
Experiences of Migrant People Living with HIV in a Multidisciplinary HIV Care Setting with Rapid B/F/TAF Initiation and Cost-Covered Treatment: The ‘ASAP’ Study
 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Design
2.3. Data Collection
2.4. Data Analysis
2.5. Patient and Stakeholder Engagement
2.6. Ethics
3. Results
3.1. Participant Demographics at Enrollment
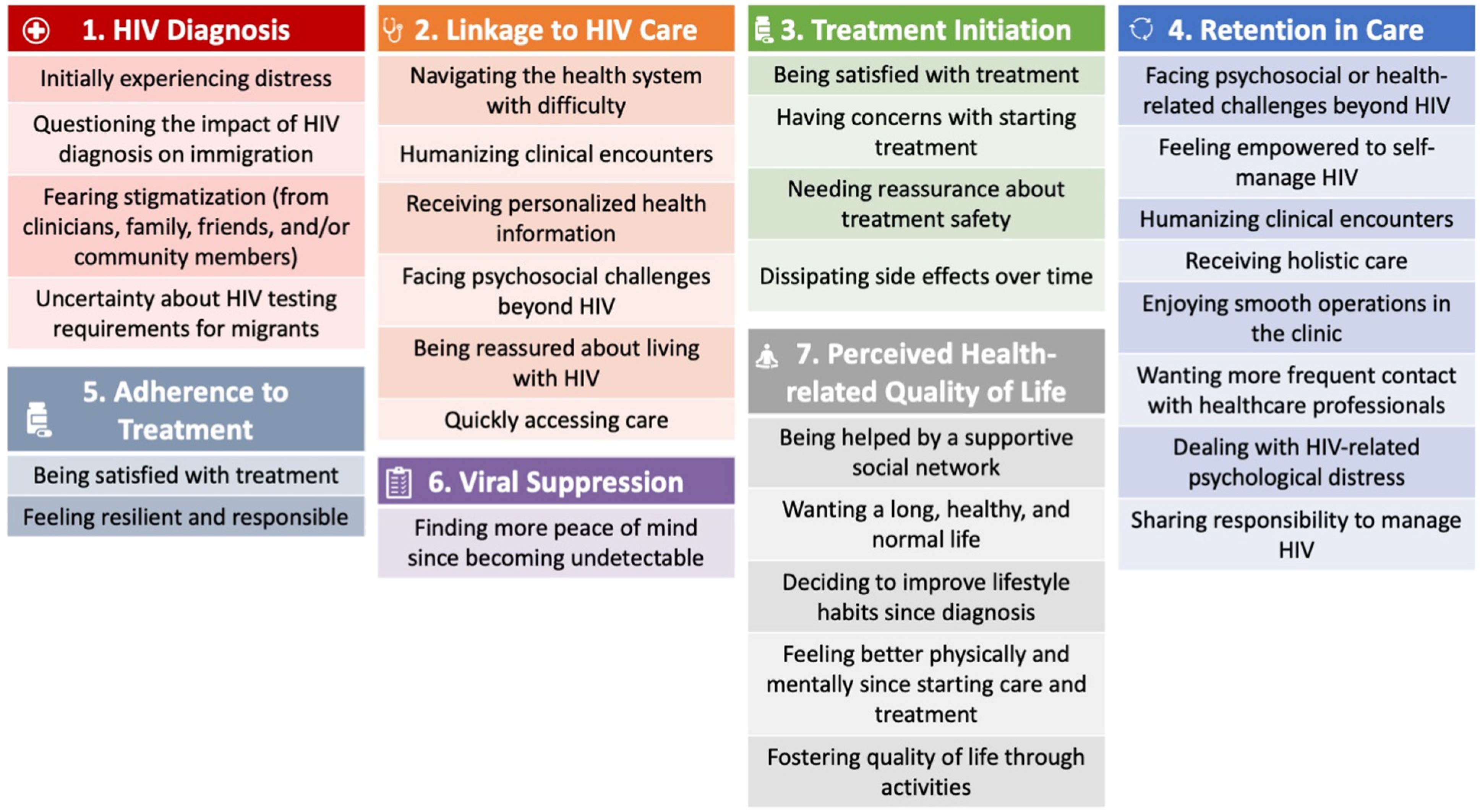
3.2. Categories
3.2.1. HIV Diagnosis
3.2.2. Linkage to HIV Care
3.2.3. Treatment Initiation
3.2.4. Retention in Care
3.2.5. Adherence to Treatment
3.2.6. Viral Suppression
3.2.7. Perceived Health-Related Quality of Life (HrQoL)
4. Discussion
4.1. Diagnosis: Dominated by Distress & Immigration-Related Concerns
4.2. Linkage: A Time of Navigation Challenges and an Opportunity to Connect with Clinicians
4.3. Treatment Initiation: Rapid ART Is Satisfying, but Concerns Exist
4.4. Retention in Care: The Burden of Challenges beyond HIV and Importance of Patient-Centered Care
4.5. Adherence to Treatment: The Heightened Importance of Taking Control over HIV
4.6. Viral Suppression: Characterized by Peace of Mind and a Sense of Control
4.7. Perceived Health-Related Quality of Life: Promoted by Social Networks and Personal Activities
4.8. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haddad, N.; Robert, A.; Weeks, A.; Popovic, N.; Siu, W.; Archibald, C. HIV: HIV in Canada—Surveillance Report, 2018. Can. Commun. Dis. Rep. 2019, 45, 304. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, P.S.; Jones, J.S.; Baral, S.D. The global north: HIV epidemiology in high-income countries. Curr. Opin. HIV AIDS 2014, 9, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.; Cunningham, C.O.; Hanna, D.B. HIV outcomes among migrants from low-and middle-income countries living in high-income countries: A review of recent evidence. Curr. Opin. Infect. Dis. 2018, 31, 25. [Google Scholar] [CrossRef] [PubMed]
- Tavares, A.M.; Fronteira, I.; Couto, I.; Machado, D.; Viveiros, M.; Abecasis, A.B.; Dias, S. HIV and tuberculosis co-infection among migrants in Europe: A systematic review on the prevalence, incidence and mortality. PLoS ONE 2017, 12, e0185526. [Google Scholar]
- Tavares, A.M.; Pingarilho, M.; Batista, J.; Viveiros, M.; Dias, S.; Toscano, C.; Gomes, P.; Abecasis, A.B. HIV and tuberculosis co-infection among migrants in Portugal: A brief study on their sociodemographic, clinical, and genomic characteristics. AIDS Res. Hum. Retrovir. 2021, 37, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Weine, S.M.; Kashuba, A.B. Labor migration and HIV risk: A systematic review of the literature. AIDS Behav. 2012, 16, 1605–1621. [Google Scholar] [CrossRef]
- Tanser, F.; Bärnighausen, T.; Vandormael, A.; Dobra, A. HIV treatment cascade in migrants and mobile populations. Curr. Opin. HIV AIDS 2015, 10, 430–438. [Google Scholar] [CrossRef]
- Reyes-Uruena, J.; Campbell, C.; Hernando, C.; Vives, N.; Folch, C.; Ferrer, L.; Fernandez-Lopez, L.; Esteve, A.; Casabona, J. Differences between migrants and Spanish-born population through the HIV care cascade, Catalonia: An analysis using multiple data sources. Epidemiol. Infect. 2017, 145, 1670–1681. [Google Scholar] [CrossRef]
- UNAIDS. Seizing the Moment: Tackling entrenched inequalities to end epidemics. Glob. AIDS Update 2020. Available online: https://www.unaids.org/en/resources/documents/2020/global-aids-report (accessed on 1 May 2022).
- Blondell, S.J.; Kitter, B.; Griffin, M.P.; Durham, J. Barriers and facilitators to HIV testing in migrants in high-income countries: A systematic review. AIDS Behav. 2015, 19, 20. [Google Scholar] [CrossRef]
- Alvarez-del Arco, D.; Monge, S.; Azcoaga, A.; Rio, I.; Hernando, V.; Gonzalez, C.; Alejos, B.; Caro, A.M.; Perez-Cachafeiro, S.; Ramirez-Rubio, O.; et al. HIV testing and counselling for migrant populations living in high-income countries: A systematic review. Eur. J. Public Health 2013, 23, 1039–1045. [Google Scholar] [CrossRef]
- Rade, D.A.; Crawford, G.; Lobo, R.; Gray, C.; Brown, G. Sexual health help-seeking behavior among migrants from sub-Saharan Africa and South East Asia living in high income countries: A systematic review. Int. J. Environ. Res. Public Health 2018, 15, 1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aung, E.; Blondell, S.J.; Durham, J. Interventions for increasing HIV testing uptake in migrants: A systematic review of evidence. AIDS Behav. 2017, 21, 2844–2859. [Google Scholar] [CrossRef] [PubMed]
- Keygnaert, I.; Guieu, A.; Ooms, G.; Vettenburg, N.; Temmerman, M.; Roelens, K. Sexual and reproductive health of migrants: Does the EU care? Health Policy 2014, 114, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Dias, S.; Gama, A.; Severo, M.; Barros, H. Factors associated with HIV testing among immigrants in Portugal. Int. J. Public Health 2011, 56, 559–566. [Google Scholar] [CrossRef]
- Hoyos, J.; Fernández-Balbuena, S.; de la Fuente, L.; Sordo, L.; Ruiz, M.; Barrio, G.; José Belza, M. Madrid Rapid HIV Testing Group. Never tested for HIV in Latin-American migrants and Spaniards: Prevalence and perceived barriers. J. Int. AIDS Soc. 2013, 16, 18560. [Google Scholar] [CrossRef]
- Ojikutu, B.; Nnaji, C.; Sithole, J.; Schneider, K.L.; Higgins-Biddle, M.; Cranston, K.; Earls, F. All black people are not alike: Differences in HIV testing patterns, knowledge, and experience of stigma between US-born and non–US-born blacks in Massachusetts. AIDS Patient Care STDs 2013, 27, 45–54. [Google Scholar] [CrossRef]
- Manirankunda, L.; Loos, J.; Alou, T.A.; Colebunders, R.; Nöstlinger, C. “It’s better not to know”: Perceived barriers to HIV voluntary counseling and testing among sub-Saharan African migrants in Belgium. AIDS Educ. Prev. 2009, 21, 582–593. [Google Scholar] [CrossRef]
- Amibor, P.; Ogunrotifa, A.B. Unravelling barriers to accessing HIV prevention services experienced by African and Caribbean communities in Canada: Lessons from Toronto. Glob. J. Health Sci. 2012, 4, 1. [Google Scholar]
- Kronfli, N.; Linthwaite, B.; Sheehan, N.; Cox, J.; Hardy, I.; Lebouché, B.; de Pokomandy, A.; Frenette, C.; Roger, M.; Klein, M.B. Delayed linkage to HIV care among asylum seekers in Quebec, Canada. BMC Public Health 2019, 19, 1683. [Google Scholar] [CrossRef]
- Arora, A.; Quesnel-Vallee, A.; Lessard, D.; Mate, K.; Rodriguez-Cruz, A.; Kronfli, N.; Engler, K.; Vedel, I.; Lebouché, B. Barriers and facilitators associated with steps of the HIV care cascade for migrants in OECD countries: A systematic mixed studies review protocol. BMJ Open 2020, 10, e040646. [Google Scholar]
- Arora, A.K.; Ortiz-Paredes, D.; Engler, K.; Lessard, D.; Mate, K.K.; Rodriguez-Cruz, A.; Kronfli, N.; Vedel, I.; Cox, J. Antiviral Speed Access Program (ASAP) Migrant Advisory Committee, Quesnel-Vallée A. Barriers and Facilitators Affecting the HIV Care Cascade for Migrant People Living with HIV in Organization for Economic Co-Operation and Development Countries: A Systematic Mixed Studies Review. AIDS Patient Care STDs 2021, 35, 288–307. [Google Scholar] [PubMed]
- Jungwirth, B. Ending the HIV Epidemic: Researchers Call for an Equity-Focused Approach. Coverage of IAS 2021, the 11th International AIDS Society Conference on HIV Science. TheBodyPro For the HIV/AIDS Workforce. Available online: https://www.thebodypro.com/article/ending-hiv-epidemic-equity-focused-approach (accessed on 30 November 2021).
- World Health Organization. Guidelines for Managing Advanced HIV Disease and Rapid Initiation of Antiretroviral Therapy. July 2017. Available online: https://www.who.int/publications/i/item/9789241550062 (accessed on 1 May 2022).
- Ter Tiero Elias Dah, I.Y.; Mensah, E.; Coulibaly, A.; Kouamé, J.B.; Traoré, I.; Mora, M.; Palvadeau, P.; Anoma, C.; Keita, B.D.; Spire, B.; et al. Rapid antiretroviral therapy initiation and its effect on treatment response in MSM in West Africa. AIDS 2021, 35, 2201. [Google Scholar]
- Ford, N.; Crawford, K.W.; Ameyan, W. Rapidly starting antiretroviral therapy to improve outcomes among disadvantaged groups. AIDS 2021, 35, 2217. [Google Scholar] [CrossRef]
- Gregori, N.; Renzetti, S.; Izzo, I.; Faletti, G.; Fumarola, B.; Degli Antoni, M.; Arsuffi, S.; Storti, S.; Tiecco, G.; Calza, S.; et al. Does Rapid Initiation of Antiretroviral Therapy At HIV Diagnosis Impact On Virological Response in a Real-Life Setting? A Single Cent. Exp. N. Italy 2021. Available online: https://www.researchsquare.com/article/rs-966688/v1 (accessed on 1 May 2022).
- Bacon, O.M.; Coffey, S.C.; Hsu, L.C.; Chin, J.C.; Havlir, D.V.; Buchbinder, S.P. Development of a Citywide Rapid Antiretroviral Therapy Initiative in San Francisco. Am. J. Prev. Med. 2021, 61, S47–S54. [Google Scholar] [CrossRef] [PubMed]
- Coffey, S.; Bacchetti, P.; Sachdev, D.; Bacon, O.; Jones, D.; Ospina-Norvell, C.; Torres, S.; Lynch, E.; Camp, C.; Mercer-Slomoff, R.; et al. RAPID antiretroviral therapy: High virologic suppression rates with immediate antiretroviral therapy initiation in a vulnerable urban clinic population. AIDS 2019, 33, 825. [Google Scholar] [CrossRef]
- O’Shea, J.G.; Gallini, J.W.; Cui, X.; Moanna, A.; Marconi, V.C. Rapid Antiretroviral Therapy Program: Development and Evaluation at a Veterans Affairs Medical Center in the Southern United States. AIDS Patient Care STDs 2022, 36, 219–225. [Google Scholar] [CrossRef]
- Ford, N.; Migone, C.; Calmy, A.; Kerschberger, B.; Kanters, S.; Nsanzimana, S.; Mills, E.J.; Meintjes, G.; Vitoria, M.; Doherty, M.; et al. Benefits and risks of rapid initiation of antiretroviral therapy. AIDS 2018, 32, 17. [Google Scholar] [CrossRef]
- Ford, N.; Geng, E.; Ellman, T.; Orrell, C.; Ehrenkranz, P.; Sikazwe, I.; Jahn, A.; Rabkin, M.; Ayisi Addo, S.; Grimsrud, A.; et al. Emerging priorities for HIV service delivery. PLoS Med. 2020, 17, e1003028. [Google Scholar] [CrossRef]
- Oben, P. Understanding the patient experience: A conceptual framework. J. Patient Exp. 2020, 7, 906–910. [Google Scholar] [CrossRef]
- Rand, L.; Dunn, M.; Slade, I.; Upadhyaya, S.; Sheehan, M. Understanding and using patient experiences as evidence in healthcare priority setting. Cost Eff. Resour. Alloc. 2019, 17, 20. [Google Scholar] [CrossRef]
- Deeks, E.D. Bictegravir/emtricitabine/tenofovir alafenamide: A review in HIV-1 infection. Drugs 2018, 78, 1817–1828. [Google Scholar] [CrossRef] [PubMed]
- Gilead Sciences Canada. Bictarvy. Product Monograph. 10 July 2018. Available online: https://pdf.hres.ca/dpd_pm/00046296.PDF (accessed on 30 November 2021).
- Rodriguez-Cruz, A.; Engler, K.; Kronfli, N.; Vicente, S.; Arora, A.; Lessard, D. A prospective cohort study examining two models of care to initiate an antiretroviral regimen suitable for rapid start in naïve newly referred HIV patients: The Antiretroviral Speed Access Program (ASAP) study protocol. BMJ Open 2022, in press. [Google Scholar]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef]
- Ritchie, J.; Spencer, L. Qualitative data analysis for applied policy research. In Analyzing Qualitative Data; Routledge: London, UK, 2002; pp. 187–208. [Google Scholar]
- Furber, C. Framework analysis: A method for analysing qualitative data. Afr. J. Midwifery Womens Health 2010, 4, 97–100. [Google Scholar] [CrossRef]
- Parkinson, S.; Eatough, V.; Holmes, J.; Stapley, E.; Midgley, N. Framework analysis: A worked example of a study exploring young people’s experiences of depression. Qual. Res. Psychol. 2016, 13, 109–129. [Google Scholar] [CrossRef] [Green Version]
- Kay, E.S.; Batey, D.S.; Mugavero, M.J. The HIV treatment cascade and care continuum: Updates, goals, and recommendations for the future. AIDS Res. Ther. 2016, 13, 1–7. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Safreed-Harmon, K.; Barton, S.E.; Costagliola, D.; Dedes, N.; Valero, J.D.A.; Gatell, J.M.; Baptista-Leite, R.; Mendão, L.; Porter, K.; et al. Beyond viral suppression of HIV–the new quality of life frontier. BMC Med. 2016, 14, 94. [Google Scholar] [CrossRef]
- Strategy for Patient-Oriented Research. Patient Engagement Framework. Canadian Institutes of Health Research. 2019. Available online: https://cihr-irsc.gc.ca/e/48413.html (accessed on 30 November 2021).
- Edelman, N.; Barron, D. Evaluation of public involvement in research: Time for a major re-think? J. Health Serv. Res. Policy 2016, 21, 209–211. [Google Scholar] [CrossRef]
- Joint United Nations Programme on HIV/AIDS. The Greater Involvement of People Living with HIV (GIPA). Policy Brief. 2007. Available online: https://data.unaids.org/pub/briefingnote/2007/jc1299_policy_brief_gipa.pdf (accessed on 30 November 2021).
- Rousseau, C.; Frounfelker, R.L. Mental health needs and services for migrants: An overview for primary care providers. J. Travel Med. 2019, 26, tay150. [Google Scholar] [CrossRef]
- Close, C.; Kouvonen, A.; Bosqui, T.; Patel, K.; O’Reilly, D.; Donnelly, M. The mental health and wellbeing of first generation migrants: A systematic-narrative review of reviews. Glob. Health 2016, 12, 47. [Google Scholar] [CrossRef]
- Kirmayer, L.J.; Narasiah, L.; Munoz, M.; Rashid, M.; Ryder, A.G.; Guzder, J.; Hassan, G.; Rousseau, C.; Pottie, K. Common mental health problems in immigrants and refugees: General approach in primary care. Can. Med. Assoc. J. 2010, 183, E959–E967. [Google Scholar] [CrossRef] [PubMed]
- Arora, A.; Adams, A.; Lebouché, B.; Quesnel-Vallée, A. Exploration of social and political factors that impede migrant healthcare availability and access in Canada amidst COVID-19. McGill J. Med. 2021, 19, 1–4. [Google Scholar] [CrossRef]
- Priebe, S.; Giacco, D.; El-Nagib, R. Public Health Aspects of Mental Health among Migrants and Refugees: A Review of the Evidence on Mental Health Care for Refugees, Asylum Seekers and Irregular Migrants in the WHO European Region; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Ridde, V.; Aho, J.; Ndao, E.M.; Benoit, M.; Hanley, J.; Lagrange, S.; Fillol, A.; Raynault, M.F.; Cloos, P. Unmet healthcare needs among migrants without medical insurance in Montreal, Canada. Glob. Public Health 2020, 15, 1603–1616. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.B.; Li, A.T.; Fung, K.P.; Wong, J.P. Improving access to mental health services for racialized immigrants, refugees, and non-status people living with HIV/AIDS. J. Health Care Poor Underserved 2015, 26, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.P.; Li, A.T.; Poon, M.K.; Fung, K.P. An exploratory study on the mental health of immigrants, refugees and non-status people living with HIV in Toronto. Int. J. Migr. Health Soc. Care 2013, 9, 122–134. [Google Scholar] [CrossRef]
- dela Cruz, A.M.; Maposa, S.; Patten, S.; Abdulmalik, I.; Magagula, P.; Mapfumo, S.; Abate, T.D.; Carter, A.; Spies, P.; Harrowing, J.; et al. “I die silently inside”. Qualitative findings from a study of people living with HIV who migrate to and settle in Canada. J. Migr. Health 2022, 5, 100088. [Google Scholar] [CrossRef]
- Vitale, A.; Ryde, J. Exploring risk factors affecting the mental health of refugee women living with HIV. Int. J. Environ. Res. Public Health 2018, 15, 2326. [Google Scholar] [CrossRef]
- Hacker, K.; Anies, M.; Folb, B.L.; Zallman, L. Barriers to health care for undocumented immigrants: A literature review. Risk Manag. Healthc. Policy 2015, 8, 175. [Google Scholar] [CrossRef]
- Kalich, A.; Heinemann, L.; Ghahari, S. A scoping review of immigrant experience of health care access barriers in Canada. J. Immigr. Minority Health 2016, 18, 697–709. [Google Scholar] [CrossRef]
- Asanin, J.; Wilson, K. “I spent nine years looking for a doctor”: Exploring access to health care among immigrants in Mississauga, Ontario, Canada. Soc. Sci. Med. 2008, 66, 1271–1283. [Google Scholar] [CrossRef]
- Lee, G.E.; Quesnel-Vallée, A. Improving access to family medicine in Québec through quotas and numerical targets. Health Reform. Obs. Obs. Des. Réformes St. 2019, 7, 1–12. [Google Scholar] [CrossRef]
- Pagkas-Bather, J.; Jaramillo, J.; Henry, J.; Grandberry, V.; Ramirez, L.F.; Cervantes, L.; Stekler, J.D.; Andrasik, M.P.; Graham, S.M. What’s PrEP?: Peer navigator acceptability among minority MSM in Washington. BMC Public Health 2020, 20, 248. [Google Scholar] [CrossRef] [PubMed]
- Pitpitan, E.V.; Mittal, M.L.; Smith, L.R. Perceived need and acceptability of a community-based peer navigator model to engage key populations in HIV care in Tijuana, Mexico. J. Int. Assoc. Provid. AIDS Care (JIAPAC) 2020, 19, 2325958220919276. [Google Scholar] [CrossRef] [PubMed]
- Flickinger, T.E.; Saha, S.; Roter, D.; Korthuis, P.T.; Sharp, V.; Cohn, J.; Moore, R.D.; Ingersoll, K.S.; Beach, M.C. Respecting patients is associated with more patient-centered communication behaviors in clinical encounters. Patient Educ. Couns. 2016, 99, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Flickinger, T.E.; Saha, S.; Roter, D.; Korthuis, P.T.; Sharp, V.; Cohn, J.; Eggly, S.; Moore, R.D.; Beach, M.C. Clinician empathy is associated with differences in patient–clinician communication behaviors and higher medication self-efficacy in HIV care. Patient Educ. Couns. 2016, 99, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Dapaah, J.M. Attitudes and behaviours of health workers and the use of HIV/AIDS health care services. Nurs. Res. Pract. 2016, 2016, 5172497. [Google Scholar] [CrossRef]
- Boyd, M.A.; Boffito, M.; Castagna, A.; Estrada, V. Rapid initiation of antiretroviral therapy at HIV diagnosis: Definition, process, knowledge gaps. HIV Med. 2019, 20, 3–11. [Google Scholar] [CrossRef]
- Dang, B.N.; Westbrook, R.A.; Njue, S.M.; Giordano, T.P. Building trust and rapport early in the new doctor-patient relationship: A longitudinal qualitative study. BMC Med. Educ. 2017, 17, 32. [Google Scholar] [CrossRef]
- Gona, C.M.; McGee, E.; DeMarco, R. “What Will Become of Me if They Take This Away? ” Zimbabwean Women’s Perceptions of “Free” ART” . J. Assoc. Nurses AIDS Care 2016, 27, 667–676. [Google Scholar] [CrossRef]
- Remien, R.H.; Bauman, L.J.; Mantell, J.; Tsoi, B.; Lopez-Rios, J.; Chhabra, R.; DiCarlo, A.; Watnick, D.; Rivera, A.; Teitelman, N.; et al. Barriers and facilitators to engagement of vulnerable populations in HIV primary care in New York City. J. Acquir. Immune Defic. Syndr. (1999) 2015, 69, S16. [Google Scholar] [CrossRef]
- Sherer, R.; Stieglitz, K.; Narra, J.; Jasek, J.; Green, L.; Moore, B.; Shott, S.; Cohen, M. HIV multidisciplinary teams work: Support services improve access to and retention in HIV primary care. AIDS Care 2002, 14, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Soto, T.A.; Bell, J.; Pillen, M.B. For The Hiv/aids Treatment Adherence, Health Outcomes And Cost Study Group. Literature on integrated HIV care: A review. AIDS Care 2004, 16, 43–55. [Google Scholar] [CrossRef]
- Elgalib, A.; Al-Sawafi, H.; Kamble, B.; Al-Harthy, S.; Al-Sariri, Q. Multidisciplinary care model for HIV improves treatment outcome: A single-centre experience from the Middle East. AIDS Care 2018, 30, 1114–1119. [Google Scholar] [CrossRef] [PubMed]
- Melvin, S.C.; Gipson, J. Peer Reviewed: The Open Arms Healthcare Center’s Integrated HIV Care Services Model. Prev. Chronic Dis. 2019, 16, E135. [Google Scholar] [CrossRef] [PubMed]
- Tadic, V.; Ashcroft, R.; Brown, J.B.; Dahrouge, S. The role of social workers in interprofessional primary healthcare teams. Healthc. Policy 2020, 16, 27. [Google Scholar] [CrossRef]
- Fraser, M.W.; Lombardi, B.M.; Wu, S.; de Saxe Zerden, L.; Richman, E.L.; Fraher, E.P. Integrated primary care and social work: A systematic review. J. Soc. Soc. Work. Res. 2018, 9, 175–215. [Google Scholar] [CrossRef]
- Ashcroft, R.; McMillan, C.; Ambrose-Miller, W.; McKee, R.; Brown, J.B. The emerging role of social work in primary health care: A survey of social workers in Ontario family health teams. Health Soc. Work. 2018, 43, 109–117. [Google Scholar]
- Zelnick, J.R.; Seepamore, B.; Daftary, A.; Amico, K.R.; Bhengu, X.; Friedland, G.; Padayatchi, N.; Naidoo, K.; O’Donnell, M.R. Training social workers to enhance patient-centered care for drug-resistant TB-HIV in South Africa. Public Health Action 2018, 8, 25–27. [Google Scholar] [CrossRef]
- Wolf, M.S.; Mitchell, C.G. Preparing social workers to address HIV/AIDS prevention and detection: Implications for professional training and education. J. Commun. Health 2002, 27, 165–180. [Google Scholar] [CrossRef]
- Grimsrud, A.; Wilkinson, L.; Eshun-Wilson, I.; Holmes, C.; Sikazwe, I.; Katz, I.T. Understanding engagement in HIV programmes: How health services can adapt to ensure no one is left behind. Curr. HIV/AIDS Rep. 2020, 17, 458–466. [Google Scholar] [CrossRef]
- Mgbako, O.; Miller, E.H.; Santoro, A.F.; Remien, R.H.; Shalev, N.; Olender, S.; Gordon, P.; Sobieszczyk, M.E. COVID-19, telemedicine, and patient empowerment in HIV care and research. AIDS Behav. 2020, 24, 1990–1993. [Google Scholar] [CrossRef] [PubMed]
- Mutchler, M.G.; Wagner, G.; Cowgill, B.O.; McKay, T.; Risley, B.; Bogart, L.M. Improving HIV/AIDS care through treatment advocacy: Going beyond client education to empowerment by facilitating client–provider relationships. AIDS Care 2011, 23, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Brondani, M.; Moniri, N.R.; Kerston, R.P. Community-based research among marginalized HIV populations: Issues of support, resources, and empowerment. Interdiscip. Perspect. Infect. Dis. 2012, 2012, 601027. [Google Scholar] [CrossRef] [PubMed]
- Robert, E.; David, P.M. “Healthcare as a refuge”: Building a culture of care in Montreal for refugees and asylum-seekers living with HIV. Int. J. Hum. Rights Healthc. 2018, 12, 16–27. [Google Scholar] [CrossRef]
- Eklund, J.H.; Holmström, I.K.; Kumlin, T.; Kaminsky, E.; Skoglund, K.; Höglander, J.; Sundler, A.J.; Condén, E.; Meranius, M.S. “Same same or different?” A review of reviews of person-centered and patient-centered care. Patient Educ. Couns. 2019, 102, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Greene, S.M.; Tuzzio, L.; Cherkin, D. A framework for making patient-centered care front and center. Perm. J. 2012, 16, 49. [Google Scholar] [CrossRef] [Green Version]
- Raker, A.R.; Feldman, M.B.; Hile, S.J.; Chandraratna, S. Positive side effects: The perceived health and psychosocial benefits of delivering an HIV self-management program for peer educators living with HIV. J. Assoc. Nurses AIDS Care 2020, 31, 517–525. [Google Scholar] [CrossRef]
- Millard, T.; Elliott, J.; Girdler, S. Self-management education programs for people living with HIV/AIDS: A systematic review. AIDS Patient Care STDs 2013, 27, 103–113. [Google Scholar] [CrossRef]
- Areri, H.A.; Marshall, A.; Harvey, G. Interventions to improve self-management of adults living with HIV on antiretroviral therapy: A systematic review. PLoS ONE 2020, 15, e0232709. [Google Scholar] [CrossRef]
- Eisinger, R.W.; Dieffenbach, C.W.; Fauci, A.S. HIV viral load and transmissibility of HIV infection: Undetectable equals untransmittable. JAMA 2019, 321, 451–452. [Google Scholar] [CrossRef]
- Nair, M.; Kumar, P.; Pandey, S.; Kazmi, S.; Moreto-Planas, L.; Ranjan, A.; Burza, S. Quality of life perceptions amongst patients co-infected with Visceral Leishmaniasis and HIV: A qualitative study from Bihar, India. PLoS ONE 2020, 15, e0227911. [Google Scholar] [CrossRef] [PubMed]
- Arora, A.K.; Lessard, D.; Dubé, K.; Lebouché, B. It’s Time to Embed Health-related Quality of Life across all Steps of the HIV Care Cascade. JAIDS J. Acquir. Immune Defic. Syndr. 2022. [Google Scholar] [CrossRef]
- Brashers, D.E.; Neidig, J.L.; Goldsmith, D.J. Social support and the management of uncertainty for people living with HIV or AIDS. Health Commun. 2004, 16, 305–331. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.L.; Ballivian, J.; Rodriguez, V.J.; Uribe, C.; Cecchini, D.; Salazar, A.S.; Cassetti, I.; Alcaide, M.L. Mental health, coping, and social support among people living with HIV in the Americas: A comparative study between Argentina and the USA during the SARS-CoV-2 pandemic. AIDS Behav. 2021, 25, 2391–2399. [Google Scholar] [CrossRef] [PubMed]
- Mendez, K.J.; Cudjoe, J.; Strohmayer, S.; Han, H.R. Recruitment and retention of women living with HIV for clinical research: A review. AIDS Behav. 2021, 25, 3267–3278. [Google Scholar] [CrossRef]
- Lebrun, L.A. Effects of length of stay and language proficiency on health care experiences among immigrants in Canada and the United States. Soc. Sci. Med. 2012, 74, 1062–1072. [Google Scholar] [CrossRef]


{kind=link}
| Participant # | Age | Sex | Sexual Orientation | Region of Birth | Immigration Status | Health Coverage | Education | Paid Employment Status | Interviews Completed | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Week 1 | Week 24 | Week 48 | |||||||||
| 1 | 41–50 | Male | Heterosexual | East Asia | Visitor | No or Low Coverage | College/CEGEP/Technical Degree | Unemployed |  | | |
| 2 | 21–30 | Male | Bisexual | East Africa | International Student | No or Low Coverage | University | Unemployed | | | |
| 3 | 21–30 | Female | Heterosexual | Southern Africa | Asylum Seeker | Sufficient | University | Paid Employment | | | |
| 4 | 51–60 | Female | Heterosexual | Southern Africa | Asylum Seeker | Sufficient | College/CEGEP/ Technical Degree | Unemployed | | | |
| 5 | 41–50 | Male | Homosexual | Southeast Asia | Asylum Seeker | Sufficient | University | Unemployed | | |  |
| 6 | 21–30 | Male | Homosexual | North Africa | International Student | No or Low Coverage | University | Unemployed | | | |
| 7 | 31–40 | Male | Homosexual | Latin America | Asylum Seeker | Sufficient | College/CEGEP/Technical Degree | Paid Employment | | | |
| 8 | 21–30 | Male | Bisexual | North Africa | Temporary Worker | No or Low Coverage | University | Paid Employment | | | |
| 9 | 31–40 | Male | Bisexual | Southern Africa | Asylum Seeker | Sufficient | University | Paid Employment | | | |
| 10 | 21–30 | Male | Homosexual | Latin America | No Status | No or Low Coverage | University | Paid Employment | | | |
| 11 | 41–50 | Male | Homosexual | Latin America | Visitor | Sufficient | University | Unemployed | | | |
| 12 | 21–30 | Male | Homosexual | East Asia | International Student | No or Low Coverage | Secondary/Professional Degree | Paid Employment | | | |
| 13 | 21–30 | Male | Homosexual | Southeast Asia | Visitor | No or Low Coverage | Secondary/Professional Degree | Unemployed | | | |
| 14 | 21–30 | Male | Heterosexual | Caribbean | Asylum Seeker | Sufficient | College/CEGEP/Technical Degree | Unemployed | | | |
| 15 | 51–60 | Male | Homosexual | Western Europe | Naturalized Citizen | Sufficient | University | Unemployed | | | |
| 16 | 31–40 | Male | Heterosexual | Caribbean | Asylum Seeker | Sufficient | University | Unemployed | | | |
| Category | Illustrative Excerpt | Contributing Participants (n/16) | Contributing Interviews (n/32) |
|---|---|---|---|
| HIV Diagnosis | |||
| Initially experiencing distress Feeling:
| “I could not believe it. I came [to Canada] with hopes, I had a dream. And I did not believe it […] I blacked out.” Participant #5, W1 | 10 7 6 6 4 | 14 8 7 6 4 |
| Questioning the impact of HIV diagnosis on immigration | “I was very concerned about how the diagnosis might impact my permanent residency process. I thought I had to go back to my country.” [Translated from French]—Participant #8, W1 | 6 | 6 |
| Fearing stigmatization (from clinicians, family, friends, and/or community members) | “I just worried about [how] to tell people around me, for the first thing.”—Participant #30, W1 | 4 | 5 |
| Uncertainty about HIV testing requirements for migrants | “Normally, the work permit does not require a medical visit. […] It was not mandatory to have a medical examination. Me, I wanted to do [the examination] for if I find a volunteer [position] in a hospital [so] I can work without any problem…” [Translated from French]—Participant #6, W1 | 3 | 3 |
| Linkage to HIV Care | |||
Facing psychosocial challenges beyond HIV
| “I feel dreaded, maybe I wasn’t eating well. I was worrying about so many things that, so many financial challenges there… I haven’t seen doctors for months, years maybe, because I don’t [have] insurance or anything and I couldn’t afford it.”—Participant #4, W48 | 12 11 8 6 4 | 23 16 10 10 4 |
Navigating the health system with difficulty
| “You have to understand as a foreigner […] for all the [health] system running in North America, I have no clue, no idea … And then the language problem as well, ok … Because especially for me, I’m a foreigner. I don’t know the procedure [for accessing care] or the round, you know.”—Participant #1, W1 | 15 15 9 | 21 20 12 |
| Humanizing clinical encounters Feeling:
| “[The care I received] was perfect, I felt loved, cared for. I felt understood, for the first time. Everything that happened to me was not planned. I did not have a plan to take care of this. Then, when I arrived here, I had it, I had a plan. I met Dr. [name omitted] and the other people and they told me it was important to start care, and they told me how it would happen. I never felt any safer than I felt around these people. I felt helped […]”—Participant #4, W1 | 14 12 10 7 5 3 | 19 15 12 7 6 3 |
| Being reassured about living with HIV | “Well, before I had misinformation, bad ideas about this disease. But when I came to the hospital, [the health professionals] calmed me down. They said to me, ‘There’s nothing to worry about. It’s just that you’re going to have treatment and then you’re going to be fine and you’re going to live your normal life.’ With their behavior, how they talk to me, all that was good. I left the clinic really happy. […] There was a big difference between how I entered the clinic and when I left the clinic.” [Translated from French]—Participant #6, W1 | 12 | 19 |
| Receiving personalized health information | “And also, I’m always asking like: ‘My blood pressure, is that a good thing?’ And they are like: ‘Yeah, yeah, that’s good.’ And I always have questions and they answer very well … Because it’s not like, you know when you ask a question and then somebody gives you one answer one way. No, they actually explain.”—Participant #3, W1 | 13 | 17 |
| Quickly accessing care | “In fact, it went very quickly, I received a call telling me that I had to show up here. I was given the news and it was very difficult to take at that time. But very quickly, I think the next day or two, I had an appointment. And I met everyone, the social worker, the nurse, the doctor.” [Translated from French]—Participant #2, W24 | 10 | 12 |
| Treatment Initiation | |||
| Being satisfied with treatment Due to:
| “The medicine is really good, it’s really great because I don’t feel bad at all. I feel fine, no pain, nothing.” [Translated from French]—Participant #14, W1 | 15 11 7 7 6 6 3 3 | 18 11 8 7 7 6 4 4 |
Having concerns with starting treatment
| “[Starting treatment] was a hard decision because [when] you start, you cannot stop to take [the treatment]. But you cannot avoid the situation, you have to take it. So, you have no choice. So, personally it’s hard because I like to choose everything that I do but, in this case, I don’t have any option.”—Participant #7, W1 | 11 8 5 | 15 9 8 |
| Needing reassurance about treatment safety | “The only thing for me is dizzy[ness]. Especially for the first day … So, I talked [about] this to Dr. [name omitted] again. He said: ‘The body needs time for the medication.’ So, it’s have to be take time.”—Participant #1, W1 | 8 | 13 |
| Dissipating side effects over time | “Well the first 2 days I was in a lot of pain. I think, like, my body was getting used to it, but I was really nauseous. And I had nightmares. A lot. […] it was intense at first, but now it’s okay.” [Translated from French]—Participant #2, W1 | 7 | 7 |
| Retention in Care | |||
Facing psychosocial or health-related challenges beyond HIV
| “Yeah, not having enough money, that is a barrier. So, I couldn’t even go, if I wanted to go get some fruit or something, the money would challenge me. I would just stay and do with whatever I had. […] Financially, if there is some organizations that can help give you something like a coupon to go get some food at [the grocery store], whatever, I would welcome that. But I don’t have that kind of access.”—Participant #4, W48 | 16 12 12 12 13 11 8 | 31 22 20 18 17 13 12 |
Feeling empowered to self-manage HIV
| “I got control of my health. So, if I come here then I understand: ‘Ok, my CD4 count is 715.’ Then I know: ‘Ok, now I know that [I’m] ok. I’m a step ahead. My health is excellent, so I have to maintain it.’ And what is CD4 count? That’s what I’m going on Google. On Google ‘what is CD4 count’. Then I know: ‘Ok. These are the white blood cells and bla, bla, bla. And what is viral load?’ That’s how I do it. So, yeah, I feel good about it. I feel like I’ve got control of my health.”—Participant #9, W48 | 15 13 13 6 | 31 29 21 6 |
Humanizing clinical encounters
| “I think I like the attitude of the staff. You know, they’re always like happy and excited to see you and talk and listen. It’s more like they’re concern[ed] about, you know, for you as a person not just like as in a patient. Ok, you know, looking at the time. It’s not like that. It’s like they have time for you. I think that’s really good because, you know, you don’t feel like you’re inconveniencing people or anything like that. So, that makes me look forward to the visits and also all the questions I have, they get answered and they get explanations. Because naturally, I’m anxious on my health questions and things, and I always get them answered.”—Participant #3, W24 | 12 9 10 10 7 8 7 | 25 21 20 15 14 12 9 |
Enjoying smooth operations in the clinic
| “Personally, I find that the system you have adopted, especially for follow-ups with foreigners without [provincial health insurance], is really effective. […] And I also like the fact that the main person I come into contact with is either [the study coordinator] or [their HIV physician] only because they are the main people that are directly related to care, and who I think are, for this team, the main players in what you call caregivers. I like the format that even if I know there are people who are ‘back-up’ like social workers or nurses, there are still only two people who come into contact with me. Because, from the moment there are too many people who intervene, it is more difficult to manage, you see. And I think that precisely for a patient, it is not what he would want that there are too many things to do. I think that’s just like enough for it to be effective…” [Translated from French]—Participant #2, W48 | 11 9 8 8 7 4 | 23 16 14 14 8 4 |
| Receiving holistic care | “[The healthcare professionals] have different responsibilities because, you know, they all have different experience in their professions. So, like, for example, I have a social worker who can help me like: ‘Oh, you can go to this if you need food, there are food banks or this, this.’ And then, the doctor will tell you about like, you know, what questions I have about health and that’s good. So, it’s like they both have different… Everybody has their own [role]. Just like, you know, how the body like the head has its function and the hands has its function, I feel like it’s like that. And then together they make like a complete.”—Participant #3, W48 | 12 | 20 |
Wanting more frequent contact with healthcare professionals
| “I know that you guys are busy but maybe when I go after a month or so, just text, email: ‘How is everything?’, whatever. It would also add more to my confidence as well, knowing there are people out there.”—Participant #4, W48 | 11 10 4 4 4 | 20 16 6 6 5 |
| Dealing with HIV-related psychological distress | “Taking medication is important to physical health, but my social and mental health is still not good.”—Participant #5, W24 | 11 | 17 |
Sharing responsibility to manage HIV
| “I feel 100% responsible. I’m on top of my game. I’m doing what’s right. I don’t forget. I don’t need an alarm, my brain I programmed it. It’s [a] mindset […] [The healthcare professionals are] 200% plus responsible for all this, yes. They’ve helped me a lot in achieving [undetectability], brought my confidence […] Everybody, the whole team involved in this, I appreciate what they have done. They have made me feel comfortable. They’ve never made me feel any different. Like I’m when I walk in, I’m like I’m coming home. So, this has really driven me to commit to it. If I [was] feeling judged or didn’t feel wanted, or looked at in a different way I wouldn’t have committed. So, they’ve helped a lot.”—Participant #4, W48 | 9 9 8 | 9 9 8 |
| Adherence to Treatment | |||
| Being satisfied with treatment Due to:
| “Oh, yeah, yeah, yeah! Absolutely! Yeah, there are a lot of changes. I feel energetic. I don’t feel that fatigued. I feel confident. I see life with HIV. So, yeah definitely things, they have changed […] on the psychological side, it’s been so positive […] now I feel much better. My emotions they’re not as how they were before. So, yeah, I feel much better […] now I feel more calm. I feel like I’m at the right place. I’m getting the right treatment…”—Participant #9, W24 | 11 8 7 6 6 5 4 4 | 23 14 10 9 7 7 5 5 |
Feeling resilient and responsible
| “I quickly got into the habit of taking [my HIV medication] because that’s what I can do to keep my partner healthy and safe. So I take it and for me it’s positive, it allows me to keep discipline and control over what’s going on. […] I don’t think I forget, or else it happens very rarely […] Then too, there is my discipline. I’m studying and working, so I can’t, I don’t have time to think about it, I maintain my discipline and I take my medicine and go to consultations, and the team is there for me too. So I don’t think about the disease anymore, I do what I have to do and I don’t have to think about it. It’s just a routine for me.” [Translated from French]—Participant #2, W24 | 11 6 4 | 18 8 4 |
| Viral Suppression | |||
| Finding more peace of mind since becoming undetectable | “Now it’s more quiet like more relaxed […] It’s like less anxiety […] Because now I know I’m undetectable so, it makes me feel like: ‘Ok, you are doing it well. It’s part of your routine. So, you are like well disciplined. So, you are doing something good for yourself.’ So, it’s a big difference. Like when I start, I was scared like: ‘Oh, maybe I’m not capable but I have to do it. I need to try it.’ And now I know I’m capable so it’s like: ‘Ok. It’s a really, really big change.’”—Participant #7, W24 | 5 | 6 |
| Perceived Health-related Quality of Life | |||
| Being helped by a supportive social network | “Everyone around me just like told me to live a stronger and don’t think so much. They always support me […] Because I have a few close friends that I [can] talk [with]. Yeah, so everyone like [comforts] me and yeah, excepts [me].”—Participant #13, W1 | 12 | 16 |
Deciding to improve lifestyle habits since diagnosis
| “My quality of life is getting better because now I’m conscious. I was living carelessly and I cannot do it anymore. So it will improve my quality of life. This is a lifetime process and I need to make changes. I am reading books and information to know if I eat right so my immune system is helping me. I know this is all for the better.”—Participant #4, W24 | 9 7 7 5 5 | 15 10 8 7 6 |
| Wanting a long, healthy, and normal life | “I hope to be healthy and be able to live normal. I still have my hopes and dreams and I hope that the treatment will help me achieve them. I just wanna be healthy and normal. I don’t ask for [more] benefits.”—Participant #5, W1 | 11 | 14 |
| Feeling better physically and mentally since starting care and treatment | “In fact, everything that I had a problem with related to my physical health was related to the virus. […] Because I was diagnosed, I think, a little too late. […] so when I started taking the medicine, well all those little things that were bothering me [with] my physical health went away. So inevitably my mental health has improved […]” [Translated from French]—Participant #8, W48 | 8 | 15 |
| Fostering quality-of-life through activities | “I think I have a good quality of life. I work. I pay more attention to what I miss. I exercise. I run three times a week. I think I improved on that.” [Translated from French]—Participant #2, W24 | 7 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arora, A.K.; Engler, K.; Lessard, D.; Kronfli, N.; Rodriguez-Cruz, A.; Huerta, E.; Lemire, B.; Routy, J.-P.; Wittmer, R.; Cox, J.; et al. Experiences of Migrant People Living with HIV in a Multidisciplinary HIV Care Setting with Rapid B/F/TAF Initiation and Cost-Covered Treatment: The ‘ASAP’ Study. J. Pers. Med. 2022, 12, 1497. https://doi.org/10.3390/jpm12091497
Arora AK, Engler K, Lessard D, Kronfli N, Rodriguez-Cruz A, Huerta E, Lemire B, Routy J-P, Wittmer R, Cox J, et al. Experiences of Migrant People Living with HIV in a Multidisciplinary HIV Care Setting with Rapid B/F/TAF Initiation and Cost-Covered Treatment: The ‘ASAP’ Study. Journal of Personalized Medicine. 2022; 12(9):1497. https://doi.org/10.3390/jpm12091497
Chicago/Turabian StyleArora, Anish K., Kim Engler, David Lessard, Nadine Kronfli, Adriana Rodriguez-Cruz, Edmundo Huerta, Benoit Lemire, Jean-Pierre Routy, René Wittmer, Joseph Cox, and et al. 2022. "Experiences of Migrant People Living with HIV in a Multidisciplinary HIV Care Setting with Rapid B/F/TAF Initiation and Cost-Covered Treatment: The ‘ASAP’ Study" Journal of Personalized Medicine 12, no. 9: 1497. https://doi.org/10.3390/jpm12091497