
A Novel Noninvasive Technique for Intracranial Pressure Waveform Monitoring in Critical Care

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Clinical Variables
2.4. Invasive ICP Monitoring (Gold Standard)
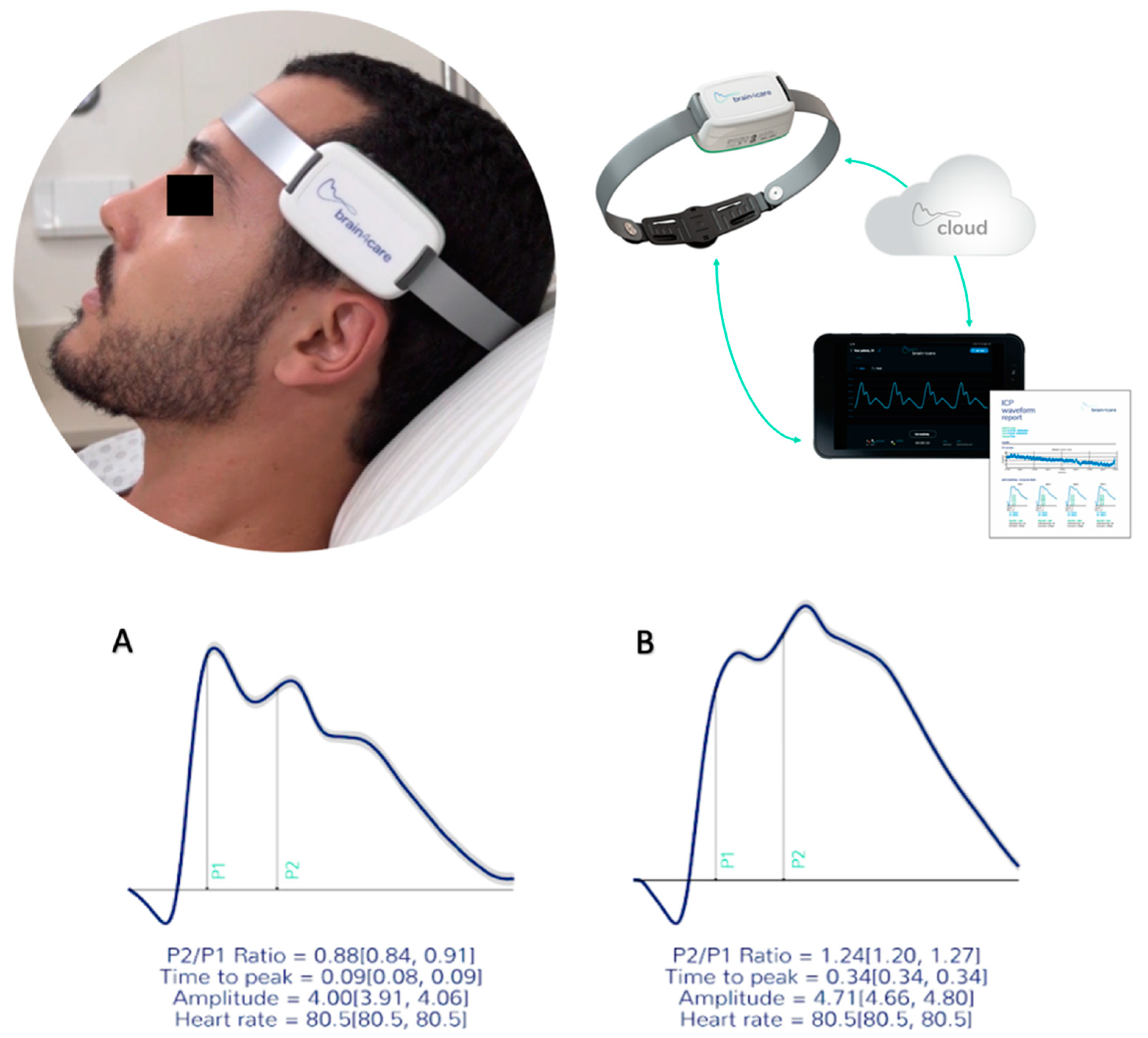
2.5. Noninvasive Intracranial Compliance Monitoring (B4C)
2.6. Sample
2.7. Statistical Analyses
3. Results
3.1. Sample Features
3.2. Correlation between ICP and B4C
4. Discussion
4.1. Main Findings
4.2. Limitations of the Study
4.3. B4C System Attributes
4.4. Considerations for the Future
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andrade, A.F.; Paiva, W.S.; Amorim, R.L.; Figueiredo, E.G.; Almeida, A.N.; Brock, R.S.; Bor-Seng-Shu, E.; Teixeira, M.J. Continuous ventricular cerebrospinal fluid drainage with intracranial pressure monitoring for management of posttraumatic diffuse brain swelling. Arq. Neuropsiquiatr. 2011, 69, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Robba, C.; Graziano, F.; Rebora, P.; Elli, F.; Giussani, C.; Oddo, M.; Meyfroidt, G.; Helbok, R.; Taccone, F.S.; Prisco, L.; et al. Intracranial pressure monitoring in patients with acute brain injury in the intensive care unit (SYNAPSE-ICU): An international, prospective observational cohort study. Lancet Neurol. 2021, 20, 548–558. [Google Scholar] [CrossRef]
- Cabella, B.; Vilela, G.H.; Mascarenhas, S.; Czosnyka, M.; Smielewski, P.; Dias, C.; Cardim, D.A.; Wang, C.C.; Mascarenhas, P.; Andrade, R.; et al. Validation of a New Noninvasive Intracranial Pressure Monitoring Method by Direct Comparison with an Invasive Technique. Acta Neurochir. Suppl. 2016, 122, 93–96. [Google Scholar] [CrossRef]
- Vilela, G.H.; Cabella, B.; Mascarenhas, S.; Czosnyka, M.; Smielewski, P.; Dias, C.; Cardim, D.A.; Mascarenhas, Y.M.; Wang, C.C.; Andrade, R.; et al. Validation of a New Minimally Invasive Intracranial Pressure Monitoring Method by Direct Comparison with an Invasive Technique. Acta Neurochir. Suppl. 2016, 122, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Frigieri, G.; Andrade, R.A.P.; Dias, C.; Spavieri, D.L.; Brunelli, R.; Cardim, D.A.; Wang, C.C.; Verzola, R.M.M.; Mascarenhas, S. Analysis of a Non-invasive Intracranial Pressure Monitoring Method in Patients with Traumatic Brain Injury. Acta Neurochir. Suppl. 2018, 126, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas, S.; Vilela, G.H.; Carlotti, C.; Damiano, L.E.; Seluque, W.; Colli, B.; Tanaka, K.; Wang, C.C.; Nonaka, K.O. The new ICP minimally invasive method shows that the Monro-Kellie doctrine is not valid. Acta Neurochir. Suppl. 2012, 114, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Bekar, A.; Dogan, S.; Abas, F.; Caner, B.; Korfali, G.; Kocaeli, H.; Yilmazlar, S.; Korfali, E. Risk factors and complications of intracranial pressure monitoring with a fiberoptic device. J. Clin. Neurosci. 2009, 16, 236–240. [Google Scholar] [CrossRef]
- Binz, D.D.; Toussaint, L.G.; Friedman, J.A. Hemorrhagic complications of ventriculostomy placement: A meta-analysis. Neurocrit. Care 2009, 10, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Paiva, W.S.; de Andrade, A.F.; Amorim, R.L.; Figueiredo, E.G.; Matushita, H.; Teixeira, M.J. Intracranial pressure monitoring in children with fulminant hepatic failure. Rev. Neurol. 2009, 48, 134–136. [Google Scholar]
- Ferreira, C.B.; Bassi, E.; Lucena, L.; Carreta, H.; Miranda, L.C.; Tierno, P.F.; Amorim, R.L.; Zampieri, F.G.; Malbouisson, L.M. Measurement of intracranial pressure and short-term outcomes of patients with traumatic brain injury: A propensity-matched analysis. Rev. Bras. Ter. Intensiva 2015, 27, 315–321. [Google Scholar] [CrossRef]
- Bor-Seng-Shu, E.; Figueiredo, E.G.; Amorim, R.L.; Teixeira, M.J.; Valbuza, J.S.; de Oliveira, M.M.; Panerai, R.B. Decompressive craniectomy: A meta-analysis of influences on intracranial pressure and cerebral perfusion pressure in the treatment of traumatic brain injury. J. Neurosurg. 2012, 117, 589–596. [Google Scholar] [CrossRef]
- Bhatia, A.; Gupta, A.K. Neuromonitoring in the intensive care unit. I. Intracranial pressure and cerebral blood flow monitoring. Intensive Care Med. 2007, 33, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Czosnyka, M.; Hutchinson, P.J.; Balestreri, M.; Hiler, M.; Smielewski, P.; Pickard, J.D. Monitoring and interpretation of intracranial pressure after head injury. Acta Neurochir. Suppl. 2006, 96, 114–118. [Google Scholar] [CrossRef]
- Fan, J.Y.; Kirkness, C.; Vicini, P.; Burr, R.; Mitchell, P. Intracranial pressure waveform morphology and intracranial adaptive capacity. Am. J. Crit. Care 2008, 17, 545–554. [Google Scholar] [CrossRef]
- Nucci, C.G.; de Bonis, P.; Mangiola, A.; Santini, P.; Sciandrone, M.; Risi, A.; Anile, C. Intracranial pressure wave morphological classification: Automated analysis and clinical validation. Acta Neurochir. 2016, 158, 581–588. [Google Scholar] [CrossRef]
- Jeng, B.C.P.; de Andrade, A.F.; Brasil, S.; Bor-Seng-Shu, E.; Belon, A.R.; Robertis, M.; de-Lima-Oliveira, M.; Rubiano, A.M.; Godoy, D.A.; Teixeira, M.J.; et al. Estimation of intracranial pressure by ultrasound of the optic nerve sheath in an animal model of intracranial hypertension. J. Clin. Neurosci. 2021, 86, 174–179. [Google Scholar] [CrossRef]
- Robba, C.; Pozzebon, S.; Moro, B.; Vincent, J.L.; Creteur, J.; Taccone, F.S. Multimodal non-invasive assessment of intracranial hypertension: An observational study. Crit. Care 2020, 24, 379. [Google Scholar] [CrossRef] [PubMed]
- Portella, G.; Cormio, M.; Citerio, G.; Contant, C.; Kiening, K.; Enblad, P.; Piper, I. Continuous cerebral compliance monitoring in severe head injury: Its relationship with intracranial pressure and cerebral perfusion pressure. Acta Neurochir. 2005, 147, 707–713. [Google Scholar] [CrossRef]
- Brasil, S.; Bor-Seng-Shu, E.; de-Lima-Oliveira, M.; Taccone, F.S.; Gattas, G.; Nunes, D.M.; Gomes de Oliveira, R.A.; Martins Tomazini, B.; Tierno, P.F.; Becker, R.A.; et al. Computed tomography angiography accuracy in brain death diagnosis. J. Neurosurg. 2019, 133, 1220–1228. [Google Scholar] [CrossRef] [PubMed]
- Czosnyka, M.; Smielewski, P.; Timofeev, I.; Lavinio, A.; Guazzo, E.; Hutchinson, P.; Pickard, J.D. Intracranial pressure: More than a number. Neurosurg. Focus 2007, 22, E10. [Google Scholar] [CrossRef]
- Nag, D.S.; Sahu, S.; Swain, A.; Kant, S. Intracranial pressure monitoring: Gold standard and recent innovations. World J. Clin. Cases 2019, 7, 1535–1553. [Google Scholar] [CrossRef] [PubMed]
- Frigieri, G.; Andrade, R.A.P.; Wang, C.C.; Spavieri, D.; Lopes, L.; Brunelli, R.; Cardim, D.A.; Verzola, R.M.M.; Mascarenhas, S. Analysis of a Minimally Invasive Intracranial Pressure Signals During Infusion at the Subarachnoid Spinal Space of Pigs. Acta Neurochir. Suppl. 2018, 126, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Cardim, D.; Robba, C.; Donnelly, J.; Bohdanowicz, M.; Schmidt, B.; Damian, M.; Varsos, G.V.; Liu, X.; Cabeleira, M.; Frigieri, G.; et al. Prospective Study on Noninvasive Assessment of Intracranial Pressure in Traumatic Brain-Injured Patients: Comparison of Four Methods. J. Neurotrauma 2016, 33, 792–802. [Google Scholar] [CrossRef] [Green Version]
- Ballestero, M.F.M.; Frigieri, G.; Cabella, B.C.T.; de Oliveira, S.M.; de Oliveira, R.S. Prediction of intracranial hypertension through noninvasive intracranial pressure waveform analysis in pediatric hydrocephalus. Childs Nerv. Syst. 2017, 33, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, T.Y.; Venkatraghavan, L.; Fisher, J.A.; Meineri, M. Internal jugular vein blood flow in the upright position during external compression and increased central venous pressure: An ultrasound study in healthy volunteers. Can. J. Anesth. 2017, 64, 854–859. [Google Scholar] [CrossRef]
- Holmlund, P.; Johansson, E.; Qvarlander, S.; Wahlin, A.; Ambarki, K.; Koskinen, L.D.; Malm, J.; Eklund, A. Human jugular vein collapse in the upright posture: Implications for postural intracranial pressure regulation. Fluids Barriers CNS 2017, 14, 17. [Google Scholar] [CrossRef]
- Andrade, R.d.A.P.; Oshiro, H.E.; Miyazaki, C.K.; Hayashi, C.Y.; Morais, M.A.; Brunelli, R.; Carmo, J.P. A nanometer resolution wearable wireless medical device for non invasive intracranial pressure monitoring. IEEE Sens. J. 2021, 21, 22270–22284. [Google Scholar] [CrossRef]
- Gomes, I.; Shibaki, J.; Padua, B.; Silva, F.; Goncalves, T.; Spavieri-Junior, D.L.; Frigieri, G.; Mascarenhas, S.; Dias, C. Comparison of Waveforms Between Noninvasive and Invasive Monitoring of Intracranial Pressure. Acta Neurochir. Suppl. 2021, 131, 135–140. [Google Scholar] [CrossRef]
- Czosnyka, M.; Czosnyka, Z. Origin of intracranial pressure pulse waveform. Acta Neurochir. 2020, 162, 1815–1817. [Google Scholar] [CrossRef]
- Brasil, S.; Solla, D.J.F.; Nogueira, R.d.C.; Jacobsen Teixeira, M.; Malbouisson, L.M.S.; Paiva, W.S. Intracranial Compliance Assessed by Intracranial Pressure Pulse Waveform. Brain Sci. 2021, 11, 971. [Google Scholar] [CrossRef]
- Hertzog, M.A. Considerations in determining sample size for pilot studies. Res. Nurs. Health 2008, 31, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Nunes Rabelo, N.; Goncalves de Sena Barbosa, M.; Pereira Silva Lemos, M.; Brasil, S.; Frigieri, G. Letter to the Editor. Intracranial pressure monitoring: Challenge beyond the threshold numerical value. J. Neurosurg. 2020, 134, 1682–1683. [Google Scholar] [CrossRef] [PubMed]
- Kazimierska, A.; Kasprowicz, M.; Czosnyka, M.; Placek, M.M.; Baledent, O.; Smielewski, P.; Czosnyka, Z. Compliance of the cerebrospinal space: Comparison of three methods. Acta Neurochir. 2021, 163, 1979–1989. [Google Scholar] [CrossRef]
- Asgari, S.; Bergsneider, M.; Hamilton, R.; Vespa, P.; Hu, X. Consistent changes in intracranial pressure waveform morphology induced by acute hypercapnic cerebral vasodilatation. Neurocrit. Care 2011, 15, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Hall, A.; O’Kane, R. The best marker for guiding the clinical management of patients with raised intracranial pressure-the RAP index or the mean pulse amplitude? Acta Neurochir. 2016, 158, 1997–2009. [Google Scholar] [CrossRef] [Green Version]
- Tokutomi, T.; Shigemori, M.; Yuge, T.; Yamamoto, F.; Watanabe, M.; Kuramoto, S.; Goto, S. Analysis of pulse wave recorded on epidural pressure in acute intracranial hypertension. Neurol. Med. Chir. 1985, 25, 418–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brasil, S.; Taccone, F.; Wayhs, S.; Tomazini, B.; Annoni, F.; Fonseca, S.; Bassi, E.; Lucena, B.; Nogueira, R.; de-Lima-Oliveira, M.; et al. Cerebral Hemodynamics and Intracranial Compliance Impairment in Critically Ill Covid-19 Patients: A Pilot Study. Sci. Rep. 2021, 11, 874. [Google Scholar] [CrossRef]
- Brasil, S.; Renck, A.C.; Taccone, F.S.; Fontoura Solla, D.J.; Tomazini, B.M.; Wayhs, S.Y.; Fonseca, S.; Bassi, E.; Lucena, B.; De Carvalho Nogueira, R.; et al. Obesity and its implications on cerebral circulation and intracranial compliance in severe COVID-19. Obes. Sci. Pract. 2021, 23, 45–57. [Google Scholar] [CrossRef]
- Rickli, C.; Cosmoski, L.D.; Dos Santos, F.A.; Frigieri, G.H.; Rabelo, N.N.; Schuinski, A.M.; Mascarenhas, S.; Vellosa, J.C.R. Use of non-invasive intracranial pressure pulse waveform to monitor patients with End-Stage Renal Disease (ESRD). PLoS ONE 2021, 16, e0240570. [Google Scholar] [CrossRef] [PubMed]
- Connolly, M.; He, X.; Gonzalez, N.; Vespa, P.; DiStefano, J.; Hu, X. Reproduction of consistent pulse-waveform changes using a computational model of the cerebral circulatory system. Med. Eng. Phys. 2014, 36, 354–363. [Google Scholar] [CrossRef] [Green Version]
- Frigieri, G.; Rabelo, N.; Nogueira, R.; Brasil, S. Management of Patients with Brain Injury Using Noninvasive Methods. Adv. New Underst. Brain Inj. 2020, 337, 671–702. [Google Scholar] [CrossRef]
- Citerio, G.; Oddo, M.; Taccone, F.S. Recommendations for the use of multimodal monitoring in the neurointensive care unit. Curr. Opin. Crit. Care 2015, 21, 113–119. [Google Scholar] [CrossRef]
- Casault, C.; Couillard, P.; Kromm, J.; Rosenthal, E.; Kramer, A.; Brindley, P. Multimodal brain monitoring following traumatic brain injury: A primer for intensive care practitioners. J. Intensive Care Soc. 2020, 127, 232–259. [Google Scholar] [CrossRef]
- Evensen, K.B.; Eide, P.K. Measuring intracranial pressure by invasive, less invasive or non-invasive means: Limitations and avenues for improvement. Fluids Barriers CNS 2020, 17, 34. [Google Scholar] [CrossRef]
- Chesnut, R.M.; Temkin, N.; Carney, N.; Dikmen, S.; Rondina, C.; Videtta, W.; Petroni, G.; Lujan, S.; Pridgeon, J.; Barber, J.; et al. A trial of intracranial-pressure monitoring in traumatic brain injury. N. Engl. J. Med. 2012, 367, 2471–2481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paschoal, F.M.J.; Nogueira, R.C.; Oliveira, M.L.; Paschoal, E.H.A.; Teixeira, M.J.; D’Albuquerque, L.A.C.; Bor-Seng-Shu, E. Cerebral hemodynamic and metabolic changes in fulminant hepatic failure. Arq. Neuropsiquiatr. 2017, 75, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Vinters, H.V.; Magaki, S.D.; Williams, C.K. Neuropathologic Findings in Chronic Kidney Disease (CKD). J. Stroke Cerebrovasc. Dis. 2021, 12, 181–203. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.M.; Geocadin, R.G.; Caturegli, G.; Chan, V.; White, B.; Dodd, O.J.; Kim, B.S.; Sussman, M.; Choi, C.W.; Whitman, G.; et al. Understanding Characteristics of Acute Brain Injury in Adult Extracorporeal Membrane Oxygenation: An Autopsy Study. Crit. Care Med. 2020, 48, e532–e536. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (41) |
|---|---|
| Age | 37.6 ± 28.2 (18; 78) |
| Male sex | 22 (53%) |
| Pathology | |
| Traumatic brain injury | 21 (51%) |
| Marshall III | 5 (24%) |
| Marshall V | 16 (76%) |
| Subarachnoid hemorrhage | 13 (31%) |
| Modified Fisher IV | 13 (100%) |
| Stroke | 6 (14%) |
| Tumor | 1 (2%) |
| Neurosurgery | |
| No | 12 (29%) |
| Craniotomy | 20 (48%) |
| Craniectomy | 9 (21%) |
| Mean arterial pressure | 131.4 ± 25.3 (92; 176) |
| Sedated regimen | |
| No sedation | 5 (12%) |
| Fentanyl | 2 (4%) |
| Propofol/Fentanyl | 16 (39%) |
| Propofol/Midazolam/Fentanyl | 12 (29%) |
| Thiopental/Fentanyl | 6 (14%) |
| SAPS3 | 52.5 ± 13.1 |
| Admission GCS | 7.5 ± 5.3 |
| Mortality | 15 (36%) |
| ICP baseline | 13.83 ± 9.7 |
| ICP compression | 17.1 ± 8.2 |
| ICP >20 mmHg during monitoring | 15 (36%) |
| Baseline | IJVS Compression | ||
|---|---|---|---|
| ICP (mmHg) | Intact skull | 15.2 ± 7.1 | 19.3 ± 7.7 |
| Craniotomy/fractures | 15.6 ± 7.4 | 19.7 ± 7.4 | |
| Craniectomy | 20.8 ± 9.4 | 23.93 ± 8.8 | |
| Δ | % | ||
| P2/P1 ratio variation | ICP intact | +0.08 ± 0.5 | +8.43 |
| B4C intact | +0.11 ± 0.6 | +10.11 | |
| ICP craniotomy/fractures | +0.07 ± 0.3 | +5.60 | |
| B4C craniotomy/fractures | +0.05 ± 0.4 | +4.45 | |
| ICP craniectomy | −0.04 ± 0.2 | −3.42 | |
| B4C craniectomy | −0.01 ± 0.2 | −1.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brasil, S.; Solla, D.J.F.; Nogueira, R.d.C.; Teixeira, M.J.; Malbouisson, L.M.S.; Paiva, W.d.S. A Novel Noninvasive Technique for Intracranial Pressure Waveform Monitoring in Critical Care. J. Pers. Med. 2021, 11, 1302. https://doi.org/10.3390/jpm11121302
Brasil S, Solla DJF, Nogueira RdC, Teixeira MJ, Malbouisson LMS, Paiva WdS. A Novel Noninvasive Technique for Intracranial Pressure Waveform Monitoring in Critical Care. Journal of Personalized Medicine. 2021; 11(12):1302. https://doi.org/10.3390/jpm11121302
Chicago/Turabian StyleBrasil, Sérgio, Davi Jorge Fontoura Solla, Ricardo de Carvalho Nogueira, Manoel Jacobsen Teixeira, Luiz Marcelo Sá Malbouisson, and Wellingson da Silva Paiva. 2021. "A Novel Noninvasive Technique for Intracranial Pressure Waveform Monitoring in Critical Care" Journal of Personalized Medicine 11, no. 12: 1302. https://doi.org/10.3390/jpm11121302