
Effects of Pelvic-Floor Muscle Training in Patients with Pelvic Organ Prolapse Approached with Surgery vs. Conservative Treatment: A Systematic Review

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
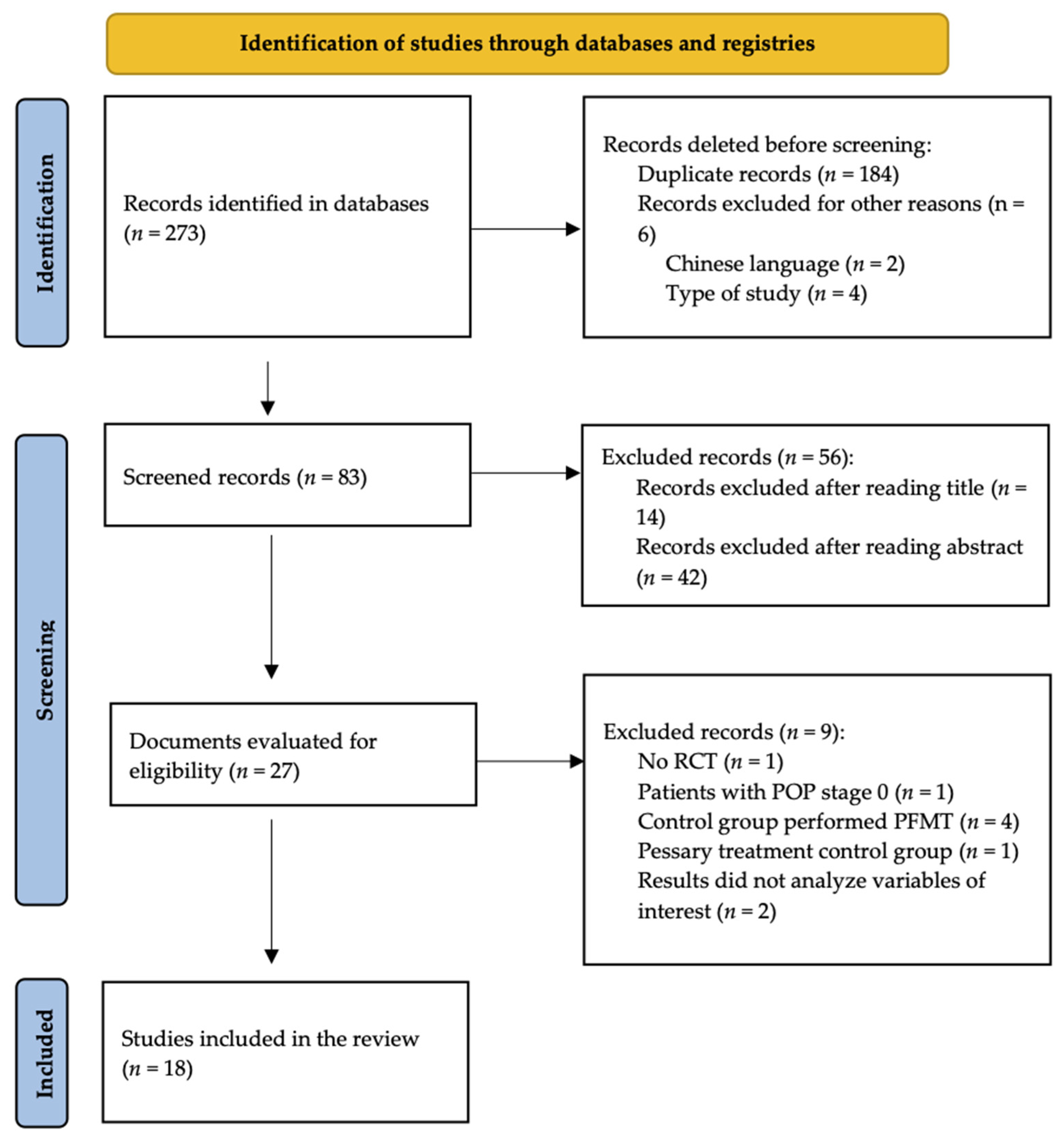
2.4. Study Selection
2.5. Methodological Quality Assessment
3. Results
3.1. POP-Q
3.2. Pelvic-Floor Distress Inventory (PFDI-20) and Subscales
3.3. POP-SS
3.4. Sexual Function (PISQ-12 and Specific Questionnaire)
3.5. Pelvic-Floor Function by Manual Assessment, EMG, or Manometry
3.6. Quality of Life (P-QOL, ICIQ-VS, PFIQ-7, and Subscales)
3.7. Impression of Global Improvement in Patients and Change in Symptoms Reported by Patients
3.8. Surgery vs. Surgery + PFMT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weintraub, A.Y.; Glinter, H.; Marcus-Braun, N. Narrative review of the epidemiology, diagnosis and pathophysiology of pelvic organ prolapse. Int. Braz. J. Urol. 2020, 46, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Doaee, M.; Moradi-Lakeh, M.; Nourmohammadi, A.; Razavi-Ratki, S.K.; Nojomi, M. Management of pelvic organ prolapse and quality of life: A systematic review and meta-analysis. Int. Urogynecology J. 2013, 25, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Pahernik, S.; Pandey, A. Pelvic organ prolapse. J. Urol. Urogynakologie 2019, 26, 87–91. [Google Scholar] [CrossRef]
- Haya, N.; Feiner, B.; Baessler, K.; Christmann-Schmid, C.; Maher, C. Perioperative interventions in pelvic organ prolapse surgery. Cochrane Database Syst. Rev. 2018, 2018, CD013105. [Google Scholar] [CrossRef] [PubMed]
- Madhu, C.; Swift, S.; Moloney-Geany, S.; Drake, M.J. How to use the Pelvic Organ Prolapse Quantification (POP-Q) system? Neurourol. Urodyn. 2018, 37, S39–S43. [Google Scholar] [CrossRef] [Green Version]
- Fleischer, K.; Thiagamoorthy, G. Pelvic organ prolapse management. Post Reprod. Health 2020, 26, 79–85. [Google Scholar] [CrossRef]
- Vergeldt, T.F.M.; Weemhoff, M.; IntHout, J.; Kluivers, K.B. Risk factors for pelvic organ prolapse and its recurrence: A systematic review. Int. Urogynecology J. 2015, 26, 1559–1573. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Gong, Y.; Wang, B. The efficacy of pelvic floor muscle training for pelvic organ prolapse: A systematic review and meta-analysis. Int. Urogynecology J. 2015, 27, 981–992. [Google Scholar] [CrossRef]
- Hagen, S.; Stark, D. Conservative prevention and management of pelvic organ prolapse in women. Cochrane Database Syst. Rev. 2011, 2011, CD003882. [Google Scholar] [CrossRef]
- Tso, C.; Lee, W.; Austin-Ketch, T.; Winkler, H.; Zitkus, B. Nonsurgical Treatment Options for Women with Pelvic Organ Prolapse. Nurs. Women’s Health 2018, 22, 228–239. [Google Scholar] [CrossRef]
- Sociedad Española De Ginecología y Obstetricia. Prolapso de los órganos pélvicos. Progresos Obstet. Ginecol. 2020, 63, 54–59. [Google Scholar]
- Wiegersma, M.; Panman, C.M.C.R.; Hesselink, L.C.; Malmberg, A.G.; Berger, M.Y.; Kollen, B.J.; Dekker, J.H. Predictors of Success for Pelvic Floor Muscle Training in Pelvic Organ Prolapse. Phys. Ther. 2018, 99, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Giagio, S.; Innocenti, T.; Salvioli, S.; Lami, A.; Meriggiola, M.C.; Pillastrini, P.; Gava, G. Completeness of exercise reporting among randomized controlled trials on pelvic floor muscle training for women with pelvic organ prolapse: A systematic review. Neurourol. Urodyn. 2021, 40, 1424–1432. [Google Scholar] [CrossRef] [PubMed]
- Hagen, S.; Glazener, C.; McClurg, D.; Macarthur, C.; Elders, A.; Herbison, G.P.; Wilson, D.; Toozs-Hobson, P.; Hemming, C.; Hay-Smith, J.; et al. Pelvic floor muscle training for secondary prevention of pelvic organ prolapse (PREVPROL): A multicentre randomised controlled trial. Lancet 2016, 389, 393–402. [Google Scholar] [CrossRef] [Green Version]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Alves, F.K.; Riccetto, C.; Adami, D.B.; Marques, J.; Pereira, L.C.; Palma, P.; Botelho, S. A pelvic floor muscle training program in postmenopausal women: A randomized controlled trial. Maturitas 2015, 81, 300–305. [Google Scholar] [CrossRef]
- Resende, A.P.M.; Stüpp, L.; Bernardes, B.T.; Oliveira, E.; Castro, R.A.; Girão, M.J.B.C.; Sartori, M.G.F. Can hypopressive exercises provide additional benefits to pelvic floor muscle training in women with pelvic organ prolapse? Neurourol. Urodyn. 2012, 31, 121–125. [Google Scholar] [CrossRef]
- Brækken, I.H.; Majida, M.; Engh, M.E.; Bø, K. Can Pelvic Floor Muscle Training Improve Sexual Function in Women with Pelvic Organ Prolapse? A Randomized Controlled Trial. J. Sex. Med. 2015, 12, 470–480. [Google Scholar] [CrossRef]
- Wiegersma, M.; Panman, C.M.C.R.; Kollen, B.J.; Berger, M.Y.; Lisman-Van Leeuwen, Y.; Dekker, J.H. Effect of pelvic floor muscle training compared with watchful waiting in older women with symptomatic mild pelvic organ prolapse: Randomised controlled trial in primary care. BMJ 2014, 349, g7378. [Google Scholar] [CrossRef] [Green Version]
- Hagen, S.; Stark, D.; Glazener, C.; Dickson, S.; Barry, S.J.; Elders, A.; Frawley, H.; Galea, M.; Logan, J.; McDonald, A.; et al. Individualised pelvic floor muscle training in women with pelvic organ prolapse (POPPY): A multicentre randomised controlled trial. Lancet 2014, 383, 796–806. [Google Scholar] [CrossRef] [Green Version]
- Due, U.; Brostrøm, S.; Lose, G. Lifestyle advice with or without pelvic floor muscle training for pelvic organ prolapse: A randomized controlled trial. Int. Urogynecology J. 2015, 27, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Stuepp, L.; Resende, A.P.M.; Oliveira, E.; Castro, R.; Girão, M.J.B.C.; Sartori, M.G.F. Pelvic floor muscle training for treatment of pelvic organ prolapse: An assessor-blinded randomized controlled trial. Int. Urogynecol. J. 2011, 22, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Due, U.; Brostrøm, S.; Lose, G. The 12-month effects of structured lifestyle advice and pelvic floor muscle training for pelvic organ prolapse. Acta Obstet. Gynecol. Scand. 2016, 95, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Panman, C.M.; Wiegersma, M.; Kollen, B.J.; Berger, M.Y.; Leeuwen, Y.L.; Vermeulen, K.M.; Dekker, J.H. Two-year effects and cost-effectiveness of pelvic floor muscle training in mild pelvic organ prolapse: A randomised controlled trial in primary care. BJOG Int. J. Obstet. Gynaecol. 2016, 124, 511–520. [Google Scholar] [CrossRef]
- Barber, M.D.; Brubaker, L.; Burgio, K.L.; Richter, H.; Nygaard, I.; Weidner, A.C.; Menefee, S.A.; Lukacz, E.S.; Norton, P.; Schaffer, J.; et al. Comparison of 2 Transvaginal Surgical Approaches and Perioperative Behavioral Therapy for Apical Vaginal Prolapse: The OPTIMAL randomized trial. JAMA 2014, 311, 1023–1034. [Google Scholar] [CrossRef]
- Liang, Y.; Li, X.; Wang, J.; Liu, Y.; Yang, Y.; Dong, M. Effect of Pelvic Floor Muscle Training on Improving Prolapse-related Symptoms After Surgery. J. Nurse Pr. 2019, 15, 600–605. [Google Scholar] [CrossRef]
- Nyhus, M.; Mathew, S.; Salvesen, K.; Stafne, S.; Volløyhaug, I. Effect of preoperative pelvic floor muscle training on pelvic floor muscle contraction and symptomatic and anatomical pelvic organ prolapse after surgery: Randomized controlled trial. Ultrasound Obstet. Gynecol. 2020, 56, 28–36. [Google Scholar] [CrossRef]
- Jelovsek, J.E.; Barber, M.D.; Brubaker, L.; Norton, P.; Gantz, M.; Richter, H.; Weidner, A.; Menefee, S.; Schaffer, J.; Pugh, N.; et al. Effect of Uterosacral Ligament Suspension vs Sacrospinous Ligament Fixation With or Without Perioperative Behavioral Therapy for Pelvic Organ Vaginal Prolapse on Surgical Outcomes and Prolapse Symptoms at 5 Years in the OPTIMAL Randomized Clinical Trial. JAMA 2018, 319, 1554–1565. [Google Scholar] [CrossRef]
- Weidner, A.C.; Barber, M.D.; Markland, A.; Rahn, D.D.; Hsu, Y.; Mueller, E.R.; Jakus-Waldman, S.; Dyer, K.Y.; Warren, L.K.; Gantz, M.G.; et al. Perioperative Behavioral Therapy and Pelvic Muscle Strengthening Do Not Enhance Quality of Life After Pelvic Surgery: Secondary Report of a Randomized Controlled Trial. Phys. Ther. 2017, 97, 1075–1083. [Google Scholar] [CrossRef]
- Duarte, T.B.; Bø, K.; Brito, L.G.; Bueno, S.M.; Barcelos, T.; Bonacin, M.; Ferreira, C.H. Perioperative pelvic floor muscle training did not improve outcomes in women undergoing pelvic organ prolapse surgery: A randomised trial. J. Physiother. 2019, 66, 27–32. [Google Scholar] [CrossRef]
- Mathew, S.; Nyhus, M.; Salvesen, K.; Stafne, S.N.; Volløyhaug, I. The effect of preoperative pelvic floor muscle training on urinary and colorectal-anal distress in women undergoing pelvic organ prolapse surgery—A randomized controlled trial. Int. Urogynecology J. 2021, 32, 2787–2794. [Google Scholar] [CrossRef] [PubMed]
- McClurg, D.; Hilton, P.; Dolan, L.; Monga, A.; Hagen, S.; Frawley, H.; Dickinson, L. Pelvic floor muscle training as an adjunct to prolapse surgery: A randomised feasibility study. Int. Urogynecology J. 2014, 25, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moser, H.; Luginbuehl, H.; Baeyens, J.-P.; Radlinger, L. Reliability and validity of pelvic floor muscle displacement measurements during voluntary contractions. Int. Urogynecology J. 2019, 30, 2093–2100. [Google Scholar] [CrossRef] [PubMed]
- Frawley, H.C.; Galea, M.; Phillips, B.A.; Sherburn, M.; Bø, K. Effect of test position on pelvic floor muscle assessment. Int. Urogynecology J. 2005, 17, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.-W.; Wei, F.; Wang, H.-L.; Pan, Y.-Q.; Zhen, J.-Y.; Zhang, J.-X.; Yang, K.-H. Does pelvic floor muscle training augment the effect of surgery in women with pelvic organ prolapse? A systematic review of randomized controlled trials. Neurourol. Urodyn. 2015, 35, 666–674. [Google Scholar] [CrossRef]
- Ge, J.; Wei, X.; Zhang, H.; Fang, G. Pelvic floor muscle training in the treatment of pelvic organ prolapse: A meta-analysis of randomized controlled trials. Actas Urol. Esp. 2020, 45, 73–82. [Google Scholar] [CrossRef]
- Kashyap, R.; Jain, V.; Singh, A. Comparative effect of 2 packages of pelvic floor muscle training on the clinical course of stage I-III pelvic organ prolapse. Int. J. Gynecol. Obstet. 2013, 121, 69–73. [Google Scholar] [CrossRef]
- Mastwyk, S.; McClelland, J.; Rosamilia, A.; Frawley, H. The impact of pelvic organ prolapse and/or continence surgery on pelvic floor muscle function in women: A systematic review. Neurourol. Urodyn. 2019, 38, 1467–1481. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Database | Search Strategy |
|---|---|
| PubMed | ((“Pelvic Organ Prolapse” [Mesh] OR “POP”) AND (“pelvic floor muscle training” OR “pelvic floor muscle exercise” OR “kegel exercise”) AND (“surgery”)) |
| SCOPUS | (TITLE-ABS ((“pelvic organ prolapse” OR “pop”)) AND TITLE-ABS ((“pelvic floor muscle training” OR “pelvic floor muscle exercise” OR “kegel exercise”))) AND TITLE-ABS (“surgery”)) |
| Cochrane | (“Pelvic Organ Prolapse” OR “POP”) AND (“pelvic floor muscle training” OR “pelvic floor muscle exercise” OR “kegel exercise”) AND (“surgery”) in Record Title |
| Cinahl | AB (pelvic organ prolapse or pop) AND AB (pelvic floor muscle training or pelvic floor muscle exercise or kegel exercise) AND AB surgery |
| PEDro | Pelvic organ prolapse AND pelvic floor muscle training AND surgery |
| Studies | Age | Population | N Patients | Applied Therapy | F-U | |||
|---|---|---|---|---|---|---|---|---|
| C | I | C | I | C | I | |||
| Alves et al. [16] 2015 | 65.67 | 66.11 | Women POP I/II/III | 10 | 18 | Global exercise program without PFMT | Global exercise program (12 sessions) PFMT (home): 30 min × 2 times/wk, 6 wk | 6 wk |
| Resende et al. [17] 2012 | 58.7 | 51.9 | Women POP II | 16 | 21 | Lifestyle advice | PFMT (home): 3x8-12 rep MVC + 3 FC day, 3 months Lifestyle advice | 3 months |
| Braekken et al. [18] 2015 | 48.3 | 49.4 | Women POP I/II/III | 50 | 59 | Lifestyle advice | PFMT (supervised + home): 18 sessions + 3x8-12rep near MVC day, 6 months Lifestyle advice | 6 months |
| Wiegersma et al. [19] 2014 | 64.0 | 64.5 | Women POP I/II | 142 | 145 | Watchful waiting | PFMT with physiotherapist PFMT (home): 2–3 times/day, individual protocol, 3–5 times/wk, 3 months Lifestyle advice | 3 months |
| Hagen et al. [20] 2014 | 57.50 | 56.20 | Women POP I/II/III | 222 | 224 | Lifestyle advice | PFMT with physiotherapist 5 sessions PFMT (home): 3x10-50 FC a day, 16 wk Lifestyle advice | 6 and 12 months |
| Due et al. [21] 2015 | 58 | 60 | Women POP II/III | 53 | 56 | 6 group sessions (Lifestyle advice) | 6 group sessions + 6 PFMT with physiotherapist PFMT (home): 3x10 MVC maintained 10 sec, 5 days/wk, 12 wk Lifestyle advice | 3 and 6 months |
| Hagen et al. [14] 2017 | 46.6 | 46.4 | Women POP I/II/III | 206 | 206 | Lifestyle advice | 5 sessions PFMT with physiotherapist PFMT (home): 3x10-50 FC a day, 16 wk Lifestyle advice | 2 years |
| Stüpp et al. [22] 2011 | 58.12 | 52.95 | Women POP II | 16 | 21 | Lifestyle advice | 7 sessions PFMT with physiotherapist PFMT (home): 3x8-12 maintained contractions 6–10 sec, 12 wk Lifestyle advice | 14 wk |
| Due et al. [23] 2016 | - | - | Women POP II/III | 43 | 40 | 6 group sessions (Lifestyle advice) | 6 group sessions + 6 PFMT with physiotherapist PFMT (home): 3x10 MVC maintained 10 sec, 5 days/wk, 12 wk Lifestyle advice | 12 months |
| Panman et al. [24] 2016 | 64.0 | 64.5 | Women POP I/II | 142 | 145 | Watchful waiting | PFMT with physiotherapist PFMT (home): 2–3 times/day, individual protocol, 3–5 times/wk, 2 years | 12 months 2 years |
| Barber et al. [25] 2014 | 56.9 | 57.5 | Women POP II/III/IV | 188 | 186 | Surgery + routine perioperative care | Surgery + PFMT (supervised + home) PRE: 1 session, POST: 4 sessions HOME: individualized protocol 3x45-60 rep 1–10 sec contraction, at 3 months 15 contractions daily max duration, 24 months | 6 months and 2 years |
| Liang et al. [26] 2019 | 63.3 | 61.6 | - | 43 | 47 | Surgery + Lifestyle advice | Surgery + PFMT (supervised + home): PRE: 1 session, POST: 3 sessions HOME: 2–3x15–30 min 10 sec contraction-10 sec rest + FC daily, 60 days | 42 and 60 days |
| Nyhus et al. [27] 2020 | 60.6 | 60.1 | Women POP ≥ II | 76 | 75 | Surgery | Surgery + PFMT PRE (home): 3x8-12 maintained contractions 6–8 sec daily Group option 1 day/wk 22 wk | 6 months |
| Jelovsek et al. [28] 2018 | 57.4 | 57 | Women POP II/III/IV | 144 | 141 | Surgery + routine pre-operative care | Surgery + PFMT (supervised + home) PRE: 1 session, POST: 4 sessions HOME: individualized protocol 3x45-60 rep 1–10 sec contraction, at 3 months 15 contractions daily max duration, 24 months | 5 years |
| Weidner et al. [29] 2017 | 56.9 | 57.5 | Women POP II/III/IV | 188 | 186 | Surgery + routine pre-operative care | Surgery + PFMT (supervised + home) PRE: 1 session, POST: 4 sessions HOME: individualized protocol 3x45-60 rep 1–10 sec contraction, at 3 months 15 contractions daily max duration, 24 months | 6 and 12 months 2 years |
| Duarte et al. [30] 2020 | - | - | Women POP II/III/IV | 46 | 48 | Surgery | Surgery + PFMT (supervised + home): PRE: 2 times/wk, 2 wk, POST: 7 sessions HOME: 3 days/wk, 4x10 MVC 7 sec contraction 7 sec rest + 5 FC | 40 and 90 days |
| Mathew et al. [31] 2021 | 60.6 | 60.1 | Women POP ≥ II | 76 | 75 | Surgery | Surgery + PFMT (home): 3x8-12 maintained contractions 6–8 sec daily. Group option 1 day/wk 22 wk | 6 months |
| McClurg et al. [32] 2013 | 60 | 60 | Women POP I/II/III | 29 | 28 | Surgery + routine pre-operative care | Surgery + PFMT: PRE (home): 3x10 MVC held up to 10 sec and 4 sec rest POST (supervised + home): 5 sessions/wk, 12 wk, individualized protocol with BFB, EE and exercise balls if necessary | 6 and 12 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espiño-Albela, A.; Castaño-García, C.; Díaz-Mohedo, E.; Ibáñez-Vera, A.J. Effects of Pelvic-Floor Muscle Training in Patients with Pelvic Organ Prolapse Approached with Surgery vs. Conservative Treatment: A Systematic Review. J. Pers. Med. 2022, 12, 806. https://doi.org/10.3390/jpm12050806
Espiño-Albela A, Castaño-García C, Díaz-Mohedo E, Ibáñez-Vera AJ. Effects of Pelvic-Floor Muscle Training in Patients with Pelvic Organ Prolapse Approached with Surgery vs. Conservative Treatment: A Systematic Review. Journal of Personalized Medicine. 2022; 12(5):806. https://doi.org/10.3390/jpm12050806
Chicago/Turabian StyleEspiño-Albela, Andrea, Carla Castaño-García, Esther Díaz-Mohedo, and Alfonso Javier Ibáñez-Vera. 2022. "Effects of Pelvic-Floor Muscle Training in Patients with Pelvic Organ Prolapse Approached with Surgery vs. Conservative Treatment: A Systematic Review" Journal of Personalized Medicine 12, no. 5: 806. https://doi.org/10.3390/jpm12050806