
Psoas Muscle Area Predicts Mortality after Left Ventricular Assist Device Implantation

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
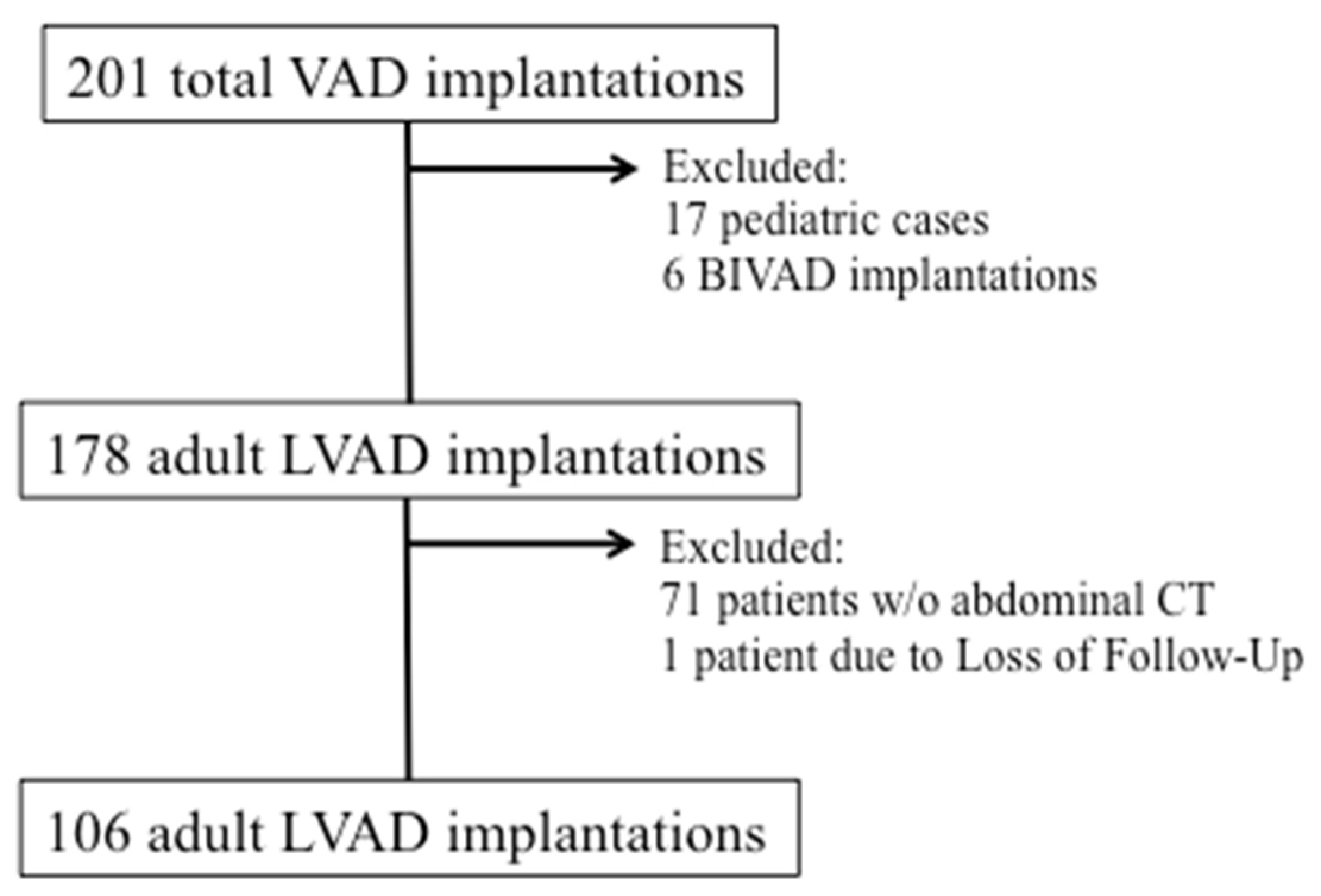
2.1. Patient Population
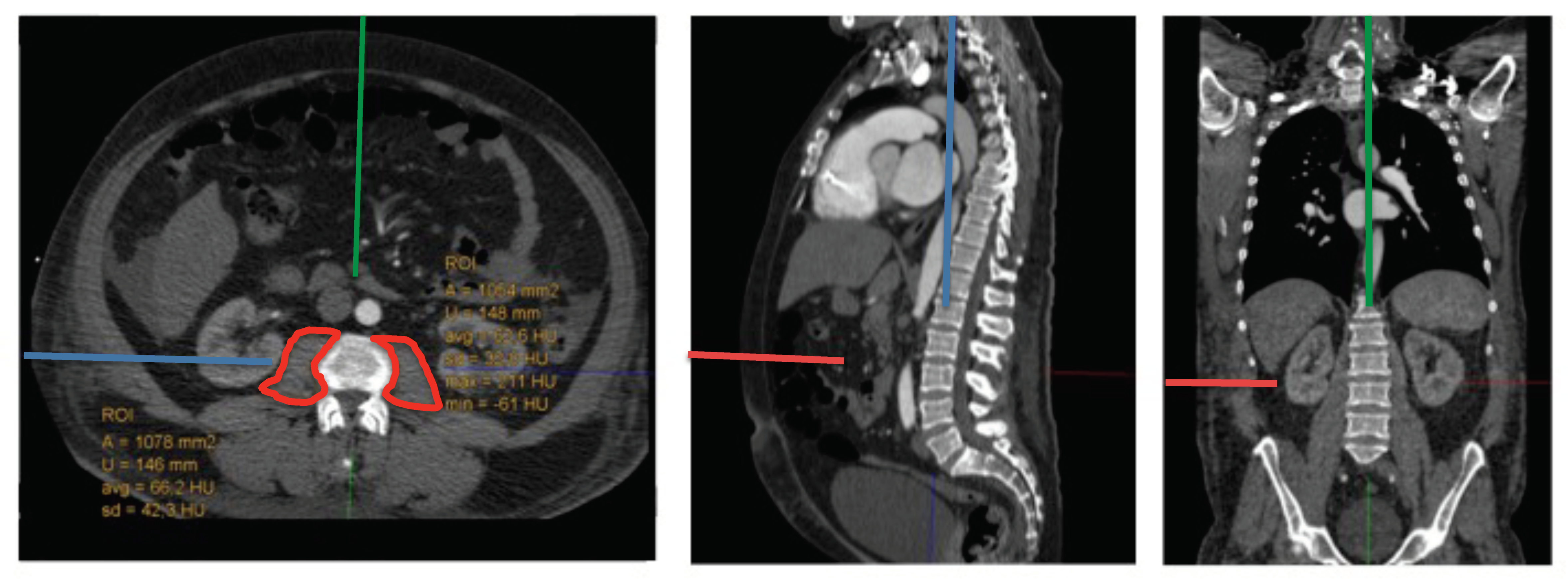
2.2. Measurement of Indexed Psoas Mean Area (PMAi)
2.3. Study Outcomes
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
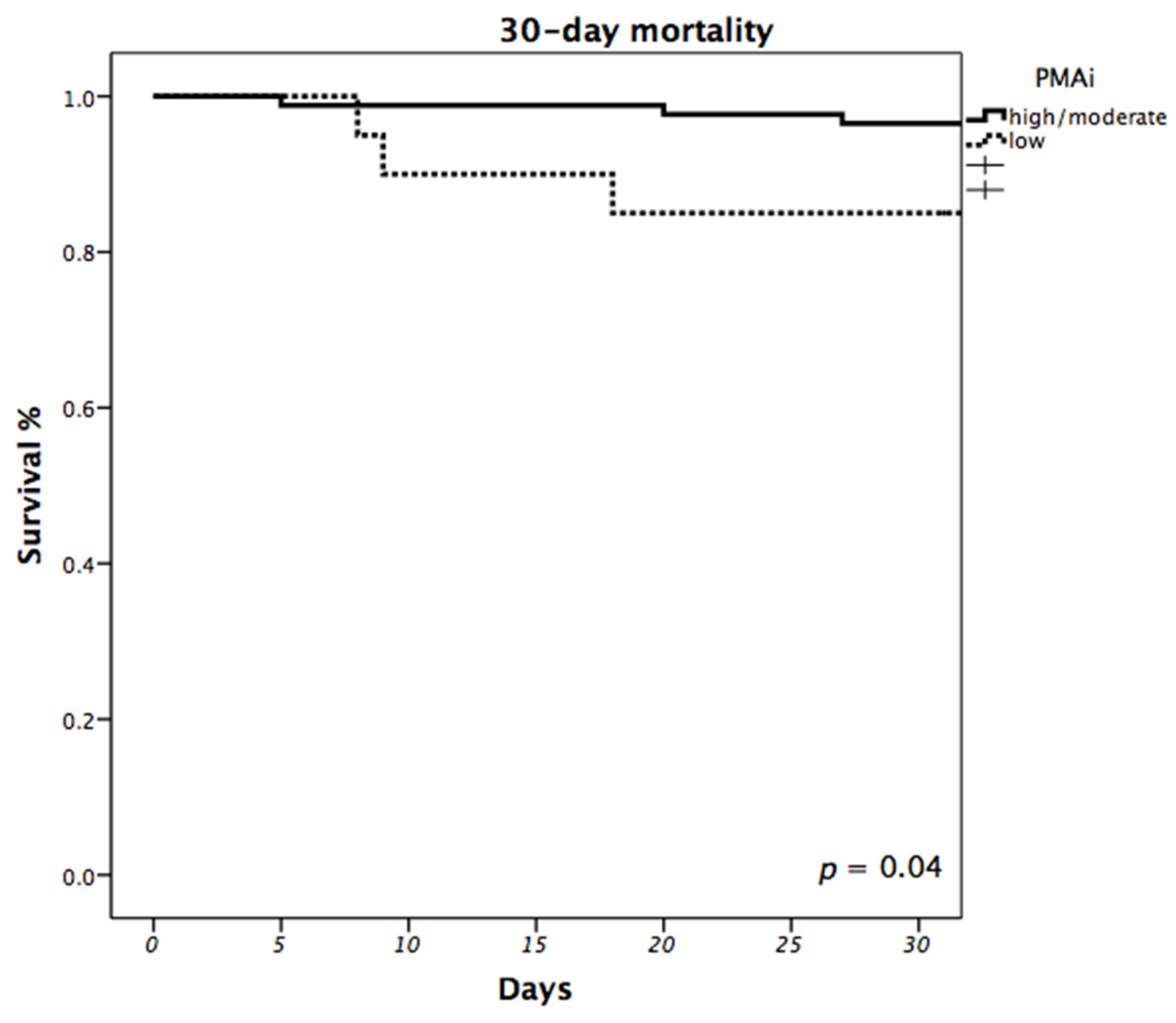
3.2. Impact of PMAi on Mortality
3.3. Impact of PMAi on Post-Operative Intensive Care Effort
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Variable | Total Population (n = 106) | High/Moderate PMAi (n = 86) | Low PMAi (n = 20) | p-Value |
|---|---|---|---|---|
| Renal Dysfunction | 20 (18.9) | 15 (17.4) | 5 (25) | 0.526 |
| Arrhythmias | 33 (31.1) | 28 (32.6) | 5 (25) | 0.928 |
| Hemolysis | 12 (11.3) | 9 (10.5) | 3 (15) | 0.566 |
| Hepatic Dysfunction | 9 (8.5) | 7 (8.1) | 2 (10) | 0.677 |
| Hypertension | 6 (5.7) | 4 (4.7) | 2 (10) | 0.316 |
| Major Bleeding | ||||
| requiring surgery | 16 (15.1) | 11 (12.8) | 5 (25) | 0.295 |
| gastrointestinal | 6 (5.7) | 4 (4.7) | 2 (10) | |
| both of the above | 7 (6.6) | 6 (7) | 1 (5) | |
| Major Infection | ||||
| sepsis | 17 (16) | 14 (16.3) | 3 (15) | 1.0 |
| driveline | 1 (0.9) | 1 (1.2) | 0 | |
| local | 2 (1.9) | 2 (2.3) | 0 | |
| Neurological Dysfunction | ||||
| ischemic stroke | 7 (6.6) | 6 (7) | 1 (5) | 0.9 |
| hemorrhagic stroke | 0 | 0 | 0 | |
| other | 17 (16) | 13 (15.1) | 4 (20) | |
| Pericardial Fluid Collection | 12 (11.3) | 9 (10.5) | 3 (15) | 0.694 |
| Psychiatric | 26 (24.5) | 20 (23.3) | 6 (30) | 0.568 |
| Respiratory Insufficiency | 24 (22.6) | 19 (22.1) | 5 (25) | 0.772 |
| Right Heart Failure | ||||
| right heart decompensation | 4 (3.8) | 3 (3.5) | 1 (5) | 0.729 |
| ECMO implant | 2 (1.9) | 2 (2.3) | 0 | |
| Venous Thromboembolism | 2 (1.9) | 1 (1.2) | 1 (5) | 0.343 |
| Wound Dehiscence | 4 (3.8) | 2 (2.3) | 2 (10) | 0.161 |
| Readmission ICU | 12 (11.3) | 10 (11.6) | 2 (10) | 1.0 |
| Other Complication | 19 (17.9) | 15 (17.4) | 4 (20) | 0.754 |
References
- Roger, V.L. Epidemiology of Myocardial Infarction. Med. Clin. N. Am. 2007, 91, 537–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braunwald, E. The war against heart failure: The Lancet lecture. Lancet 2015, 385, 812–824. [Google Scholar] [CrossRef]
- Gustafsson, F.; Rogers, J.G. Left ventricular assist device therapy in advanced heart failure: Patient selection and outcomes. Eur. J. Heart Fail. 2017, 19, 595–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, L.W.; Pagani, F.D.; Young, J.B.; Jessup, M.; Miller, L.; Kormos, R.L.; Naftel, D.C.; Ulisney, K.; Desvigne-Nickens, P.; Kirklin, J.K. Mechanical Circulatory Support Intermacs Profiles of Advanced Heart Failure: The Current Picture. J. Heart Lung Transplant. 2009, 28, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, B.; Graham, M.M.; Afilalo, J.; Hassan, A.; Arora, R.C. Frailty as a risk predictor in cardiac surgery: Beyond the eyeball test. J. Thorac. Cardiovasc. Surg. 2018, 156, 172–176.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, S.J.G.; Frizelle, F.A.; Geddes, J.A.; Eglinton, T.W.; Hampton, M.B. Frailty in surgical patients. Int. J. Color. Dis. 2018, 33, 1657–1666. [Google Scholar] [CrossRef] [PubMed]
- Hülsmann, M.; Quittan, M.; Berger, R.; Crevenna, R.; Springer, C.; Nuhr, M.; Mörtl, D.; Moser, P.; Pacher, R. Muscle strength as a predictor of long-term survival in severe congestive heart failure. Eur. J. Heart Fail. 2004, 6, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Kofler, M.; Reinstadler, S.J.; Mayr, A.; Stastny, L.; Reindl, M.; Dumfarth, J.; Dachs, T.M.; Wachter, K.; Rustenbach, C.J.; Friedrich, G.; et al. Prognostic implications of psoas muscle area in patients undergoing transcatheter aortic valve implantation. Eur. J. Cardio-Thorac. Surg. 2018, 55, 210–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paknikar, R.; Friedman, J.; Cron, D.; Deeb, G.M.; Chetcuti, S.; Grossman, P.M.; Wang, S.; Englesbe, M.; Patel, H.J. Psoas muscle size as a frailty measure for open and transcatheter aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2016, 151, 745–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flint, B. Hall CA: Body Surface Area (BSA); StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Kirklin, J.K.; Xie, R.; Cowger, J.; de By, T.M.; Nakatani, T.; Schueler, S.; Taylor, R.; Lannon, J.; Mohacsi, P.; Gummert, J.; et al. Second annual report from the ISHLT Mechanically Assisted Circulatory Support Registry. J. Heart Lung Transplant. 2018, 37, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Piffard, M.; Coniat, K.N.; Simon, O.; Leuillet, S.; Rémy, A.; Barandon, L.; Ouattara, A. Independent risk factors for ICU mortality after left ventricular assist device implantation. Artif. Organs 2020, 44, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.J.; Wu, C.; Jones, M.; Kato, T.S.; Dam, T.T.; Givens, R.C.; Templeton, D.L.; Maurer, M.S.; Naka, Y.; Takayama, H.; et al. Reduced Handgrip Strength as a Marker of Frailty Predicts Clinical Outcomes in Patients With Heart Failure Undergoing Ventricular Assist Device Placement. J. Card. Fail. 2014, 20, 310–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afilalo, J.; Eisenberg, M.J.; Morin, J.-F.; Bergman, H.; Monette, J.; Noiseux, N.; Perrault, L.P.; Alexander, K.P.; Langlois, Y.; Dendukuri, N.; et al. Gait Speed as an Incremental Predictor of Mortality and Major Morbidity in Elderly Patients Undergoing Cardiac Surgery. J. Am. Coll. Cardiol. 2010, 56, 1668–1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, S.M.; Manghelli, J.L.; Vader, J.M.; Keeney, T.; Novak, E.L.; Felius, J.; Martinez, S.C.; Nassif, M.E.; Lima, B.; Silvestry, S.C.; et al. Prospective Assessment of Frailty Using the Fried Criteria in Patients Undergoing Left Ventricular Assist Device Therapy. Am. J. Cardiol. 2017, 120, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, M.; Kamiya, K.; Matsunaga, A.; Kitamura, T.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Tanaka, S.; Nakamura, T.; Maekawa, E.; et al. Prognostic Value of Psoas Muscle Area and Density in Patients Who Undergo Cardiovascular Surgery. Can. J. Cardiol. 2017, 33, 1652–1659. [Google Scholar] [CrossRef] [PubMed]
- Heberton, G.A.; Nassif, M.; Bierhals, A.; Novak, E.; LaRue, S.J.; Lima, B.; Hall, S.; Silvestry, S.; Joseph, S.M. Usefulness of Psoas Muscle Area Determined by Computed Tomography to Predict Mortality or Prolonged Length of Hospital Stay in Patients Undergoing Left Ventricular Assist Device Implantation. Am. J. Cardiol. 2016, 118, 1363–1367. [Google Scholar] [CrossRef] [PubMed]
- Teigen, L.M.; John, R.; Kuchnia, A.J.; Nagel, E.M.; Earthman, C.P.; Kealhofer, J.; Martin, C.; Cogswell, R. Preoperative Pectoralis Muscle Quantity and Attenuation by Computed Tomography Are Novel and Powerful Predictors of Mortality After Left Ventricular Assist Device Implantation. Circ. Heart Fail. 2017, 10, e004069. [Google Scholar] [CrossRef] [PubMed]



| Variable | Total Population (n = 106) | High/Moderate PMAi (n = 86) | Low PMAi (n = 20) | p-Value |
|---|---|---|---|---|
| Sex | ||||
| male, n (%) | 96 (90.6) | 79 (90.7) | 18 (90) | 0.92 |
| female, n (%) | 10 (9.4) | 8 (9.3) | 2 (10) | |
| Age at implant | 65 (IQR 12) | 65 (IQR 12) | 63 ± 9 | 0.80 |
| INTERMACS profile, n (%) | ||||
| 1 | 26 (24.5) | 18 (20.9) | 8 (40) | 0.24 |
| 2 | 18 (17) | 14 (16.3) | 4 (20) | |
| 3 | 16 (15.1) | 13 (15.1) | 3 (15) | |
| 4 | 42 (39.6) | 38 (44.2) | 4 (20) | |
| 5 | 3 (2.8) | 2 (2.3) | 1 (5) | |
| 6 | 0 | 0 | 0 | |
| 7 | 1 (0.9) | 1 (1.2) | 0 | |
| Etiology of Heart Failure | ||||
| ischemic, n (%) | 68 (64.2) | 58 (67.4) | 10 (50) | 0.25 |
| dilated, n (%) | 36 (34) | 27 (31.4) | 9 (45) | |
| other, n (%) | 2 (1.9) | 1 (1.2) | 1 (5) | |
| Implantation Strategy | ||||
| BTT, n (%) | 4 (3.8) | 4 (4.7) | 0 | 0.59 |
| BTC, n (%) | 79 (74.5) | 63 (73.3) | 16 (80) | |
| DT, n (%) | 23 (21.7) | 19 (22.1) | 4 (20) | |
| BMI, kg/m2 | 26.4 (IQR 7.6) | 26.6 (IQR 7.7) | 28.0 ±6.2 | 0.46 |
| Body surface area, m2 | 2.0 ± 0.2 | 2.0 ± 0.2 | 2.0 ± 0.2 | 0.80 |
| Comorbidities, n (%) | ||||
| Atrial fibrillation | 31 (29.2) | 26 (30.2) | 5 (25) | 0.64 |
| Diabetes Mellitus | ||||
| oral therapy | 26 (24.5) | 22 (25.6) | 4 (20) | 0.52 |
| insulin dependent | 13 (12.3) | 9 (10.5) | 4 (20) | |
| History of Stroke | 9 (8.5) | 8 (9.3) | 1 (5) | 0.51 |
| Arterial HT | 38 (35.8) | 32 (37.2) | 6 (30) | 0.55 |
| Pulmonary HT | 37 (34.9) | 33 (38.4) | 4 (20) | 0.12 |
| COPD | 19 (17.9) | 14 (16.3) | 5 (25) | 0.38 |
| Dyslipidemia | 35 (33) | 30 (34.9) | 5 (25) | 0.40 |
| Chronic renal failure | 41 (38.7) | 33 (38.4) | 8 (40) | 0.90 |
| PVD | 5 (4.7) | 4 (4.7) | 1 (5) | 0.95 |
| Cerebrov. disease | 1 (0.9) | 0 | 1 (5) | 0.07 |
| Redo case | 28 (26.4) | 23 (26.7) | 5 (25) | 0.87 |
| Access, n (%) | ||||
| Full sternotomy | 62 (58.5) | 53 (61.6) | 9 (45) | 0.17 |
| Less invasive strategy | 44 (41.5) | 33 (38.4) | 11 (55) | |
| Creatinine, mg/dL | 1.49 (IQR 0.8) | 1.53 ± 0.5 | 1.72 ± 0.9 | 0.46 |
| Total bilirubin, mg/dL | 0.86 (IQR 0.8) | 0.86 (IQR 0.8) | 0.67 (IQR 1.4) | 0.23 |
| Albumin, g/L | 35.2 (IQR 9.7) | 35.6 (IQR 9.65) | 33.9 (IQR 13.2) | 0.26 |
| PMAi L3, mm2/m2 | 942.6 ± 234.5 | 991.82 ± 207.1 | 618.15 (IQR 73.9) | <0.001 |
| Variables | Hazard Ratio | Confidence Interval (95%) | p-Value |
|---|---|---|---|
| Group PMAi | |||
| high/moderate | Ref. | 2.736–272.797 | 0.005 |
| low | 27.3 | ||
| Redo | 29.8 | 1.894–467.644 | 0.016 |
| Access | |||
| FS | Ref. | 0.000–9.073 × 10199 | 0.956 |
| LIS | 0.000 | ||
| Bilirubin | 1.426 | 1.093–1.860 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wittmann, F.; Schlöglhofer, T.; Riebandt, J.; Schaefer, A.-K.; Wiedemann, D.; Tschernko, E.; Beitzke, D.; Loewe, C.; Laufer, G.; Zimpfer, D. Psoas Muscle Area Predicts Mortality after Left Ventricular Assist Device Implantation. Life 2021, 11, 922. https://doi.org/10.3390/life11090922
Wittmann F, Schlöglhofer T, Riebandt J, Schaefer A-K, Wiedemann D, Tschernko E, Beitzke D, Loewe C, Laufer G, Zimpfer D. Psoas Muscle Area Predicts Mortality after Left Ventricular Assist Device Implantation. Life. 2021; 11(9):922. https://doi.org/10.3390/life11090922
Chicago/Turabian StyleWittmann, Franziska, Thomas Schlöglhofer, Julia Riebandt, Anne-Kristin Schaefer, Dominik Wiedemann, Edda Tschernko, Dietrich Beitzke, Christian Loewe, Günther Laufer, and Daniel Zimpfer. 2021. "Psoas Muscle Area Predicts Mortality after Left Ventricular Assist Device Implantation" Life 11, no. 9: 922. https://doi.org/10.3390/life11090922