
Fever, Tachypnea, and Monocyte Distribution Width Predicts Length of Stay for Patients with COVID-19: A Pioneer Study

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Data Collection
2.3. Clinical Spectrum of COVID-19 Infection
2.4. New Biomarker Measurement
2.5. Statistical Analysis
2.6. Validation Study
3. Results
3.1. Patient Characteristics
3.2. Inflammatory Markers
3.3. Predictors of an LOS of >14 Days
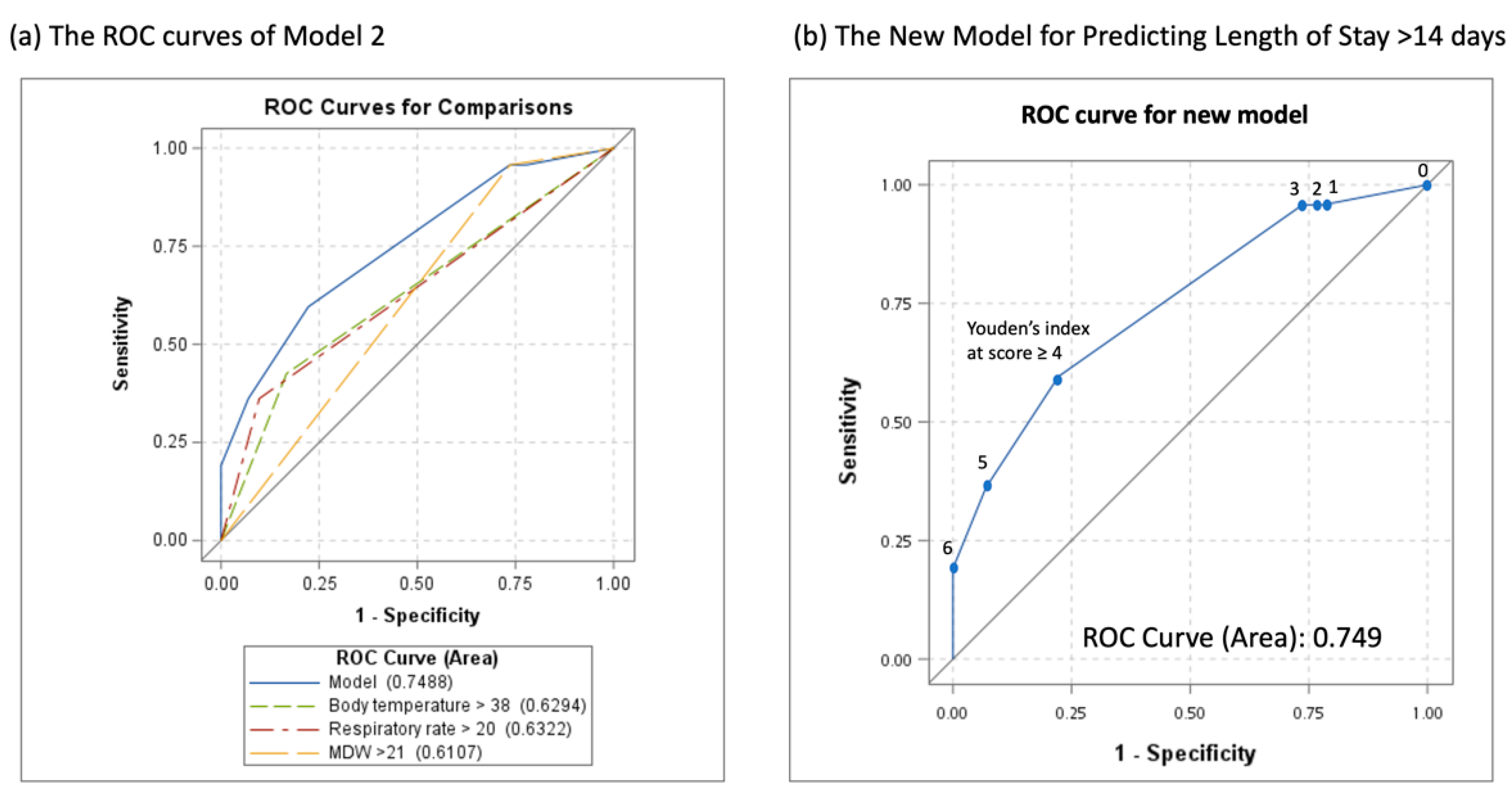
3.4. Multivariable Models for Predicting an LOS of >14 Days
3.5. Subgroup Analysis for the Non-ICU and ICU Categories
3.6. Validation Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xie, J.; Tong, Z.; Guan, X.; Du, B.; Qiu, H.; Slutsky, A.S. Critical care crisis and some recommendations during the COVID-19 epidemic in China. Intensive Care Med. 2020, 46, 837–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, H.; Tong, Z.; Ma, P.; Hu, M.; Peng, Z.; Wu, W.; Du, B. Intensive care during the coronavirus epidemic. Intensive Care Med. 2020, 46, 576–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Paterlini, M. On the front lines of coronavirus: The Italian response to covid-19. BMJ 2020, 368, m1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legido-Quigley, H.; Mateos-García, J.T.; Campos, V.R.; Gea-Sánchez, M.; Muntaner, C.; McKee, M. The resilience of the Spanish health system against the COVID-19 pandemic. Lancet Public Health 2020, 5, e251–e252. [Google Scholar] [CrossRef] [Green Version]
- Rubenfeld, G.D.; Caldwell, E.; Peabody, E.; Weaver, J.; Martin, D.P.; Neff, M.; Stern, E.J.; Hudson, L.D. Incidence and outcomes of acute lung injury. N. Engl. J. Med. 2005, 353, 1685–1693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serafim, R.B.; Póvoa, P.; Souza-Dantas, V.; Kalil, A.C.; Salluh, J.I. Clinical course and outcomes of critically ill patients with COVID-19 infection: A systematic review. Clin. Microbiol. Infect. 2021, 27, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Cook, D.J.; Thabane, L.; Friedrich, J.O.; Crozier, T.M.; Muscedere, J.; Granton, J.; Mehta, S.; Reynolds, S.C.; Lopes, R.D. Risk factors for mortality in patients admitted to intensive care units with pneumonia. Respir. Res. 2016, 17, 1–9. [Google Scholar]
- Daniel, P.; Woodhead, M.; Welham, S.; Mckeever, T.M.; Lim, W.S. Mortality reduction in adult community-acquired pneumonia in the UK (2009–2014): Results from the British Thoracic Society audit programme. Thorax 2016, 71, 1061–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenbaum, L. Facing Covid-19 in Italy—ethics, logistics, and therapeutics on the epidemic’s front line. N. Engl. J. Med. 2020, 382, 1873–1875. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Rees, E.M.; Nightingale, E.S.; Jafari, Y.; Waterlow, N.R.; Clifford, S.; Pearson, C.A.; Jombart, T.; Procter, S.R.; Knight, G.M.; Group, C.W. COVID-19 length of hospital stay: A systematic review and data synthesis. BMC Med. 2020, 18, 1–22. [Google Scholar] [CrossRef]
- Li, B. The Association Between Symptom Onset and Length of Hospital Stay in 2019 Novel Coronavirus Pneumonia Cases Without Epidemiological Trace. J. Natl. Med. Assoc. 2020, 112, 516–517. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Belliato, M.; Dimopoulos, M.-A.; Giamarellos-Bourboulis, E.J.; Jaksic, V.; Martin-Loeches, I.; Mporas, I.; Pelosi, P.; Poulakou, G.; Pournaras, S. Update in COVID-19 in the intensive care unit from the 2020 HELLENIC Athens International symposium. Anaesth. Crit. Care Pain Med. 2020, 39, 723–730. [Google Scholar] [CrossRef]
- Chen, S.; Zhang, Z.; Yang, J.; Wang, J.; Zhai, X.; Bärnighausen, T.; Wang, C. Fangcang shelter hospitals: A novel concept for responding to public health emergencies. Lancet 2020, 395, 1305–1314. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.; Jit, M.; Warren-Gash, C.; Guthrie, B.; Wang, H.H.X.; Mercer, S.W.; Sanderson, C.; McKee, M.; Troeger, C.; Ong, K.L.; et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: A modelling study. Lancet Glob Health 2020, 8, e1003–e1017. [Google Scholar] [CrossRef]
- Li, K.; Zhang, C.; Qin, L.; Zang, C.; Li, A.; Sun, J.; Zhao, Y.; Feng, Y.; Zhang, Y. A Nomogram Prediction of Length of Hospital Stay in Patients with COVID-19 Pneumonia: A Retrospective Cohort Study. Dis. Markers 2021, 2021, 5598824. [Google Scholar] [CrossRef]
- Hong, Y.; Wu, X.; Qu, J.; Gao, Y.; Chen, H.; Zhang, Z. Clinical characteristics of coronavirus disease 2019 and development of a prediction model for prolonged hospital length of stay. Ann. Transl. Med. 2020, 8, 443. [Google Scholar] [CrossRef] [PubMed]
- Di Castelnuovo, A.; Bonaccio, M.; Costanzo, S.; Gialluisi, A.; Antinori, A.; Berselli, N.; Blandi, L.; Bruno, R.; Cauda, R.; Guaraldi, G. Common cardiovascular risk factors and in-hospital mortality in 3,894 patients with COVID-19: Survival analysis and machine learning-based findings from the multicentre Italian CORIST Study. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1899–1913. [Google Scholar] [CrossRef] [PubMed]
- Mehmood, I.; Ijaz, M.; Ahmad, S.; Ahmed, T.; Bari, A.; Abro, A.; Allemailem, K.S.; Almatroudi, A.; Tahir ul Qamar, M. SARS-CoV-2: An update on genomics, risk assessment, potential therapeutics and vaccine development. Int. J. Environ. Res. Public Health 2021, 18, 1626. [Google Scholar] [CrossRef] [PubMed]
- Yanez, N.D.; Weiss, N.S.; Romand, J.-A.; Treggiari, M.M. COVID-19 mortality risk for older men and women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef] [PubMed]
- Lewnard, J.A.; Liu, V.X.; Jackson, M.L.; Schmidt, M.A.; Jewell, B.L.; Flores, J.P.; Jentz, C.; Northrup, G.R.; Mahmud, A.; Reingold, A.L.; et al. Incidence, clinical outcomes, and transmission dynamics of severe coronavirus disease 2019 in California and Washington: Prospective cohort study. BMJ 2020, 369, m1923. [Google Scholar] [CrossRef] [PubMed]
- Mahboub, B.; Al Bataineh, M.T.; Alshraideh, H.; Hamoudi, R.; Salameh, L.; Shamayleh, A. Prediction of COVID-19 hospital length of stay and risk of death using artificial intelligence-based modeling. Front. Med. 2021, 8, 592336. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Plebani, M. The critical role of laboratory medicine during coronavirus disease 2019 (COVID-19) and other viral outbreaks. Clin. Chem. Lab. Med. 2020, 58, 1063–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, B.M.; Lippi, G.; Plebani, M. Laboratory abnormalities in children with novel coronavirus disease 2019. Clin. Chem. Lab. Med. 2020, 58, 1135–1138. [Google Scholar] [CrossRef] [Green Version]
- Tan, C.; Huang, Y.; Shi, F.; Tan, K.; Ma, Q.; Chen, Y.; Jiang, X.; Li, X. C-reactive protein correlates with computed tomographic findings and predicts severe COVID-19 early. J. Med. Virol. 2020, 92, 856–862. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Plebani, M. Laboratory abnormalities in patients with COVID-2019 infection. Clin. Chem. Lab. Med. 2020, 58, 1131–1134. [Google Scholar] [CrossRef] [Green Version]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W. Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Peng, J.; Qi, D.; Yuan, G.; Deng, X.; Mei, Y.; Feng, L.; Wang, D. Diagnostic value of peripheral hematologic markers for coronavirus disease 2019 (COVID-19): A multicenter, cross-sectional study. J. Clin. Lab. Anal. 2020, 34, e23475. [Google Scholar] [CrossRef]
- Sarkar, S.; Kannan, S.; Khanna, P.; Singh, A.K. Role of platelet-to-lymphocyte count ratio (PLR), as a prognostic indicator in COVID-19: A systematic review and meta-analysis. J. Med. Virol. 2022, 94, 211–221. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.-E.; Katsaounou, P. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host Microbe 2020, 27, 992–1000.e1003. [Google Scholar] [CrossRef]
- Mardi, D.; Fwity, B.; Lobmann, R.; Ambrosch, A. Mean cell volume of neutrophils and monocytes compared with C-reactive protein, interleukin-6 and white blood cell count for prediction of sepsis and nonsystemic bacterial infections. Int. J. Lab. Hematol. 2010, 32, 410–418. [Google Scholar] [CrossRef]
- Henderson, R.B.; Hobbs, J.A.; Mathies, M.; Hogg, N. Rapid recruitment of inflammatory monocytes is independent of neutrophil migration. Blood 2003, 102, 328–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Italiani, P.; Boraschi, D. From monocytes to M1/M2 macrophages: Phenotypical vs. functional differentiation. Front. Immunol. 2014, 5, 514. [Google Scholar] [PubMed] [Green Version]
- Crouser, E.D.; Parrillo, J.E.; Seymour, C.W.; Angus, D.C.; Bicking, K.; Esguerra, V.G.; Peck-Palmer, O.M.; Magari, R.T.; Julian, M.W.; Kleven, J.M. Monocyte distribution width: A novel indicator of sepsis-2 and sepsis-3 in high-risk emergency department patients. Crit. Care Med. 2019, 47, 1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crouser, E.D.; Parrillo, J.E.; Seymour, C.; Angus, D.C.; Bicking, K.; Tejidor, L.; Magari, R.; Careaga, D.; Williams, J.; Closser, D.R. Improved early detection of sepsis in the ED with a novel monocyte distribution width biomarker. Chest 2017, 152, 518–526. [Google Scholar] [CrossRef]
- Piva, E.; Zuin, J.; Pelloso, M.; Tosato, F.; Fogar, P.; Plebani, M. Monocyte distribution width (MDW) parameter as a sepsis indicator in intensive care units. Clin. Chem. Lab. Med. 2021, 59, 1307–1314. [Google Scholar] [CrossRef]
- Hou, S.-K.; Lin, H.-A.; Chen, S.-C.; Lin, C.-F.; Lin, S.-F. Monocyte distribution width, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio improves early prediction for sepsis at the emergency. J. Pers. Med. 2021, 11, 732. [Google Scholar] [CrossRef]
- Xu, D. Clinical applications of leukocyte morphological parameters. Int. J. Pathol. Clin. Res. 2015, 1, 1. [Google Scholar] [CrossRef]
- McCullough, K.; Basta, S.; Knötig, S.; Gerber, H.; Schaffner, R.; Kim, Y.; Saalmüller, A.; Summerfield, A. Intermediate stages in monocyte–macrophage differentiation modulate phenotype and susceptibility to virus infection. Immunology 1999, 98, 203. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Mak, K.; Chen, L.; Chou, M.; Ho, C. Heterogeneity of human blood monocyte: Two subpopulations with different sizes, phenotypes and functions. Immunology 1992, 77, 298. [Google Scholar] [PubMed]
- Riva, G.; Castellano, S.; Nasillo, V.; Ottomano, A.M.; Bergonzini, G.; Paolini, A.; Lusenti, B.; Milić, J.; De Biasi, S.; Gibellini, L. Monocyte Distribution Width (MDW) as novel inflammatory marker with prognostic significance in COVID-19 patients. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Nasillo, V.; Luppi, M.; Tagliafico, E.; Trenti, T. Linking COVID-19, monocyte activation and sepsis: MDW, a novel biomarker from cytometry. EBioMedicine 2022, 75, 103754. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-A.; Lin, S.-F.; Chang, H.-W.; Lee, Y.-J.; Chen, R.-J.; Hou, S.-K. Clinical impact of monocyte distribution width and neutrophil-to-lymphocyte ratio for distinguishing COVID-19 and influenza from other upper respiratory tract infections: A pilot study. PLoS ONE 2020, 15, e0241262. [Google Scholar] [CrossRef] [PubMed]
- Alsuwaidi, L.; Al Heialy, S.; Shaikh, N.; Al Najjar, F.; Seliem, R.; Han, A.; Hachim, M. Monocyte distribution width as a novel sepsis indicator in COVID-19 patients. BMC Infect. Dis. 2022, 22, 27. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines; National Institutes of Health. (USA). Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 1 February 2022).
- Coronavirus, N. Discharge Criteria for Confirmed COVID-19 Cases; European Centre for Disease Prevention and Control (Sweden); Available online: https://www.ecdc.europa.eu/sites/default/files/documents/COVID-19-Discharge-criteria.pdf (accessed on 1 February 2021).
- Su, J.; Wu, W.; Lang, G.; Zhao, H.; Sheng, J. Transmission risk of patients with COVID-19 meeting discharge criteria should be interpreted with caution. J. Zhejiang Univ. Sci. B 2020, 21, 408. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Liu, Y.; Wei, L.; Ji, J.S.; Liu, R.; Zha, Y.; Chang, X.; Zhang, L.; Liu, Q.; Zhang, Y.; et al. What are the risk factors of hospital length of stay in the novel coronavirus pneumonia (COVID-19) patients? A survival analysis in southwest China. PLoS ONE 2022, 17, e0261216. [Google Scholar] [CrossRef] [PubMed]
- Odone, A.; Delmonte, D.; Scognamiglio, T.; Signorelli, C. COVID-19 deaths in Lombardy, Italy: Data in context. Lancet Public Health 2020, 5, e310. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Domen, J.; et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19. Cochrane Database Syst. Rev. 2021, 2, CD013665. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Evans, L.; Alshamsi, F.; Møller, M.H.; Ostermann, M.; Prescott, H.C.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E. Surviving sepsis campaign guidelines on the management of adults with coronavirus disease 2019 (COVID-19) in the ICU: First update. Crit. Care Med. 2021, 49, e219–e234. [Google Scholar] [CrossRef] [PubMed]
- Drummond, G.B.; Fischer, D.; Arvind, D.K. Current clinical methods of measurement of respiratory rate give imprecise values. ERJ Open Res. 2020, 6. [Google Scholar] [CrossRef]
- Kallioinen, N.; Hill, A.; Christofidis, M.J.; Horswill, M.S.; Watson, M.O. Quantitative systematic review: Sources of inaccuracy in manually measured adult respiratory rate data. J. Adv. Nurs. 2021, 77, 98–124. [Google Scholar] [CrossRef]
- Subbe, C.P.; Kruger, M.; Rutherford, P.; Gemmel, L. Validation of a modified Early Warning Score in medical admissions. QJM 2001, 94, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Gardner-Thorpe, J.; Love, N.; Wrightson, J.; Walsh, S.; Keeling, N. The value of Modified Early Warning Score (MEWS) in surgical in-patients: A prospective observational study. Ann. R. Coll. Surg. Engl. 2006, 88, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Polilli, E.; Sozio, F.; Frattari, A.; Persichitti, L.; Sensi, M.; Posata, R.; Di Gregorio, M.; Sciacca, A.; Flacco, M.E.; Manzoli, L. Comparison of Monocyte Distribution Width (MDW) and Procalcitonin for early recognition of sepsis. PLoS ONE 2020, 15, e0227300. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and fungal coinfection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Van Berkel, M.; Kox, M.; Frenzel, T.; Pickkers, P.; Schouten, J. Biomarkers for antimicrobial stewardship: A reappraisal in COVID-19 times? Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Buttarello, M. Laboratory diagnosis of anemia: Are the old and new red cell parameters useful in classification and treatment, how? Int. J. Lab. Hematol. 2016, 38 (Suppl. 1), 123–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, M.; Blin, T.; Collercandy, N.; Szychowiak, P.; Dequin, P.F.; Jouan, Y.; Guillon, A. Critically ill SARS-CoV-2-infected patients are not stratified as sepsis by the qSOFA. Ann. Intensive Care 2020, 10, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 1 February 2022).




{kind=link}
{kind=link}
{kind=link}
| Characteristic | LOS ≤ 14 Days (n = 72) | LOS > 14 Days (n = 48) | p Value |
|---|---|---|---|
| Age (years) † | 55.0 (39.0–65.0) | 65.0 (54.0–73.0) | 0.0036 * |
| Female sex | 40/72 (55.6%) | 17/48 (55.6%) | 0.0304 * |
| BMI (kg/m2) † | 24.5 (21.4–27.8) | 24.0 (22.2–28.1) | 0.8314 |
| Symptoms | |||
| Fever at home | 43/72 (59.4%) | 37/48 (77.1%) | 0.0481 * |
| Dyspnea | 7/72 (9.7%) | 11/48 (22.9%) | 0.0107 * |
| Vital signs at ED | |||
| Body temperature (°C) † | 36.8 (36.6–37.5) | 37.4 (36.6–38.2) | 0.0277 * |
| Heart rate (beats/min) | 86.5 (76.0–100.0) | 95.0 (76.0–104.0) | 0.3298 |
| Respiratory rate (breaths/min) † | 18.0 (17.0–20.0) | 20.0 (18.0–24.0) | <0.0001 * |
| SpO2 (%) † | 97.0 (95.0–99.0) | 96.0 (91.0–98.0) | 0.0147 * |
| SIRS score † | 1.0 (1.0–2.0) | 2.0 (1.0–2.0) | 0.1872 |
| qSOFA score † | 0 (0–0) | 0 (0–0) | 0.0011 * |
| Glasgow coma scale < 15 | 2/72 (2.8%) | 3/48 (6.3%) | 0.2320 |
| Respiratory rate ≥ 22/min | 6/72 (8.3%) | 17/48 (35.4%) | 0.0002 * |
| SBP ≤ 100 mmHg | 2/72 (2.8%) | 4/48 (8.3%) | 0.1733 |
| Charlson Comorbidity Index † | 1.0 (0.0–3.0) | 2.5 (1.0–4.0) | 0.8724 |
| Severity at ED | <0.0001 * | ||
| Mild | 39/72 (54.2%) | 9/48 (18.8%) | |
| Moderate | 25/72 (34.7%) | 11/48 (22.9%) | |
| Severe | 3/72 (4.2%) | 10/48 (20.8%) | |
| Critical | 5/72 (6.9%) | 18/48 (37.5%) | |
| Clinical course | |||
| Median LOS (days) † | 11.0 (10.0–12.0) | 21.0 (17.0–34.0) | <0.0001 * |
| Transfer to ICU | 8/72 (11.1%) | 27/48 (56.3%) | <0.0001 * |
| Mortality | 5/72 (6.9%) | 10/48 (20.8%) | 0.0242 * |
| Inflammatory markers | |||
| WBC (103 cells/μL) † | 6.0 (4.8–7.5) | 5.8 (4.7–7.6) | 0.8537 |
| RDW (%) † | 13.7 ± 1.3 | 13.5 ± 0.8 | 0.8724 |
| CRP (mg/dL) † | 1.8 (0.3–7.5) | 4.9 (1.3–11.4) | 0.0051 * |
| PCT (ng/mL) † | 0.06 (0.04–0.11) | 0.10 (0.05–0.41) | 0.1306 |
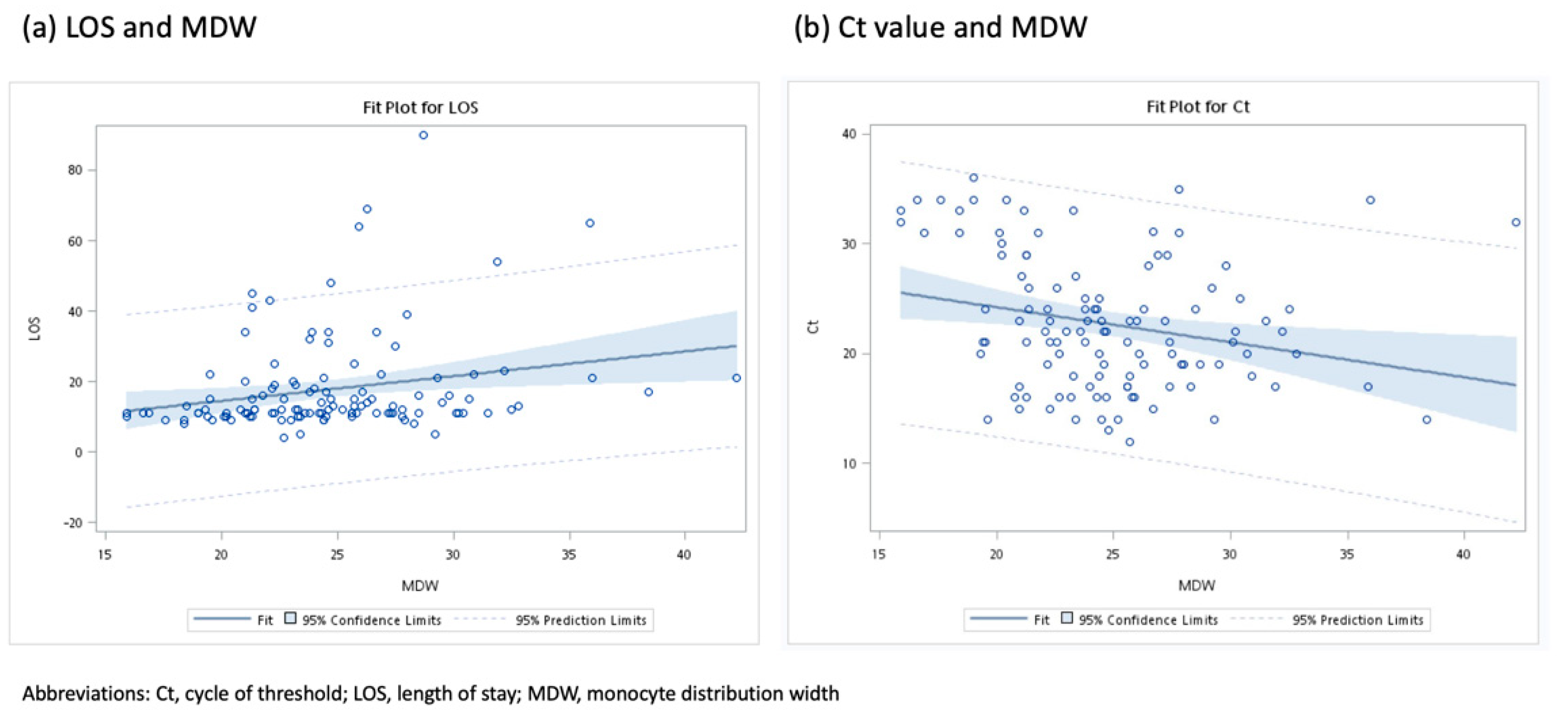
| MDW † | 23.5 (20.6–26.5) | 24.7 (22.3–28.5) | 0.0177 * |
| NLR † | 3.5 (1.7–5.7) | 4.9 (3.2–9.5) | 0.0199 * |
| PLR † | 209.0 ± 159.8 | 226.6 ± 178.2 | 0.5095 |
| Median Ct number † | 23.0 (18.0–29.0) | 21.0 (17.0–24.0) | 0.0858 |
| Characteristic | OR (95% CI) | p Value | AUC (95% CI) | Cutoff Value a | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|---|---|---|
| Age (years) | 1.04 (1.01–1.06) | 0.0044 * | 0.661 (0.561–0.761) | 63 | - | - |
| Age > 60 years | 3.25 (1.52–6.96) | 0.0024 * | 0.642 (0.554–0.731) | - | 60.4% (45.3–74.2%) | 68.1% (56.0–78.6%) |
| Sex (male vs. female) | 2.28 (1.07–4.84) | 0.0319 * | 0.601(0.511–0.690) | - | - | - |
| BMI (kg/m2) | 1.01 (0.93–1.10) | 0.7831 | 0.513 (0.395–0.631) | - | - | - |
| Body temperature (°C) | 1.68 (1.09–2.61) | 0.0189 * | 0.620 (0.514–0.727) | 38 | - | - |
| Fever > 38 °C | 3.57 (1.54–8.31) | 0.0031 * | 0.625 (0.542–0.708) | - | 41.7% (27.6–56.8%) | 83.3% (72.7–91.1%) |
| Heart rate (beats/min) | 1.01 (0.99–1.03) | 0.3273 | 0.559 (0.451–0.668) | - | - | - |
| Respiratory rate (breaths/min) | 1.33 (1.15–1.55) | 0.0002 * | 0.726 (0.637–0.815) | 20 | - | - |
| Tachypnea > 20 breaths/min | 5.09 (1.91–13.55) | 0.0011 * | 0.629 (0.552–0.705) | - | 35.4% (22.2–50.5%) | 90.3% (81.0–96.0%) |
| SpO2 (%) | 0.87 (0.79–0.96) | 0.0043 * | 0.633 (0.529–0.737) | 96 | - | - |
| SpO2 < 96% | 2.23 (1.04–4.78) | 0.0384 * | 0.594 (0.505–0.683) | - | 47.9% (33.3–62.8%) | 70.8% (58.9–80.5%) |
| SBP (mmHg) | 1.00 (0.99–1.02) | 0.8114 | 0.520 (0.411–0.629) | - | - | - |
| DBP (mmHg) | 0.99 (0.97–1.02) | 0.5626 | 0.540 (0.433–0.646) | - | - | - |
| MAP (mmHg) | 1.00 (0.97–1.02) | 0.7877 | 0.505 (0.397–0.612) | - | - | - |
| SIRS score (per score) | 1.30 (0.87–1.95) | 0.2078 | 0.568 (0.469–0.668) | - | - | - |
| qSOFA score (per score) | 3.82 (1.69–8.63) | 0.0012 * | 0.634 (0.553–0.715) | |||
| Hypertension | 2.43 (1.14–5.20) | 0.0222 * | 0.604 (0.515–0.693) | - | - | - |
| Diabetes mellitus | 0.96 (0.41–2.29) | 0.9299 | 0.504 (0.426–0.581) | - | - | - |
| Coronary artery disease | 2.33 (0.90–6.07) | 0.0825 | 0.563 (0.490–0.635) | - | - | - |
| Charlson Comorbidity Index | 1.22 (1.01–1.46) | 0.0399 * | 0.628 (0.529–0.728) | - | - | - |
| MDW | 1.13 (1.04–1.24) | 0.0070 * | 0.631 (0.531–0.731) | 21 | - | - |
| MDW ≥ 21 | 8.07 (1.78–36.52) | 0.0067 * | 0.611 (0.552–0.670) | - | 95.7% (86.5–99.5%) | 27.4% (17.6–39.1%) |
| WBC | 1.00 (1.00–1.00) | 0.8872 | 0.490 (0.383–0.597) | - | - | - |
| RDW | 0.89 (0.64–1.25) | 0.5114 | 0.491 (0.385–0.598) | - | - | - |
| CRP | 1.10 (1.03–1.18) | 0.0071 * | 0.654 (0.555–0.753) | 3 | - | - |
| CRP > 3 mg/dL | 2.26 (1.07–4.77) | 0.0319 * | 0.601 (0.511–0.691) | - | 60.4% (45.3–74.2%) | 59.7% (47.5–71.1%) |
| PCT | 1.46 (0.87–2.46) | 0.1530 | 0.661 (0.561–0.762) | - | - | - |
| NLR | 1.08 (1.01–1.16) | 0.0253 * | 0.628 (0.523–0.733) | - | - | - |
| NLR > 3 | 3.04 (1.32–7.02) | 0.0093 * | 0.618 (0.536–0.700) | 3 | 79.2% (65.0–89.5%) | 44.4% (32.7–56.6%) |
| PLR | 1.00 (1.00–1.00) | 0.5714 | 0.536 (0.431–0.641) | - | - | - |
| Characteristic | Model 1 a OR (95% CI) | p Value | Model 2 b OR (95% CI) | p Value | Points Assigned for Model 3 c | Model 3 a OR (95% CI) |
|---|---|---|---|---|---|---|
| Variable | ||||||
| Age > 60 years | 1.85 (0.55–6.19) | 0.3208 | - | - | - | - |
| Sex (male vs. female) | 1.48 (0.60–3.67) | 0.4001 | - | - | - | - |
| BT > 38 °C | 2.46 (0.92–6.55) | 0.0717 | 2.82 (1.13–7.02) | 0.0259 * | 1 | |
| RR > 20 breaths/min | 3.74 (1.12–12.54) | 0.0320 * | 4.76 (1.67–13.55) | 0.0034 * | 2 | |
| SpO2 < 96% | 0.78 (0.28–2.20) | 0.6356 | - | - | - | - |
| Hypertension | 1.55 (0.60–4.01) | 0.3720 | - | - | - | - |
| MDW ≥ 21 | 4.72 (0.92–24.15) | 0.0624 | 5.67 (1.19–27.10) | 0.0296 * | 3 | |
| CRP > 3 mg/dL | 0.88 (0.29–2.69) | 0.8274 | - | - | - | - |
| NLR < 3 | 1.68 (0.54–5.22) | 0.3705 | - | - | - | - |
| Charlson Comorbidity Index | 0.95 (0.70–1.30) | 0.7545 | - | - | - | - |
| New score (per score) | 2.10 (1.48–2.99) | |||||
| Model fit | ||||||
| AUC (95% CI) | 0.787 (0.701–0.874) | 0.749 (0.665–0.833) | 0.749 (0.665–0.833) | |||
| AIC | 161.68 | 140.97 | 137.66 | |||
| Hosmer–Lemeshow test | 8.785 (10 groups) | 0.3607 | 3.381 (6 groups) | 0.4963 | 4.270 (6 groups) |
| Characteristic | Sensitivity (95% CI) | Specificity (95% CI) | Youden’s Index |
|---|---|---|---|
| Score by using Model 3 | |||
| ≥1 | 93.8% (86.9%–100.0%) | 22.2% (12.6%–31.8%) | 16.0% |
| ≥2 | 93.8% (86.9%–100.0%) | 23.6% (13.8%–33.4%) | 17.4% |
| ≥3 | 93.8% (86.9%–100.0%) | 26.4% (16.2%–36.7%) | 20.2% |
| ≥4 | 58.3% (44.4%–72.3%) | 77.8% (68.2%–87.4%) | 36.1% * |
| ≥5 | 35.4% (21.9%–49.0%) | 93.1% (87.2%–98.3%) | 28.4% |
| ≥6 | 18.8% (7.8%–29.8%) | 100.0% (100.0%–100.0%) | 18.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.-F.; Lin, H.-A.; Chuang, H.-C.; Tsai, H.-W.; Kuo, N.; Chen, S.-C.; Hou, S.-K. Fever, Tachypnea, and Monocyte Distribution Width Predicts Length of Stay for Patients with COVID-19: A Pioneer Study. J. Pers. Med. 2022, 12, 449. https://doi.org/10.3390/jpm12030449
Lin S-F, Lin H-A, Chuang H-C, Tsai H-W, Kuo N, Chen S-C, Hou S-K. Fever, Tachypnea, and Monocyte Distribution Width Predicts Length of Stay for Patients with COVID-19: A Pioneer Study. Journal of Personalized Medicine. 2022; 12(3):449. https://doi.org/10.3390/jpm12030449
Chicago/Turabian StyleLin, Sheng-Feng, Hui-An Lin, Han-Chuan Chuang, Hung-Wei Tsai, Ning Kuo, Shao-Chun Chen, and Sen-Kuang Hou. 2022. "Fever, Tachypnea, and Monocyte Distribution Width Predicts Length of Stay for Patients with COVID-19: A Pioneer Study" Journal of Personalized Medicine 12, no. 3: 449. https://doi.org/10.3390/jpm12030449