

Markers for the Prediction of Probably Sarcopenia in Middle-Aged Individuals
 , ,
, ,
Abstract
:1. Introduction
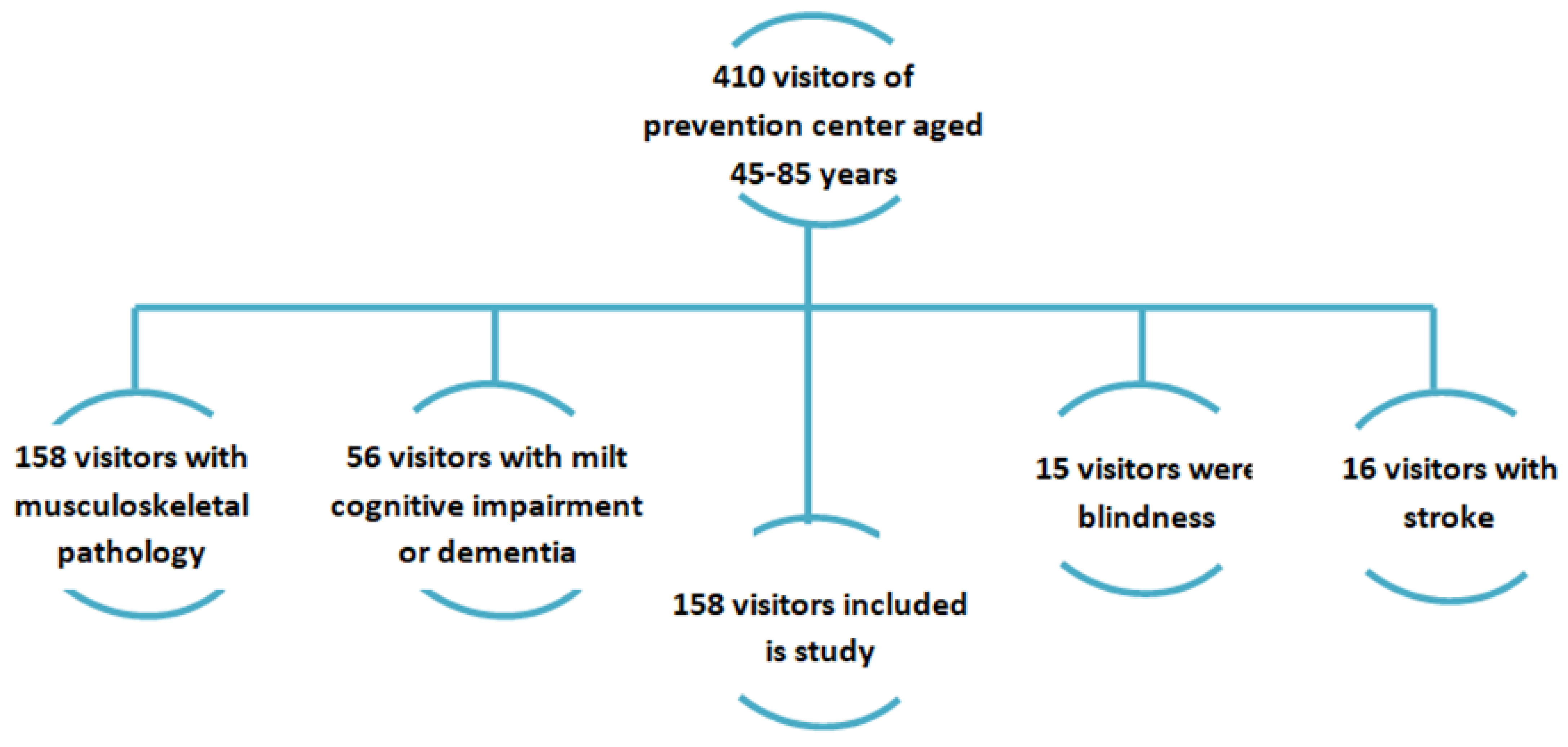
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations News Service Section. UN News Centre Opening Remarks at Press Event on Day of Seven Billion; UN News Service Section: New York, NY, USA, 2011. [Google Scholar]
- Grigorieva, I.I.; Raskina, T.A.; Letaeva, M.V.; Malyshenko, O.S.; Averkieva, Y.V.; Masenko, V.L.; Kokov, A.N. Sarcopenia: Features of pathogenesis and diagnosis. Fundam. Clin. Med. 2019, 4, 105–116. [Google Scholar] [CrossRef] [Green Version]
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta- analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogat, S.V. The prevalence of sarcopenia in patients of older age groups. Gerontology 2014, 3, 305–310. (In Russian) [Google Scholar]
- Bischoff-Ferrari, H.A.; Orav, J.E.; Kanis, J.A.; Rizzoli, R.; Schlögl, M.; Staehelin, H.B.; Willett, W.C.; Dawson-Hughes, B. Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos. Int. 2015, 26, 2793–2802. [Google Scholar] [CrossRef]
- Misnikova, I.V.; Kovaleva, Y.A.; Klimina, N.A. Sarkopenic obesity. Russ. Med. J. 2017, 25, 24–29. (In Russian) [Google Scholar]
- Nipp, R.D.; Fuchs, G.; El-Jawahri, A.; Mario, J.; Troschel, F.M.; Greer, J.A.; Gallagher, E.R.; Jackson, V.A.; Kambadakone, A.; Hong, T.S.; et al. Sarcopenia is Associated with Quality of Life and Depression in Patients with Advanced Cancer. Oncologist 2018, 23, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Morville, T.; Sahl, R.E.; Trammell, S.A.; Svenningsen, J.S.; Gillum, M.P.; Helge, J.W.; Clemmensen, C. Divergent effects of resistance and endurance exercise on plasma bile acids, FGF19, and FGF21 in humans. JCI Insight 2018, 3, e122737. [Google Scholar] [CrossRef]
- Sanchis-Gomar, F.; Pareja-Galeano, H.; Santos-Lozano, A.; Garatachea, N.; Fiuza-Luces, C.; Venturini, L.; Ricevuti, G.; Lucia, A.; Emanuele, E. A preliminary candidate approach identifies the combination of chemerin, fetuin-A, and fibroblast growth factors 19 and 21 as a potential biomarker panel of successful aging. Age 2015, 37, 42. [Google Scholar] [CrossRef] [Green Version]
- Yamakage, H.; Tanaka, M.; Inoue, T.; Odori, S.; Kusakabe, T.; Satoh-Asahara, N. Effects of dapagliflozin on the serum levels of fibroblast growth factor 21 and myokines and muscle mass in Japanese patients with type 2 diabetes: A randomized, controlled trial. J. Diabetes Investig. 2020, 11, 653–661. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Y.; Nie, C.; Min, J.; Liu, X.; Li, M.; Chen, H.; Xu, H.; Wang, M.; Ni, T.; Li, Y.; et al. Novel loci and pathways significantly associated with longevity. Sci Rep. 2016, 6, 21243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Marco, S.; Mazroui, R.; Dallaire, P.; Chittur, S.; Tenenbaum, S.A.; Radzioch, D.; Marette, A.; Gallouzi, I.-E. NF-κB-mediated MyoD decay during muscle wasting requires nitric oxide synthase mRNA stabilization, HuR protein, and nitric oxide release. Mol. Cell. Biol. 2005, 25, 6533–6545. [Google Scholar] [CrossRef] [PubMed]
- Hall, D.T.; Ma, J.F.; Marco, S.D.; Di Marco, S.; Gallouzi, I.-E. Inducible nitric oxide synthase (iNOS) in muscle wasting syndrome, sarcopenia, and cachexia. Aging 2011, 3, 702–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coggan, A.R.; Racette, S.B.; Thies, D.; Peterson, L.R.; Stratford, R.E., Jr. Simultaneous Pharmacokinetic Analysis of Nitrate and its Reduced Metabolite, Nitrite, Following Ingestion of Inorganic Nitrate in a Mixed Patient Population. Pharm. Res. 2020, 37, 235. [Google Scholar] [CrossRef] [PubMed]
- Barrera, G.; Pizzimenti, S.; Daga, M.; Dianzani, C.; Arcaro, A.; Cetrangolo, G.P.; Giordano, G.; Cucci, M.A.; Graf, M.; Gentile, F. Lipid Peroxidation-Derived Aldehydes, 4-Hydroxynonenal and Malondialdehyde in Aging-Related Disorders. Antioxidants 2018, 7, 102. [Google Scholar] [CrossRef] [Green Version]
- Standley, R.A.; Distefano, G.; Pereira, S.L.; Tian, M.; Kelly, O.J.; Coen, P.M.; Deutz, N.E.P.; Wolfe, R.R.; Goodpaster, B.H. Effects of β-hydroxy-β-methylbutyrate on skeletal muscle mitochondrial content and dynamics, and lipids after 10 days of bed rest in older adults. J. Appl. Physiol. 2017, 123, 1092–1100. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Niti, M.; Yap, K.B.; Tan, C.T.Y.; Nyunt, M.S.Z.; Feng, L.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; et al. Effects of multi-domain lifestyle interventions on sarcopenia measures and blood biomarkers: Secondary analysis of a randomized controlled trial of community-dwelling pre-frail and frail older adults. Aging 2021, 13, 9330–9347. [Google Scholar] [CrossRef]
- Krzymińska-Siemaszko, R.; Fryzowicz, A.; Czepulis, N.; Kaluźniak-Szymanowska, A.; Dworak, L.B.; Wieczorowska-Tobis, K. The impact of the age range of young healthy reference population on the cut-off points for low muscle mass necessary for the diagnosis of sarcopenia. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 4321–4332. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Shahar, S.; Kamaruddin, N.S.; Badrasawi, M.; Sakian, N.I.; Manaf, Z.A.; Yassin, Z.; Joseph, L. Effectiveness of exercise and protein supplementation intervention on body composition, functional fitness, and oxidative stress among elderly Malays with sarcopenia. Clin. Interv. Aging 2013, 8, 1365–1375. [Google Scholar] [CrossRef] [Green Version]
- Soysal, P.; Smith, L.; Isik, A.T. Validation of population-based cut-offs for low muscle mass and strength. Eur. Geriatr. Med. 2020, 11, 713–714. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.X.; Li, J.; Chen, C.; Yin, T.; Wang, Q.A.; Li, X.X.; Wang, F.X.; Zhao, J.H.; Zhao, Y.; Zhang, Y.H. Reference values of skeletal muscle mass, fat mass and fat-to-muscle ratio for rural middle age and older adults in western China. Arch. Gerontol. Geriatr. 2021, 95, 104389. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Park, K.S.; Yoo, J.I. Associations between the quality of life in sarcopenia measured with the SarQoL® and nutritional status. Health Qual. Life Outcomes 2021, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Krzymińska-Siemaszko, R.; Deskur-Śmielecka, E.; Styszyński, A.; Wieczorowska-Tobis, K. Polish Translation and Validation of the Mini Sarcopenia Risk Assessment (MSRA) Questionnaire to Assess Nutritional and Non-Nutritional Risk Factors of Sarcopenia in Older Adults. Nutrients 2021, 13, 1061. [Google Scholar] [CrossRef] [PubMed]
- Vandewoude, M.F.J.; Alish, C.J.; Sauer, A.C.; Hegazi, R.A. Malnutrition-sarcopenia syndrome: Is this the future of nutrition screening and assessment for older adults? J. Aging Res. 2012, 2012, 651570. [Google Scholar] [CrossRef]
- Suetta, C.; Haddock, B.; Alcazar, J.; Noerst, T.; Hansen, O.M.; Ludvig, H.; Kamper, R.S.; Schnohr, P.; Prescott, E.; Andersen, L.L.; et al. The Copenhagen Sarcopenia Study: Lean mass, strength, power, and physical function in a Danish cohort aged 20–93 years. J. Cachexia Sarcopenia Muscle 2019, 10, 1316–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geerinck, A.; Bruyère, O.; Locquet, M.; Reginster, J.Y.; Beaudart, C. Evaluation of the Responsiveness of the SarQoL® Questionnaire, a Patient-Reported Outcome Measure Specific to Sarcopenia. Adv. Ther. 2018, 35, 1842–1858. [Google Scholar] [CrossRef] [Green Version]
- Verreijen, A.M.; Engberink, M.F.; Memelink, R.G.; van der Plas, S.E.; Visser, M.; Weijs, P.J. Effect of a high protein diet and/or resistance exercise on the preservation of fat free mass during weight loss in overweight and obese older adults: A randomized controlled trial. Nutr. J. 2017, 16, 10. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, T. Updates on Lifestyle-Related Diseases and Bone Metabolism. The metabolic syndrome and bone metabolism. Clin. Calcium 2014, 24, 1599–1604. [Google Scholar]
- Hernández-Martínez, P.; Olmos, J.M.; Llorca, J.; Hernández, J.L.; González-Macías, J. Sarcopenic osteoporosis, sarcopenic obesity, and sarcopenic osteoporotic obesity in the Camargo cohort (Cantabria, Spain). Arch. Osteoporos. 2022, 17, 105. [Google Scholar] [CrossRef]
- Roh, E.; Hwang, S.Y.; Yoo, H.J.; Baik, S.H.; Cho, B.; Park, Y.S.; Kim, H.J.; Lee, S.-G.; Kim, B.J.; Jang, H.C.; et al. Association of plasma FGF21 levels with muscle mass and muscle strength in a national multicentre cohort study: Korean Frailty and Aging Cohort Study. Age Ageing 2021, 50, 1971–1978. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, M.; Miyakawa, M.; Sugiyama, M.; Miyoshi, M.; Arakawa, T. Unloading during skeletal muscle regeneration retards iNOS-expressing macrophage recruitment and perturbs satellite cell accumulation. Histochem. Cell Biol. 2020, 154, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Bulatova, I.A.; Shchekotova, A.P.; Krivtsov, A.V.; Ulitina, P.V.; Larionova, G.G.; Paducheva, S.V. Significance of malondialdehyde and glutathione transferase in assessing liver damage and monitoring therapy in chronic hepatitis. Fundam. Res. 2014, 4, 246–251. [Google Scholar]
- Sim, M.; Lewis, J.R.; Blekkenhorst, L.C.; Bondonno, C.P.; Devine, A.; Zhu, K.; Peeling, P.; Prince, R.L.; Hodgson, J.M. Dietary nitrate intake is associated with muscle function in older women. J. Cachexia Sarcopenia Muscle 2019, 10, 601–610. [Google Scholar] [CrossRef]
- Valenzuela, P.L.; Morales, J.S.; Emanuele, E.; Pareja-Galeano, H.; Lucia, A. Supplements with purported effects on muscle mass and strength. Eur. J. Nutr. 2019, 58, 2983–3008. [Google Scholar] [CrossRef]
- Córdova, A.; Caballero-García, A.; Noriega-González, D.; Bello, H.J.; Pons, A.; Roche, E. Nitric-Oxide-Inducing Factors on Vitamin D Changes in Older People Susceptible to Suffer from Sarcopenia. Int. J. Environ. Res. Public Health 2022, 19, 5938. [Google Scholar] [CrossRef]
- Pin, F.; Beltrà, M.; Garcia-Castillo, L.; Pardini, B.; Birolo, G.; Matullo, G.; Penna, F.; Guttridge, D.; Costelli, P. Extracellular vesicles derived from tumor cells as a trigger of energy crisis in the skeletal muscle. J. Cachexia Sarcopenia Muscle 2022, 13, 481–494. [Google Scholar] [CrossRef]
- Kawamoto, R.; Kohara, K.; Katoh, T.; Kusunoki, T.; Ohtsuka, N.; Abe, M.; Kumagi, T.; Miki, T. Changes in oxidized low-density lipoprotein cholesterol are associated with changes in handgrip strength in Japanese community-dwelling persons. Endocrine 2015, 48, 871–877. [Google Scholar] [CrossRef]
- Petyaev, I.M.; Klochkov, V.A.; Chalyk, N.E.; Pristensky, D.V.; Chernyshova, M.P.; Kyle, N.H.; Bashmakov, Y.K. Markers of Hypoxia and Oxidative Stress in Aging Volunteers Ingesting Lycosomal Formulation of Dark Chocolate Containing Astaxanthin. J. Nutr. Health Aging 2018, 22, 1092–1098. [Google Scholar] [CrossRef]
- Wang, S.; Zhou, H.; Zhao, C.; He, H. Effect of Exercise Training on Body Composition and Inflammatory Cytokine Levels in Overweight and Obese Individuals: A Systematic Review and Network Meta-Analysis. Front. Immunol. 2022, 13, 921085. [Google Scholar] [CrossRef]


{kind=link}
| Parameters | Women | p | Men | p | ||
|---|---|---|---|---|---|---|
| Main Group (n = 118) | Control Group (n = 28) | Main Group (n = 47) | Control Group (n = 28) | |||
| Age, years | 54 [48–65] | 55 [48–66] | 0.453 | 53 [49–59] | 52 [47–56.5] | 0.534 |
| Body mass index kg/m2 | 28.5 [25.1–31.8] | 28.5 [25.1–31.8] | 0.285 | 28.5 [25.1–31.8] | 28.5 [25.1–31.8] | 0.285 |
| Waist-to-hip ratio | 0.97 [0.93–1.01] | 0.96 [0.9–1.02] | 0.435 | 0.94 [0.8–1.02] | 0.95 [0.8–1.05] | 0.435 |
| Right hand, kg | 24 [19–31] | 40 [38–53] | 0.001 | 17 [15–24] | 35 [27–39] | 0.001 |
| Left hand, kg | 23 [19–29] | 38 [33–51] | 0.001 | 15 [13–22] | 33 [25–36] | 0.001 |
| Gait speed, m/s | 0.95 [0.8–1.25] | 1.15 [0.8–1.4] | <0.001 | 1.0 [0.9–1.3] | 1.2 [0.9–1.5] | <0.001 |
| Glycemia, mmol/L | 4.9 [4.6–5.3] | 4.95 [4.6–5.3] | 0.834 | 4.7 [4.3–5.2] | 4.5 [4.2–5.0] | 0.745 |
| Options | Main Group | Control Group | p |
|---|---|---|---|
| SarQol | 80.54 [67.89–86.895] | 78.03 [63.81–89.19] | 0.833 |
| HADS (anaxiety) | 4 [2–7] | 4 [2–6] | 0.108 |
| HADS (depression) | 4 [2–6] | 3 [1–5] | 0.142 |
| SF36, physical component | 55 [49–59] | 56 [50–60] | 0.228 |
| SF36, psychological component | 45 [42–48] | 46 [43–49] | 0.499 |
| Parameters | Women | p | Men | p | ||
|---|---|---|---|---|---|---|
| Main Group (n = 118) | Control Group (n = 28) | Main Group (n = 47) | Control Group (n = 28) | |||
| Body fat mass (kg) | 28 [25.1–36] | 26.5 [20.65–35] | 0.011 | 30 [26.1–38] | 26.5 [20.65–35] | 0.002 |
| Body fat percentage (%) | 35.9 [35.4–41.3] | 33.7 [29.85–40.1] | 0.0001 | 39.7 [35.6–44.8] | 35.1 [29.7–40.5] | 0.0001 |
| Visceral fat area (cm2) | 144.2 [128.3–176.1] | 129.1 [92.2–169.25] | 0.002 | 154.7 [128.3–198.4] | 132.3 [95.3–183.5] | 0.002 |
| Skeletal muscle mass (kg2) | 25.5 [23.4–27.9] | 28.6 [22.9–33.3] | 0.043 | 23.2 [21.4–27.4] | 26.4 [22.5–34.1] | 0.003 |
| Appendicular muscle mass (m2) | 6.7 [5.9–7.3] | 7.8 [6.5–8.9] | <0.001 | 6.4 [5.85–7.1] | 7.6 [6.3–8.5] | <0.001 |
| Protein content | 8.9 [8.1–10.0] | 9.5 [8.25–11.6] | 0.048 | 8.4 [7.5–9.4] | 9.3 [8.25–11.6] | 0.002 |
| Minerals | 3.1 [2.8–3.4] | 3.9 [2.9–4.0] | 0.03 | 3.0 [2.5–3.5] | 3.6 [2.8–3.9] | 0.044 |
| Metabolites | Main Group (F = M = 47) | Control Group (F = M = 28) | p |
|---|---|---|---|
| Fibroblast growth factor 21 ng/L | 263.8 [251.4–274.8] | 267 [246.5–273.5] | 0.80 |
| Nitrates, mmol/L | 0.21 [0.21–0.355] | 0.105 [0.07–0.14] | 0.05 |
| Malondialdehyde (MDA), µmol/L | 290.32 [260.97–290.32] | 147.42 [78.06–216.77] | 0.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samoilova, Y.G.; Matveeva, M.V.; Khoroshunova, E.A.; Kudlay, D.A.; Oleynik, O.A.; Spirina, L.V. Markers for the Prediction of Probably Sarcopenia in Middle-Aged Individuals. J. Pers. Med. 2022, 12, 1830. https://doi.org/10.3390/jpm12111830
Samoilova YG, Matveeva MV, Khoroshunova EA, Kudlay DA, Oleynik OA, Spirina LV. Markers for the Prediction of Probably Sarcopenia in Middle-Aged Individuals. Journal of Personalized Medicine. 2022; 12(11):1830. https://doi.org/10.3390/jpm12111830
Chicago/Turabian StyleSamoilova, Yulia G., Mariia V. Matveeva, Ekaterina A. Khoroshunova, Dmitry A. Kudlay, Oxana A. Oleynik, and Liudmila V. Spirina. 2022. "Markers for the Prediction of Probably Sarcopenia in Middle-Aged Individuals" Journal of Personalized Medicine 12, no. 11: 1830. https://doi.org/10.3390/jpm12111830