
Acute Left Atrial Response to Different Eccentric Resistance Exercise Loads in Patients with Heart Failure with Middle Range Ejection Fraction: A Pilot Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Population
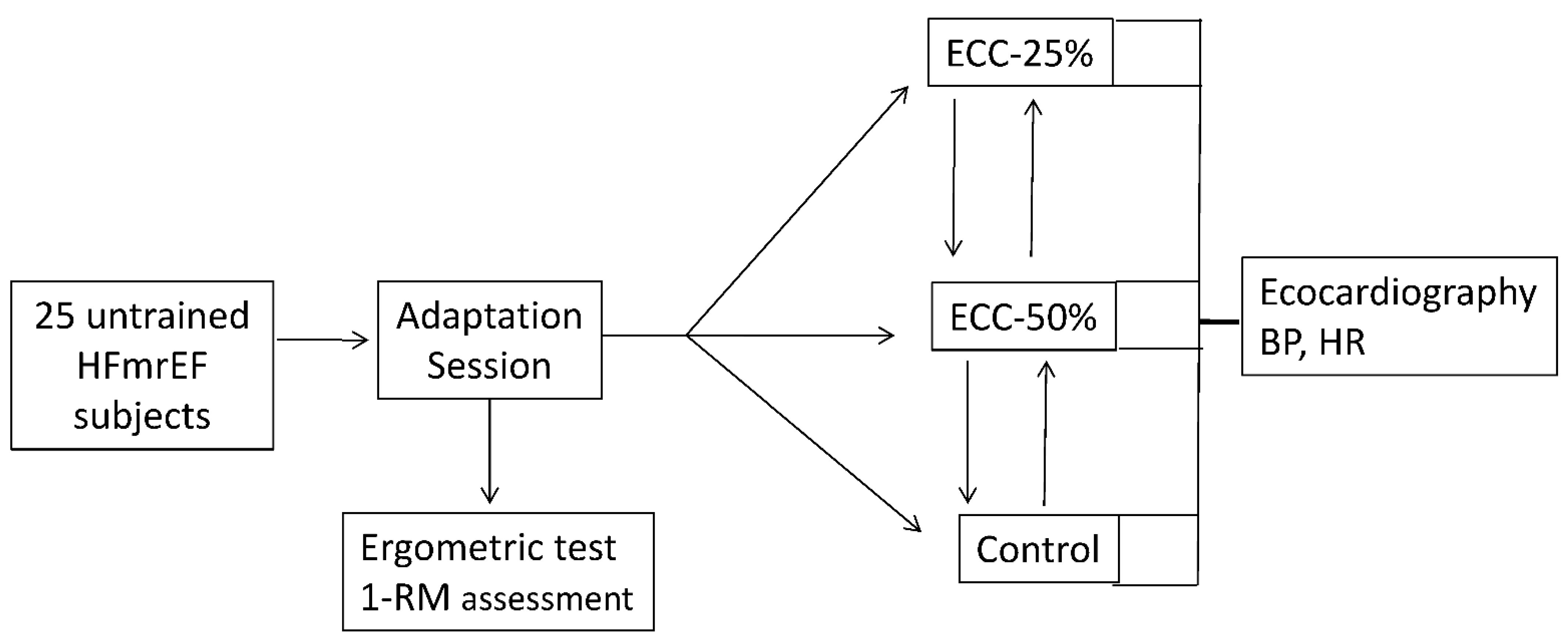
2.2. Study Design
2.3. Assessments
2.4. Statistical Analysis
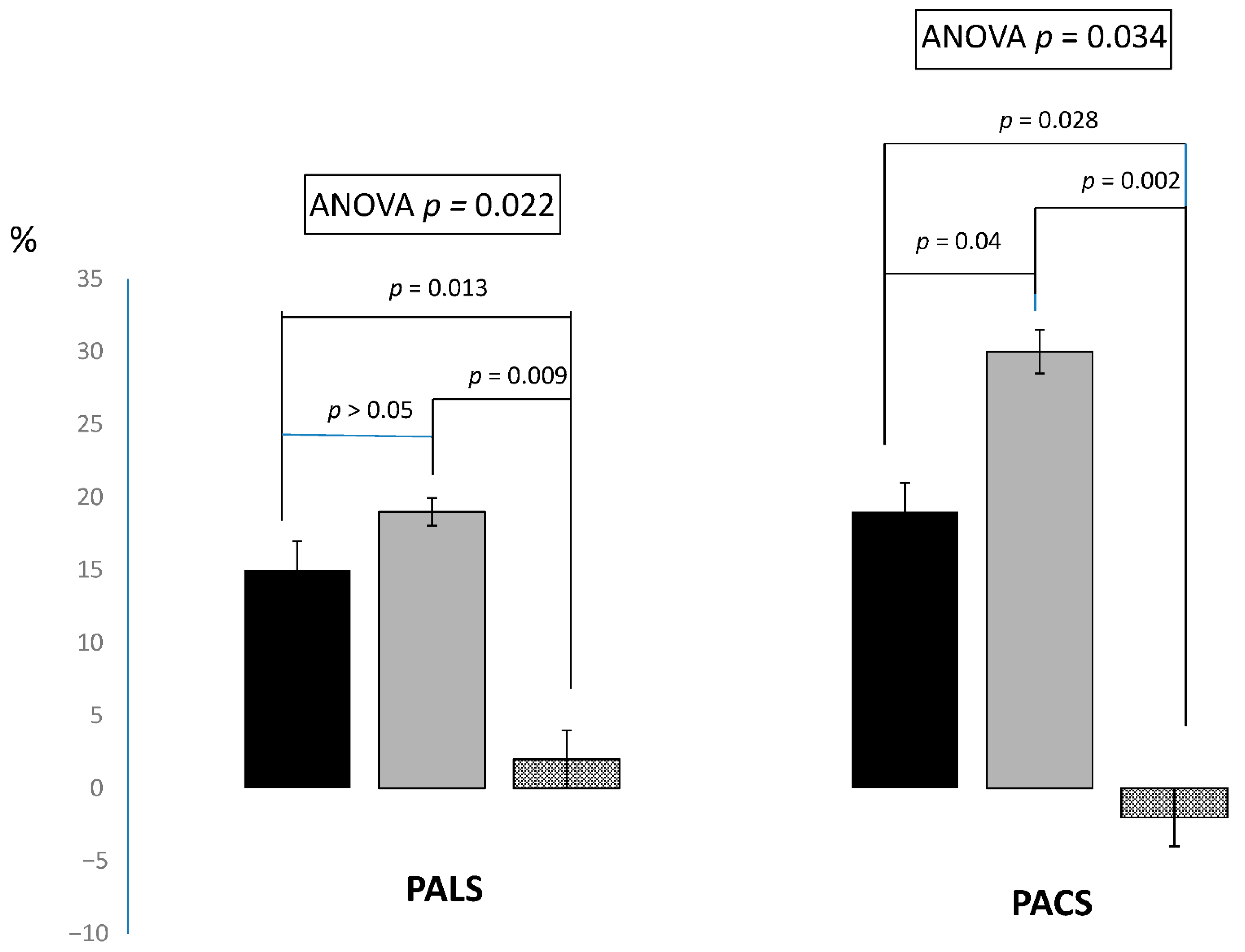
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Del Buono, M.G.; Arena, R.; Borlaug, B.A.; Carbone, S.; Canada, J.M.; Kirkman, D.L.; Garten, R.; Rodriguez-Miguelez, P.; Guazzi, M.; Lavie, C.J.; et al. Exercise Intolerance in Patients with Heart Failure: JACC State-of-the-Art Review. J. Am. Coll Cardiol. 2019, 73, 2209–2225. [Google Scholar] [CrossRef] [PubMed]
- Cattadori, G.; Segurini, C.; Picozzi, A.; Padeletti, L.; Anzà, C. Exercise and heart failure: An update. ESC Heart Fail. 2018, 5, 222–232. [Google Scholar] [CrossRef]
- Franklin, B.A.; Bonzheim, K.; Gordon, S.; Timmis, G.C. Resistance training in cardiac rehabilitation. J. Cardiopulm Rehabil. 1991, 11, 99–107. [Google Scholar] [CrossRef]
- Burd, N.A.; West, D.W.; Staples, A.W.; Atherton, P.J.; Baker, J.M.; Moore, D.R.; Holwerda, A.M.; Parise, G.; Rennie, M.J.; Baker, S.K.; et al. Low-load high volume resistance exercise stimulates muscle protein synthesis more than high-load low volume resistance exercise in young men. PLoS ONE. 2010, 5, e12033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurley, B.F.; Roth, S.M. Strength training in the elderly: Effects on risk factors for age-related diseases. Sports Med. 2000, 30, 249–268. [Google Scholar] [CrossRef] [PubMed]
- Delagardelle, C.; Feiereisen, P. Strength training for patients with chronic heart failure. Eura Medicophys. 2005, 41, 57–65. [Google Scholar] [PubMed]
- Pepera, G.; Christina, M.; Katerina, K.; Argirios, P.; Varsamo, A. Effects of multicomponent exercise training intervention on hemodynamic and physical function in older residents of long-term care facilities: A multicenter randomized clinical controlled trial. J. Bodyw. Mov. Ther. 2021, 28, 231–237. [Google Scholar] [CrossRef]
- Garza, M.A.; Wason, E.A.; Cruger, J.R.; Chung, E.; Zhang, J.Q. Strength training attenuates post-infarct cardiac dysfunction and remodeling. J. Physiol. Sci. 2019, 69, 523–530. [Google Scholar] [CrossRef]
- Overend, T.; Versteegh, T.; Thompson, E.; Birmingham, T.; Vandervoort, A. Cardiovascular stress associated with concentric and eccentric isokinetic exercise in young and older adults. J. Gerontol. Seri. A. 2000, 55, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Stöhr, E.; Stembridge, M.; Shave, R.; Samuel, J.; Stone, K.; Esformes, J. Systolic and diastolic LV mechanics during and following resistance exercise. Med. Sci. Sports Exerc. 2017, 49, 2. [Google Scholar] [CrossRef]
- Howlett, L.A.; O’Sullivan, K.; Sculthorpe, N.; Richards, J. The effect of varying intensities of lower limb eccentric muscle contractions on left ventricular function. Eur. J. Appl. Physiol. 2020, 120, 539–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheetham, C.; Green, D.; Collis, J.; Dembo, L.; O’Driscoll, G. Effect of aerobic and resistance exercise on central hemodynamic responses in severe chronic heart failure. J. Appl. Phisiol. 2002, 93, 175–180. [Google Scholar] [CrossRef] [Green Version]
- Gjøvaag, T.F.; MIrtaheri, P.; Simon, K.; Berdal, G.; Tuchel, I.; Westle, T.; Bruusgaard, K.A.; Nilsson, B.B.; Hisdal, J. Hemodynamic Responses to Resistance Exercise in Patients with Coronary Artery Disease. Med. Sci. Sports Exerc. 2016, 48, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Kambic, T.; Hadžić, V.; Lainscak, M. Hemodynamic Response to High- and Low-Load Resistance Exercise in Patients with Coronary Artery Disease: A Randomized, Crossover Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 3905. [Google Scholar] [CrossRef] [PubMed]
- Lamotte, M.; Chevalier, A.; Jamon, A.; Brassine, E.; Van de Borne, P. Hemodynamic response of an isokinetic testing and training session. Isokinet. Exerc. Sci. 2009, 17, 135–143. [Google Scholar] [CrossRef]
- Wright, S.; Esfandiari, S.; Elmayergi, N.; Sasson, Z.; Goodman, J.M. Left atrial functional changes following short-term exercise training. Eur. J. Appl. Physiol. 2014, 114, 2667–2675. [Google Scholar] [CrossRef]
- Henein, M.Y.; Cameli, M.; Lindqvist, P.; Wiklund, U.; Mandoli, G.E.; Mondillo, S. Peak Atrial Longitudinal Strain (PALS): Better Call it Stretch? Int. Cardiovasc. Forum J. 2018, 15, 3–5. [Google Scholar] [CrossRef]
- Santoro, A.; Alvino, F.; Antonelli, G.; Molle, R.; Mondillo, S. Left atrial strain after maximal exercise in competitive waterpolo players. Intern. J. Cardiovasc. Imaging 2016, 32, 399–405. [Google Scholar] [CrossRef]
- Sareban, M.; Winkert, K.; Berger, M.M.; Niebauer, J.; Steinacker, J.M.; Treff, G. Speckle tracking-derived bi-atrial strain before and after eleven weeks of training in elite rowers. Sci. Rep. 2018, 8, 14300. [Google Scholar] [CrossRef] [Green Version]
- Sugimoto, T.; Bandera, F.; Alfonzetti, E.; Bussadori, C.; Guazzi, M. Left atrial function dynamics during exercise in heart failure pathophysiological implications on the rightheart and exercise ventilation inefficiency. JACC Cardiovasc. Imaging 2017, 10, 1253–1264. [Google Scholar] [CrossRef]
- Brown, L.E.; Weir, J.P. ASEP Procedures Recommendation I: Accurate Assessment of Muscular Strength and Power. J. Exerc. Physiol. 2001, 4, 1–21. [Google Scholar]
- Brzycki, M. Strength Testing—Predicting a One-Rep Max from Reps-to-Fatigue. J. Phys. Educ. Recreat. Dance 1993, 64, 88–90. [Google Scholar] [CrossRef]
- Stöhr, E.J.; Stembridge, M.; Esformes, J.I. In vivo human cardiac shortening and lengthening velocity is region dependent and not coupled with heart rate: ‘longitudinal’ strain rate markedly underestimates apical contribution. Exp. Physiol. 2015, 100, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Kasner, M.; Sinning, D.; Burkhoff, D.; Tschöpe, C. Diastolic pressure-volume quotient (DPVQ) as a novel echocardiographic index for estimation of LV stiffness in HFpEF. Clin. Res. Cardiol. 2015, 104, 955–963. [Google Scholar] [CrossRef]
- Machino-Ohtsuka, T.; Seo, Y.; Tada, H.; Ishizu, T.; Machino, T.; Yamasaki, H.; Igarashi, M.; Xu, D.; Sekiguchi, Y.; Aonuma, K. Left atrial stiffness relates to left ventricular diastolic dysfunction and recurrence after pulmonary vein isolation for atrial fibrillation. J. Cardiovasc. Electrophysiol. 2011, 22, 999–1006. [Google Scholar] [CrossRef]
- Fukuta, H.; Little, W.C. The cardiac cycle and the physiologic basis of left ventricular contraction, ejection, relaxation, and filling. Heart Fail. Clin. 2008, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, Y.; Roberts, J.P.; Tan, P.; Klopfenstein, C.E.; Klopfenstein, H.S. Effect of dynamic exercise on left atrial function in conscious dogs. J. Physiol. 1994, 481, 457–468. [Google Scholar] [CrossRef] [Green Version]
- Cuspidi, C.; Tadic, M.; Sala, C.; Gherbesi, E.; Grassi, G.; Mancia, G. Left atrialfunction in elite athletes:A meta-analysis of two-dimensional speckle tracking echocardiographic studies. Clin. Cardiol. 2019, 42, 579–587. [Google Scholar] [CrossRef] [Green Version]
- Tan, Y.T.; Wenzelburger, F.; Lee, E.; Nightingale, P.; Heatlie, G.; Leyva, F.; Sanderson, J.E. Reduced left atrial function on exercise in patients with heart failure and normal ejection fraction. Heart 2010, 96, 1017–1023. [Google Scholar] [CrossRef]
- Lentini, A.C.; Mckelvie, R.S.; McCartney, N.; Tomlinson, C.W.; MacDougall, J.D. Left ventricular response in healthy young men during heavy-intensity weight-lifting esercise. J. Appl. Physiolog. 1993, 75, 2703–2710. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Marwick, T.H. Use and Limitations of E/e’ to Assess Left Ventricular Filling Pressure by Echocardiography. J. Cardiovasc. Ultrasound. 2011, 19, 169–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, O.S.; Smiseth, O.A.; Dokainish, H.; Abudiab, M.M.; Schutt, R.C.; Kumar, A.; Sato, K.; Harb, S.; Gude, E.; Remme, E.W.; et al. Estimating Left Ventricular Filling Pressure by Echocardiography. J. Am. Coll. Cardiol. 2017, 69, 1937–1948. [Google Scholar] [CrossRef] [PubMed]
- Pathan, F.; D’Elia, N.; Nolan, M.T.; Marwick, T.H.; Negishi, K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70.e8. [Google Scholar] [CrossRef] [PubMed]
- Anwar, A.M.; Geleijnse, M.L.; Soliman, O.I.; Nemes, A.; ten Cate, F.J. Left atrial Frank-Starling law assessed by real-time, three-dimensional echocardiographic left atrial volume changes. Heart 2007, 93, 1393–1397. [Google Scholar] [CrossRef] [Green Version]
- Caminiti, G.; Iellamo, F.; Perrone, M.A.; D’Antoni, V.; Catena, M.; Manzi, V.; Morsella, V.; Franchini, A.; Volterrani, M. Central Hemodynamic Adjustments during Post-Exercise Hypotension in Hypertensive Patients with Ischemic Heart Disease: Concurrent Circuit Exercise versus High-Intensity Interval Exercise. A Preliminary Study. J. Clin. Med. 2021, 10, 5881. [Google Scholar] [CrossRef] [PubMed]
- Zile, M.R.; Kjellstrom, B.; Bennett, T.; Cho, Y.; Baicu, C.F.; Aaron, M.F.; Abraham, W.T.; Bourge, R.C.; Kueffer, F.J. Effects of exercise on left ventricular systolic and diastolic properties in patients with heart failure and a preserved ejection fraction versus heart failure and a reduced ejection fraction. Circ. Heart Fail. 2013, 6, 508–516. [Google Scholar] [CrossRef] [Green Version]
- Andersen, M.J.; Ersbøll, M.; Bro-Jeppesen, J.; Gustafsson, F.; Hassager, C.; Køber, L.; Borlaug, B.A.; Boesgaard, S.; Kjærgaard, J.; Møller, J.E. Exercise hemodynamics in patients with and without diastolic dysfunction and preserved ejection fraction after myocardial infarction. Circ. Heart Fail. 2012, 5, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Stefani, L.; Toncelli, L.; Di Tante, V.; Vono, M.; Cappelli, B.; Pedrizzetti, G.; Galanti, G. Supernormal functional reserve of apical segments in elite soccer players: An ultrasound speckle tracking handgrip stress study. Cardiovas. Ultrasound 2008, 1, 14. [Google Scholar] [CrossRef] [Green Version]
- Weiner, R.B.; Weyman, A.E.; Kim, J.H.; Wang, T.J.; Picard, M.H.; Baggish, A.L. The impact of isometric handgrip testing on left ventricular twist mechanics. J. Physiol. 2012, 590, 5141–5150. [Google Scholar] [CrossRef] [Green Version]
- MacDougall, J.D.; Tuxen, D.; Sale, D.G.; Moroz, J.R.; Sutton, J.R. Arterial blood pressure response to heavy resistance exercise. J. Appl. Physiol. 1985, 58, 785–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Age, years | 71.4 ± 7.5 |
| BMI, kg/m2 | 27.5 ± 6.3 |
| Waist circumference, cm | 104.2 ± 31.6 |
| Male/female | 20/5 |
| Previous PCI/CABG | 16/14 |
| NYHA class (II-III) | 19/6 |
| EF (%) | 46.7± 6.2 |
| NT-pro BNP | 465.0 ± 59.3 |
| Comorbidities | |
| Carotid artery disease, n (%) | 13 (52) |
| Hypertension, n (%) | 25/(100) |
| Diabetes, n (%) | 6 (24) |
| Hypercholesterolemia, n (%) | 21 (84) |
| Previous Smoke habit, n (%) | 18 (60) |
| Treatment | |
| Anti-platelets agents, n (%) | 25 (100) |
| ACE-Is/ARBs, n (%) | 22 (88) |
| Betablockers, n (%) | 18 (60) |
| Diuretics, n (%) | 8 (32) |
| Statins, n (%) | 25 (100) |
| ECC-20% | ECC-50% | Control | ||||
|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | T0 | T1 | |
| HR, bpm | 61.2 ± 22.4 | 68.6 ± 23.2 * | 64.5 ± 27.5 | 71.2 ± 31.8 * | 64.1 ± 26.6 | 66.2 ± 25.7 |
| SBP, mmHg 1 | 113.6 ± 28.2 | 132.7 ± 25.6 * | 107.8 ± 23.5 | 133.7 ± 19.4 * | 109.2 ± 39.6 | 107.4 ± 28.4 |
| DBP, mmHg | 74.1 ± 11.5 | 78.4 ± 10.4 | 73.6 ± 17.1 | 75.5 ± 10.8 | 73,9 ± 13.3 | 74.0 ± 15.8 |
| MAP, mmHg | 87.8 ± 11.6 | 94.8 ± 9.6 * | 87.2 ± 13.7 | 96.3 ± 11.1 * | 87.2 ± 13.7 | 87.2 ± 13.7 |
| DP, mmHg | 69.5 ± 13.3 | 91.0 ± 22.1 | 68.4 ± 17.7 | 95.2 ± 19.4 | 68.3 ± 20.5 | 68.4 ± 16.9 |
| LA PALS, % | 28.2 ± 8.2 | 32.7 ± 11.6 * | 28.2 ± 10.1 | 33.5 ± 8.4 * | 28.2 ± 10.1 | 28.6 ± 7.3 |
| LA PACS, % | 14.0 ± 3.6 | 16.7 ± 3.8 * | 14.2 ± 3.7 | 18.5 ± 4.6 * † | 14.5 ± 2.9 | 14.3 ± 3.4 |
| LAVI | 33.4 ± 5.1 | 32.9 ± 3.9 | 33.2 ± 4.7 | 33.5 ± 5.0 | 33.2 ± 4.3 | 33.6 ± 6.5 |
| EDV, mL | 125.6 ±34.5 | 123.4 ± 40.4 | 123.7 ± 36.2 | 126.2 ± 26.9 | 125.9 ± 30.4 | 126.0 ± 28.7 |
| ESV, mL | 67.2 ± 26.3 | 62.9 ± 24.9 | 62.3 ± 18.4 | 65.3 ± 22.1 | 66.4 ± 19.5 | 67.1 ± 20.8 |
| E, cm/s | 57.7 ± 17.88 | 71.6 ± 21.3 | 55.6 ± 18.7 | 71.2 ± 15.6 | 57.1 ± 16.0 | 58.3 ± 17.1 |
| A, cm/s | 59.4 ± 22.6 | 68.5 ± 16.8 | 58.3 ± 19.5 | 73.3 ± 16.2 | 58.4 ± 19.2 | 61.2 ± 21.0 |
| E’ | 6.7 ± 1.5 | 7.5 ± 2.2 * | 7.0 ± 1.9 | 7.5 ± 1.4 * | 6.6 ± 2.0 | 6.8 ± 1.8 |
| A’ | 5.8 ± 1.4 | 7.1 ± 3.0 * | 5.4 ± 1.4 | 7.8 ± 3.0 * | 56 ± 1.9 | 5.8 ± 2.2 |
| E/E’ | 8.6 ± 1.7 | 9.5 ± 1.9 * | 7.9 ± 2.5 | 9.4 ± 1.4 * | 8.3 ± 2.2 | 8.1 ± 1.9 |
| LA stiffness | 0.30 ± 0.2 | 0.29 ± 0.4 | 0.28 ± 0.2 | 0.28 ± 0.3 | 0.29 ± 0.4 | 0.28 ± 0.3 |
| LV stiffness | 68.9 ± 8.3 | 76.3 ± 10.5 * | 63.8 ± 11.8 | 74.4 ± 12.0 * | 65.9 ± 15.2 | 64.2 ± 9.7 |
| EF, % | 46.2 ± 3.6 | 46.8 ± 2.8 | 45.9 ± 4.5. | 46.1 ± 3.3 | 46.3 ± 5.1 | 46.1 ± 3.9 |
| LV GLS, % | −13.8 ± 1.7 | −16.3 ± 2.2 | −13.1 ± 1.8 | −14.6 ± 2.4 | −13.4 ± 2.4 | −13.5 ± 1.9 |
| SV, mL | 58.4 ± 17.3 | 56.1 ± 11.0 | 61.4 ± 19.2 | 62.8 ± 16.8 | 61.4 ± 13.2 | 60.9 ± 18.7 |
| CO, l/min | 3.5 ± 1.5 | 4.1 ± 1.3 * | 3.7 ± 1.2 | 4.2 ± 1.8 * | 3.6 ± 1.7 | 3.7 ± 1.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caminiti, G.; Perrone, M.A.; Iellamo, F.; D’Antoni, V.; Catena, M.; Franchini, A.; Volterrani, M. Acute Left Atrial Response to Different Eccentric Resistance Exercise Loads in Patients with Heart Failure with Middle Range Ejection Fraction: A Pilot Study. J. Pers. Med. 2022, 12, 689. https://doi.org/10.3390/jpm12050689
Caminiti G, Perrone MA, Iellamo F, D’Antoni V, Catena M, Franchini A, Volterrani M. Acute Left Atrial Response to Different Eccentric Resistance Exercise Loads in Patients with Heart Failure with Middle Range Ejection Fraction: A Pilot Study. Journal of Personalized Medicine. 2022; 12(5):689. https://doi.org/10.3390/jpm12050689
Chicago/Turabian StyleCaminiti, Giuseppe, Marco Alfonso Perrone, Ferdinando Iellamo, Valentino D’Antoni, Matteo Catena, Alessio Franchini, and Maurizio Volterrani. 2022. "Acute Left Atrial Response to Different Eccentric Resistance Exercise Loads in Patients with Heart Failure with Middle Range Ejection Fraction: A Pilot Study" Journal of Personalized Medicine 12, no. 5: 689. https://doi.org/10.3390/jpm12050689