
A Comparative Analysis of Anticardiolipin, Anti-Β2-Glycoprotein-1, and Lupus Anticoagulants in Saudi Women with Recurrent Spontaneous Abortions

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Data Collection
2.3. Data Analysis
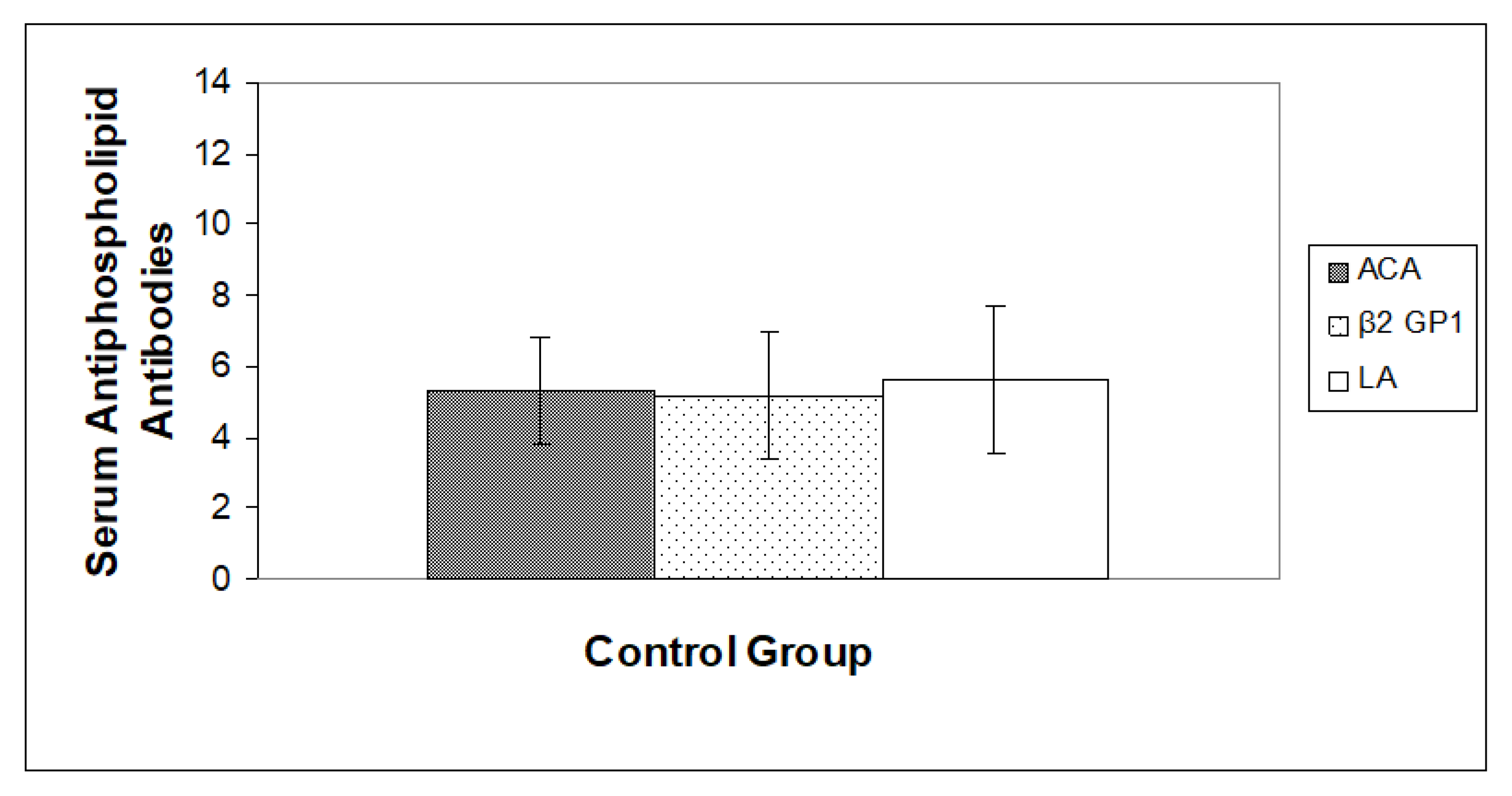
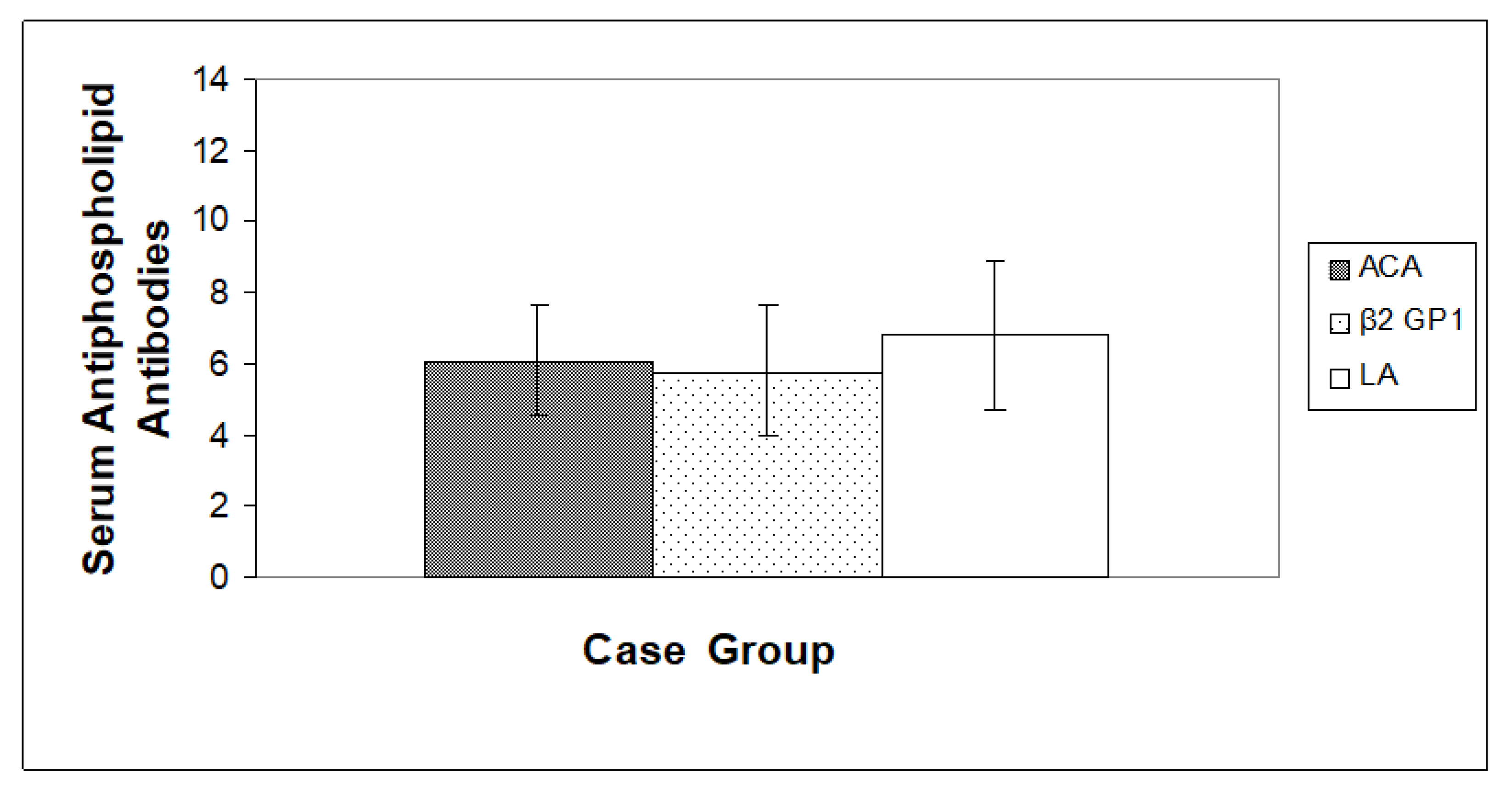
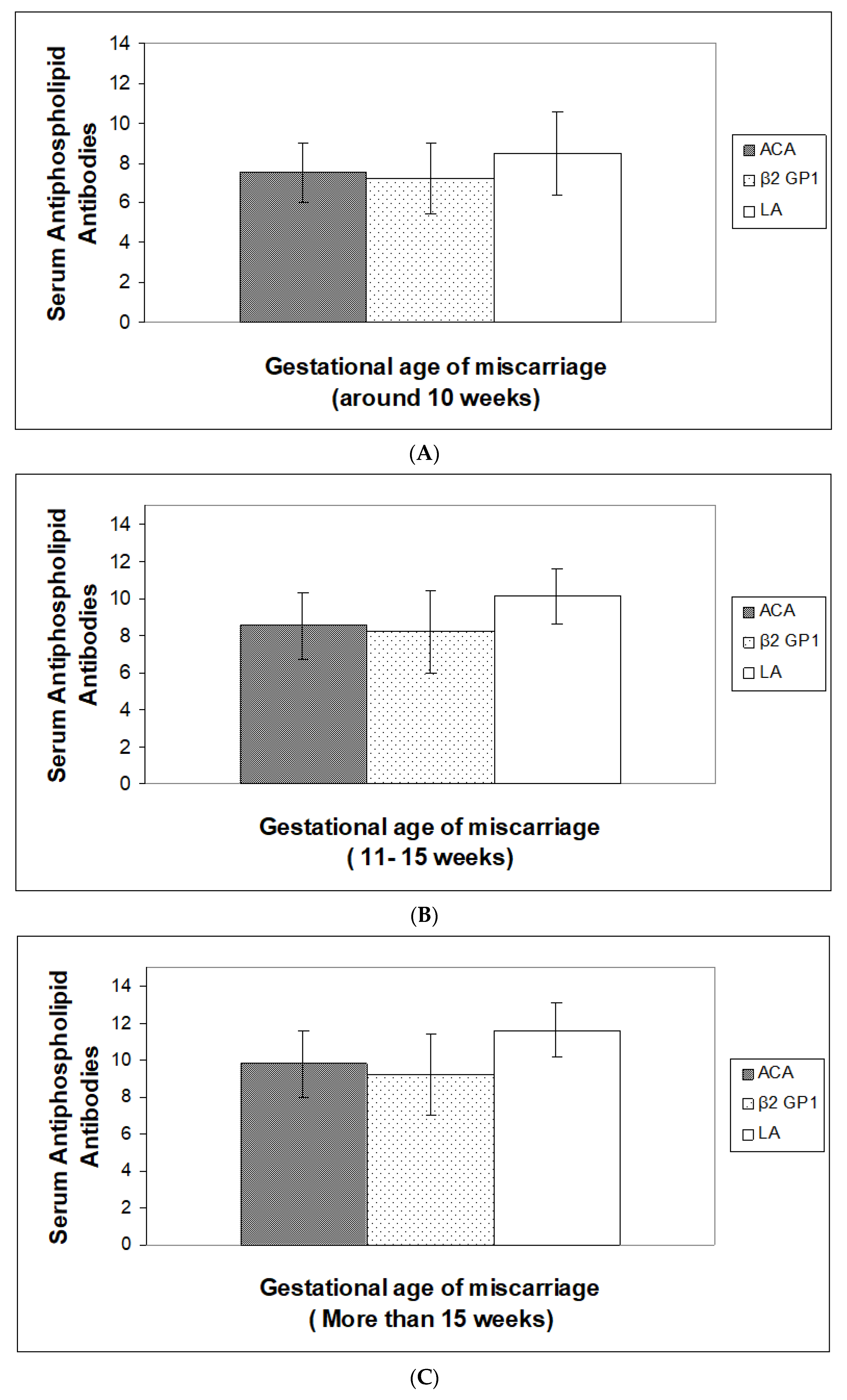
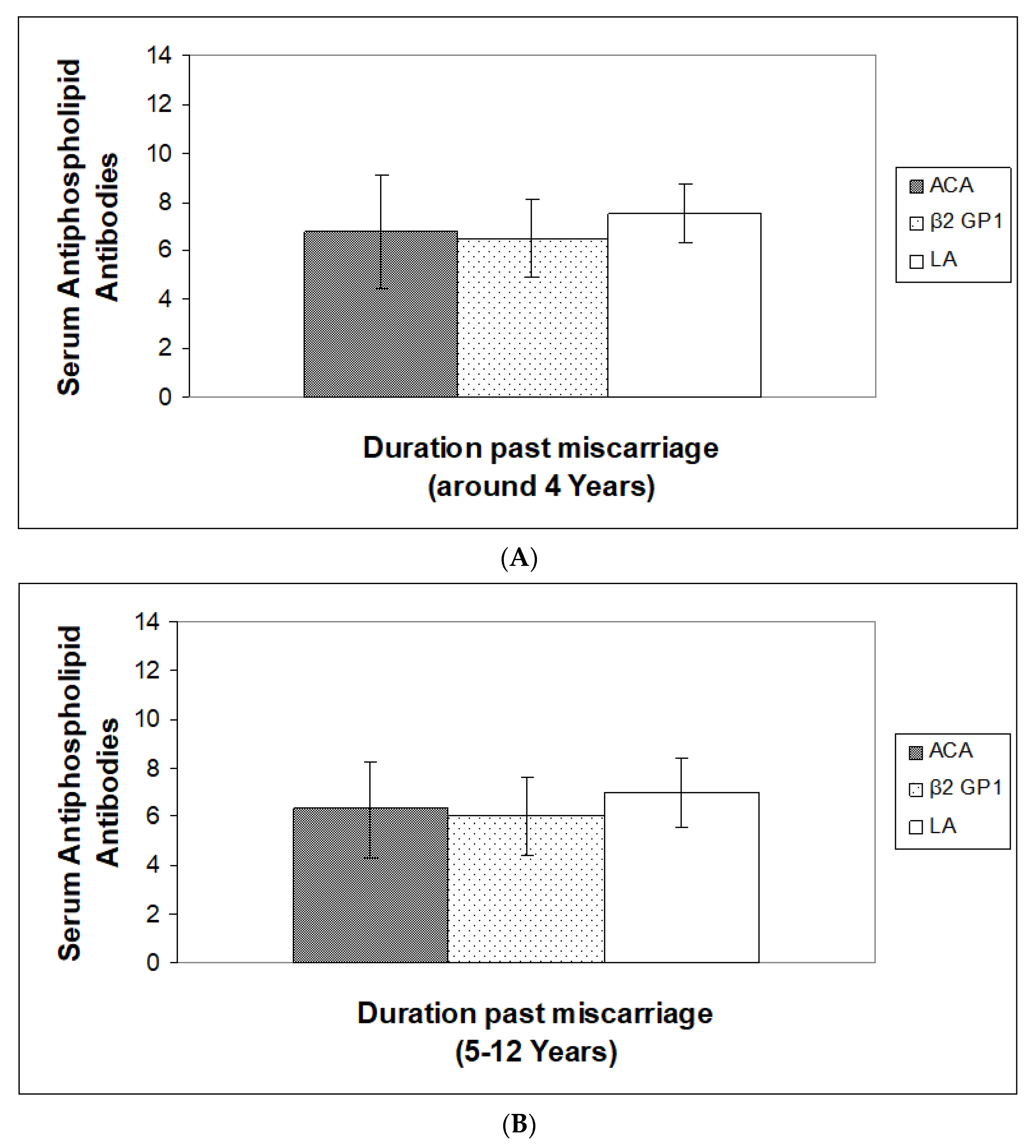
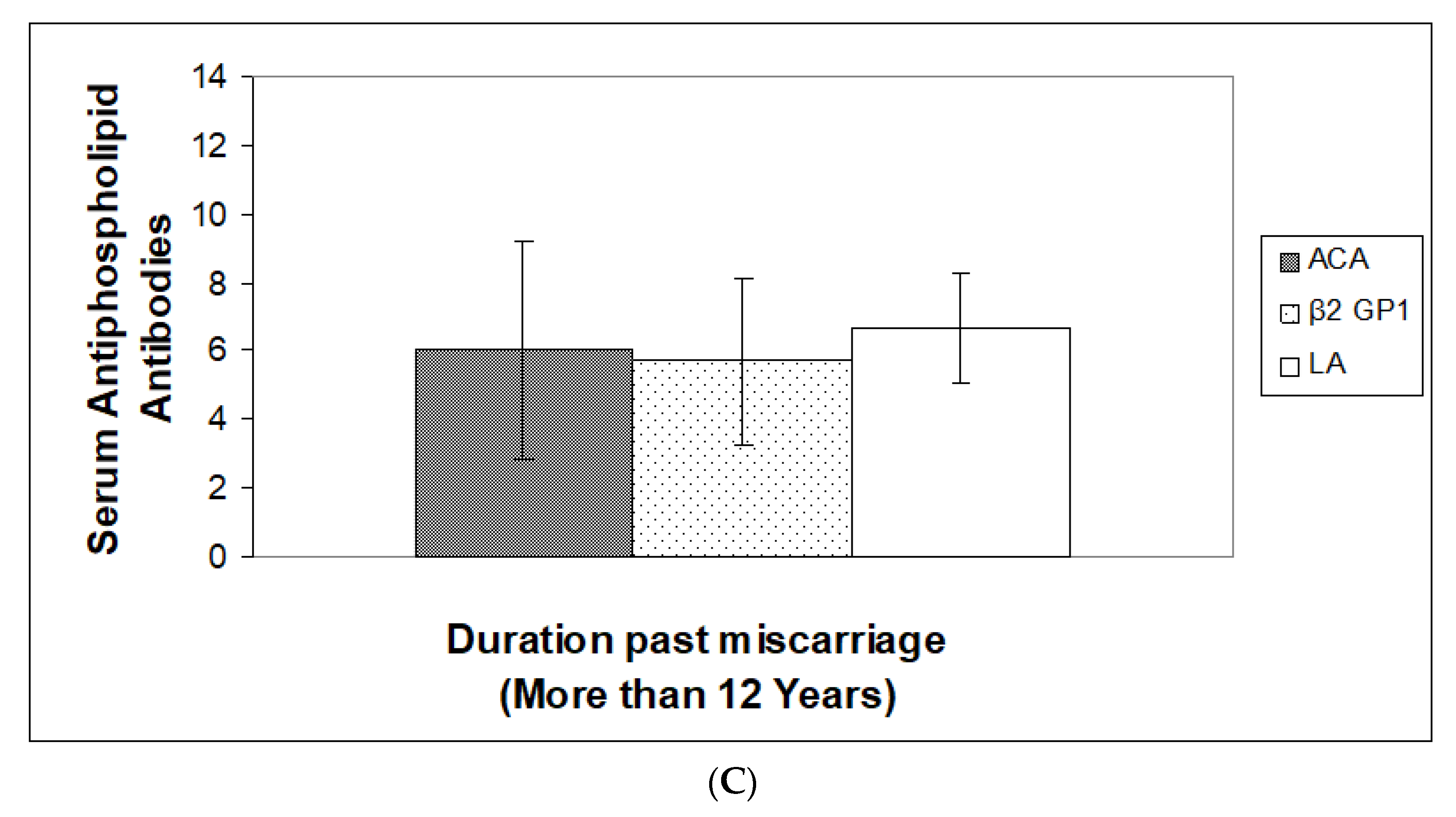
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, j.; Chen, D.; Duan, X.; Li, L.; Tang, Y.; Peng, B. The association between antiphospholipid antibodies and late fetal loss: A systematic review and meta-analysis. Acta. Obstet. Gynecol. Scand. 2019, 98, 1523–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendell, A.W.; Ghavari, A.E.; Koike, T.; Lockshin, M.D.; Branch, D.W.; Piette, J.C.; Brey, R.; Derksen, R.; Harris, E.N.; Hughes, G.R.V.; et al. International consensus statement on preliminary classification for definitive antiphospholipid syndrome. Arthritis Rheum. 1999, 42, 1309–1311. [Google Scholar]
- De Godoy, J.M.; de Godoy, M.F.; Braile, D.M.; Torres, C.A. Prevalence of anticardiolipin antibodies in peripheral arterial thrombosis. Angiology 2000, 51, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Samaritan, L.R.; Gharavi, A.E.; Soberano, C.; Levy, R.A.; Lockshin, M.D. Phospholipid binding of antiphospholipid antibodies and placental anticoagulant protein. J. Clin. Immunol. 1992, 12, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simone, D.I.; Meroni, P.L.; de Papa, N.; Raschi, E.; Caliandro, N.; De Carolis, S.; Khamashta, M.A.; Atsumi, T.; Hughes, G.R.V.; Balestrieri, G.; et al. Antiphospholipid antibodies affect trophoblast gonadotropin secretion and invasiveness by binding directly and through adhered beta2-glycoprotein I. Arthritis Rheum. 2000, 43, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Bu, C.; Zhang, C.; Li, Z.; Gao, L.; Xie, Z.; Cai, G. Autoantibodies to plasminogen and tissue plasminogen activator in women with recurrent pregnancy loss. Clin. Exp. Immunol. 2007, 149, 31–39. [Google Scholar] [CrossRef]
- Bakimer, R.; Fishman, P.; Blank, M.; Sredni, B.; Djaldetti, M.; Shoenfeld, Y. Induction of primary antiphospholipid syndrome in mice by immunization with a human monoclonal anticardiolipin antibody. J. Clin. Investig. 1992, 89, 15558–15563. [Google Scholar] [CrossRef] [Green Version]
- Salazar-Paramo, M.; Jara, L.J.; Ramos, A.; Barile, L.; Machado, G.; García-De, L.; Torre, I. Longitudinal study of antinuclear and anticardiolipin antibodies in pregnant women with systemic lupus erythematosus and antiphospholipid syndrome. Rheumatol. Int. 2002, 22, 142–147. [Google Scholar] [CrossRef]
- Semin, P. Catastrophic antiphospholipid syndrome and pregnancy. Semin. Perinatol. 2018, 42, 26–32. [Google Scholar]
- Radu, A.; Dudu, S.C.; Ciobanu, A.; Peltecu, G.; Iancu, G.; Botezatu, R.; Gica, N.; Panaitescu, A.M. Pregnancy Management in Women with Antiphospholidic Syndrome. Maedica 2019, 14, 148–160. [Google Scholar]
- Galli, M.; Barbui, T. Antiphospholipid antibodies and thrombosis: Strength of association. Hematol. J. 2003, 4, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Hanly, J.G. Antiphospholipid syndrome: An overview. Cmaj 2003, 168, 1675–1682. [Google Scholar] [PubMed]
- Jerrold, S.L.; Branch, W.B.; Munther, A.K. Antiohospholipid syndrome. N. Engl. J Med. 2002, 46, 752–763. [Google Scholar]
- Schousboe, I. Beta 2 glycoprotein 1: A plasma inhibitor of the contact activation of the intrinsic blood coagulation pathway. Blood 1985, 66, 1086–1091. [Google Scholar] [CrossRef] [PubMed]
- Bevers, E.M.; Galli, M.; Barbui, T.; Comfurius, P.; Zwaal, R.F. Lupus anticoagulant IgGs (LA) are not directed to phospholipids only but to a complex of lipid bound human prothrombin. Thromb. Hemost. 1991, 66, 629–632. [Google Scholar]
- Oosting, J.D.; Derksen, R.H.; Bobbink, I.W.; Hackeng, T.M.; Bouma, B.N.; de Groot, P.G. Antiphospholipid antibodies directed against a combination of phospholipids with prothrombin, protein C or protein S: An explanation for their pathologic mechanism. Blood 1993, 81, 2618–2625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alijotas-Reig, J.; Esteve-Valverde, E.; Anunciación-Llunell, A.; Marques-Soares, J.; Pardos-Gea, J.; Miró-Mur, F. Pathogenesis, Diagnosis and Management of Obstetric Antiphospholipid Syndrome: A Comprehensive Review. J. Clin. Med. 2022, 11, 675. [Google Scholar] [CrossRef] [PubMed]
- Loizou, S.; McCrea, J.D.; Rudge, A.C.; Reynolds, R.; Boyle, C.C.; Harris, E.N. Measurement of anti-cardiolipin antibodies by an enzyme-linked immunosorbent assay (ELISA): Standardization and quantitation of results. Clin Exp. Immunol. 1985, 62, 738–745. [Google Scholar]
- Harris, E.N.; Gharavi, A.E.; Patel, S.P.; Hughes, G.R. Evaluation of the anti-cardiolipin antibody test: Report of an international workshop held 4 April 1986. Clin. Exp Immunol. 1987, 68, 215–222. [Google Scholar]
- Schjetlein, R.; Sletnes, K.E.; Wisloff, F. A quantitative, semi-automated and computer-assisted test for lupus anticoagulant. Thromb. Res. 1993, 69, 239–250. [Google Scholar] [CrossRef]
- Jacobsen, E.M.; Barna-Cler, L.; Taylor, J.M.; Triplett, D.A.; Wisloff, F. The Lupus Ratio test—An interlaboratory study on the detection of Lupus anticoagulants by an APTT-based, integrated, and semi-quantitative test. Fifth International Survey of Lupus Anticoagulants–ISLA 5. Thromb. Haemost. 2000, 83, 704–708. [Google Scholar] [PubMed]
- Lockwood, C.J.; Romero, R.; Feinberg, R.F.; Clyne, L.P.; Coster, B.; Hobbins, J.C. The prevalence and biologic significance of lupus anticoagulant and anticardiolipin antibodies in a general obstetric population. Am. J. Obstet. Gynecol. 1989, 161, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Love, P.E.; Santoro, S.A. Antiphospholipid antibodies: Anticardiolipin and lupus anticoagulant in systemic lupus erythematosus (SLE) and in non-SLE disorders; prevalence and clinical. Ann. Intern. Med. 1990, 112, 682–698. [Google Scholar] [CrossRef] [PubMed]
- Infante-Rivard, C.; David, M.; Gauthier, R.; Rivard, G.E. Lupus anticoagulants, anticardiolipin antibodies, and fetal loss. A case-control study. N. Eng. J Med. 1991, 325, 1063–1066. [Google Scholar] [CrossRef] [PubMed]
- De Wolf, F.; Carreras, L.O.; Moerman, P.; Vermylen, J.; Van Assche, A.; Renaer, M. Decidual vasculopathy and extensive placental infarction in a patient with repeated thromboembolic accidents, recurrent fetal loss, and a lupus anticoagulant. Am. J. Obstet. Gynecol. 1982, 142, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Franco, C.; Walker, M.; Robertson, J.; Fitzgerald, B.; Keating, S.; McLeod, A.; Kingdom, J.C. Placental infarction and thrombophilia. Obstet. Gynecol. 2011, 117, 929–934. [Google Scholar] [CrossRef]
- Urbanus, R.T.; De Groot, P.G. Antiphospholipid antibodies—We’re not quite there yet. Blood Rev. 2011, 25, 97–106. [Google Scholar] [CrossRef]
- Velayuthaprabhu, S.; Archunan, G. Evaluation of anticardiolipin antibodies and antiphosphatidylserine antibodies in women with recurrent abortion. Indian. J. Med. Sci. 2005, 59, 347–352. [Google Scholar]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.; Groot, P.G.D.E.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef]
- Sheth, J.J.; Sheth, F.J. Study of anticardiolipin antibodies in repeated abortions-an institutional experience. Indian J. Pathol. Microbiol. 2001, 44, 117–121. [Google Scholar]
- Megan, R.W.; Ann, E.C.; Corey, D.A.; Leslie, S. Severe thrombotic complications secondary to antiphospholipid syndrome and undiagnosed systemic lupus erythematosus. Cmaj 2022, 19, E1243–E1247. [Google Scholar]
- Nicola, B.; Elio, T.; Danito, V.; Marilina, T.; Renato, T. Prevalence and clinical correlation of antiphospholipid-binding protein antibodies in anticardiolipin- negative patients with systemic lupus erythematosus and women with unexplained recurrent miscarriages. Arch. Pathol. Lab. Med. 2005, 129, 61–68. [Google Scholar]
- Arnold, J.; Holems, Z.; Pickering, W.; Farmer, C.; Regan, L.; Cohen, H. Anti-beta, glycoprotein 1 and antiannexin V antibodies in women with recurrent miscarriage. Br. J. Haematol. 2001, 113, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Nalli, C.; Lini, D.; Andreoli, L.; Crisafulli, F.; Fredi, M.; Lazzaroni, M.G.; Bitsadze, V.; Calligaro, A.; Canti, V.; Caporali, R.; et al. Low Preconception Complement Levels Are Associated with Adverse Pregnancy Outcomes in a Multicenter Study of 260 Pregnancies in 197 Women with Antiphospholipid Syndrome or Carriers of Antiphospholipid Antibodies. Biomedicines 2021, 9, 671. [Google Scholar] [CrossRef] [PubMed]
- Branch, D.W.; Silver, R.; Pierangeli, S.; van Leeuwen, I.; Harris, E.N. Antiphospholipid antibodies other than lupus anticoagulant and anticardiolipin antibodies in women with recurrent pregnancy loss, fertile controls and antiphospholipid syndrome. Thromb. Haemost. 1997, 77, 934–937. [Google Scholar]
- Ani, M.; Michelle, P.; Laurence, S.M. Lupus anticoagulant, disease activity and low complement in the first trimester are predictive of pregnancy loss. Lupus Sci. Med. 2015, 2, e000095. [Google Scholar]
- Gezer, S. Anti phospholipid syndrome. Rusts Univ. Med. J. 2003, 49, 696–741. [Google Scholar]
- Arreola-Diaz, R.; Majluf-Cruz, A.; Sanchez-Torres, L.E.; J Hernandez-Juarez, J. The Pathophysiology of the Antiphospholipid Syndrome: A Perspective from the Blood Coagulation System. Clin. Appl. Thromb. Hemost. 2022, 28, 1–18. [Google Scholar] [CrossRef]
- Martin Killian, M.; Thijs, E. Risk of Thrombosis, Pregnancy Morbidity or Death in Antiphospholipid Syndrome. Front. Cardiovasc. Med. 2022, 9, 852777–852786. [Google Scholar] [CrossRef]
- Pavla, B.C.; Lud, S.; Adéla, S.; Jana, Ú.; Eva, K.; Gayane, M.; David, F.; Barbora, P.; Jana, U.; Jana, P.; et al. Determination of thrombogenicity levels of various antiphospholipid antibodies by a modified thrombin generation assay in patients with suspected antiphospholipid syndrome. Int. J. Mol Sci. 2022, 23, 8973. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Case Group | Control Group |
|---|---|---|
| Number of Patients (n) | 100 | 100 |
| Sex (female) | 100 | 100 |
| Age ± SD; years old | 30.5 ± 12.60 | 30.5 ± 12.60 |
| Race (Saudi): Caucasian/Black | 81/19 | 80/20 |
| Body Mass Index (BMI) | 28.52 ± 6.81 | 28.08 ± 6.52 |
| Thrombosis, Y/N | 88/12 | 0/100 |
| Systemic Lupus Erythematosus (SLE), Y/N | 77/23 | 26/74 |
| Diabetes, Y/N | 0/100 | 1/99 |
| Placental Abruption, Y/N | 0/100 | 2/98 |
| Placenta Previa, Y/N | 0/100 | 2/98 |
| Inherited Thrombophilia * Y/N | 2/98 | 1/99 |
| Pregnancy Loss, Y/N | 96/04 | 0/100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaikhomar, O.A.; Ali, S.T. A Comparative Analysis of Anticardiolipin, Anti-Β2-Glycoprotein-1, and Lupus Anticoagulants in Saudi Women with Recurrent Spontaneous Abortions. J. Pers. Med. 2023, 13, 2. https://doi.org/10.3390/jpm13010002
Shaikhomar OA, Ali ST. A Comparative Analysis of Anticardiolipin, Anti-Β2-Glycoprotein-1, and Lupus Anticoagulants in Saudi Women with Recurrent Spontaneous Abortions. Journal of Personalized Medicine. 2023; 13(1):2. https://doi.org/10.3390/jpm13010002
Chicago/Turabian StyleShaikhomar, Osama Abdulrahman, and Syed Tabrez Ali. 2023. "A Comparative Analysis of Anticardiolipin, Anti-Β2-Glycoprotein-1, and Lupus Anticoagulants in Saudi Women with Recurrent Spontaneous Abortions" Journal of Personalized Medicine 13, no. 1: 2. https://doi.org/10.3390/jpm13010002