
Predictors of Efavirenz Plasma Exposure, Auto-Induction Profile, and Effect of Pharmacogenetic Variations among HIV-Infected Children in Ethiopia: A Prospective Cohort Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Area, and Participants
2.2. Antiretroviral Therapy and Laboratory Analysis
2.3. Genotyping for CYP2B6, CYP3A5, SLCO1B1, ABCB1, and UGT2B7
2.4. Quantification of Efavirenz Plasma Concentration
2.4.1. Chemicals and Reagents
2.4.2. LC-MS/MS Method and Validation
2.5. Statistical Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Baseline Characteristics of Study Participants
3.2. Genotype and Allele Frequency Distribution
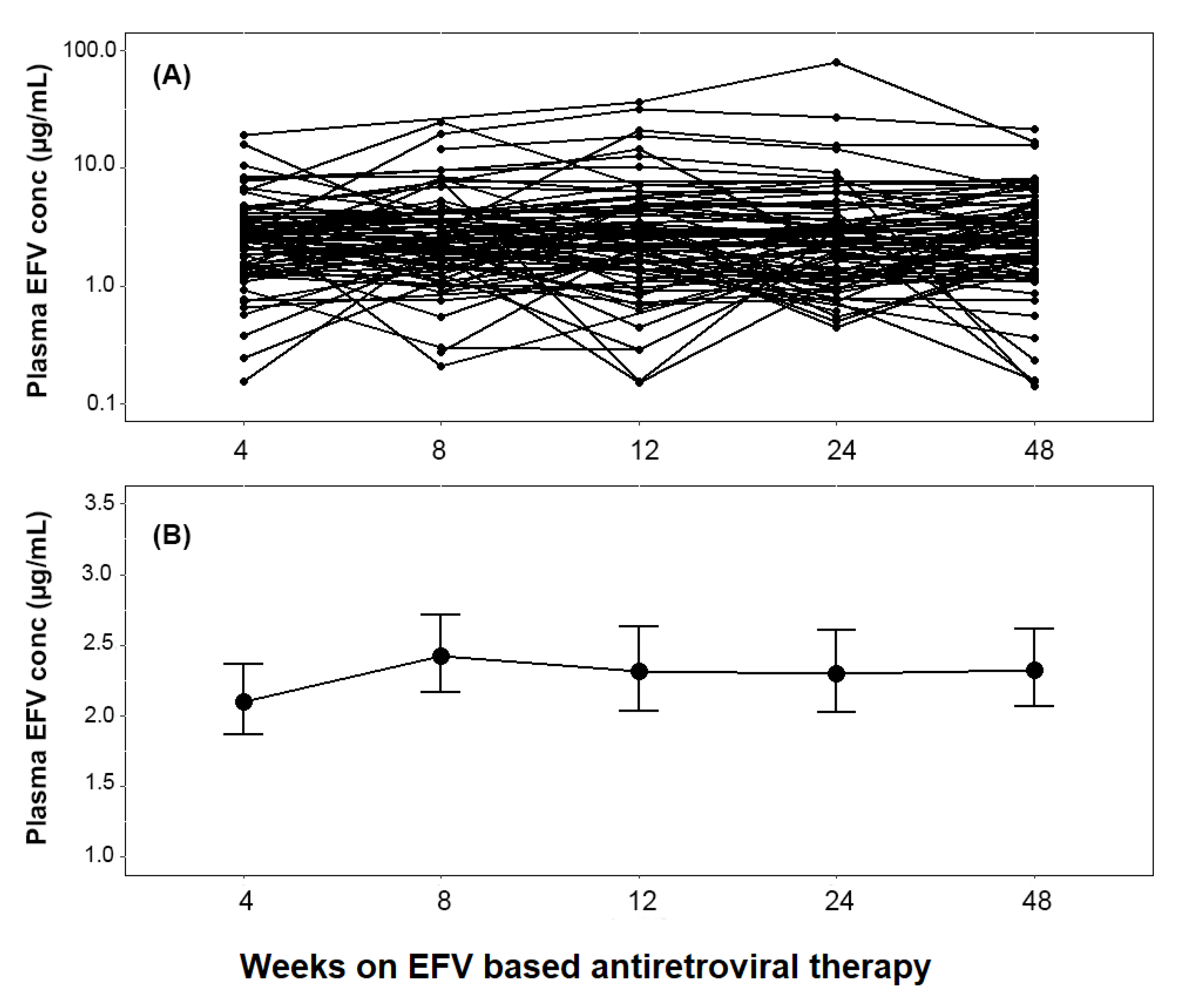
3.3. Change in Plasma Efavirenz Concentration over Time
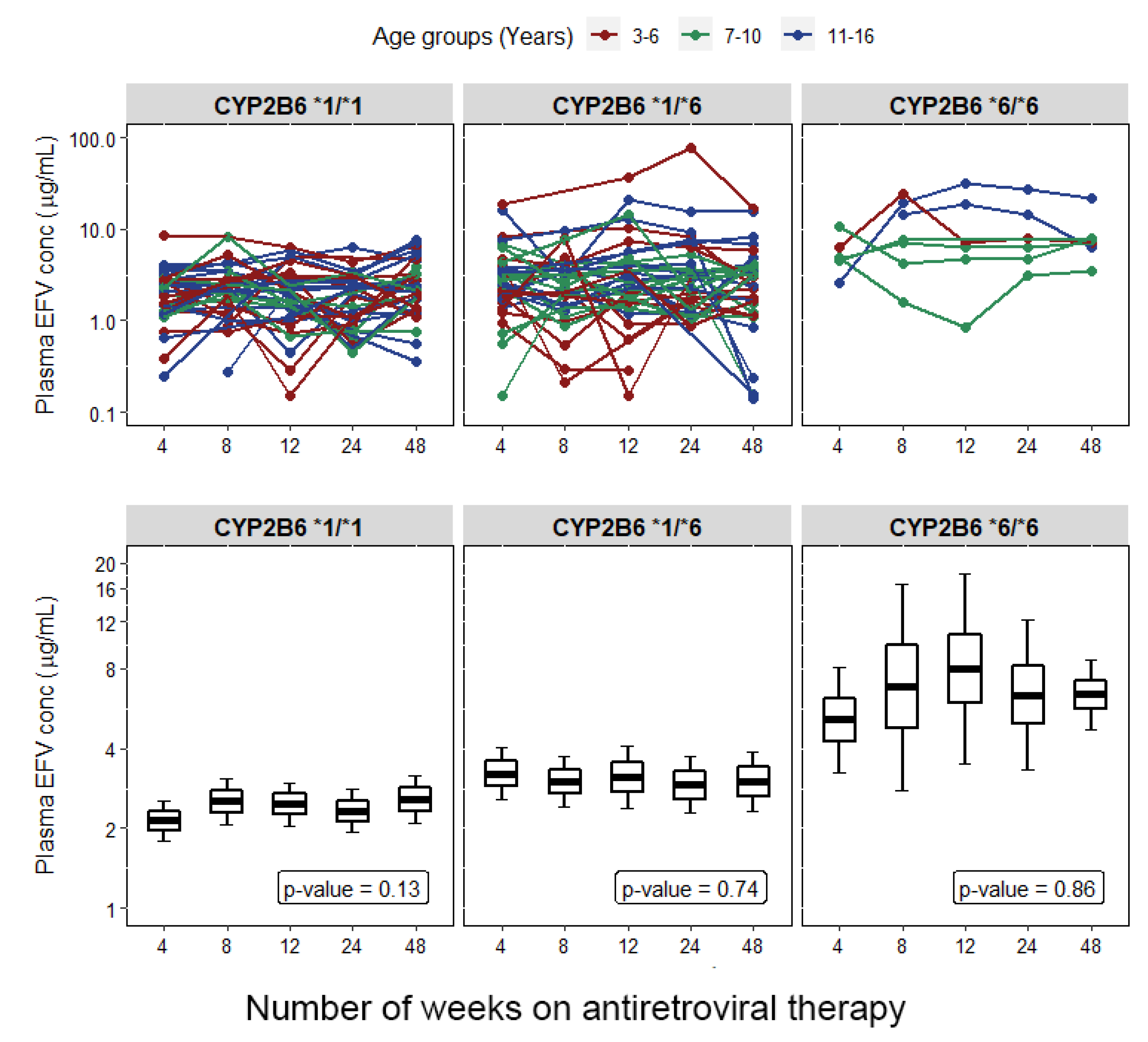
3.4. Effect of Genotype on Plasma Efavirenz Concentration at Each Study Time Point
3.5. Predictors of Plasma Efavirenz Exposure over Time
3.6. Predictors of Efavirenz Concentration over Time among CYP2B6 *1/*1 Genotype
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Global HIV & AIDS Statistics—2020 Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 10 August 2021).
- UNAIDS. Fast-Track, Ending the AIDS Epidemic by 2030, UNAIDS World AIDS Day Report 2014, JC2686. Available online: https://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014report_en.pdf (accessed on 10 August 2021).
- World Health Organization. Paediatric Antiretroviral Drug Optimization (PADO) Meeting 4. Meeting Report—10–12 December 2018. Available online: https://www.who.int/hiv/pub/meetingreports/paediatric-arv-optimization-pado4/en/ (accessed on 22 October 2021).
- World Health Organization. Update of Recommendations on First- and Second-Line Antiretroviral Regimens. Geneva, Switzerland: Licence: CC BY-NC-SA 3.0 IGO. Available online: https://apps.who.int/iris/bitstream/handle/10665/325892/WHO-CDS-HIV-19.15-eng.pdf?ua=1 (accessed on 22 July 2021).
- Tadesse, B.T.; Chala, A.; Mukonzo, J.; Chaka, T.E.; Tadesse, S.; Makonnen, E.; Brumme, Z.L.; Brumme, C.J.; Aklillu, E. Rates and Correlates of Short Term Virologic Response among Treatment-Naive HIV-Infected Children Initiating Antiretroviral Therapy in Ethiopia: A Multi-Center Prospective Cohort Study. Pathogens 2019, 8, 161. [Google Scholar] [CrossRef] [Green Version]
- Tadesse, B.T.; Foster, B.A.; Latour, E.; Lim, J.Y.; Jerene, D.; Ruff, A.; Aklillu, E. Predictors of Virologic Failure Among a Cohort of HIV-infected Children in Southern Ethiopia. Pediatr. Infect. Dis. J. 2021, 40, 60–65. [Google Scholar] [CrossRef]
- Tadesse, B.T.; Kinloch, N.N.; Baraki, B.; Lapointe, H.R.; Cobarrubias, K.D.; Brockman, M.A.; Brumme, C.J.; Foster, B.A.; Jerene, D.; Makonnen, E.; et al. High Levels of Dual-Class Drug Resistance in HIV-Infected Children Failing First-Line Antiretroviral Therapy in Southern Ethiopia. Viruses 2018, 10, 60. [Google Scholar] [CrossRef] [Green Version]
- Tadesse, B.T.; Tsai, O.; Chala, A.; Chaka, T.E.; Eromo, T.; Lapointe, H.R.; Baraki, B.; Shahid, A.; Tadesse, S.; Makonnen, E.; et al. Prevalence and Correlates of Pre-Treatment HIV Drug Resistance among HIV-Infected Children in Ethiopia. Viruses 2019, 11, 877. [Google Scholar] [CrossRef] [Green Version]
- Tadesse, B.T.; Foster, B.A.; Chala, A.; Chaka, T.E.; Bizuayehu, T.; Ayalew, F.; Tadesse, S.; Jerene, D.; Makonnen, E.; Tadesse, B.T.; et al. HIV and cART-Associated Dyslipidemia Among HIV-Infected Children. J. Clin. Med. 2019, 8, 430. [Google Scholar] [CrossRef] [Green Version]
- Tadesse, B.T.; Foster, B.A.; Kabeta, A.; Ayalew, F.; H/Meskel, G.; Jerene, D.; Makonnen, E.; Aklillu, E. Hepatic and renal toxicity and associated factors among HIV-infected children on antiretroviral therapy: A prospective cohort study. HIV Med. 2019, 20, 147–156. [Google Scholar] [CrossRef] [PubMed]
- EFMOH. Ministry of Health Federal Democratic Republic of Ethiopia: National Guidelunes for Comprehensive HIV Prevention, Care and Treatment. 2017, pp. 44–46. Available online: https://www.afro.who.int/sites/default/files/2019-04/National%20Comprehensive%20HIV%20Care%20%20Guideline%202018.pdf (accessed on 18 August 2021).
- McDonagh, E.M.; Lau, J.L.; Alvarellos, M.L.; Altman, R.B.; Klein, T.E. PharmGKB summary: Efavirenz pathway, pharmacokinetics. Pharm. Genom. 2015, 25, 363–376. [Google Scholar] [CrossRef] [Green Version]
- Weiss, J.; Herzog, M.; Konig, S.; Storch, C.H.; Ketabi-Kiyanvash, N.; Haefeli, W.E. Induction of multiple drug transporters by efavirenz. J. Pharmacol. Sci. 2009, 109, 242–250. [Google Scholar] [CrossRef] [Green Version]
- Burhenne, J.; Matthee, A.K.; Pasakova, I.; Roder, C.; Heinrich, T.; Haefeli, W.E.; Mikus, G.; Weiss, J. No evidence for induction of ABC transporters in peripheral blood mononuclear cells in humans after 14 days of efavirenz treatment. Antimicrob. Agents Chemother. 2010, 54, 4185–4191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukonzo, J.K.; Röshammar, D.; Waako, P.; Andersson, M.; Fukasawa, T.; Milani, L.; Svensson, J.O.; Ogwal-Okeng, J.; Gustafsson, L.L.; Aklillu, E. A novel polymorphism in ABCB1 gene, CYP2B6* 6 and sex predict single-dose efavirenz population pharmacokinetics in Ugandans. Br. J. Clin. Pharmacol. 2009, 68, 690–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukonzo, J.K.; Okwera, A.; Nakasujja, N.; Luzze, H.; Sebuwufu, D.; Ogwal-Okeng, J.; Waako, P.; Gustafsson, L.L.; Aklillu, E. Influence of efavirenz pharmacokinetics and pharmacogenetics on neuropsychological disorders in Ugandan HIV-positive patients with or without tuberculosis: A prospective cohort study. BMC Infect. Dis. 2013, 13, 261. [Google Scholar] [CrossRef] [Green Version]
- Swart, M.; Ren, Y.; Smith, P.; Dandara, C. ABCB1 4036A>G and 1236C>T Polymorphisms Affect Plasma Efavirenz Levels in South African HIV/AIDS Patients. Front. Genet. 2012, 3, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngaimisi, E.; Habtewold, A.; Minzi, O.; Makonnen, E.; Mugusi, S.; Amogne, W.; Yimer, G.; Riedel, K.D.; Janabi, M.; Aderaye, G.; et al. Importance of ethnicity, CYP2B6 and ABCB1 genotype for efavirenz pharmacokinetics and treatment outcomes: A parallel-group prospective cohort study in two sub-Saharan Africa populations. PLoS ONE 2013, 8, e67946. [Google Scholar] [CrossRef] [Green Version]
- Mugusi, S.; Habtewold, A.; Ngaimisi, E.; Amogne, W.; Yimer, G.; Minzi, O.; Makonnen, E.; Sudfeld, C.; Burhenne, J.; Aklillu, E. Impact of Population and Pharmacogenetics Variations on Efavirenz Pharmacokinetics and Immunologic Outcomes During Anti-Tuberculosis Co-Therapy: A Parallel Prospective Cohort Study in Two Sub-Sahara African Populations. Front. Pharmacol. 2020, 11, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukonzo, J.K.; Bisaso, R.K.; Ogwal-Okeng, J.; Gustafsson, L.L.; Owen, J.S.; Aklillu, E. CYP2B6 genotype-based efavirenz dose recommendations during rifampicin-based antituberculosis cotreatment for a sub-Saharan Africa population. Pharmacogenomics 2016, 17, 603–613. [Google Scholar] [CrossRef]
- Mukonzo, J.K.; Owen, J.S.; Ogwal-Okeng, J.; Kuteesa, R.B.; Nanzigu, S.; Sewankambo, N.; Thabane, L.; Gustafsson, L.L.; Ross, C.; Aklillu, E. Pharmacogenetic-based efavirenz dose modification: Suggestions for an African population and the different CYP2B6 genotypes. PLoS ONE 2014, 9, e86919. [Google Scholar] [CrossRef]
- Dhoro, M.; Zvada, S.; Ngara, B.; Nhachi, C.; Kadzirange, G.; Chonzi, P.; Masimirembwa, C. CYP2B6*6, CYP2B6*18, Body weight and sex are predictors of efavirenz pharmacokinetics and treatment response: Population pharmacokinetic modeling in an HIV/AIDS and TB cohort in Zimbabwe. BMC Pharm. Toxicol. 2015, 16, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Group, E.S.; Carey, D.; Puls, R.; Amin, J.; Losso, M.; Phanupak, P.; Foulkes, S.; Mohapi, L.; Crabtree-Ramirez, B.; Jessen, H.; et al. Efficacy and safety of efavirenz 400 mg daily versus 600 mg daily: 96-week data from the randomised, double-blind, placebo-controlled, non-inferiority ENCORE1 study. Lancet Infect. Dis. 2015, 15, 793–802. [Google Scholar] [CrossRef] [Green Version]
- Dickinson, L.; Amin, J.; Else, L.; Boffito, M.; Egan, D.; Owen, A.; Khoo, S.; Back, D.; Orrell, C.; Clarke, A.; et al. Pharmacokinetic and Pharmacodynamic Comparison of Once-Daily Efavirenz (400 mg vs. 600 mg) in Treatment-Naive HIV-Infected Patients: Results of the ENCORE1 Study. Clin. Pharm. Ther. 2015, 98, 406–416. [Google Scholar] [CrossRef] [PubMed]
- (WHO), W.H.O. World Health Organization (2016): Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for A Public Health Approach—Second Edition. Available online: http://apps.who.int/iris/bitstream/10665/208825/1/9789241549684_eng.pdf?ua=1 (accessed on 11 January 2021).
- Mukonzo, J.K. The challenge of paediatric efavirenz dosing: Implications and way forward for the sub-Saharan Africa. AIDS 2014, 28, 1855–1857. [Google Scholar] [CrossRef]
- World Health Organization. Optimizing Treatment Options and Improving Access to Priority Products for Children Living with HIV. Available online: http://www.who.int/hiv/pub/toolkits/brief-optimization-paedriatic-art.pdf?ua=1 (accessed on 18 August 2021).
- Ren, Y.; Nuttall, J.J.; Egbers, C.; Eley, B.S.; Meyers, T.M.; Smith, P.J.; Maartens, G.; McIlleron, H.M. High prevalence of subtherapeutic plasma concentrations of efavirenz in children. J. Acquir. Immune Defic. Syndr. 2007, 45, 133–136. [Google Scholar] [CrossRef]
- Fillekes, Q.; Natukunda, E.; Balungi, J.; Kendall, L.; Bwakura-Dangarembizi, M.; Keishanyu, R.; Ferrier, A.; Lutakome, J.; Gibb, D.M.; Burger, D.M.; et al. Pediatric underdosing of efavirenz: A pharmacokinetic study in Uganda. J. Acquir. Immune Defic. Syndr. 2011, 58, 392–398. [Google Scholar] [CrossRef]
- Viljoen, M.; Karlsson, M.O.; Meyers, T.M.; Gous, H.; Dandara, C.; Rheeders, M. Influence of CYP2B6 516G>T polymorphism and interoccasion variability (IOV) on the population pharmacokinetics of efavirenz in HIV-infected South African children. Eur. J. Clin. Pharmacol. 2012, 68, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Habtewold, A.; Amogne, W.; Makonnen, E.; Yimer, G.; Riedel, K.D.; Ueda, N.; Worku, A.; Haefeli, W.E.; Lindquist, L.; Aderaye, G.; et al. Long-term effect of efavirenz autoinduction on plasma/peripheral blood mononuclear cell drug exposure and CD4 count is influenced by UGT2B7 and CYP2B6 genotypes among HIV patients. J. Antimicrob. Chemother. 2011, 66, 2350–2361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habtewold, A.; Aklillu, E.; Makonnen, E.; Yimer, G.; Bertilsson, L.; Burhenne, J.; Owen, J.S. Population Pharmacokinetic Model Linking Plasma and Peripheral Blood Mononuclear Cell Concentrations of Efavirenz and Its Metabolite, 8-Hydroxy-Efavirenz, in HIV Patients. Antimicrob. Agents Chemother. 2017, 61, e00207-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habtewold, A.; Aklillu, E.; Makonnen, E.; Amogne, W.; Yimer, G.; Aderaye, G.; Bertilsson, L.; Owen, J.S.; Burhenne, J. Long-Term Effect of Rifampicin-Based Anti-TB Regimen Coadministration on the Pharmacokinetic Parameters of Efavirenz and 8-Hydroxy-Efavirenz in Ethiopian Patients. J. Clin. Pharmacol. 2016, 56, 1538–1549. [Google Scholar] [CrossRef]
- Yimer, G.; Amogne, W.; Habtewold, A.; Makonnen, E.; Ueda, N.; Suda, A.; Worku, A.; Haefeli, W.E.; Burhenne, J.; Aderaye, G.; et al. High plasma efavirenz level and CYP2B6*6 are associated with efavirenz-based HAART-induced liver injury in the treatment of naïve HIV patients from Ethiopia: A prospective cohort study. Pharm. J. 2012, 12, 499–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aklillu, E.; Zumla, A.; Habtewold, A.; Amogne, W.; Makonnen, E.; Yimer, G.; Burhenne, J.; Diczfalusy, U. Early or deferred initiation of efavirenz during rifampicin-based TB therapy has no significant effect on CYP3A induction in TB-HIV infected patients. Br. J. Pharmacol. 2021, 178, 3294–3308. [Google Scholar] [CrossRef]
- EMA (European Medicine Agency). Guideline on Bioanalytical Method Validation EMEA/CHMP/EWP/192217/2009 Rev. 1 Corr. 2. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-bioanalytical-method-validation_en.pdf (accessed on 18 August 2021).
- Mutagonda, R.F.; Kamuhabwa, A.A.R.; Minzi, O.M.S.; Massawe, S.N.; Asghar, M.; Homann, M.V.; Färnert, A.; Aklillu, E. Effect of pharmacogenetics on plasma lumefantrine pharmacokinetics and malaria treatment outcome in pregnant women. Malar J. 2017, 16, 267. [Google Scholar] [CrossRef]
- Gebeyehu, E.; Engidawork, E.; Bijnsdorp, A.; Aminy, A.; Diczfalusy, U.; Aklillu, E. Sex and CYP3A5 genotype influence total CYP3A activity: High CYP3A activity and a unique distribution of CYP3A5 variant alleles in Ethiopians. Pharm. J. 2011, 11, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faucette, S.R.; Zhang, T.C.; Moore, R.; Sueyoshi, T.; Omiecinski, C.J.; LeCluyse, E.L.; Negishi, M.; Wang, H. Relative activation of human pregnane X receptor versus constitutive androstane receptor defines distinct classes of CYP2B6 and CYP3A4 inducers. J. Pharmacol. Exp. Ther. 2007, 320, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Faucette, S.R.; Sueyoshi, T.; Smith, C.M.; Negishi, M.; Lecluyse, E.L.; Wang, H. Differential regulation of hepatic CYP2B6 and CYP3A4 genes by constitutive androstane receptor but not pregnane X receptor. J. Pharmacol. Exp. Ther. 2006, 317, 1200–1209. [Google Scholar] [CrossRef] [Green Version]
- Kitabi, E.N.; Minzi, O.M.S.; Mugusi, S.; Sasi, P.; Janabi, M.; Mugusi, F.; Bertilsson, L.; Burhenne, J.; Aklillu, E. Long-term efavirenz pharmacokinetics is comparable between Tanzanian HIV and HIV/Tuberculosis patients with the same CYP2B6*6 genotype. Sci. Rep. 2018, 8, 16316. [Google Scholar] [CrossRef]
- Ngaimisi, E.; Minzi, O.; Mugusi, S.; Sasi, P.; Riedel, K.D.; Suda, A.; Ueda, N.; Bakari, M.; Janabi, M.; Mugusi, F.; et al. Pharmacokinetic and pharmacogenomic modelling of the CYP3A activity marker 4beta-hydroxycholesterol during efavirenz treatment and efavirenz/rifampicin co-treatment. J. Antimicrob. Chemother. 2014, 69, 3311–3319. [Google Scholar] [CrossRef] [Green Version]
- Ngaimisi, E.; Mugusi, S.; Minzi, O.; Sasi, P.; Riedel, K.; Suda, A.; Ueda, N.; Janabi, M.; Mugusi, F.; Haefeli, W.; et al. Long-Term Efavirenz Autoinduction and Its Effect on Plasma Exposure in HIV Patients. Clin. Pharmacol. Ther. 2010, 88, 676–684. [Google Scholar] [CrossRef]
- Van de Wijer, L.; McHaile, D.N.; de Mast, Q.; Mmbaga, B.T.; Rommelse, N.N.J.; Duinmaijer, A.; van der Ven, A.; Schellekens, A.F.A.; Kinabo, G.D. Neuropsychiatric symptoms in Tanzanian HIV-infected children receiving long-term efavirenz treatment: A multicentre, cross-sectional, observational study. Lancet HIV 2019, 6, e250–e258. [Google Scholar] [CrossRef] [Green Version]
- Hammond, C.K.; Eley, B.; Ing, N.; Wilmshurst, J.M. Neuropsychiatric and Neurocognitive Manifestations in HIV-Infected Children Treated with Efavirenz in South Africa-A Retrospective Case Series. Front. Neurol. 2019, 10, 742. [Google Scholar] [CrossRef] [Green Version]
- Van de Wijer, L.; Schellekens, A.F.A.; Burger, D.M.; Homberg, J.R.; de Mast, Q.; van der Ven, A. Rethinking the risk-benefit ratio of efavirenz in HIV-infected children. Lancet Infect. Dis. 2016, 16, e76–e81. [Google Scholar] [CrossRef]
- Mukonzo, J.K.; Nanzigu, S.; Waako, P.; Ogwal-Okeng, J.; Gustafson, L.L.; Aklillu, E. CYP2B6 genotype, but not rifampicin-based anti-TB cotreatments, explains variability in long-term efavirenz plasma exposure. Pharmacogenomics 2014, 15, 1423–1435. [Google Scholar] [CrossRef]
- Habtewold, A.; Amogne, W.; Makonnen, E.; Yimer, G.; Nylen, H.; Riedel, K.D.; Aderaye, G.; Bertilsson, L.; Burhenne, J.; Diczfalusy, U.; et al. Pharmacogenetic and pharmacokinetic aspects of CYP3A induction by efavirenz in HIV patients. Pharm. J. 2013, 13, 484–489. [Google Scholar] [CrossRef] [Green Version]
- Nylén, H.; Habtewold, A.; Makonnen, E.; Yimer, G.; Bertilsson, L.; Burhenne, J.; Diczfalusy, U.; Aklillu, E. Prevalence and risk factors for efavirenz-based antiretroviral treatment–associated severe vitamin D deficiency: A prospective cohort study. Medicine 2016, 95. [Google Scholar] [CrossRef] [PubMed]
- Sinxadi, P.Z.; McIlleron, H.M.; Dave, J.A.; Smith, P.J.; Levitt, N.S.; Haas, D.W.; Maartens, G. Plasma Efavirenz Concentrations Are Associated with Lipid and Glucose Concentrations. Medicine 2016, 95, e2385. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Takada, T.; Yamanashi, Y.; Ogura, M.; Masuo, Y.; Harada-Shiba, M.; Suzuki, H. VLDL/LDL acts as a drug carrier and regulates the transport and metabolism of drugs in the body. Sci. Rep. 2017, 7, 633. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Categorical Variables | Proportion n (%) | |
|---|---|---|
| Sex | Male | 63 (56.8) |
| Female | 49(43.2) | |
| Height for age Z-score | Normal | 72 (66.1) |
| Stunted | 37 (33.9) | |
| Weight for age Z-score | Normal | 44 (62.9) |
| Underweight | 26 (37.1) | |
| BMI for age percentile | 5th–85th (Normal) | 60 (56.6) |
| <5th (Wasted) | 46 (43.4) | |
| Types of ART initiated | ABC/3TC/EFV | 36 (33) |
| AZT/3TC/EFV | 15 (13.6) | |
| TDF/3TC/EFV | 59 (53.6) | |
| Hepatitis B virus surface antigen | Negative | 106 (98.1) |
| Positive | 2 (1.9) | |
| Hepatitis B virus antibody | Negative | 105 (99.1) |
| Positive | 1 (0.9) | |
| WHO clinical stage | Stage 1 | 44 (39.6) |
| Stage 2 | 23 (20.7) | |
| Stage 3 | 33 (29.7) | |
| Stage 4 | 10 (9) | |
| Any co-medication | Yes | 13 (11.7) |
| No | 98 (88.3) | |
| Continuous Variables | Median (IQR) | |
| Age at enrolment (years) | 9.0 (5–13) | |
| Mid-upper arm circumference (cm) | 15 (14–17) | |
| CD4 count (cells/dL) | 330 (200–671) | |
| Viral load (copies/mL) | 16,105 (1987–75,761) | |
| Aspartate aminotransferase (units/L) | 38 (30–48) | |
| Alanine aminotransferase (units/L) | 27 (20–39) | |
| Alkaline phosphatase (units/L) | 304 (188–410) | |
| Blood urea nitrogen (mg/dL) | 18 (12–27) | |
| Total bilirubin (mg/dL) | 0.8 (0.4–1.1) | |
| Creatinine (mg/dL) | 0.6 (0.4–0.7) | |
| Albumin, median (mg/dl) | 3.8 (3.1–4.2) | |
| Hemoglobin (mg/dL) | 12.4 (11.5–13.3) | |
| Hematocrit (%) | 37.4 (35.1–40.5) | |
| Total cholesterol (mg/dL) | 119 (95–150) | |
| High-density lipoprotein (mg/dL) | 47 (35–65) | |
| Low-density lipoprotein (mg/dL) | 45 (33–64) | |
| Triglycerides (mg/dL) | 106 (87–162) | |
| Variant Allele | Minor Allele Frequency (%) | Genotype | Frequency (N)% |
|---|---|---|---|
| CYP2B6*6 | 30.1 | *1/*1 | 49 (47.6) |
| *1/*6 | 46 (44.6) | ||
| *6/*6 | 8 (7.8) | ||
| CYP3A5*3 | 67.0 | *1/*1 | 10 (9.7) |
| *1/*3 | 48 (46.6) | ||
| *3/*3 | 45 (43.7) | ||
| CYP3A5*6 | 10.2 | *1/*1 | 82 (79.6) |
| *1/*6 | 21 (20.4) | ||
| *6/*6 | 0 | ||
| ABCB1 c.3435 C > T | 19.4 | C/C | 66 (64.1) |
| C/T | 34 (33) | ||
| T/T | 3 (2.9) | ||
| ABCB1 c.4036A > G | 18.0 | A/A | 72 (69.9) |
| A/G | 25 (24.3) | ||
| G/G | 6 (5.8) | ||
| SLCO1B1 g.38664 C >T | 52.9 | C/C | 25 (24.3) |
| C/T | 47 (45.6) | ||
| T/T | 31 (30.1) | ||
| SLCO1B1*5 | 13.6 | *1/*1 | 78 (75.7) |
| *1/*5 | 22 (21.4) | ||
| *5/*5 | 3 (2.9) | ||
| SLCO1B1*1B | 64.1 | A/A | 12 (11.7) |
| A/G | 50 (48.5) | ||
| G/G | 41 (39.8) | ||
| UGT2B7*2 | 45.6 | G/G | 27 (26.2) |
| A/G | 58 (56.3) | ||
| A/A | 18 (17.5) |
| Predictor | Predictor Values | Univariate * | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient Estimates (Log10 Scale) | p | Between-Subject Variability | Within-Subject Variability | Coefficient Estimates (Log10 Scale) | p | Between-Subject Variability | Within-Subject Variability | ||
| Time on ART (Weeks) | Reference (Week 4) | 0.335 | 0.000 | 34% | 34% | 0.181 | 0.17 | 28% | 34% |
| Week 8 | 0.052 | 0.34 | 0.057 | 0.31 | |||||
| Week 12 | 0.024 | 0.67 | 0.017 | 0.77 | |||||
| Week 24 | −0.008 | 0.88 | −0.009 | 0.88 | |||||
| Week 48 | 0.003 | 0.95 | −0.006 | 0.91 | |||||
| Type of ART regimen | Reference (ABC/3TC/EFV) | 0.240 | 0.002 | 33% | 34% | ||||
| AZT/3TC/EFV | 0.040 | 0.77 | 0.038 | 0.75 | |||||
| TDF/3TC/EFV | 0.170 | 0.05 | 0.117 | 0.16 | |||||
| Baseline LDL | Intercept | 0.530 | 0.000 | 33% | 34% | ||||
| LDL | 0.0001 | 0.02 | −0.003 | 0.04 | |||||
| Age at enrollment | Intercept | 0.180 | 0.09 | 33% | 34% | ||||
| Age | 0.020 | 0.10 | 0.009 | 0.36 | |||||
| CYP2B6*6 | Reference (*1/*1) | 0.230 | 0.001 | 29% | 34% | ||||
| *1/*6 or *6/*6 | 0.610 | <0.0001 | 0.574 | 0.00 | |||||
| ABCB1 c.3435 C > T | Reference (C/C) | 0.280 | <0.0001 | 33% | 34% | ||||
| C/T or T/T | 0.180 | 0.03 | 0.173 | 0.03 | |||||
| Predictor | Predictor Values | Univariate * | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient Estimates (Log10 Scale) | p | Between-Subject Variability | Within-Subject Variability | Coefficient Estimates (Log10 Scale) | p | Between-Subject Variability | Within-Subject Variability | ||
| Time on treatment (Weeks) | Intercept (Week 4) | 0.159 | 0.02 | 27% | 28% | 0.145 | 0.51 | 22% | 26% |
| Week 8 | 0.166 | 0.02 | 0.151 | 0.03 | |||||
| Week 12 | 0.072 | 0.28 | 0.044 | 0.51 | |||||
| Week 24 | 0.014 | 0.83 | −0.030 | 0.66 | |||||
| Week 48 | 0.155 | 0.02 | 0.115 | 0.09 | |||||
| Baseline ALT | Intercept | 0.100 | 0.24 | 27% | 28% | ||||
| ALT | 0.000 | 0.18 | 0.004 | 0.03 | |||||
| Baseline ALP | Intercept | −0.070 | 0.48 | 24% | 28% | ||||
| ALP | 0.000 | 0.01 | 0.001 | 0.008 | |||||
| Baseline Total Cholesterol | Intercept | 0.310 | 0.01 | 27% | 27% | ||||
| Total Cholesterol | 0.000 | 0.19 | 0.003 | 0.03 | |||||
| Baseline LDL | Intercept | 0.390 | 0.00 | 25% | 28% | ||||
| LDL | 0.000 | 0.01 | −0.005 | 0.03 | |||||
| Baseline Triglycerides | Intercept | 0.360 | 0.01 | 27% | 28% | ||||
| Triglycerides | 0.000 | 0.07 | −0.003 | 0.02 | |||||
| ABCB1 c.4036A>G | Reference (A/A) | 0.100 | 0.16 | 27% | 27% | ||||
| A/G or G/G | 0.150 | 0.15 | 0.011 | 0.91 | |||||
| SLCO1B1 g.38664C>T | Reference (C/C) | 0.310 | 0.00 | 25% | 28% | ||||
| C/T or T/T | −0.220 | 0.04 | −0.205 | 0.09 | |||||
| SLCO1B1 *1B | Reference (A/A or A/G) | 0.230 | 0.00 | 27% | 27% | ||||
| G/G | −0.190 | 0.06 | 0.048 | 0.70 | |||||
| Baseline AST | Intercept | 0.120 | 0.08 | 26% | 28% | ||||
| AST | 0.220 | 0.08 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chala, A.; Tadesse, B.T.; Chaka, T.E.; Mukonzo, J.; Kitabi, E.N.; Tadesse, S.; Pohanka, A.; Makonnen, E.; Aklillu, E. Predictors of Efavirenz Plasma Exposure, Auto-Induction Profile, and Effect of Pharmacogenetic Variations among HIV-Infected Children in Ethiopia: A Prospective Cohort Study. J. Pers. Med. 2021, 11, 1303. https://doi.org/10.3390/jpm11121303
Chala A, Tadesse BT, Chaka TE, Mukonzo J, Kitabi EN, Tadesse S, Pohanka A, Makonnen E, Aklillu E. Predictors of Efavirenz Plasma Exposure, Auto-Induction Profile, and Effect of Pharmacogenetic Variations among HIV-Infected Children in Ethiopia: A Prospective Cohort Study. Journal of Personalized Medicine. 2021; 11(12):1303. https://doi.org/10.3390/jpm11121303
Chicago/Turabian StyleChala, Adugna, Birkneh Tilahun Tadesse, Tolossa Eticha Chaka, Jackson Mukonzo, Eliford Ngaimisi Kitabi, Sintayehu Tadesse, Anton Pohanka, Eyasu Makonnen, and Eleni Aklillu. 2021. "Predictors of Efavirenz Plasma Exposure, Auto-Induction Profile, and Effect of Pharmacogenetic Variations among HIV-Infected Children in Ethiopia: A Prospective Cohort Study" Journal of Personalized Medicine 11, no. 12: 1303. https://doi.org/10.3390/jpm11121303