
Early Hypocalcemia in Severe Trauma: An Independent Risk Factor for Coagulopathy and Massive Transfusion
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Data
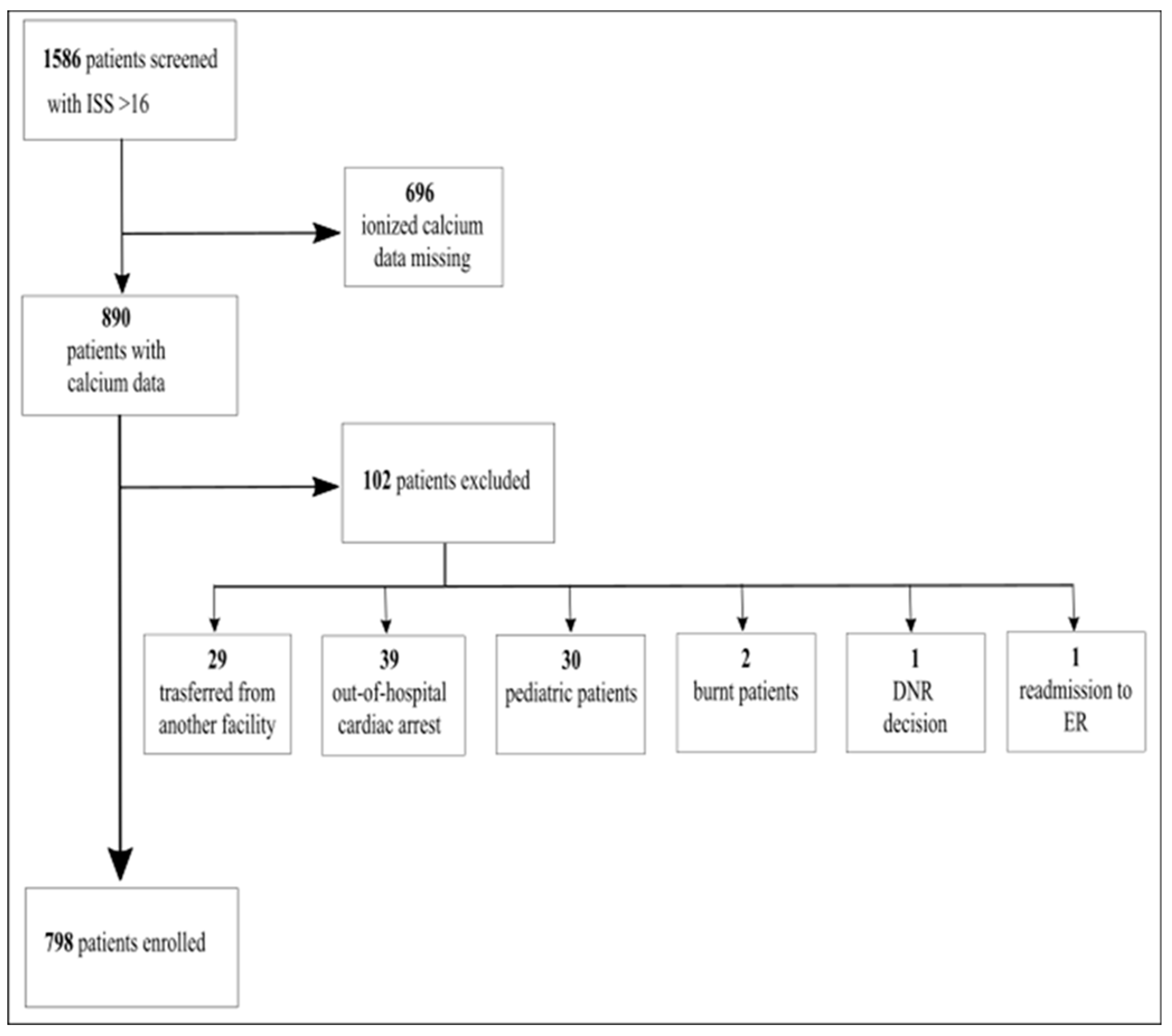
2.3. Sample
2.4. Definitions
2.5. Statistical Analysis
2.6. Endpoints
2.7. Statistical Analysis
3. Results
4. Discussion
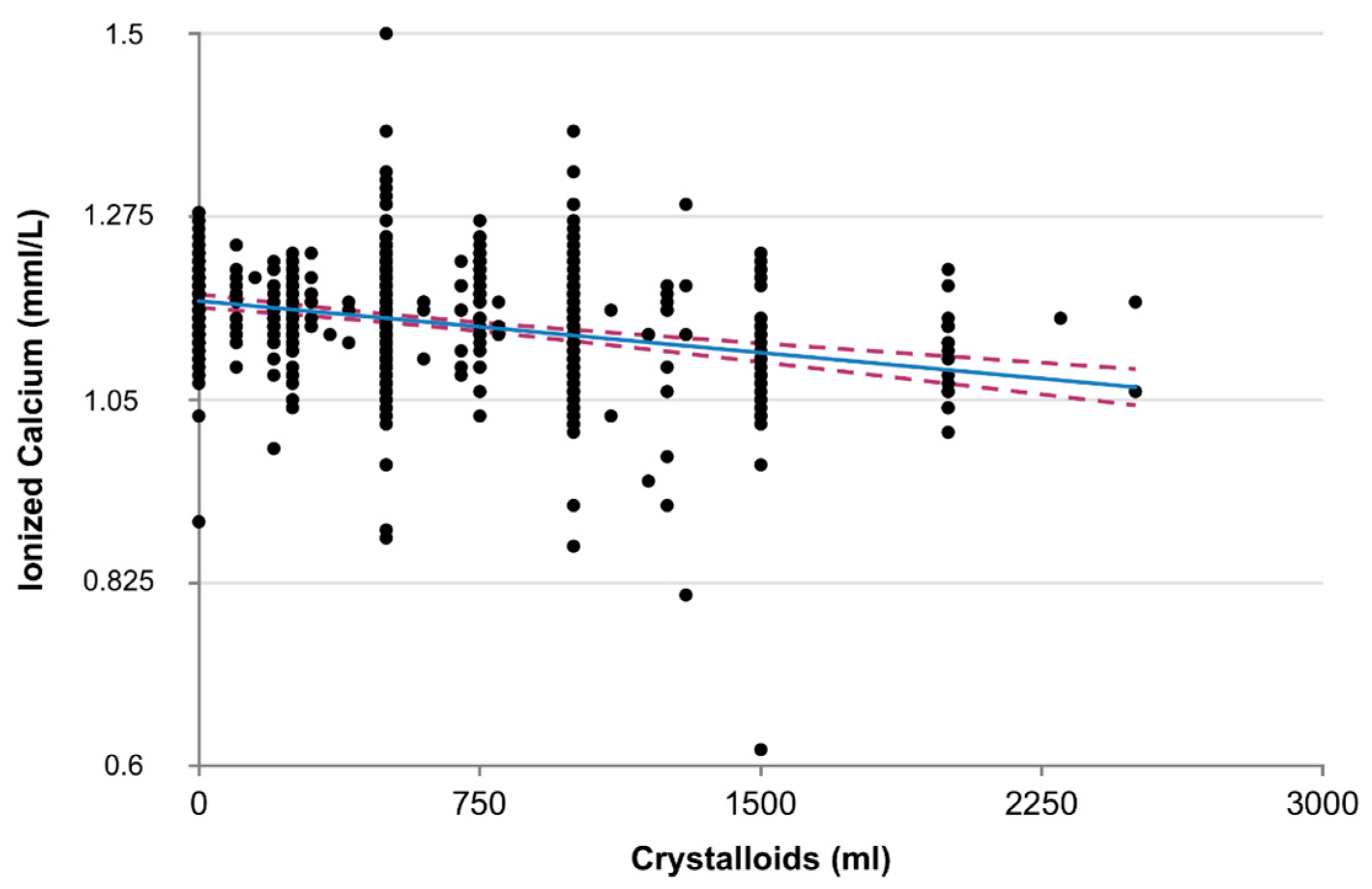
4.1. Crystalloids and Colloids Infusions
4.2. Alcohol Intake
4.3. Crush Injuries
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Magnotti, L.J.; Bradburn, E.H.; Webb, D.L.; Berry, S.D.; Fischer, P.E.; Zarzaur, B.L.; Schroeppel, T.J.; Fabian, T.C.; Croce, M.A. Admission ionized calcium levels predict the need for multiple transfusions: A prospective study of 591 critically ill trauma patients. J. Trauma 2011, 70, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Vivien, B.; Langeron, O.; Morell, E.; Devilliers, C.; Carli, P.A.; Coriat, P.; Riou, B. Early hypocalcemia in severe trauma. Crit. Care Med. 2005, 33, 1946–1952. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, K.; Lamberg-Allardt, C.; Tunninen, R.; Karonen, S.-L.; Tähtelä, R.; Ylikahri, R.; Välimäki, M. Transient hypoparathyroidism during acute alcohol intoxication. N. Engl. J. Med. 1991, 324, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Molina, P.E.; Sulzer, J.K.; Whitaker, A.M. Alcohol abuse and the injured host: Dysregulation of counterregulatory mechanisms review. Shock 2013, 39, 240–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odeh, M. The role of reperfusion-induced injury in the pathogenesis of the crush syndrome. N. Engl. J. Med. 1991, 324, 1417–1422. [Google Scholar] [CrossRef] [PubMed]
- James, M.F.; Roche, A.M. Dose-response relationship between plasma ionized calcium concentration and thrombelastography. J. Cardiothorac. Vasc. Anesth. 2004, 18, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Wray, J.P.; Bridwell, R.E.; Schauer, S.G.; Shackelford, S.A.; Bebarta, V.S.; Wright, F.L.; Bynum, J.; Long, B. The diamond of death: Hypocalcemia in trauma and resuscitation. Am. J. Emerg. Med. 2021, 41, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.M.; Leonard, A.D. Concentration-dependent effect of hypocalcaemia on mortality of patients with critical bleeding requiring massive transfusion: A cohort study. Anaesth. Intensive Care 2011, 39, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peltan, I.D.; Vusse, L.K.V.; Maier, R.V.; Watkins, T.R. An international normalized ratio-based definition of acute traumatic coagulopathy is associated with mortality, venous thromboembolism, and multiple organ failure after injury. Crit. Care Med. 2015, 43, 1429–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, S.P.; O’Neill, B.; Haddon, W.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Cherry, R.A.; Bradburn, E.; Carney, D.E.; Shaffer, M.L.; Gabbay, R.A.; Cooney, R.N. Do early ionized calcium levels really matter in trauma patients. J. Trauma 2006, 61, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Vasudeva, M.; Mathew, J.K.; Fitzgerald, M.C.; Cheung, Z.; Mitra, B. Hypocalcaemia and traumatic coagulopathy: An observational analysis. Vox Sang. 2020, 115, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Igarashi, M.; Kameue, T.; Nanzaki, S. Ionized hypocalcemia during out-of-hospital cardiac arrest and cardiopulmonary resuscitation is not due to binding by lactate. Intensive Care Med. 1997, 23, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Brooke, M.; Yeung, L.; Miraflor, E.; Garcia, A.; Victorino, G.P. Lactate predicts massive transfusion in hemodynamically normal patients. J. Surg. Res. 2016, 204, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Kronstedt, S.; Roberts, N.; Ditzel, R.; Elder, J.; Steen, A.; Thompson, K.; Anderson, J.; Siegler, J. Hypocalcemia as a predictor of mortality and transfusion. A scoping review of hypocalcemia in trauma and hemostatic resuscitation. Transfusion 2022, 62, S158–S166. [Google Scholar] [CrossRef] [PubMed]
- MacKay, E.J.; Stubna, M.D.; Holena, D.N.; Reilly, P.M.; Seamon, M.J.; Smith, B.P.; Kaplan, L.J.; Cannon, J.W. Abnormal Calcium Levels During Trauma Resuscitation Are Associated with Increased Mortality, Increased Blood Product Use, and Greater Hospital Resource Consumption: A Pilot Investigation. Anesth. Dig. 2017, 125, 895–901. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Normocalcemia n = 669 | Hypocalcemia n = 129 | Total n = 798 | |
|---|---|---|---|
| Characteristics | |||
| Age, yrs, mean +/− SD | 47 ± 20 | 46 ± 20 | 47 ± 20 |
| Male, n (%) | 502 (75) | 91 (71) | 593 (74) |
| Female, n (%) | 167 (25) | 37 (29) | 204 (26) |
| Blunt trauma, n (%) | 669 (100) | 128 (100) | 797 (100) |
| Penetrating trauma, n (%) | 0 (0) | 0 (0) | 0 (0) |
| Crush trauma, n (%) | 8 (1) | 0 (0) * | 8 (1) |
| Isolated Head or Spine trauma, n (%) | 152 (23) | 22 (17) | 174 (22) |
| Alcohol intake, n (%) | 62 (15) n = 409 | 22 (27) ** n= 80 | 87 (18) n = 489 |
| Anticoagulant/ antiplatelet use, n(%) | 13 (2) n = 625 | 1 (1) n = 120 | 14 (2) n = 745 |
| ISS, median (95% CI) | 26 (20–33) | 38 (28–50) * | 26 (21–36) |
| Prehospital phase | |||
| SAP, mmHg, mean ± SD | 127 ± 29 n = 661 | 105 ± 36 * n = 122 | 123 ± 31 n = 783 |
| HR, beats/min, mean ± SD | 92 ± 25 n = 665 | 100 ± 29 * n = 127 | 93 ± 26 n = 792 |
| SI, mean ± SD | 0.8 ± 0.3 n = 661 | 1.1 ± 0.6 * n = 122 | 0.8 ± 0.4 n = 783 |
| Glasgow Coma Scale, median (95%CI) | 15 (12–15) n = 664 | 13 (6–15) * | 15 (11–15) n = 792 |
| Cristalloids, mL, mean ± SD | 710 ± 456 n = 204 | 985 ± 509 * n = 56 | 578 ± 450 |
| Colloids, mL, mean ± SD | 7 ± 66 n = 662 | 47 ± 156 * n = 126 | 13 ± 88 n = 788 |
| Trauma center admission | |||
| Hospital SAP, mmHg, mean ± SD | 133 ± 28 n = 668 | 114 ± 29 * n = 124 | 130 ± 29 n = 792 |
| Hospital HR, beats/min, mean ± SD | 90 ± 23 | 103 ± 26 * n = 125 | 92 ± 24 |
| Prehospital time, mins, mean ± SD | 71 ± 23 n = 129 | 77 ± 24 n = 21 | 72 ± 23 n = 150 |
| Outcome | |||
| Massive tansfusion, n (%) | 22 (3.3) | 33 (25.8) * | 55 (6.9) |
| Multiple transfusions, n (%) | 83 (12.4) | 66 (51.6) * | 149 (18.7) |
| pRBC, units, mean ± SD | 1.5 ± 3.3 | 7.5 ± 9.2* | 2.5 ± 5.4 |
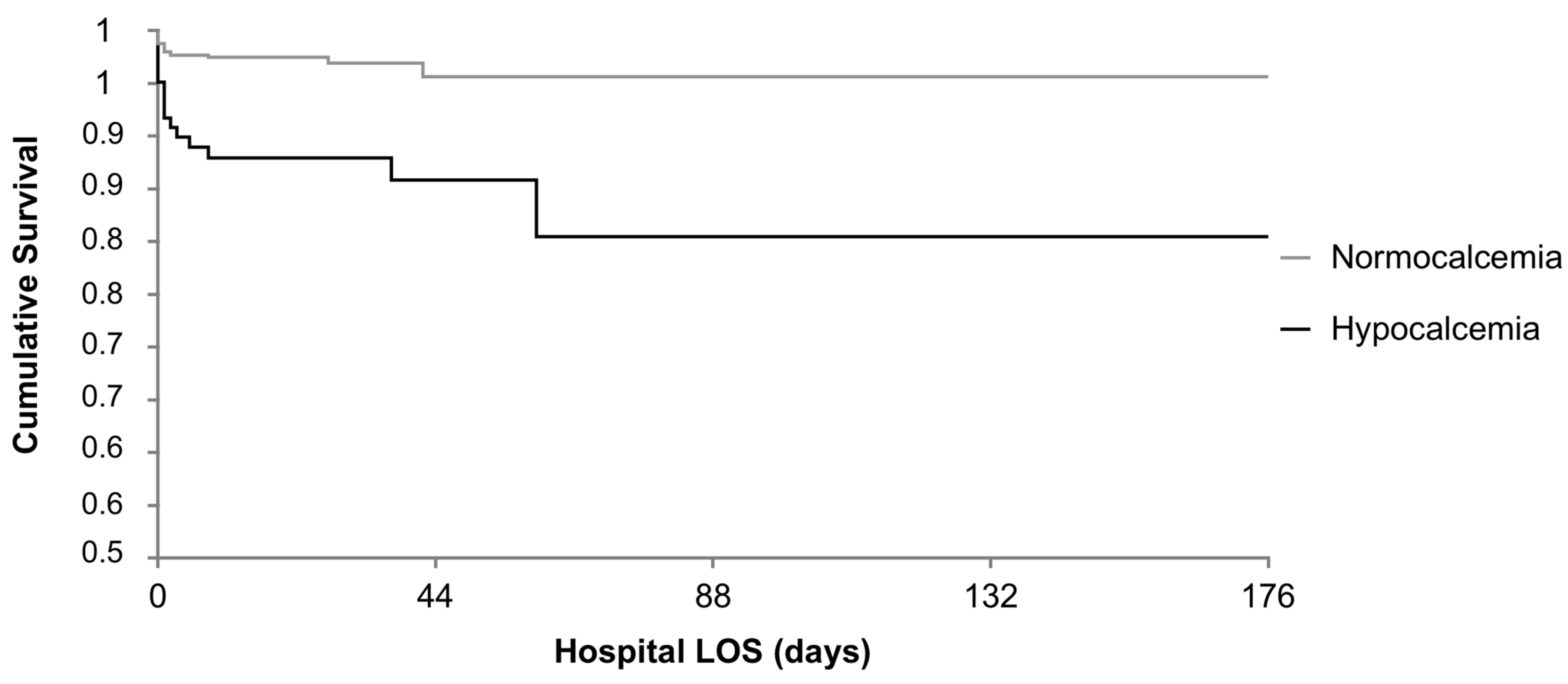
| Observed death, n (%) | 18 (2.7) n = 659 | 16 (12.9) * n = 124 | 34 (4.3) n = 783 |
| Normocalcemia n = 669 | Hypocalcemia n = 129 | |
|---|---|---|
| Ionized calcium, mmol/L, mean ± SD | 1.17 ± 0.05 n = 667 | 1.03 ± 0.09 * |
| Prothrombin time INR, mean ± SD | 1.12 ± 0.21 n = 576 | 1.41 ± 0.4 * n = 103 |
| aPTT ratio, mean ± SD | 0.88 ± 0.22 n = 573 | 1.20 ± 0.63 * n = 102 |
| Base Excess, mmol/L, mean ± SD | −3.5 ± 3.9 n = 621 | −8.6 ± 9.8 * n = 125 |
| Lactates, mmol/L, mean ± SD | 2.6 ± 1.6 n = 663 | 4.3 ± 3.3 * n = 127 |
| OR (95% CI) | p-Value | |
|---|---|---|
| ISS | 1.07 (1.04–1.10) | <0.0001 |
| Lactates, mmol/L | 1.29 (1.13–1.48) | <0.001 |
| Cristalloids, mL | 1.00 (1.00–1.00) | 0.003 |
| Hypocalcemia (Ionized calcium < 1.1 mmol/L) | 2.42 (1.13–5.16) | 0.02 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Alcohol intake | 2.32 (1.13–4.74) | 0.02 |
| INR > 1.5 | 9.47 (2.89–31.0) | 0.0002 |
| Cristalloids, mL | 1.00 (1.00–1.00) | 0.01 |
| ISS | 1.03 (1.00–1.06) | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vettorello, M.; Altomare, M.; Spota, A.; Cioffi, S.P.B.; Rossmann, M.; Mingoli, A.; Chiara, O.; Cimbanassi, S. Early Hypocalcemia in Severe Trauma: An Independent Risk Factor for Coagulopathy and Massive Transfusion. J. Pers. Med. 2023, 13, 63. https://doi.org/10.3390/jpm13010063
Vettorello M, Altomare M, Spota A, Cioffi SPB, Rossmann M, Mingoli A, Chiara O, Cimbanassi S. Early Hypocalcemia in Severe Trauma: An Independent Risk Factor for Coagulopathy and Massive Transfusion. Journal of Personalized Medicine. 2023; 13(1):63. https://doi.org/10.3390/jpm13010063
Chicago/Turabian StyleVettorello, Marco, Michele Altomare, Andrea Spota, Stefano Piero Bernardo Cioffi, Marta Rossmann, Andrea Mingoli, Osvaldo Chiara, and Stefania Cimbanassi. 2023. "Early Hypocalcemia in Severe Trauma: An Independent Risk Factor for Coagulopathy and Massive Transfusion" Journal of Personalized Medicine 13, no. 1: 63. https://doi.org/10.3390/jpm13010063