


Exploring Clinical and Biological Features of Premature Births among Pregnant Women with SARS-CoV-2 Infection during the Pregnancy Period
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Ethics and Design
2.2. Inclusion and Exclusion Circumstances
2.3. Study Variables and Definitions
2.4. Statistical Analysis
3. Results
3.1. Background Analysis
3.2. Patient Outcomes
3.3. Neonatal Outcomes
3.4. Laboratory Analysis
4. Discussion
4.1. Important Findings
4.2. Study Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. Can. Med Assoc. J. 2021, 193, E540–E548. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-L.; Liu, Y.-Y.; Wu, C.-H.; Wang, C.-Y.; Wang, C.-H.; Long, C.-Y. Impact of COVID-19 on Pregnancy. Int. J. Med Sci. 2021, 18, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Timircan, M.; Bratosin, F.; Vidican, I.; Suciu, O.; Turaiche, M.; Bota, A.V.; Mitrescu, S.; Marincu, I. Coping Strategies and Health-Related Quality of Life in Pregnant Women with SARS-CoV-2 Infection. Medicina 2021, 57, 1113. [Google Scholar] [CrossRef]
- Ryean, G.A.; Purandare, N.C.; McAuliffe, F.M.; Hod, M.; Purandare, C.N. Clinical update on COVID -19 in pregnancy: A review article. J. Obstet. Gynaecol. Res. 2020, 46, 1235–1245. [Google Scholar] [CrossRef] [PubMed]
- Uta, M.; Neamtu, R.; Bernad, E.; Mocanu, A.G.; Gluhovschi, A.; Popescu, A.; Dahma, G.; Dumitru, C.; Stelea, L.; Citu, C.; et al. The Influence of Nutritional Supplementation for Iron Deficiency Anemia on Pregnancies Associated with SARS-CoV-2 Infection. Nutrients 2022, 14, 836. [Google Scholar] [CrossRef] [PubMed]
- Zaky, S.; Hosny, H.; Elassal, G.; Asem, N.; Baki, A.A.; Kamal, E.; Abdelbary, A.; Said, A.; Ibrahim, H.; Taema, K.; et al. Clinical evaluation of pregnant women with SARS-CoV2 pneumonia: A real-life study from Egypt. J. Egypt. Public Health Assoc. 2021, 96, 29. [Google Scholar] [CrossRef]
- Limaye, M.A.; Roman, A.S.; Trostle, M.E.; Venkatesh, P.; Martinez, M.L.; Brubaker, S.G.; Chervenak, J.; Wei, L.S.; Sahani, P.; Grossman, T.B.; et al. Predictors of severe and critical disease in pregnant women with SARS-CoV-2. J. Matern. Fetal Neonatal Med. 2021, 1–5. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Margan, M.-M.; Craina, M.; Neamtu, R.; Gorun, O.M.; Burlea, B.; Bratosin, F.; Rosca, O.; Grigoras, M.L.; et al. Calcium, Magnesium, and Zinc Supplementation during Pregnancy: The Additive Value of Micronutrients on Maternal Immune Response after SARS-CoV-2 Infection. Nutrients 2022, 14, 1445. [Google Scholar] [CrossRef]
- Yu, W.; Hu, X.; Cao, B. Viral Infections During Pregnancy: The Big Challenge Threatening Maternal and Fetal Health. Matern. Fetal Med. 2021, 4, 72–86. [Google Scholar] [CrossRef]
- Boeriu, E.; Borda, A.; Vulcanescu, D.D.; Sarbu, V.; Arghirescu, S.T.; Ciorica, O.; Bratosin, F.; Marincu, I.; Horhat, F.G. Diagnosis and Management of Febrile Neutropenia in Pediatric Oncology Patients—A Systematic Review. Diagnostics 2022, 12, 1800. [Google Scholar] [CrossRef]
- Auriti, C.; De Rose, D.U.; Santisi, A.; Martini, L.; Piersigilli, F.; Bersani, I.; Ronchetti, M.P.; Caforio, L. Pregnancy and Viral infections: Mechanisms of fetal damage, diagnosis and prevention of neonatal adverse outcomes from cytomegalovirus to SARS-CoV-2 and Zika virus. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166198. [Google Scholar] [CrossRef] [PubMed]
- Margan, R.; Margan, M.-M.; Fira-Mladinescu, C.; Putnoky, S.; Tuta-Sas, I.; Bagiu, R.; Popa, Z.L.; Bernad, E.; Ciuca, I.M.; Bratosin, F.; et al. Impact of Stress and Financials on Romanian Infertile Women Accessing Assisted Reproductive Treatment. Int. J. Environ. Res. Public Health 2022, 19, 3256. [Google Scholar] [CrossRef] [PubMed]
- Sathiya, R.; Rajendran, J.; Sumathi, S. COVID-19 and Preeclampsia: Overlapping Features in Pregnancy. Rambam Maimonides Med. J. 2022, 13, e0007. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, M.; Garcia-Ruiz, I.; Maiz, N.; Rodo, C.; Garcia-Manau, P.; Serrano, B.; Lopez-Martinez, R.M.; Balcells, J.; Fernandez-Hidalgo, N.; Carreras, E.; et al. Pre-eclampsia-like syndrome induced by severe COVID-19: A prospective observational study. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 1374–1380. [Google Scholar] [CrossRef]
- Wood, R.; Sinnott, C.; Goldfarb, I.; Clapp, M.; McElrath, T.; Little, S. Preterm Birth During the Coronavirus Disease 2019 (COVID-19) Pandemic in a Large Hospital System in the United States. Obstet. Gynecol. 2021, 137, 403–404. [Google Scholar] [CrossRef]
- Karasek, D.; Baer, R.J.; McLemore, M.R.; Bell, A.J.; Blebu, B.E.; Casey, J.A.; Coleman-Phox, K.; Costello, J.M.; Felder, J.N.; Flowers, E.; et al. The association of COVID-19 infection in pregnancy with preterm birth: A retrospective cohort study in California. Lancet Reg. Health 2021, 2, 100027. [Google Scholar] [CrossRef]
- Citu, C.; Neamtu, R.; Sorop, V.B.; Horhat, D.I.; Gorun, F.; Tudorache, E.; Gorun, O.M.; Boarta, A.; Tuta-Sas, I.; Citu, I.M. Assessing SARS-CoV-2 Vertical Transmission and Neonatal Complications. J Clin Med. 2021, 10, 5253. [Google Scholar] [CrossRef]
- Epelboin, S.; Labrosse, J.; De Mouzon, J.; Fauque, P.; Gervoise-Boyer, M.-J.; Levy, R.; Sermondade, N.; Hesters, L.; Bergère, M.; Devienne, C.; et al. Obstetrical outcomes and maternal morbidities associated with COVID-19 in pregnant women in France: A national retrospective cohort study. PLoS Med. 2021, 18, e1003857. [Google Scholar] [CrossRef]
- Guo, F.; Yang, X. A Comprehensive Review of the Management of Pregnant Women with COVID-19: Useful Information for Obstetricians. Infect. Drug Resist. 2021, 14, 3363–3378. [Google Scholar] [CrossRef]
- Adhikari, E.H.; Moreno, W.; Zofkie, A.C.; Macdonald, L.; McIntire, D.D.; Collins, R.R.J.; Spong, C.Y. Pregnancy Outcomes Among Women with and Without Severe Acute Respiratory Syndrome Coronavirus 2 Infection. JAMA Netw. Open 2020, 3, e2029256. [Google Scholar] [CrossRef]
- Crovetto, F.; Crispi, F.; Llurba, E.; Pascal, R.; Larroya, M.; Trilla, C.; Camacho, M.; Medina, C.; Dobaño, C.; Gomez-Roig, M.D.; et al. Impact of Severe Acute Respiratory Syndrome Coronavirus 2 Infection on Pregnancy Outcomes: A Population-based Study. Clin. Infect. Dis. 2021, 73, 1768–1775. [Google Scholar] [CrossRef] [PubMed]
- Citu, I.M.; Citu, C.; Gorun, F.; Sas, I.; Bratosin, F.; Motoc, A.; Burlea, B.; Rosca, O.; Malita, D.; Gorun, O.M. The Risk of Spontaneous Abortion Does Not Increase Following First Trimester mRNA COVID-19 Vaccination. J. Clin. Med. 2022, 11, 1698. [Google Scholar] [CrossRef] [PubMed]
- Pratama, N.R.; Wafa, I.A.; Budi, D.S.; Putra, M.; Wardhana, M.P.; Wungu, C.D.K. mRNA COVID-19 vaccines in pregnancy: A systematic review. PLoS ONE 2022, 17, e0261350. [Google Scholar] [CrossRef] [PubMed]
- Horhat, R.M.; Vlaicu, B.; Bagiu, R.; Putnoky, S.; Bagiu, I.C.; Horhat, D.I.; Szuhanek, C.; Sinescu, C.; Negrutiu, M.L.; Nica, L. A Ten-year Time Laps, Regarding Drug Consumption in the Western Part of Romania. Rev. Chim. 2018, 69, 1371–1375. [Google Scholar] [CrossRef]
- Alshehri, M.M.; Quispe, C.; Herrera-Bravo, J.; Sharifi-Rad, J.; Tutuncu, S.; Aydar, E.F.; Topkaya, C.; Mertdinc, Z.; Ozcelik, B.; Aital, M.; et al. A Review of Recent Studies on the Antioxidant and Anti-Infectious Properties of Senna Plants. Oxidative Med. Cell. Longev. 2022, 2022, 6025900. [Google Scholar] [CrossRef]
- Jianu, C.; Moleriu, R.; Stoin, D.; Cocan, I.; Bujancă, G.; Pop, G.; Lukinich-Gruia, A.T.; Muntean, D.; Rusu, L.-C.; Horhat, D.I. Antioxidant and Antibacterial Activity of Nepeta × faassenii Bergmans ex Stearn Essential Oil. Appl. Sci. 2021, 11, 442. [Google Scholar] [CrossRef]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical transmission of coronavirus disease 2019: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021, 224, 35–53.e3. [Google Scholar] [CrossRef]
- Rad, H.S.; Röhl, J.; Stylianou, N.; Allenby, M.C.; Bazaz, S.R.; Warkiani, M.E.; Guimaraes, F.S.F.; Clifton, V.L.; Kulasinghe, A. The Effects of COVID-19 on the Placenta During Pregnancy. Front. Immunol. 2021, 12, 743022, Erratum in Front Immunol. 2022, 13, 998406. [Google Scholar] [CrossRef]
- Balachandren, N.; Davies, M.C.; Hall, J.A.; Stephenson, J.M.; David, A.L.; Barrett, G.; O’Neill, H.C.; Ploubidis, G.B.; Yasmin, E.; Mavrelos, D. SARS-CoV-2 infection in the first trimester and the risk of early miscarriage: A UK population-based prospective cohort study of 3041 pregnancies conceived during the pandemic. Hum. Reprod. 2022, 37, 1126–1133. [Google Scholar] [CrossRef]
- Piekos, S.N.; Roper, R.T.; Hwang, Y.M.; Sorensen, T.; Price, N.D.; Hood, L.; Hadlock, J.J. The effect of maternal SARS-CoV-2 infection timing on birth outcomes: A retrospective multicentre cohort study. Lancet Digit. Health 2022, 4, e95–e104. [Google Scholar] [CrossRef]
- Fell, D.B.; Dimanlig-Cruz, S.; Regan, A.K.; Håberg, S.E.; Gravel, C.A.; Oakley, L.; Alton, G.D.; Török, E.; Dhinsa, T.; Shah, P.S.; et al. Risk of preterm birth, small for gestational age at birth, and stillbirth after COVID-19 vaccination during pregnancy: Population based retrospective cohort study. BMJ 2022, 378, e071416. [Google Scholar] [CrossRef] [PubMed]
- Jacoby, V.L.; Murtha, A.; Afshar, Y.; Gaw, S.L.; Asiodu, I.; Tolosa, J.; Norton, M.E.; Boscardin, W.J.; Flaherman, V. Risk of pregnancy loss before 20 weeks’ gestation in study participants with COVID-19. Am. J. Obstet. Gynecol. 2021, 225, 456–457. [Google Scholar] [CrossRef] [PubMed]
- La Marca, A.; Capuzzo, M.; Paglia, T.; Roli, L.; Trenti, T.; Nelson, S.M. Testing for SARS-CoV-2 (COVID-19): A systematic review and clinical guide to molecular and serological in-vitro diagnostic assays. Reprod. Biomed. Online 2020, 41, 483–499. [Google Scholar] [CrossRef]
- Xu, Y.; Chen, Y.; Tang, X. Guidelines for the diagnosis and treatment of coronavirus disease 2019 (COVID-19) in China. Glob. Health Med. 2020, 2, 66–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Citu, C.; Chiriac, V.D.; Citu, I.M.; Gorun, O.M.; Burlea, B.; Bratosin, F.; Popescu, D.-E.; Ratiu, A.; Buca, O.; Gorun, F. Appraisal of COVID-19 Vaccination Acceptance in the Romanian Pregnant Population. Vaccines 2022, 10, 952. [Google Scholar] [CrossRef]
- Riley, L.E. mRNA COVID-19 Vaccines in Pregnant Women. N. Engl. J. Med. 2021, 384, 2342–2343, Erratum in N. Engl. J. Med. 2021, 385, 1536. [Google Scholar] [CrossRef]
- Marincu, I.; Citu, C.; Bratosin, F.; Bogdan, I.; Timircan, M.; Gurban, C.V.; Bota, A.V.; Braescu, L.; Grigoras, M.L. Clinical Characteristics and Outcomes of COVID-19 Hospitalized Patients: A Comparison between Complete mRNA Vaccination Profile and Natural Immunity. J. Pers. Med. 2022, 12, 259. [Google Scholar] [CrossRef]
- Stephen, G.; Mgongo, M.; Hashim, T.H.; Katanga, J.; Stray-Pedersen, B.; Msuya, S.E. Anaemia in Pregnancy: Prevalence, Risk Factors, and Adverse Perinatal Outcomes in Northern Tanzania. Anemia 2018, 2018, 1846280. [Google Scholar] [CrossRef] [Green Version]
- Fallach, N.; Segal, Y.; Agassy, J.; Perez, G.; Peretz, A.; Chodick, G.; Gazit, S.; Patalon, T.; Ben Tov, A.; Goldshtein, I. Pregnancy outcomes after SARS-CoV-2 infection by trimester: A large, population-based cohort study. PLoS ONE 2022, 17, e0270893. [Google Scholar] [CrossRef]
- Ko, J.Y.; DeSisto, C.L.; Simeone, R.M.; Ellington, S.; Galang, R.R.; Oduyebo, T.; Gilboa, S.M.; Lavery, A.M.; Gundlapalli, A.V.; Shapiro-Mendoza, C.K. Adverse Pregnancy Outcomes, Maternal Complications, and Severe Illness Among US Delivery Hospitalizations with and Without a Coronavirus Disease 2019 (COVID-19) Diagnosis. Clin. Infect. Dis. 2021, 73 (Suppl. 1), S24–S31. [Google Scholar] [CrossRef]
- Chaubey, I.; Vignesh, R.; Babu, H.; Wagoner, I.; Govindaraj, S.; Velu, V. SARS-CoV-2 in Pregnant Women: Consequences of Vertical Transmission. Front. Cell Infect. Microbiol. 2021, 11, 717104. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, M.; Johnstone, E.D.; Simcox, L.E.; Myers, J.E. The impact of COVID-19 on pregnancy outcomes in a diverse cohort in England. Sci. Rep. 2022, 12, 942. [Google Scholar] [CrossRef] [PubMed]
- Brandt, J.S.; Hill, J.; Reddy, A.; Schuster, M.; Patrick, H.S.; Rosen, T.; Sauer, M.V.; Boyle, C.; Ananth, C.V. Epidemiology of coronavirus disease 2019 in pregnancy: Risk factors and associations with adverse maternal and neonatal outcomes. Am. J. Obstet. Gynecol. 2021, 224, 389.e1–389.e9. [Google Scholar] [CrossRef]
- Jering, K.S.; Claggett, B.L.; Cunningham, J.W.; Rosenthal, N.; Vardeny, O.; Greene, M.F.; Solomon, S.D. Clinical Characteristics and Outcomes of Hospitalized Women Giving Birth with and Without COVID-19. JAMA Intern. Med. 2021, 181, 714–717. [Google Scholar] [CrossRef]
- Timircan, M.; Bratosin, F.; Vidican, I.; Suciu, O.; Tirnea, L.; Avram, V.; Marincu, I. Exploring Pregnancy Outcomes Associated with SARS-CoV-2 Infection. Medicina 2021, 57, 796. [Google Scholar] [CrossRef]
- Díaz-Corvillón, P.; Mönckeberg, M.; Barros, A.; Illanes, S.E.; Soldati, A.; Nien, J.-K.; Schepeler, M.; Caradeux, J. Routine screening for SARS-CoV-2 in unselected pregnant women at delivery. PLoS ONE 2020, 15, e0239887. [Google Scholar] [CrossRef]
- Norman, M.; Navér, L.; Söderling, J.; Ahlberg, M.; Askling, H.H.; Aronsson, B.; Byström, E.; Jonsson, J.; Sengpiel, V.; Ludvigsson, J.F.; et al. Association of maternal SARS-CoV-2 infection in pregnancy with neonatal outcomes. JAMA 2021, 325, 2076–2086. [Google Scholar] [CrossRef]
- Khunti, K.; Del Prato, S.; Mathieu, C.; Kahn, S.E.; Gabbay, R.A.; Buse, J.B. COVID-19, Hyperglycemia, and New-Onset Diabetes. Diabetes Care 2021, 44, 2645–2655. [Google Scholar] [CrossRef]
- Zanardo, V.; Tortora, D.; Sandri, A.; Severino, L.; Mesirca, P.; Straface, G. COVID-19 pandemic: Impact on gestational diabetes mellitus prevalence. Diabetes Res. Clin. Pract. 2022, 183, 109149. [Google Scholar] [CrossRef]
- Jinca, C.; Petrescu, C.A.M.; Boeriu, E.; Oprisoni, A.; Balint-Gib, L.; Baica, M.; Popa, C.; Andreescu, N.; Serban, M.; Ursu, E.; et al. The impact of immunological and biomolecular investigations on the outcome of children with acute lymphoblastic leukemia—Experience of IIIrd Paediatric Clinic Timisoara. Rev. Romana Med. Lab. 2018, 26, 77–85. [Google Scholar] [CrossRef]
- Atak, Z.; Ocakoglu, S.R.; Topal, S.; Macunluoglu, A.C. Increased maternal mortality in unvaccinated SARS-CoV-2 infected pregnant patients. J. Obstet. Gynaecol. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables * | COVID-19 Prematurity Group (n = 61) | COVID-19 No Prematurity Group (n = 124) | No COVID-19 Prematurity Group (n = 243) | p-Value |
|---|---|---|---|---|
| General characteristics | ||||
| Age (years), mean ± SD | 30.1 ± 4.8 | 29.6 ± 4.6 | 28.9 ± 4.9 | 0.147 |
| Pre-pregnancy BMI, mean ± SD | 22.5 ± 2.9 | 22.7 ± 2.5 | 22.1 ± 2.8 | 0.122 |
| Previous pregnancies | 0.920 | |||
| 1 | 38 (62.3%) | 76 (61.3%) | 150 (61.7%) | |
| 2 | 14 (23.0%) | 29 (23.4%) | 63 (25.9%) | |
| ≥3 | 9 (14.8%) | 19 (15.3%) | 30 (12.3%) | |
| Number of births | 0.348 | |||
| 0 | 4 (6.6%) | 8 (6.5%) | 28 (11.5%) | |
| 1 | 41 (67.2%) | 90 (72.6%) | 155 (63.8%) | |
| ≥2 | 16 (26.2%) | 26 (21.0%) | 60 (24.7%) | |
| History of twin birth | 1 (1.6%) | 1 (0.8%) | 3 (1.2%) | 0.874 |
| Comorbidities ** | ||||
| Diabetes Mellitus | 2 (3.3%) | 5 (4.0%) | 10 (4.1%) | 0.955 |
| Asthma | 4 (6.6%) | 8 (6.5%) | 14 (5.8%) | 0.952 |
| Coagulation disorders | 2 (3.3%) | 3 (2.4%) | 7 (2.9%) | 0.940 |
| High blood pressure | 9 (11.8%) | 11 (8.9%) | 28 (11.5%) | 0.478 |
| Thyroid disorders | 1 (1.6%) | 2 (1.6%) | 5 (2.1%) | 0.946 |
| UTI | 5 (8.2%) | 10 (8.1%) | 19 (7.8%) | 0.993 |
| Depression | 6 (9.8%) | 14 (11.3%) | 23 (9.5%) | 0.858 |
| Others | 3 (4.9%) | 5 (4.0%) | 12 (4.9%) | 0.922 |
| History of pregnancy loss | 0.112 | |||
| Yes | 7 (11.5%) | 6 (4.8%) | 13 (5.3%) | |
| No | 54 (88.5%) | 118 (95.2%) | 230 (94.7%) | |
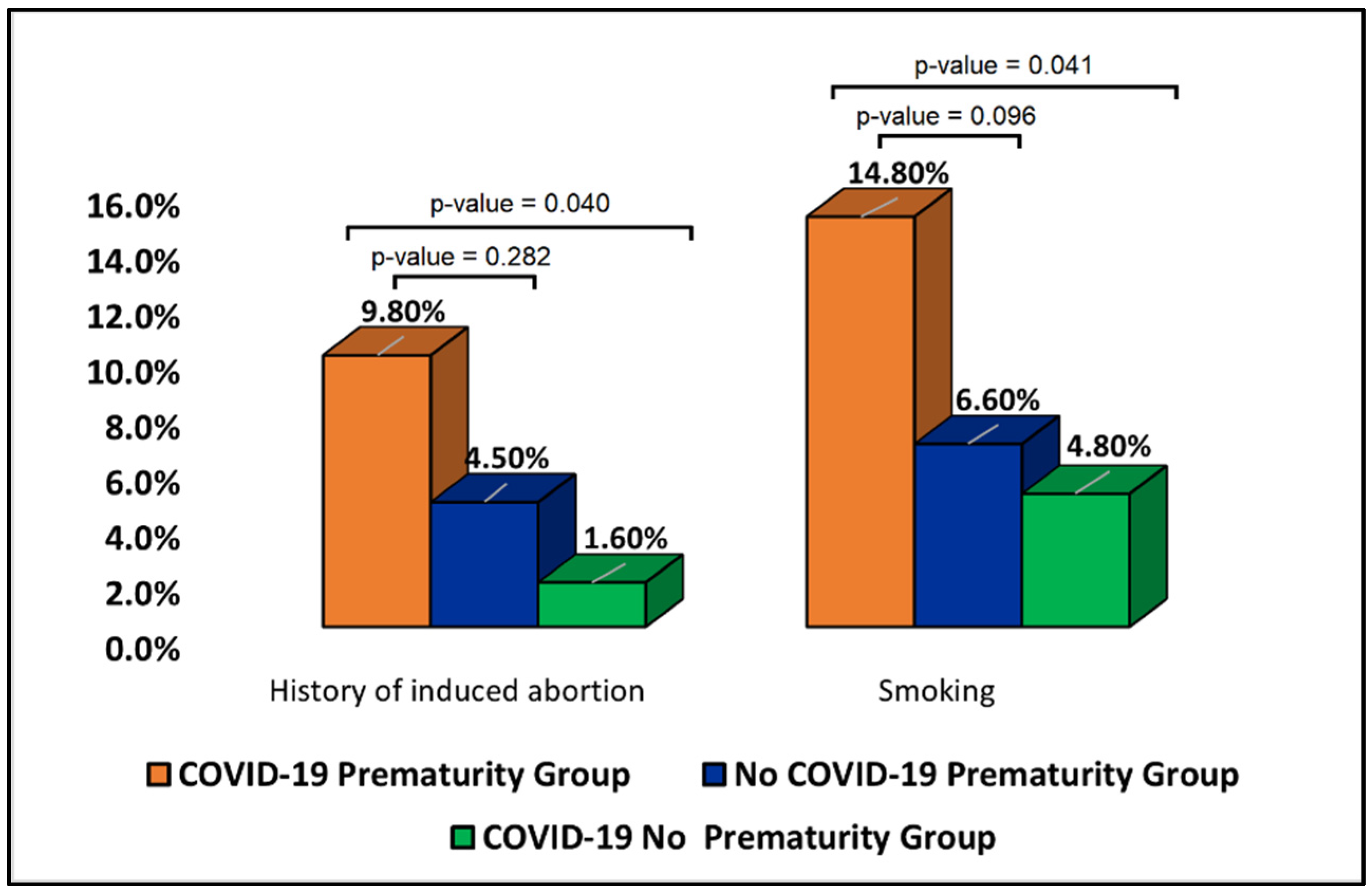
| History of induced abortion | 0.040 | |||
| Yes | 6 (9.8%) | 2 (1.6%) | 11 (4.5%) | |
| No | 53 (86.9%) | 119 (96.0%) | 228 (94.7%) | |
| COVID-19 vaccination status | 0.815 | |||
| Yes | 4 (6.6%) | 7 (5.6%) | 18 (7.4%) | |
| No | 57 (93.4%) | 117 (94.4%) | 58 (92.6%) | |
| COVID-19 vaccine doses | 0.824 | |||
| 1 | 1 (25.0%) | 3 (42.9%) | 6 (33.3%) | |
| ≥2 | 3 (75.0%) | 4 (57.1%) | 12 (66.7%) | |
| Smoking status | 0.041 | |||
| Yes | 9 (14.8%) | 6 (4.8%) | 16 (6.6%) | |
| No | 52 (85.2%) | 118 (95.2%) | 227 (93.4%) |
| Variables * | COVID-19 Prematurity Group (n = 61) | COVID-19 No Prematurity Group (n = 124) | No COVID-19 Prematurity Group (n = 243) | p-Value |
|---|---|---|---|---|
| Complications during previous pregnancies | ||||
| Pregnancy-associated DM | 3 (4.9%) | 7 (5.6%) | 11 (4.5%) | 0.895 |
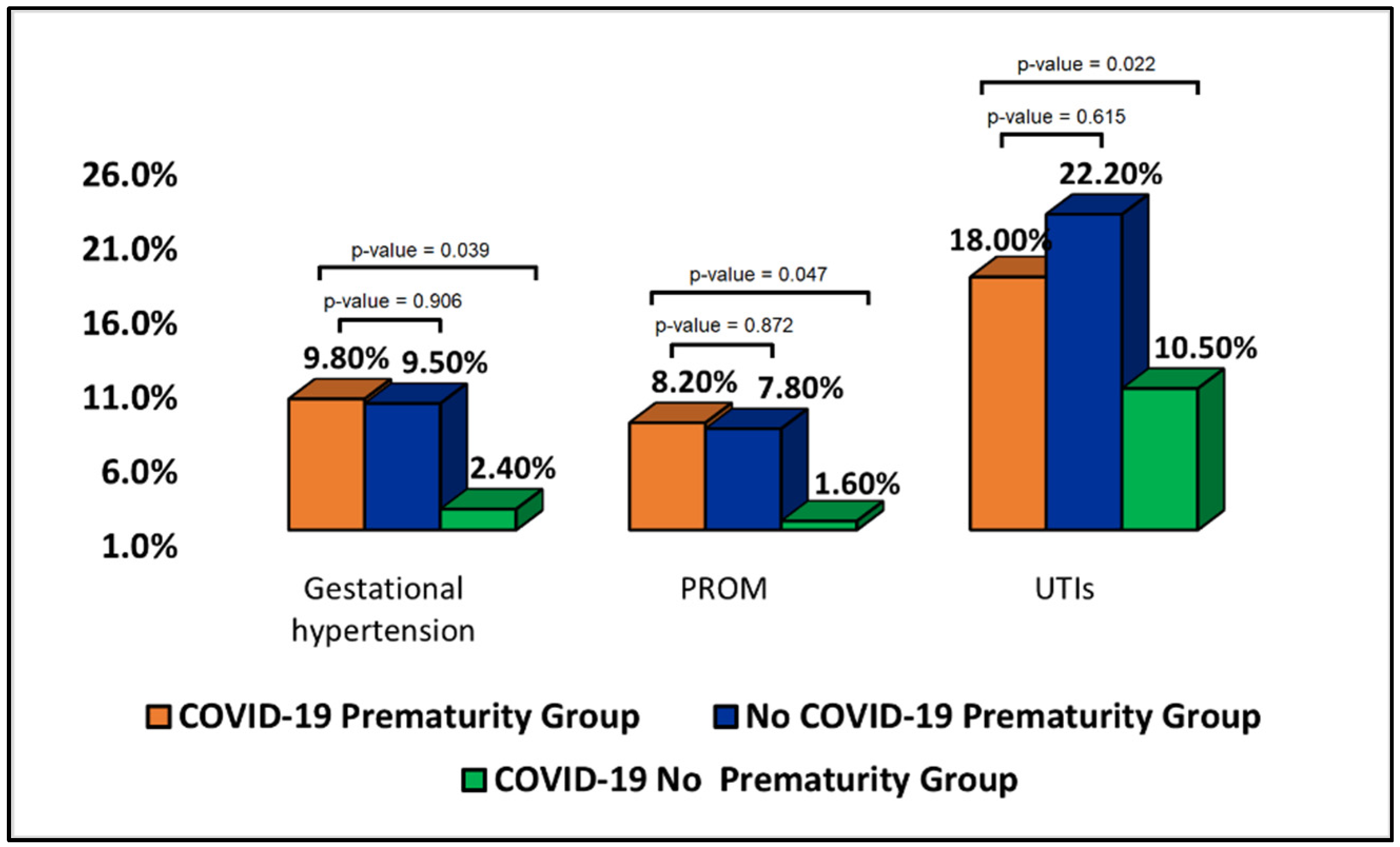
| Gestational hypertension | 6 (9.8%) | 3 (2.4%) | 23 (9.5%) | 0.039 |
| Preeclampsia | 2 (3.3%) | 1 (0.8%) | 8 (3.3%) | 0.338 |
| Abnormal placental implantation | 4 (6.6%) | 3 (2.4%) | 13 (5.3%) | 0.341 |
| PROM | 5 (8.2%) | 2 (1.6%) | 19 (7.8%) | 0.047 |
| UTIs | 11 (18.0%) | 13 (10.5%) | 54 (22.2%) | 0.022 |
| Cesarean delivery | 14 (23.0%) | 22 (17.7%) | 55 (22.6%) | 0.523 |
| Oligohydramnios | 0 (0.0%) | 1 (0.8%) | 6 (2.5%) | 0.273 |
| Polyhydramnios | 2 (3.3%) | 2 (1.6%) | 11 (4.5%) | 0.354 |
| Anemia | 12 (19.7%) | 18 (14.5%) | 52 (21.4%) | 0.283 |
| Endometritis | 2 (3.3%) | 0 (0.0%) | 7 (2.9%) | 0.150 |
| Trimester of SARS-CoV-2 infection | 0.005 | |||
| 1st trimester | 9 (14.8%) | 47 (37.9%) | – | |
| 2nd trimester | 23 (37.7%) | 37 (29.8%) | – | |
| 3rd trimester | 29 (47.5%) | 40 (32.3%) | – | |
| Symptomatic SARS-CoV-2 infection | 0.021 | |||
| Yes | 40 (76.4%) | 59 (47.6%) | – | |
| No | 21 (23.6%) | 65 (52.4%) | – | |
| Current pregnancy complications | ||||
| Pregnancy-associated DM | 4 (6.6%) | 6 (4.8%) | 18 (7.4%) | 0.642 |
| Gestational hypertension | 7 (9.8%) | 1 (0.8%) | 26 (10.7%) | 0.002 |
| Preeclampsia | 1 (1.6%) | 2 (1.6%) | 5 (2.1%) | 0.946 |
| Abnormal placental implantation | 2 (3.3%) | 3 (2.4%) | 13 (5.3%) | 0.341 |
| PROM | 6 (9.8%) | 2 (1.6%) | 17 (7.0%) | 0.040 |
| UTIs | 13 (21.3%) | 14 (11.3%) | 58 (23.9%) | 0.016 |
| Cesarean delivery | 16 (26.2%) | 25 (20.2%) | 61 (25.1%) | 0.514 |
| Oligohydramnios | 2 (3.3%) | 0 (0.0%) | 6 (2.5%) | 0.173 |
| Polyhydramnios | 3 (4.9%) | 1 (0.8%) | 7 (2.9%) | 0.219 |
| Anemia | 15 (24.6%) | 16 (12.9%) | 59 (24.3%) | 0.031 |
| Endometritis | 4 (6.6%) | 4 (3.2%) | 12 (4.9%) | 0.574 |
| Variables * | COVID-19 Prematurity Group (n = 61) | COVID-19 No Prematurity Group (n = 124) | No COVID-19 Prematurity Group (n = 243) | p-Value |
|---|---|---|---|---|
| Neonatal Outcomes | ||||
| Anemia | 9 (14.8%) | 16 (12.9%) | 40 (16.5%) | 0.664 |
| Puerperal infection | 3 (4.9%) | 3 (2.4%) | 11 (4.5%) | 0.570 |
| NRDS | 3 (4.9%) | 1 (0.8%) | 12 (4.9%) | 0.124 |
| Meconium aspiration | 5 (4.0%) | 8 (6.5%) | 22 (9.1%) | 0.690 |
| Small for gestational age | 10 (16.4%) | 9 (7.3%) | 38 (15.6%) | 0.061 |
| Sepsis | 4 (6.6%) | 1 (0.8%) | 14 (5.8%) | 0.063 |
| ICU admission | 6 (9.8%) | 0 (0.0%) | 19 (7.8%) | 0.003 |
| Mortality | 1 (1.6%) | 0 (0.0%) | 5 (2.1%) | 0.280 |
| SARS-CoV-2 infection | 2 (3.3%) | 2 (1.6%) | – | 0.463 |
| Birth weight | 0.001 | |||
| <1500 g | 1 (1.6%) | 0 (0.0%) | 5 (2.1%) | |
| 1500–2500 g | 12 (19.7%) | 6 (4.8%) | 47 (19.3%) | |
| >2500 g | 48 (82.7%) | 118 (93.4%) | 191 (94.6%) | |
| Severity of prematurity | 0.670 | |||
| Moderate to late preterm (32–37 weeks) | 42 (68.9%) | – | 177 (72.8%) | |
| Very preterm (28–32 weeks) | 16 (26.2%) | – | 59 (24.3%) | |
| Extremely preterm (<28 weeks) | 3 (4.9%) | – | 7 (2.9%) | |
| APGAR score | <0.001 | |||
| ≥9 | 7 (11.5%) | 78 (62.9%) | 32 (13.2%) | |
| 7–8 | 40 (65.6%) | 34 (27.4%) | 172 (70.8%) | |
| ≤6 | 14 (23.0%) | 12 (9.7%) | 39 (16.0%) |
| Variables * | Normal Range | At Admission | p-Value | Before Discharge | p-Value | ||
|---|---|---|---|---|---|---|---|
| COVID-19 Prematurity Group (n = 61) | COVID-19 No Prematurity Group (n = 124) | COVID-19 Prematurity Group (n = 61) | COVID-19 No Prematurity Group (n = 124) | ||||
| RBC (millions/mm3) | 4.35–5.65 | 16 (26.2%) | 22 (17.7%) | 0.179 | 13 (21.3%) | 20 (16.1%) | 0.386 |
| PLT (thousands/mm3) | 150–450 | 14 (23.0%) | 19 (15.3%) | 0.202 | 12 (19.7%) | 16 (12.9%) | 0.227 |
| WBC (thousands/mm3) | 4.5–11.0 | 38 (62.3%) | 76 (61.3%) | 0.894 | 22 (36.1%) | 51 (41.1%) | 0.507 |
| Lymphocytes (thousands/mm3) | 1.0–4.8 | 40 (65.6%) | 65 (52.4%) | 0.089 | 23 (37.7%) | 31 (25.0%) | 0.079 |
| Hb (g/dL) | 11.0–15.0 | 17 (27.9%) | 19 (15.3%) | 0.042 | 14 (23.0%) | 15 (12.1%) | 0.056 |
| Hematocrit (%) | 30–37 | 13 (21.3%) | 14 (11.3%) | 0.069 | 10 (16.4%) | 11 (8.9%) | 0.129 |
| Creatinine (µmol/L) | 0.4–08 | 3 (4.9%) | 3 (2.4%) | 0.367 | 6 (9.8%) | 6 (4.8%) | 0.194 |
| BUN (mmol/L) | 2.1–8.5 | 4 (6.6%) | 8 (6.5%) | 0.978 | 7 (11.5%) | 5 (4.0%) | 0.053 |
| GFR | >60 | 6 (9.8%) | 5 (4.0%) | 0.116 | 6 (9.8%) | 7 (5.6%) | 0.294 |
| Fasting glucose (mg/dL) | <95 | 5 (8.2%) | 10 (8.1%) | 0.975 | 11 (18.0%) | 14 (11.3%) | 0.207 |
| ALT (U/L) | 7–35 | 7 (11.5%) | 6 (4.8%) | 0.096 | 15 (24.6%) | 19 (15.3%) | 0.126 |
| AST (U/L) | 10–40 | 8 (13.1%) | 14 (11.3%) | 0.718 | 12 (19.7%) | 14 (11.3%) | 0.123 |
| Ferritin (ng/mL) | 15–300 | 23 (37.7%) | 31 (25.0%) | 0.073 | 17 (27.9%) | 26 (21.0%) | 0.296 |
| LDH (U/L) | 100–300 | 9 (14.8%) | 16 (12.9%) | 0.729 | 6 (9.8%) | 5 (4.0%) | 0.116 |
| Procalcitonin (ng/mL) | <0.5 | 12 (19.7%) | 11 (8.9%) | 0.036 | 9 (14.8%) | 8 (6.5%) | 0.066 |
| CRP (mg/L) | 0–10 | 29 (47.5%) | 40 (32.3%) | 0.043 | 11 (18.0%) | 13 (10.5%) | 0.150 |
| IL-6 (pg/mL) | 0–16 | 21 (34.4%) | 23 (18.5%) | 0.017 | 10 (16.4%) | 12 (9.7%) | 0.184 |
| ESR (mm/h) | 0–22 | 20 (32.8%) | 29 (23.4%) | 0.173 | 13 (21.3%) | 19 (15.3%) | 0.311 |
| Fibrinogen (g/L) | 2–4 | 24 (39.3%) | 39 (31.5%) | 0.286 | 13 (21.3%) | 20 (16.1%) | 0.386 |
| D-dimers (ng/mL) | <250 | 18 (29.5%) | 32 (25.8%) | 0.594 | 16 (26.2%) | 24 (19.4%) | 0.285 |
| Variables * | Normal Range | COVID-19 Prematurity Group (n = 61) | COVID-19 No Prematurity Group (n = 124) | No COVID-19 Prematurity Group (n = 243) | p-Value |
|---|---|---|---|---|---|
| RBC (millions/mm3) | 4.35–5.65 | 18 (29.5%) | 26 (21.0%) | 63 (25.9%) | 0.664 |
| PLT (thousands/mm3) | 150–450 | 11 (18.0%) | 16 (12.9%) | 47 (19.3%) | 0.300 |
| WBC (thousands/mm3) | 4.5–11.0 | 16 (26.2%) | 14 (11.3%) | 38 (15.6%) | 0.042 |
| Lymphocytes (thousands/mm3) | 1.0–4.8 | 12 (19.7%) | 20 (16.1%) | 32 (13.2%) | 0.404 |
| Hb (g/dL) | 11.0–15.0 | 13 (21.3%) | 26 (21.0%) | 29 (11.9%) | 0.037 |
| Hematocrit (%) | 36–48 | 16 (26.2%) | 24 (19.4%) | 58 (23.9%) | 0.497 |
| Creatinine (µmol/L) | 0.74–1.35 | 4 (6.6%) | 6 (4.8%) | 11 (4.5%) | 0.805 |
| BUN (mmol/L) | 2.1–8.5 | 3 (4.9%) | 4 (3.2%) | 13 (5.3%) | 0.656 |
| GFR | >60 | 6 (9.8%) | 14 (11.3%) | 18 (7.4%) | 0.446 |
| Fasting glucose (mg/dL) | 72–125 | 7 (11.5%) | 20 (16.1%) | 32 (13.2%) | 0.629 |
| ALT (U/L) | 7–35 | 5 (8.2%) | 10 (8.1%) | 19 (7.8%) | 0.993 |
| AST (U/L) | 10–40 | 4 (6.6%) | 8 (6.5%) | 14 (5.8%) | 0.952 |
| Ferritin (ng/mL) | 15–300 | 14 (23.0%) | 19 (15.3%) | 63 (25.9%) | 0.070 |
| LDH (U/L) | 100–300 | 6 (9.8%) | 7 (5.6%) | 27 (11.1%) | 0.232 |
| Procalcitonin (ng/mL) | <0.5 | 2 (3.3%) | 1 (0.8%) | 3 (1.2%) | 0.382 |
| CRP (mg/L) | 0–10 | 11 (18.0%) | 11 (8.9%) | 18 (7.4%) | 0.024 |
| IL-6 (pg/mL) | 0–16 | 8 (13.1%) | 12 (9.7%) | 22 (9.1%) | 0.738 |
| ESR (mm/h) | 0–22 | 7 (11.5%) | 19 (15.3%) | 20 (8.2%) | 0.113 |
| Fibrinogen (g/L) | 2–4 | 4 (6.6%) | 7 (5.6%) | 16 (6.6%) | 0.937 |
| D-dimer (ng/mL) | <250 | 8 (13.1%) | 14 (11.3%) | 15 (6.2%) | 0.104 |
| β for Premature Birth * | (95% CI of β) | Significance | |
|---|---|---|---|
| SARS-CoV-2 infection (independent constant) ** | 1.09 | 0.94–1.15 | 0.067 |
| Covariates (predictors)—clinical | |||
| History of induced abortion | 1.13 | 0.82–1.34 | 0.091 |
| Smoking | 2.07 | 1.25–2.84 | 0.002 |
| Gestational hypertension | 2.36 | 1.44–3.78 | <0.001 |
| PROM | 1.94 | 1.13–3.69 | <0.001 |
| UTIs | 1.82 | 1.27–3.22 | <0.001 |
| 3rd Trimester of SARS-CoV-2 infection | 1.55 | 1.38–2.93 | 0.014 |
| Symptomatic SARS-CoV-2 infection | 1.23 | 1.09–2.21 | 0.036 |
| Covariates (predictors)—biological | |||
| Anemia | 3.65 | 1.46–5.39 | <0.001 |
| Elevated procalcitonin | 1.09 | 0.91–1.43 | 0.063 |
| Elevated CRP | 2.11 | 1.34–3.06 | <0.001 |
| Elevated IL-6 | 1.92 | 1.20–2.47 | 0.001 |
| Elevated WBC | 1.13 | 0.98–1.42 | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hrubaru, I.; Motoc, A.; Bratosin, F.; Rosca, O.; Folescu, R.; Moise, M.L.; Neagoe, O.; Citu, I.M.; Feciche, B.; Gorun, F.; et al. Exploring Clinical and Biological Features of Premature Births among Pregnant Women with SARS-CoV-2 Infection during the Pregnancy Period. J. Pers. Med. 2022, 12, 1871. https://doi.org/10.3390/jpm12111871
Hrubaru I, Motoc A, Bratosin F, Rosca O, Folescu R, Moise ML, Neagoe O, Citu IM, Feciche B, Gorun F, et al. Exploring Clinical and Biological Features of Premature Births among Pregnant Women with SARS-CoV-2 Infection during the Pregnancy Period. Journal of Personalized Medicine. 2022; 12(11):1871. https://doi.org/10.3390/jpm12111871
Chicago/Turabian StyleHrubaru, Ingrid, Andrei Motoc, Felix Bratosin, Ovidiu Rosca, Roxana Folescu, Marius Liviu Moise, Octavian Neagoe, Ioana Mihaela Citu, Bogdan Feciche, Florin Gorun, and et al. 2022. "Exploring Clinical and Biological Features of Premature Births among Pregnant Women with SARS-CoV-2 Infection during the Pregnancy Period" Journal of Personalized Medicine 12, no. 11: 1871. https://doi.org/10.3390/jpm12111871