 (1.60) | 0.029 * |
| Unfavorable n (%) | 0 (0%) | 0 (0%) | |
| Neutral n (%) | 16 (76%) | 10 (59%) | |
| Favorable n (%) | 5 (23%) | 7 (41%) | |
| HNI Child report M (SD) | 9.45 (1.75) | 10.14 (2.32) | 0.422 |
| Unfavorable n (%) | 0 (0) | 1 (7) | |
| Neutral n (%) | 8 (73) | 6 (43) | |
| Favorable n (%) | 3(27) | 7 (50) | |
| Physical activity parent report | |||
| Score M (SD) | −0.33 (2.03) | 0.06 (2.36) | 0.585 |
| Low n (%) | 3 (14) | 3 (18) | |
| Medium n (%) | 15 (72) | 10 (59) | |
| High n (%) | 3 (14) | 4 (23) | |
| Physical activity child report | |||
| Score M (SD) | −1.11 (2.87) | −0.53 (2.70) | 0.54 |
| Low n (%) | 12 (57) | 11 (52) | |
| Medium n (%) | 6 (29) | 6 (29) | |
| High n (%) | 3 (14) | 4 (19) | |
| Screentime watching n (%) | 0.141 | ||
| ≤0.5 h | 10 (48) | 11(58) | |
| 1–2 h | 11 (52) | 6 (32) | |
| ≥3 h | 0 (0) | 2 (10) | |
| Screentime gaming n (%) | 0.631 | ||
| ≤0.5 h | 19 (95) | 15 (83) | |
| 1–2 h | 1(5) | 3 (17) | |
| ≥3 h | 0 (0) | 0 (0) | |
| Intentions to live healthy | |||
| Score (max 65) M (SD) | 26.65 (7.06) | 25.63 (6.45) | 0.684 |
| Parents’Characteristics | FI-Group (n = 30) | CI-Group (n = 33) | p-Value |
| Age (years), Median, M (SD), (range) | 42, 42.01 (3.68) (36–47) | 42, 42.3 (5.12) (36–52) | 0.876 |
| Sex m; f n (%) | 12 (38.7); 18 (61.3) | 14 (42.4); 19 (57.6) | 0.659 |
| Weight (kg), Median, M (SD), (range) | 77, 78.2 (8.1), (63–88) | 79, 77.2 (6.54), (68–89) | 0.687 |
| Height (cm), M (SD), (range) | 173.2 (6.54) (161–184) | 173.5 (3.72) (167–180) | 0.897 |
| BMI z-score, M (SD), range | 26.1 (6.54) (22.8–32) | 25.6 (2.47) (22.3–30.6) | 0.775 |
| Normal weight n (%) | 18 (60) | 21 (64) | - |
| Thinness n (%) | 5 (17) | 2 (6) | |
| Overweight n (%) | 4 (13) | 8 (24) | |
| Obesity n (%) | 3 (10) | 2 (6) | |
| Knowledge score (both) M (SD) | |||
| Total score (max 45) | 27.57 (3.60) 61% | 26.93 (5.80) 60% | 0.544 |
| Food pyramid score (max 11) | 7.43 (1.74) 68% | 6.71 (2.02) 61% | 0.086 |
| Energy density score (max 15) | 9.33 (1.92) 62% | 9.6 (2.44) 64% | 0.586 |
| Stress score (max 15) | 8.12 (1.65) 55% | 8.19 (1.12) 55% | 0.422 |
| Knowledge score (m) M (SD) | |||
| Total score (max 45) | 27.86 (2.99) 62% | 26.48 (6.47) 59% | 0.38 |
| Food pyramid score (max 11) | 7.1 (1.64) 65% | 6.19 (1.94) 56% | 0.11 |
| Energy density score (max 15) | 9.14 (1.46) 63% | 9.24 (2.49) 66% | 0.88 |
| Stress score (max 15) | 8.05 (0.80) 55% | 7.86 (1.90) 55% | 0.675 |
| Knowledge score (f) M (SD) | |||
| Total score (max 45) | 29.29 (4.08) 65% | 29.38 (4.77) 65% | 0.945 |
| Food pyramid score (max 11) | 7.76 (1.81) 71% | 7.24 (2) 66% | 0.379 |
| Energy density score (max 15) | 9.52 (2.32) 63% | 9.95 (2.4) 66% | 0.559 |
| Stress score (max 15) | 8.19 (1.17) 55% | 8.52 (0.98) 55% | 0.322 |
| FI T0 (n = 21) | FI T1 (n = 21) | FI T2 (n = 21) | CI T0 (n = 21) | CI T1 (n = 21) | CI T2 (n = 21) | FI–CI | Time | Group × Time | |
|---|---|---|---|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | Mean (SD) | F(2,40) | F(2,40) | |
| % | % | % | % | % | % | p | p | p | |
| (95% CI) | Eta² | Eta² | |||||||
| Knowledge (both) | |||||||||
| Total Score | 27.83 (2.96) | 29.77 (5.86) | 30.07 (2.53) | 27.11 (5.61) | 30.98 (2.46) | 29.91 (1.75) | 0.11 (3.69) | 13.73 | 1.37 |
| (max 45) | 62% | 66% | 67% | 60% | 69% | 66% | p = 0.846 [−1.03; 1.25] | p < 0.001 ** 0.156 | p = 0.258 0.018 |
| Food pyramid | 7.43 (1.81) | 8.53 (1.40) | 8.77 (1.00) | 6.82 (1.97) | 8.59 (1.02) | 8.59 (1.05) | −0.24 (1.42) | 26.20 | 0.99 |
| (max 11) | 68% | 78% | 80% | 62% | 78% | 78% | p = 0.265 [−0.68; 0.19] | p < 0.001 ** 0.261 | p = 0.374 0.013 |
| Energy density | 0.82 (0.14) | 0.86 (0.20) | 0.84 (0.16) | 0.82 (0.21) | 0.90 (0.11) | 0.81 (0.14) | 0.00 (1.62) | 3.35 | 0.86 |
| score (max 15) | 5% | 6% | 6% | 5% | 6% | 5% | p = 0.895 [−0.05; 0.05] | p = 0.038 * 0.043 | p = 0.426 0.011 |
| Stress score | 8.07 (0.98) | 8.43 (2.18) | 7.96 (0.58) | 8.28 (1.40) | 8.46 (0.55) | 8.30 (0.59) | 0.19 (1.17) | 1.76 | 0.39 |
| (max 15) | 54% | 56% | 53% | 55% | 56% | 55% | p = 0.289 [−0.17; 0.05] | p = 0.176 0.024 | p = 0.680 0.005 |
| Knowledge Scores | T0 vs. T1 | T0 vs. T2 | T1 vs. T2 |
|---|---|---|---|
| Mean (SD), p (95% CI) | Mean (SD), p (95% CI) | Mean (SD), p (95% CI) | |
| (Both) | |||
| Total | −2.90 (0.72), p < 0.001 ** [−4.66; −1.14] | −2.52 (0.56), p < 0.001 ** [−3.90; −1.14] | 0.38 (0.50), p = 1 [−0.85; 1.62] |
| Food pyramid | −1.43 (0.27), p < 0.001 ** [−2.08; −0.78] | −1.55 (0.24), p < 0.001 ** [−2.14; −0.95] | −0.12 (0.20), p = 1 [−0.61; 0.37] |
| Energy density | −0.06 (0.03), p = 0.115 [−0.12; 0.01] | −0.01 (0.03), p = 1 [−0.07; 0.06] | 0.05 (0.20), p = 0.036 [0.00; 0.10] |
| Stress | −0.27 (0.20), p = −612 [−0.77; 0.24] | 0.04 (0.15), p = 1 [−0.33; 0.42] | 0.31 (0.17), p = 0.228 [−0.11; 0.72] |
| FI | FI | FI | FI | CI | CI | CI | CI | FI–CI | Time | Group × Time | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 21) T0 | (n = 21) T1 | (n = 21) T2 | (n = 21) T3 | (n = 19) T0 | (n = 19) T1 | (n = 19) T2 | (n = 19) T3 | Mean (SD) p | F(2,40) p | F(2,40) p | |
| (95% CI) | Eta2 | Eta2 | |||||||||
| Knowledge scores | |||||||||||
| Total | 27.24 (5.12) | 38.00 (6.10) | 37.53 (3.83) | 37.35 (5.70) | 27.67 (6.69) | 37.00 (5.13) | 35.48 (5.04) | 34.71 (6.60) | −1.32 (8.98) | 47.52 | 1.00 |
| (max 60) | 45% | 63% | 63% | 62% | 46% | 62% | 59% | 58% | p = 0.359 [−4.19; 1.56] | p < 0.001 ** 0.569 | p = 0.398 0.027 |
| Food pyramid | 0.49 (0.17) | 0.75 (0.20) | 0.77 (0.15) | 0.77 (0.15) | 0.50 (0.11) | 0.79 (0.16) | 0.73 (0.15) | 0.73 (0.13) | −0.10 (0.19) | 36.45 | 0.92 |
| (max 26) | 2% | 3% | 3% | 3% | 2% | 3% | 3% | 3% | p = 0.745 [−0.07; 0.05] | p < 0.001 ** 0.49 | p = 0.432 0.024 |
| Energy density | 0.55 (0.24) | 0.74 (0.26) | 0.77 (0.20) | 0.75 (0.22) | 0.59 (0.28) | 0.66 (0.21) | 0.70 (0.24) | 0.64 (0.27) | −0.07 (0.32) | 9.40 | 0.10 |
| (max 15) | 4% | 5% | 5% | 5% | 4% | 4% | 5% | 4% | p = 0.145 [−0.19; 0.03] | p < 0.001 ** 0.23 | p = 0.960 0.003 |
| Stress | 0.64 (0.16) | 0.66 (0.8) | 0.64 (0.09) | 0.67 (0.14) | 0.71 (0.21) | 0.70 (0.12) | 0.63 (0.15) | 0.65 (0.13) | 0.02 (0.25) | 2.09 | 2.28 |
| (max 15) | 4% | 4% | 4% | 4% | 5% | 5% | 4% | 4% | p = 0.955 [−0.07; 0.07] | p = 0.106 0.055 | p = 0.083 0.6 |
| HNI (RbP) | 2.22 (0.44) | ---- | 2.33 (0.50) | 2.33 (0.50) | 2.20 (0.45) | --- | 2.20 (0.45) | 2.00 (0.00) | −0.16 (1.08) p = 0.358 | 0.20 p = 0.817 | 0.51 p = 0.659 |
| [−0.53; 0.21] | 0.017 | 0.04 | |||||||||
| Score | 9.11 (1.54) | ---- | 9.56 (1.88) | 9.67 (1.94) | 9.20 (1.30) | --- | 9.40 (1.14) | 8.60 (1.14) | −0.38 (4.43) p = 0.602 | 0.31 p = 0.735 | 0.78 p = 0.470 |
| [−1.92; 1.16] | 0.025 | 0.061 | |||||||||
| Unfavorable % | 0% | 0% | 0% | 0% | 0% | 0% | |||||
| Neutral % | 79% | 66% | 38% | 59% | 57% | 87% | |||||
| Favorable % | 21% | 33% | 62% | 41% | 43% | 13% | |||||
| HNI (RbC) | 2.43 (0.53) | ---- | 2.29 (0.76) | 2.14 (0.38) | 2.80 (0.45) | --- | 2.80 (0.45) | 2.80 (0.45) | 0.51 (1.26) p = 0.025 * | 0.24 p = 0.792 | 0.24 p = 0.792 |
| [0.08; 0.95] | 0.023 | 0.023 | |||||||||
| Score | 9.71 (2.06) | --- | 9.29 (3.68) | 8.71 (1.38) | 11.00 (1.22) | --- | 10.80 (2.77) | 11.20 (1.92) | 1.76 (6.32) p = 0.109 | 0.13 p = 0.882 | 0.29 p = 0.752 |
| [−0.47; 3.99] | 0.012 | 0.028 | |||||||||
| Unfavorable % | 36% | 4% | 0% | 7% | 0% | 9% | |||||
| Neutral % | 13% | 41% | 80% | 43% | 43% | 45% | |||||
| Favorable % | 50% | 53% | 20% | 49% | 57% | 45% | |||||
| Physical activity level | |||||||||||
| (RbP) | 2.17 (0.75) | --- | 2.00 (0.00) | 2.33 (0.52) | 2.20 (0.84) | --- | 2.40 (0.89) | 2.60 (0.55) | 0.23 (1.71) p = 0.413 | 0.83 p = 0.449 | 0.29 p = 0.755 |
| Score | 0.33 (2.42) | --- | 0.67 (0.82) | 1.67 (2.07) | 0.60 (2.61) | --- | 1.00 (2.83) | 3.00 (2.83) | 0.64 (6.58) p = 0.551 | 2.92 p = 0.080 | 0.27 p = 0.769 |
| [−1.71; 3.00] | 0.245 | 0.029 | |||||||||
| Low activity % | 13% | 10% | 4% | 17% | 14% | 23% | |||||
| Medium activity % | 65% | 41% | 59% | 59% | 53% | 33% | |||||
| High activity % | 13% | 50% | 36% | 24% | 24% | 44% | |||||
| (RbC) | 1.42 (0.67) | --- | 2.00 (0.74) | 1.83 (0.83) | 1.93 (0.83) | --- | 2.00 (0.88) | 2.14 (0.77) | 0.27 (1.71) p = 0.319 | 3.72 p = 0.032 | 1.79 p = 0.178 |
| [−0.28; 0.83] | 0.134 | 0.07 | |||||||||
| Score | −1.73 (2.82) | --- | 0.09 (2.59) | −0.09 (2.88) | −0.08 (2.78) | --- | 0.69 (3.54) | 1.30 (3.82) | 1.22 (7.02) p = 0.288 | 4.60 p = 0.015 | 0.52 p = 0.600 |
| [−1.10; 3.53] | 0.173 | 0.023 | |||||||||
| Low activity % | 52% | 30% | 47% | 52% | 47% | 20% | |||||
| Medium activity % | 26% | 45% | 22% | 29% | 26% | 45% | |||||
| High activity % | 13% | 25% | 30% | 19% | 26% | 35% | |||||
| Media consumption | |||||||||||
| Video/TV | 1.42 (0.52) | --- | 1.33 (0.65) | 1.50 (0.52) | 1.20 (0.63) | --- | 1.20 (0.63) | 1.10 (0.57) | −0.25 (1.33) p = 0.255 | 0.07 p = 0.929 | 0.50 p = 0.501 |
| [−0.70; 0.20] | 0.004 | 0.034 | |||||||||
| ≤0.5 h | 100% | 89% | 95% | 88% | 100% | 100% | |||||
| 1–2 h | 0% | 11% | 5% | 12% | 0% | 0% | |||||
| ≥3 h | 0% | 0% | 0% | 0% | 0% | 0% | |||||
| Computer | 0.64 (0.63) | --- | 1.07 (1.07) | 0.93 (0.73) | 0.83 (0.72) | --- | 0.58 (0.67) | 0.67 (0.65) | −0.19 (1.52) p = 0.444 | 0.16 p = 0.849 | 2.37 p = 0.104 |
| [−0.68; 0.31] | 0.007 | 0.09 | |||||||||
| ≤0.5 h | 100% | 93% | 100% | 100% | 100% | 100% | |||||
| 1–2 h | 0% | 0% | 0% | 0% | 0% | 0% | |||||
| ≥3 h | 0% | 7% | 0% | 0% | 0% | 0% | |||||
| T0 vs. T1 | T0 vs. 2 | T0 vs. T3 | T1 vs. T2 | T1 vs. T3 | T2 vs. T3 | |
|---|---|---|---|---|---|---|
| Mean (SD), p | Mean (SD), p | Mean (SD), p | Mean (SD), p | Mean (SD), p | Mean (SD), p | |
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | |
| Knowledge | ||||||
| Total score | −10.05 (1.31), p < 0.001 ** | −9.05 (0.97), p < 0.001 ** | −8.58 (1.21), p < 0.001 ** | 0.10 (0.73), p = 1 | 1.47 (0.83), p = 0.507 | 0.47 (0.75), p = 1 |
| [−13.21; −6.89] | [−11.75; −6.35] | [11.97; −5.20] | [−1.59; 3.05] | [−0.84; 3.77] | [−1.62; 2.56] | |
| Food pyramid score | −0.27 (0.40), p < 0.001 ** | −0.25 (0.03), p < 0.001 ** | −0.25 (0.03), p < 0.001 ** | 0.02 (0.03), p = 1 | 0.02 (0.03), p = 1 | 0.00 (0.02), p = 1 |
| [−0.38; −0.16] | [−0.34; −0.16] | [−0.34; −0.16] | [−0.05; 0.10] | [−0.05; 0.09] | [−0.06; 0.06] | |
| Energy density score | −0.18 (0.05), p = 0.007 * | −0.22 (0.05), p < 0.001 ** | −0.18 (0.06), p = 0.018 * | −0.03 (0.03), p = 1 | 0.01 (0.4), p = 1 | 0.04 (0.40), p = 1 |
| [−0.33; 0.38] | [−0.35; −0.08] | [−0.33; −0.02] | [−0.11; 0.05] | [−0.10; 0.12] | [−0.07; 0.15] | |
| Stress score | −0.01 (0.03), p = 1 | 0.03 (0.03), p = 1 | 0.01 (0.04), p = 1 | 0.04 (0.02), p = 0.86 | 0.02 (0.02), p = 1 | −0.03 (0.02), p = 1 |
| [−0.1; 0.09] | [−0.06; 0.13] | [−0.09; 0.12] | [−0.04; 0.09] | [−0.04; 0.08] | [−0.09; 0.04] | |
| HNI RbP | --- | −0.06 (0.18), p = 1 | 0.04 (0.16), p = 1 | --- | --- | 0.10 (0.14), p = 1 |
| [−0.55; 0.44] | [−0.385; 0.47] | [−0.27; 0.47] | ||||
| HNI score | --- | −0.32 (0.56), p = 1 | 0.02 (0.45), p = 1 | --- | --- | 0.34 (0.44), p = 1 |
| [−1.89; 1.25] | [−1.23; 1.28] | [−0.88; 1.56] | ||||
| HNI RbC | --- | 0.07 (0.20), p = 1 | 0.14 (0.17), p = 1 | --- | --- | 0.07 (0.24), p = 1 |
| [−0.51; 0.66] | [−0.35; 0.64] | [−0.62; 0.77] | ||||
| HNI score | --- | 0.31 (0.95), p = 1 | 0.40 (0.48), p = 1 | --- | --- | 0.09 (0.99), p = 1 |
| [−2.40; 3.03] | [−0.976; 1.78] | [−2.76; 2.93] | ||||
| Physical activity RbP | --- | −0.02 (0.24), p = 1 | −0.28 (0.29), p = 1 | --- | --- | −0.27 (0.20), p = 0.678 |
| [−0.72; 0.69] | [−1.12; 0.56] | [−0.87; 0.03] | ||||
| Score | --- | −0.37 (0.56), p = 1 | −1.87 (0.99), p = 0.277 | --- | --- | −1.50 (0.84), p = 0.328 |
| [−2.00; 1.27] | [−4.78; 1.04] | [−3.98; 0.98] | ||||
| Physical activity RbC | --- | −0.33 (0.14), p = 0.079 | −0.31 (0.14), p = 0.08 | --- | --- | 0.01 (0.13), p = 1 |
| [−0.68; 0.03] | [−0.66; 0.03] | [−0.34; 0.36] | ||||
| Score | --- | −1.29 (0.51), p = 0.056 | −1.15 (0.54), p = 0.032 * | --- | --- | −0.22 (0.56), p = 1 |
| [−2.61; 0.03] | [−2.91; −0.11] | [−1.68; 1.24] | ||||
| Media Consumption | ||||||
| Video/TV | --- | 0.04 (0.10), p = 1 | 0.01 (0.12), p = 1 | --- | --- | −0.03 (0.12), p = 1 |
| [−0.24; 0.32] | [−0.29; 0.31] | [−0.35; 0.29] | ||||
| Computer | --- | −0.09 (0.17), p = 1 | −0.06 (0.14), p = 1 | --- | 0.03 (0.16), p = 1 | |
| [−0.52; 0.35] | [−0.43; 0.31] | [−0.39; 0.45] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weiland, A.; Reiband, N.; Schäffeler, N.; Zurstiege, G.; Giel, K.E.; Zipfel, S.; Mack, I. A Serious Game for the Prevention of Obesity in School Children–Impact of Parent’s Involvement: A Randomized Controlled Trial. Life 2022, 12, 779. https://doi.org/10.3390/life12060779
Weiland A, Reiband N, Schäffeler N, Zurstiege G, Giel KE, Zipfel S, Mack I. A Serious Game for the Prevention of Obesity in School Children–Impact of Parent’s Involvement: A Randomized Controlled Trial. Life. 2022; 12(6):779. https://doi.org/10.3390/life12060779
Chicago/Turabian StyleWeiland, Alisa, Nadine Reiband, Norbert Schäffeler, Guido Zurstiege, Katrin Elisabeth Giel, Stephan Zipfel, and Isabelle Mack. 2022. "A Serious Game for the Prevention of Obesity in School Children–Impact of Parent’s Involvement: A Randomized Controlled Trial" Life 12, no. 6: 779. https://doi.org/10.3390/life12060779