
Effects of Resistance Exercise with or without Whey Protein Supplementation on Ocular Changes after a 21-Day Head-Down Bed Rest

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
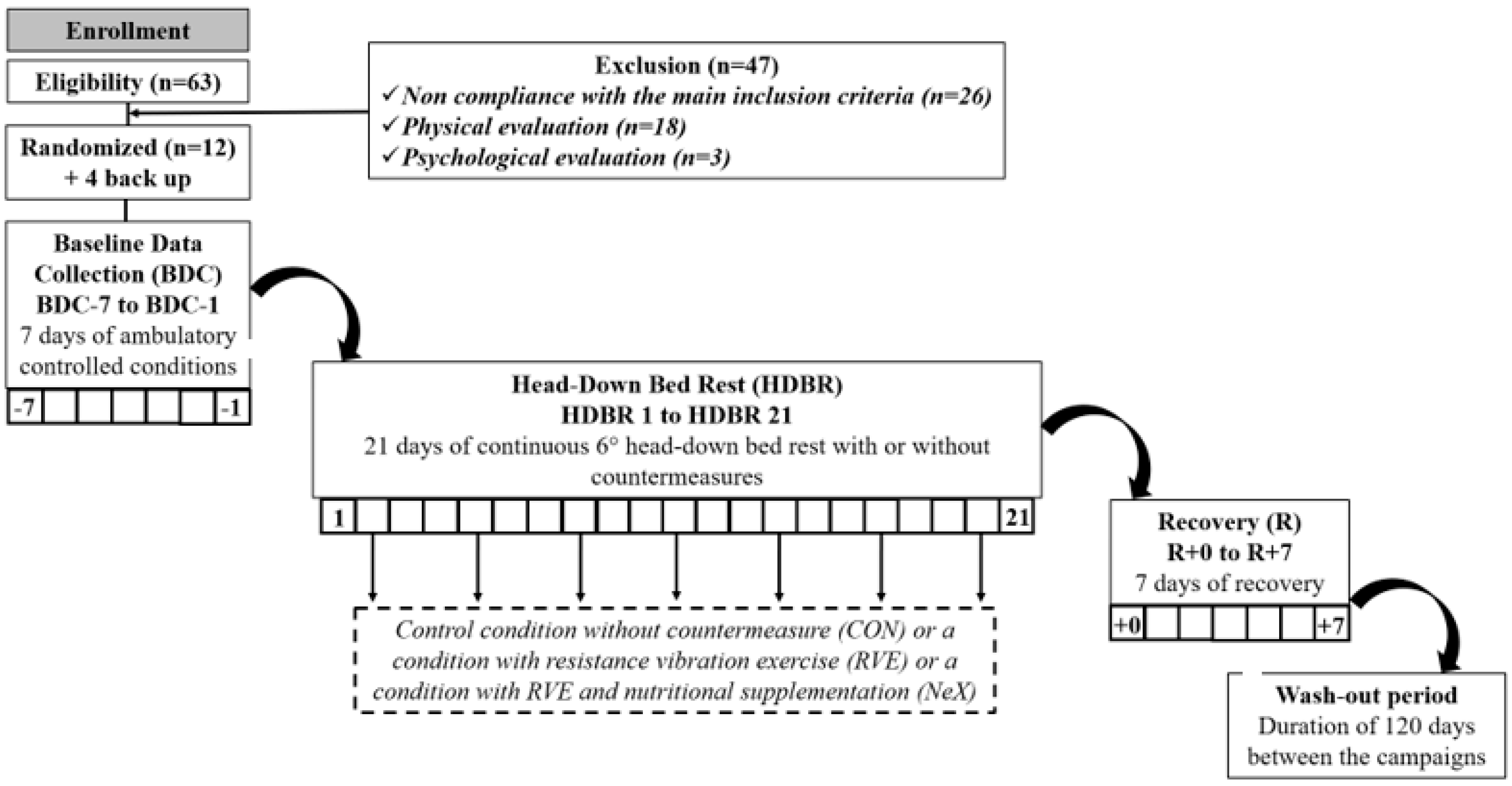
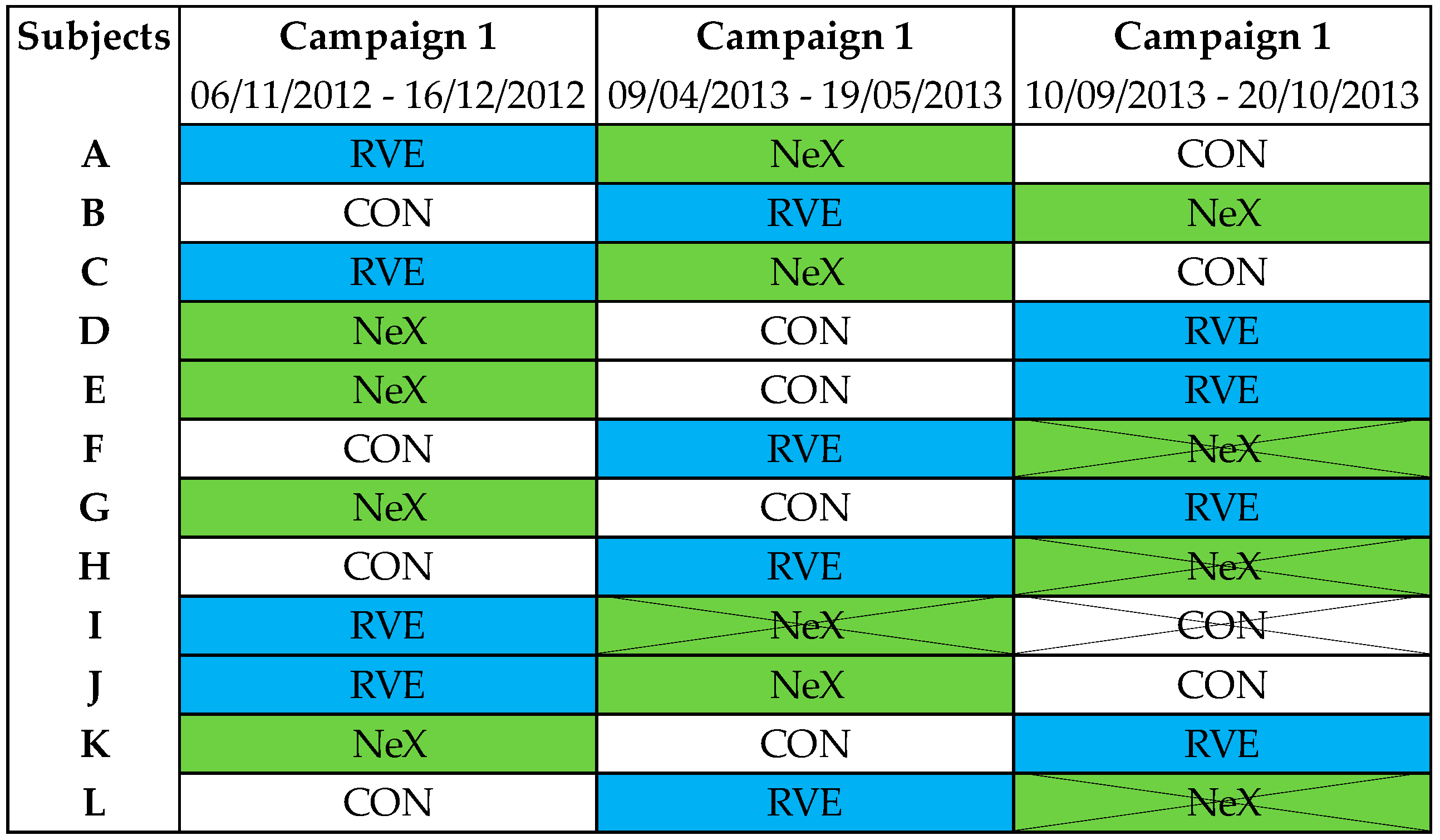
2.2. General Description
2.3. Countermeasures Description
2.3.1. Resistance Vibration Protocol
2.3.2. Nutritional Supplementation
2.4. Intraocular Pressure Measures
2.5. Optical Coherence Tomography Measures
2.6. Eye Examination
2.7. Statistical Analysis
3. Results
3.1. Eye Examination
3.2. Intraocular Pressure Measures
3.3. Optical Coherence Tomography Measures
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, A.G. Neuroimaging in Space Flight Associated Neuro-Ocular Syndrome (SANS). Eye 2021, 35, 1799–1800. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.G.; Mader, T.H.; Gibson, C.R.; Tarver, W.; Rabiei, P.; Riascos, R.F.; Galdamez, L.A.; Brunstetter, T. Spaceflight Associated Neuro-Ocular Syndrome (SANS) and the Neuro-Ophthalmologic Effects of Microgravity: A Review and an Update. NPJ Microgravity 2020, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macias, B.R.; Patel, N.B.; Gibson, C.R.; Samuels, B.C.; Laurie, S.S.; Otto, C.; Ferguson, C.R.; Lee, S.M.C.; Ploutz-Snyder, R.; Kramer, L.A.; et al. Association of Long-Duration Spaceflight With Anterior and Posterior Ocular Structure Changes in Astronauts and Their Recovery. JAMA Ophthalmol. 2020, 138, 553. [Google Scholar] [CrossRef] [PubMed]
- English, K.L.; Downs, M.; Goetchius, E.; Buxton, R.; Ryder, J.W.; Ploutz-Snyder, R.; Guilliams, M.; Scott, J.M.; Ploutz-Snyder, L.L. High Intensity Training during Spaceflight: Results from the NASA Sprint Study. NPJ Microgravity 2020, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Sandal, P.H.; Kim, D.; Fiebig, L.; Winnard, A.; Caplan, N.; Green, D.A.; Weber, T. Effectiveness of Nutritional Countermeasures in Microgravity and Its Ground-Based Analogues to Ameliorate Musculoskeletal and Cardiopulmonary Deconditioning—A Systematic Review. PLoS ONE 2020, 15, e0234412. [Google Scholar] [CrossRef] [PubMed]
- Zwart, S.R.; Gibson, C.R.; Mader, T.H.; Ericson, K.; Ploutz-Snyder, R.; Heer, M.; Smith, S.M. Vision Changes after Spaceflight Are Related to Alterations in Folate– and Vitamin B-12–Dependent One-Carbon Metabolism. J. Nutr. 2012, 142, 427–431. [Google Scholar] [CrossRef] [Green Version]
- Lempert, P.; Cooper, K.H.; Culver, J.F.; Tredici, T.J. The Effect of Exercise on Intraocular Pressure. Am. J. Ophthalmol. 1967, 63, 1673–1676. [Google Scholar] [CrossRef]
- Vieira, G.M. Intraocular Pressure Variation During Weight Lifting. Arch. Ophthalmol. 2006, 124, 1251. [Google Scholar] [CrossRef] [Green Version]
- Michael, A.P. Spaceflight Induced Changes in the Central Nervous System. In Into Space—A Journey of How Humans Adapt and Live in Microgravity; Russomano, T., Rehnberg, L., Eds.; InTechOpen: London, UK, 2018; ISBN 978-1-78923-220-2. [Google Scholar]
- Lane, H.W.; Bourland, C.; Barrett, A.; Heer, M.; Smith, S.M. The Role of Nutritional Research in the Success of Human Space Flight. Adv. Nutr. 2013, 4, 521–523. [Google Scholar] [CrossRef] [Green Version]
- Pavy-Le Traon, A.; Heer, M.; Narici, M.V.; Rittweger, J.; Vernikos, J. From Space to Earth: Advances in Human Physiology from 20 Years of Bed Rest Studies (1986–2006). Eur. J. Appl. Physiol. 2007, 101, 143–194. [Google Scholar] [CrossRef]
- Kermorgant, M.; Nasr, N.; Custaud, M.-A.; Navasiolava, N.; Arbeille, P.; Guinet, P.; Labrunée, M.; Besnier, F.; Arvanitis, D.N.; Czosnyka, M.; et al. Effects of Resistance Exercise and Nutritional Supplementation on Dynamic Cerebral Autoregulation in Head-Down Bed Rest. Front. Physiol. 2019, 10, 1114. [Google Scholar] [CrossRef] [Green Version]
- Draeger, J.; Schwartz, R.; Groenhoff, S.; Stern, C. Self-Tonometry under Microgravity Conditions. Clin. Investig. 1993, 71. [Google Scholar] [CrossRef]
- Draeger, J.; Schwartz, R.; Groenhoff, S.; Stern, C. Self tonometry during the German 1993 Spacelab D2 mission. Ophthalmologe 1994, 91, 697–699. [Google Scholar]
- Stenger, M.B.; Tarver, W.J.; Brunstetter, T.; Gibson, C.R.; Laurie, S.S.; Lee, S.M.C. Evidence Report: Risk of Spaceflight Associated Neuro- Ocular Syndrome (SANS); Houston National Aeronautics Space Administration (NASA): Houston, TX, USA, 2017; pp. 1–109. [Google Scholar]
- Huang, A.S.; Stenger, M.B.; Macias, B.R. Gravitational Influence on Intraocular Pressure: Implications for Spaceflight and Disease. J. Glaucoma 2019, 28, 756–764. [Google Scholar] [CrossRef]
- Chiquet, C.; Custaud, M.-A.; Le Traon, A.P.; Millet, C.; Gharib, C.; Denis, P. Changes in Intraocular Pressure during Prolonged (7-Day) Head-Down Tilt Bedrest. J. Glaucoma 2003, 12, 204–208. [Google Scholar] [CrossRef]
- Jóhannesson, G.; Eklund, A.; Lindén, C. Intracranial and Intraocular Pressure at the Lamina Cribrosa: Gradient Effects. Curr. Neurol. Neurosci. Rep. 2018, 18, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taibbi, G.; Kaplowitz, K.; Cromwell, R.L.; Godley, B.F.; Zanello, S.B.; Vizzeri, G. Effects of 30-Day Head-Down Bed Rest on Ocular Structures and Visual Function in a Healthy Subject. Aviat. Space Environ. Med. 2013, 84, 148–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taibbi, G.; Cromwell, R.L.; Zanello, S.B.; Yarbough, P.O.; Ploutz-Snyder, R.J.; Godley, B.F.; Vizzeri, G. Ocular Outcomes Comparison Between 14- and 70-Day Head-Down-Tilt Bed Rest. Investig. Ophthalmol. Vis. Sci. 2016, 57, 495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritsch, J.M.; Charles, J.B.; Bennett, B.S.; Jones, M.M.; Eckberg, D.L. Short-Duration Spaceflight Impairs Human Carotid Baroreceptor-Cardiac Reflex Responses. J. Appl. Physiol. 1992, 73, 664–671. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, A.; Lin, C.; Shackelford, L.; Sinitsyn, V.; Evans, H.; Belichenko, O.; Schenkman, B.; Kozlovskaya, I.; Oganov, V.; Bakulin, A.; et al. Muscle Volume, MRI Relaxation Times (T2), and Body Composition after Spaceflight. J. Appl. Physiol. 2000, 89, 2158–2164. [Google Scholar] [CrossRef]
- Shackelford, L.C.; LeBlanc, A.D.; Driscoll, T.B.; Evans, H.J.; Rianon, N.J.; Smith, S.M.; Spector, E.; Feeback, D.L.; Lai, D. Resistance Exercise as a Countermeasure to Disuse-Induced Bone Loss. J. Appl. Physiol. 2004, 97, 119–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekjavic, I.B.; Amoaku, W.; Mlinar, T.; Jaki Mekjavic, P. Hypercapnia Augments Resistive Exercise-induced Elevations in Intraocular Pressure in Older Individuals. Exp. Physiol. 2020, 105, 641–651. [Google Scholar] [CrossRef]
- Hargens, A.R.; Macias, B.R.; Otto, C.A.; Liu, J.H.K. Intracranial Pressure and Its Effect on Vision in Space and on Earth: Vision Impairment in Space; World Scientific Publishing Company: Singapore, 2017; ISBN 978-981-4667-12-8. [Google Scholar]
- Marshall-Bowman, K.; Barratt, M.R.; Gibson, C.R. Ophthalmic Changes and Increased Intracranial Pressure Associated with Long Duration Spaceflight: An Emerging Understanding. Acta Astronaut. 2013, 87, 77–87. [Google Scholar] [CrossRef]
- Dickerman, R.D.; Smith, G.H.; Langham-Roof, L.; McConathy, W.J.; East, J.W.; Smith, A.B. Intra-Ocular Pressure Changes during Maximal Isometric Contraction: Does This Reflect Intra-Cranial Pressure or Retinal Venous Pressure? Neurol. Res. 1999, 21, 243–246. [Google Scholar] [CrossRef]
- Avunduk, A.M.; Yilmaz, B.; Şahin, N.; Kapicioglu, Z.; Dayanır, V. The Comparison of Intraocular Pressure Reductions after Isometric and Isokinetic Exercises in Normal Individuals. Ophthalmologica 1999, 213, 290–294. [Google Scholar] [CrossRef]
- Chromiak, J.A.; Abadie, B.R.; Braswell, R.A.; Koh, Y.S.; Chilek, D.R. Resistance Training Exercises Acutely Reduce Intraocular Pressure in Physically Active Men and Women. J. Strength Cond. Res. 2003, 17, 715–720. [Google Scholar] [CrossRef]
- Rüfer, F.; Schiller, J.; Klettner, A.; Lanzl, I.; Roider, J.; Weisser, B. Comparison of the Influence of Aerobic and Resistance Exercise of the Upper and Lower Limb on Intraocular Pressure. Acta Ophthalmol. 2014, 92, 249–252. [Google Scholar] [CrossRef] [Green Version]
- Vieira, G.M.; Penna, E.P.; Marques, M.B.; Bezerra, R.F. The Accute Effects of Resistance Exercise on Intraocular Pressure. Arq. Bras. Oftalmol. 2003, 66, 431–435. [Google Scholar] [CrossRef]
- Taibbi, G.; Cromwell, R.L.; Zanello, S.B.; Yarbough, P.O.; Ploutz-Snyder, R.J.; Godley, B.F.; Vizzeri, G. Ophthalmological Evaluation of Integrated Resistance and Aerobic Training During 70-Day Bed Rest. Aerosp. Med. Hum. Perform. 2017, 88, 633–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwart, S.R.; Davis-Street, J.E.; Paddon-Jones, D.; Ferrando, A.A.; Wolfe, R.R.; Smith, S.M. Amino Acid Supplementation Alters Bone Metabolism during Simulated Weightlessness. J. Appl. Physiol. 2005, 99, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Newborg, B. Pseudotumor Cerebri Treated by Rice Reduction Diet. Arch. Intern. Med. 1974, 133, 802–807. [Google Scholar] [CrossRef]
- Mader, T.H.; Gibson, C.R.; Pass, A.F.; Kramer, L.A.; Lee, A.G.; Fogarty, J.; Tarver, W.J.; Dervay, J.P.; Hamilton, D.R.; Sargsyan, A.; et al. Optic Disc Edema, Globe Flattening, Choroidal Folds, and Hyperopic Shifts Observed in Astronauts after Long-Duration Space Flight. Ophthalmology 2011, 118, 2058–2069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blottner, D.; Bosutti, A.; Degens, H.; Schiffl, G.; Gutsmann, M.; Buehlmeier, J.; Rittweger, J.; Ganse, B.; Heer, M.; Salanova, M. Whey Protein plus Bicarbonate Supplement Has Little Effects on Structural Atrophy and Proteolysis Marker Immunopatterns in Skeletal Muscle Disuse during 21 Days of Bed Rest. J. Musculoskelet. Neuronal Interact. 2014, 14, 432–444. [Google Scholar]
- Bosutti, A.; Salanova, M.; Blottner, D.; Buehlmeier, J.; Mulder, E.; Rittweger, J.; Yap, M.H.; Ganse, B.; Degens, H. Whey Protein with Potassium Bicarbonate Supplement Attenuates the Reduction in Muscle Oxidative Capacity during 19 Days of Bed Rest. J. Appl. Physiol. 2016, 121, 838–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spaeth, G.L. Potassium, Acetazolamide, and Intraocular Pressure. Arch. Ophthalmol. 1967, 78, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.I.; Streeten, D.H. Idiopathic Intracranial Hypertension and Orthostatic Edema May Share a Common Pathogenesis. Neurology 1998, 50, 1099–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.G.; Tarver, W.J.; Mader, T.H.; Gibson, C.R.; Hart, S.F.; Otto, C.A. Neuro-Ophthalmology of Space Flight. J. Neuroophthalmol. 2016, 36, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Mader, T.H.; Gibson, C.R.; Pass, A.F.; Lee, A.G.; Killer, H.E.; Hansen, H.-C.; Dervay, J.P.; Barratt, M.R.; Tarver, W.J.; Sargsyan, A.E.; et al. Optic Disc Edema in an Astronaut after Repeat Long-Duration Space Flight. J. Neuroophthalmol. 2013, 33, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Vaghefi, E.; Shon, C.; Reading, S.; Sutherland, T.; Borges, V.; Phillips, G.; Niederer, R.L.; Danesh-Meyer, H. Intraocular Pressure Fluctuation during Resistance Exercise. BMJ Open Ophthalmol. 2021, 6, e000723. [Google Scholar] [CrossRef]
- Patel, N.; Pass, A.; Mason, S.; Gibson, C.R.; Otto, C. Optical Coherence Tomography Analysis of the Optic Nerve Head and Surrounding Structures in Long-Duration International Space Station Astronauts. JAMA Ophthalmol. 2018, 136, 193–200. [Google Scholar] [CrossRef]
- Laurie, S.S.; Macias, B.R.; Dunn, J.T.; Young, M.; Stern, C.; Lee, S.M.C.; Stenger, M.B. Optic Disc Edema after 30 Days of Strict Head-down Tilt Bed Rest. Ophthalmology 2019, 126, 467–468. [Google Scholar] [CrossRef] [PubMed]
- Laurie, S.S.; Lee, S.M.C.; Macias, B.R.; Patel, N.; Stern, C.; Young, M.; Stenger, M.B. Optic Disc Edema and Choroidal Engorgement in Astronauts During Spaceflight and Individuals Exposed to Bed Rest. JAMA Ophthalmol. 2020, 138, 165. [Google Scholar] [CrossRef] [PubMed]
- Bessler, P.; Klee, S.; Kellner, U.; Haueisen, J. Silent Substitution Stimulation of S-Cone Pathway and L- and M-Cone Pathway in Glaucoma. Investig. Ophthalmol. Vis. Sci. 2010, 51, 319–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rieger, S.; Klee, S.; Baumgarten, D. Experimental Characterization and Correlation of Mayer Waves in Retinal Vessel Diameter and Arterial Blood Pressure. Front. Physiol. 2018, 9, 892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louwies, T.; Jaki Mekjavic, P.; Cox, B.; Eiken, O.; Mekjavic, I.B.; Kounalakis, S.; De Boever, P. Separate and Combined Effects of Hypoxia and Horizontal Bed Rest on Retinal Blood Vessel Diameters. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4927–4932. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| CON | RVE | NeX | ANOVA Table Condition, Time, Condition × Time | ||||
|---|---|---|---|---|---|---|---|
| BDC | R | BDC | R | BDC | R | ||
| Average (µm) | 101.4 ± 9.5 | 101.1 ± 8.2 | 100.0 ± 8.9 | 101.4 ± 7.6 | 100.7 ± 8.4 | 101.8 ± 8.6 | p = 0.20, p = 0.18, p = 0.10 |
| (93.5–109.3) | (94.3–107.9) | (92.6–107.5) | (95.0–107.7) | (93.7–107.8) | (94.6–109.0) | ||
| Superior (µm) | 125.5 ± 15.8 | 126.1 ± 15.1 | 124.1 ± 15.3 | 125.1 ± 12.6 | 125.3 ± 13.9 | 126.5 ± 14.5 | p = 0.24, p = 0.25, p = 0.86 |
| (112.3–138.7) | (113.5–138.7) | (111.3–136.8) | (114.6–135.6) | (113.7–136.9) | (114.3–138.6) | ||
| Nasal (µm) | 77.9 ± 13.8 | 76.8 ± 12.6 | 76.4 ± 13.8 | 77.5 ± 12.6 | 75.2 ± 12.8 | 77.1 ± 13.5 | p = 0.33, p = 0.35, p = 0.06 |
| (66.4–89.4) | (66.2–87.3) | (64.9–88.0) | (67.0–88.0) | (64.5–85.9) | (65.7–88.4) | ||
| Inferior (µm) | 131.1 ± 16.1 | 130.8 ± 14.6 | 129.3 ± 16.5 | 131.4 ± 16.3 | 130.2 ± 16.8 | 130.7 ± 16.7 | p = 0.63, p = 0.18, p = 0.16 |
| (117.6–144.5) | (118.6–142.9) | (115.5–143.2) | (117.8–145.1) | (116.2–144.2) | (116.7–144.6) | ||
| Temporal (µm) | 71.1 ± 8.1 | 70.8 ± 8.9 | 70.3 ± 8.6 | 71.4 ± 9.8 | 72.1 ± 8.3 | 73.1 ± 9.7 | p = 0.04, p = 0.37, p = 0.27 |
| (64.3–77.9) | (63.4–78.3) | (63.1–77.4) | (63.2–79.5) | (65.2–79.1) | (65.0–81.2) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kermorgant, M.; Hammoud, S.; Mahieu, L.; Geeraerts, T.; Beck, A.; Bareille, M.-P.; Soler, V.; Pavy-Le Traon, A.; Quintyn, J.-C. Effects of Resistance Exercise with or without Whey Protein Supplementation on Ocular Changes after a 21-Day Head-Down Bed Rest. Life 2021, 11, 741. https://doi.org/10.3390/life11080741
Kermorgant M, Hammoud S, Mahieu L, Geeraerts T, Beck A, Bareille M-P, Soler V, Pavy-Le Traon A, Quintyn J-C. Effects of Resistance Exercise with or without Whey Protein Supplementation on Ocular Changes after a 21-Day Head-Down Bed Rest. Life. 2021; 11(8):741. https://doi.org/10.3390/life11080741
Chicago/Turabian StyleKermorgant, Marc, Sirine Hammoud, Laurence Mahieu, Thomas Geeraerts, Arnaud Beck, Marie-Pierre Bareille, Vincent Soler, Anne Pavy-Le Traon, and Jean-Claude Quintyn. 2021. "Effects of Resistance Exercise with or without Whey Protein Supplementation on Ocular Changes after a 21-Day Head-Down Bed Rest" Life 11, no. 8: 741. https://doi.org/10.3390/life11080741