Long Term Metabolic and Inflammatory Effects of Second-Generation Antipsychotics: A Study in Mentally Disordered Offenders

 ,
,
Abstract
:1. Introduction
1.1. Forensic Psychiatry
1.2. Antipsychotic Drugs and Metabolic Disturbances
2. Materials and Methods
2.1. Patients
2.2. Biochemical/ Hematological Assessment
2.3. Anthropometric Measurements
2.4. Blood Pressure Determination
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leistedt, S.; Bongaerts, X.; Macquet, D. Forensic psychiatry in Belgium in 2021: An overview of the current situation. Forensic Sci. Int. Mind Law 2021, 2, 100047. [Google Scholar] [CrossRef]
- Tataru, N.; Marinov, P.; Douzenis, A.; Novotni, A.; Kecman, B. Forensic psychiatry in some Balkan countries. Curr. Opin. Psychiatry 2010, 23, 472–480. [Google Scholar] [CrossRef]
- Zhang, J.-P.; Lencz, T.; Zhang, R.X.; Nitta, M.; Maayan, L.; John, M.; Robinson, D.G.; Fleischhacker, W.W.; Kahn, R.S.; Ophoff, R.A.; et al. Pharmacogenetic associations of antipsychotic drug-related weight gain: A systematic review and meta-analysis. Schizophr. Bull. 2016, 42, 1418–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musil, R.; Obermeier, M.; Russ, P.; Hamerle, M. Weight gain and antipsychotics: A drug safety review. Expert Opin. Drug Saf. 2014, 14, 73–96. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Lencz, T.; Malhotra, A.K. Antipsychotic drugs and obesity. Trends Mol. Med. 2011, 17, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvi, V.; Barone-Adesi, F.; D’Ambrosio, V.; Albert, U.; Maina, G. High H1-affinity antidepressants and risk of metabolic syndrome in bipolar disorder. Psychopharmacology 2015, 233, 49–56. [Google Scholar] [CrossRef] [PubMed]
- De Hert, M.; Detraux, J.; Van Winkel, R.; Yu, W.; Correll, C.U. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat. Rev. Endocrinol. 2011, 8, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Siafis, S.; Tzachanis, D.; Samara, M.; Papazisis, G. Antipsychotic drugs: From receptor-binding profiles to metabolic side effects. Curr. Neuropharmacol. 2018, 16, 1210–1223. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Mitchell, A.; De Hert, M.; Wampers, M.; Ward, P.; Rosenbaum, S.; Correll, C.U. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: A systematic review and meta-analysis. World Psychiatry 2015, 14, 339–347. [Google Scholar] [CrossRef]
- Brietzke, E.; Mansur, R.B.; Subramaniapillai, M.; Balanzá-Martínez, V.; Vinberg, M.; González-Pinto, A.; Rosenblat, J.D.; Ho, R.; McIntyre, R.S. Ketogenic diet as a metabolic therapy for mood disorders: Evidence and developments. Neurosci. Biobehav. Rev. 2018, 94, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Joffe, B.I.; Rosen, L.M.; Sullivan, T.B.; Joffe, R.T. Cardiovascular and cerebrovascular risk factors and events associated with second-generation antipsychotic compared to antidepressant use in a non-elderly adult sample: Results from a claims-based inception cohort study. World Psychiatry 2015, 14, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasnain, M.; Vieweg, W.V.R.; Hollett, B.; Victor, R.W. Weight gain and glucose dysregulation with second-generation antipsychotics and antidepressants: A review for primary care physicians. Postgrad. Med. 2012, 124, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Barton, B.B.; Segger, F.; Fischer, K.; Obermeier, M.; Musil, R. Update on weight-gain caused by antipsychotics: A systematic review and meta-analysis. Expert Opin. Drug Saf. 2020, 19, 295–314. [Google Scholar] [CrossRef] [PubMed]
- Bak, M.; Fransen, A.; Janssen, J.; van Os, J.; Drukker, M. Almost all antipsychotics result in weight gain: A meta-analysis. PLoS ONE 2014, 9, e94112. [Google Scholar] [CrossRef]
- Spertus, J.; Horvitz-Lennon, M.; Abing, H.; Normand, S.-L. Risk of weight gain for specific antipsychotic drugs: A meta-analysis. npj Schizophr. 2018, 4, 12. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, A.; Johnston, M.E. Weight-gain in psychiatric treatment: Risks, implications, and strategies for prevention and management. Mens Sana Monogr. 2010, 8, 53–68. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Chen, J.-D.; Zheng, X.-Y. Potential mechanisms of atypical antipsychotic-induced hypertriglyceridemia. Psychopharmacology 2013, 229, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Lee, J.I. Metabolic Disturbances independent of body mass in patients with schizophrenia taking atypical antipsychotics. Psychiatry Investig. 2015, 12, 242–248. [Google Scholar] [CrossRef]
- Kahn, R.S.; Fleischhacker, W.W.; Boter, H.; Davidson, M.; Vergouwe, Y.; Keet, I.P.; Gheorghe, M.D.; Rybakowski, J.K.; Galderisi, S.; Libiger, J.; et al. Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: An open randomised clinical trial. Lancet 2008, 371, 1085–1097. [Google Scholar] [CrossRef] [Green Version]
- Lieberman, J.A.; Stroup, T.; McEvoy, J.P.; Swartz, M.S.; Rosenheck, R.A.; Perkins, D.O.; Keefe, R.S.; Davis, S.M.; Davis, C.E.; Lebowitz, B.; et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N. Engl. J. Med. 2005, 353, 1209–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, T.; Lieberman, J.; McEvoy, J.; Swartz, M.; Davis, S.; Rosenheck, R.; Perkins, D.; Keefe, R.; Severe, J.; Hsiao, J.; et al. Effectiveness of olanzapine, quetiapine, risperidone, and ziprasidone in patients with chronic schizophrenia following discontinuation of a previous atypical antipsychotic. Am. J. Psychiatry 2006, 163, 611. [Google Scholar] [CrossRef]
- Rummel-Kluge, C.; Komossa, K.; Schwarz, S.; Hunger, H.; Schmid, F.; Lobos, C.A.; Kissling, W.; Davis, J.M.; Leucht, S. Head-to-head comparisons of metabolic side effects of second generation antipsychotics in the treatment of schizophrenia: A systematic review and meta-analysis. Schizophr. Res. 2010, 123, 225–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correll, C.U.; Robinson, D.G.; Schooler, N.R.; Brunette, M.F.; Mueser, K.T.; Rosenheck, R.A.; Marcy, P.; Addington, J.; Estroff, S.E.; Robinson, J.; et al. Cardiometabolic risk in patients with first-episode schizophrenia spectrum disorders. JAMA Psychiatry 2014, 71, 1350–1363. [Google Scholar] [CrossRef]
- Komossa, K.; Rummel-Kluge, C.; Hunger, H.; Schwarz, S.; Bhoopathi, P.S.; Kissling, W.; Leucht, S. Ziprasidone versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst. Rev. 2009, 7, CD006627. [Google Scholar] [CrossRef] [Green Version]
- Vázquez-Bourgon, J.; Pérez-Iglesias, R.; de la Foz, V.O.G.; Pinilla, P.S.; Martínez, D.; Crespo-Facorro, B. Long-term metabolic effects of aripiprazole, ziprasidone and quetiapine: A pragmatic clinical trial in drug-naïve patients with a first-episode of non-affective psychosis. Psychopharmacology 2017, 235, 245–255. [Google Scholar] [CrossRef]
- Farrer, S. Beyond statins: Emerging evidence for HDL-Increasing Therapies and diet in treating cardiovascular disease. Adv. Prev. Med. 2018, 2018, 6024747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, B.; Steiner, J.; Bernstein, H.-G.; Dodd, S.; Pasco, J.A.; Dean, O.; Nardin, P.; Gonçalves, C.; Berk, M. C-reactive protein is increased in schizophrenia but is not altered by antipsychotics: Meta-analysis and implications. Mol. Psychiatry 2015, 21, 554–564. [Google Scholar] [CrossRef]
- Abdel-Wahab, B.A.; Metwally, M.E. Clozapine-induced cardiotoxicity: Role of oxidative stress, tumour necrosis factor alpha and NF-κβ. Cardiovasc. Toxicol. 2014, 15, 355–365. [Google Scholar] [CrossRef]
- Howell, S.; Yarovova, E.; Khwanda, A.; Rosen, S.D. Cardiovascular effects of psychotic illnesses and antipsychotic therapy. Heart 2019, 105, 1852–1859. [Google Scholar] [CrossRef] [PubMed]
- Nikolić-Kokić, A.; Tatalović, N.; Nestorov, J.; Mijović, M.; Mijusković, A.; Miler, M.; Dusic, Z.O.; Nikolić, M.; Milošević, V.; Blagojević, D.; et al. Clozapine, ziprasidone, and sertindole-induced morphological changes in the rat heart and their relationship to antioxidant enzymes function. J. Toxicol. Environ. Health Part A 2018, 81, 844–853. [Google Scholar] [CrossRef]
- Pillinger, T.; Osimo, E.F.; de Marvao, A.; Berry, M.A.; Whitehurst, T.; Statton, B.; Quinlan, M.; Brugger, S.; Vazir, A.; Cook, S.A.; et al. Cardiac structure and function in patients with schizophrenia taking antipsychotic drugs: An MRI study. Transl. Psychiatry 2019, 9, 163. [Google Scholar] [CrossRef] [Green Version]
- Correll, C.U. Cardiometabolic risk of second-generation antipsychotic medications during first-time use in children and adolescents. JAMA 2009, 302, 1765–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scigliano, G.; Ronchetti, G. Antipsychotic-induced metabolic and cardiovascular side effects in schizophrenia: A novel mechanistic hypothesis. CNS Drugs 2013, 27, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atmaca, M.; Kuloglu, M.; Tezcan, E.; Ustundag, B. Serum leptin and triglyceride levels in patients on treatment with atypical antipsychotics. J. Clin. Psychiatry 2003, 64, 598–604. [Google Scholar] [CrossRef]
- Melkersson, K.I.; Hulting, A.-L.; Brismar, K.E. Elevated levels of insulin, leptin, and blood lipids in olanzapine-treated patients with schizophrenia or related psychoses. J. Clin. Psychiatry 2000, 61, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, Y.; Kajiyama, K.; Ishiguro, C.; Uyama, Y. Atypical antipsychotics and the risk of hyperlipidemia: A sequence symmetry analysis. Drug Saf. 2015, 38, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Nasrallah, H.A. Atypical antipsychotic-induced metabolic side effects: Insights from receptor-binding profiles. Mol. Psychiatry 2007, 13, 27–35. [Google Scholar] [CrossRef]
- Henderson, D.C.; Cagliero, E.; Copeland, P.M.; Borba, C.P.; Evins, A.E.; Hayden, D.; Weber, M.T.; Anderson, E.J.; Allison, D.B.; Daley, T.B.; et al. Glucose metabolism in patients with schizophrenia treated with atypical antipsychotic agents. Arch. Gen. Psychiatry 2005, 62, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firth, J.; Veronese, N.; Cotter, J.; Shivappa, N.; Hebert, J.R.; Ee, C.; Smith, L.; Stubbs, B.; Jackson, S.E.; Sarris, J. What is the role of dietary inflammation in severe mental illness? A review of observational and experimental findings. Front. Psychiatry 2019, 10, 350. [Google Scholar] [CrossRef] [PubMed]
- Whicher, C.A.; Price, H.C.; Holt, R.I.G. Mechanisms in endocrinology: Antipsychotic medication and type 2 diabetes and impaired glucose regulation. Eur. J. Endocrinol. 2018, 178, R245–R258. [Google Scholar] [CrossRef] [Green Version]
- Tenback, D.E.; Van Kessel, F.; Jessurun, J.; Pijl, Y.J.; Heerdink, E.R.; Van Harten, P.N. Risk factors for inactivity in patients in long-term care with severe mental illness. Tijdschr. Psychiatr. 2013, 55, 83–91. [Google Scholar]
- Schulte, P.F.; Bocxe, J.T.; Doodeman, H.J.; Van Haelst, I.M.; Cohen, D. Risk of new-onset diabetes after long-term treatment with clozapine in comparison to other antipsychotics in patients with schizophrenia. J. Clin. Psychopharmacol. 2016, 36, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Saedisomeolia, A.; Djalali, M.; Moghadam, A.M.; Ramezankhani, A.; Najmi, L. Folate and vitamin B12 status in schizophrenic patients. J. Res. Med. Sci. 2011, 16, S437–S441. [Google Scholar]
- Al-Daghri, N.M.; Rahman, S.; Sabico, S.; Yakout, S.; Wani, K.; Al-Attas, O.S.; Saravanan, P.; Tripathi, G.; McTernan, P.G.; Alokail, M.S. Association of Vitamin B12 with Pro-inflammatory cytokines and biochemical markers related to cardiometabolic risk in saudi subjects. Nutrients 2016, 8, 460. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Ν | % | ||
|---|---|---|---|
| Gender | Females | 4 | 11.4% |
| Males | 31 | 88.6% | |
| Antipsychotic medication | AP1 | 17 | 48.6% |
| AP2 | 18 | 51.4% | |
| Diagnosis | Schizophrenia | 24 | 68.6% |
| Other non-organic psychosis | 7 | 20% | |
| Chronic delusional disorders | 1 | 2.95 | |
| Mixed and other personality disorders | 1 | 2.9% | |
| Mental disorders and behavioral disorders | 2 | 5.7% | |
| Other medication | Anticoagulants (1st year) | 2 | 5.7% |
| Anticoagulants (2ndyear) | 5 | 14.3% | |
| Anticoagulants (3rd year) | 5 | 14.3% | |
| Antihypertensives (1st year) | 4 | 11.4% | |
| Antihypertensives (2ndyear) | 7 | 20% | |
| Antihypertensives (3rdyear) | 8 | 22.9% | |
| Antidiabetic (1st year) | 4 | 11.4% | |
| Antidiabetic (2nd year) | 5 | 14.3% | |
| Antidiabetic (3rd year) | 4 | 11.4% | |
| Antilipidemics (1st year) | 5 | 14.3% | |
| Antilipidemics(2nd year) | 7 | 20% | |
| Antilipidemics (3rd year) | 9 | 25.7% | |
| Medication for CVD (1st year) | 10 | 28.6% | |
| Medication for CVD (2ndyear) | 10 | 28.6% | |
| Medication for CVD (3rd year) | 11 | 31.4% |
| (A) | |||||||||
| Variables | Total T1 | Total T2 | p-Value | AP1 T1 | AP1 T2 | p-Value | AP2 T1 | AP2 T2 | p-Value |
| Weight (kg) | 85.26 (15.59) 1 | 86.37 (16.40) 1 | 0.38 2 | 86.47 (18.54) 1 | 88.82 (18.74) 1 | 0.17 2 | 84.11 (12.64) 1 | 84.06 (14.00) 1 | 0.98 2 |
| BMI (kg/m2) | 29.09 (6.05) 1 | 29.42 (5.88) 1 | 0.26 | 30.10 (7.09) 1 | 30.84 (6.59) 1 | 0.21 2 | 28.14 (4.88) 1 | 28.07 (4.95) 1 | 0.61 |
| Glucose (mg/dL) | 94.00 (13.00) | 94.00 (24.00) | 0.19 | 94.00 (12.00) | 94.00 (26.00) | 0.08 | 97.17 (11.32) | 94.50 (27.00) | 0.65 |
| Cholesterol (mg/dL) | 174.71 (36.18) 1 | 171.11 (38.81) 1 | 0.69 | 166.00 (31.77) 1 | 164.65 (43.55) 1 | 0.30 | 182.94 (38.99) 1 | 177.22 (33.86) 1 | 0.65 |
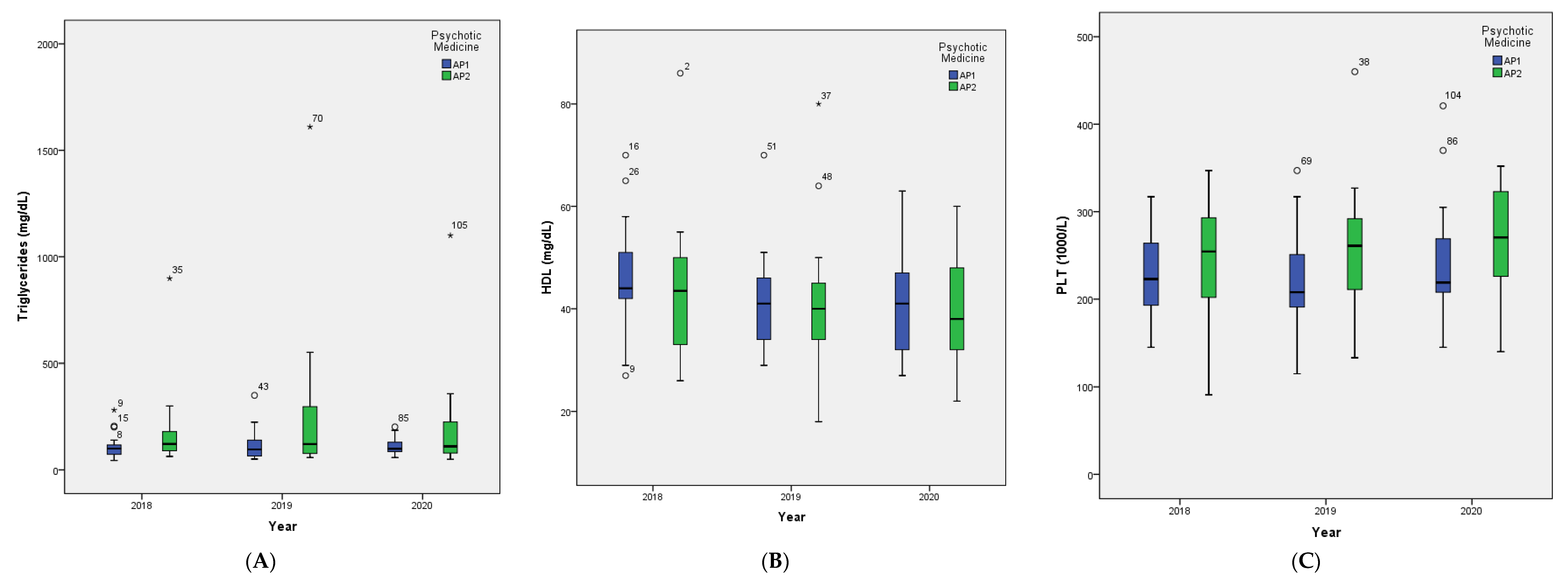
| Triglyce-rides (mg/dL) | 109.00 (69.00) | 108.00 (126.00) | 0.12 | 100.00 (58.00) | 119.82 (76.89) 1 | 0.69 2 | 122.00 (110.00) | 121.50 (228.00) | 0.07 |
| HDL (mg/dL) | 45.03 (12.48) 1 | 41.77 (12.01) 1 | 0.00 | 46.47 (11.17) | 42.06 (9.83) | 0.01 | 43.67 (13.78) | 41.50 (14.06) | 0.107 2 |
| LDL (mm Hg) | 97.23 (32.24) 1 | 98.91 (31.76) 1 | 0.46 | 94.06 (28.17) 1 | 99.12 (37.69) 1 | 0.98 | 100.22 (36.22) 1 | 98.72 (26.07) 1 | 0.28 |
| Systolic BP (mm Hg) | 121.23 (12.93) 1 | 123.94 (14.85) 1 | 0.13 2 | 120.71 (15.34) 1 | 125.12 (17.00) 1 | 0.17 2 | 121.72 (10.59) 1 | 122.83 (12.89) 1 | 0.52 2 |
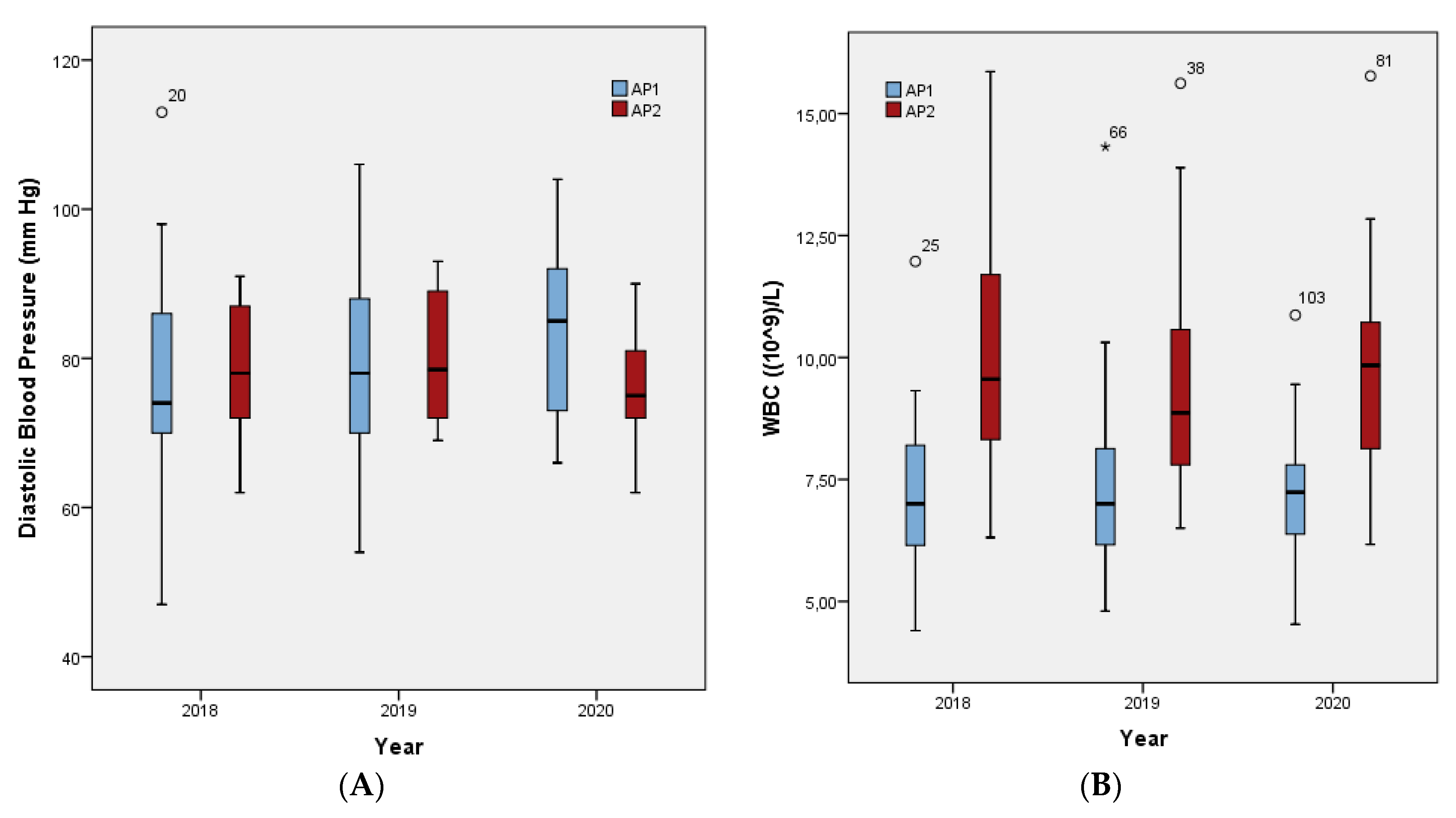
| Diastolic BP (mm Hg) | 78.26 (11.91) 1 | 79.63 (11.67) 1 | 0.39 | 78.00 (15.17) 1 | 80.06 (14.76) 1 | 0.46 2 | 78.50 (8.18) 1 | 79.22 (8.17) 1 | 0.81 |
| WBC (103/L) | 8.75 (2.57) 1 | 8.65 (2.58) 1 | 0.91 | 7.35 (1.91) 1 | 7.62 (2.29) 1 | 0.33 | 9.56 (3.47) | 9.62 (2.51) 1 | 0.41 |
| PLT (103/L) | 240.51 (61.17) 1 | 239.77 (69.37) 1 | 0.94 2 | 227.82 (54.31) 1 | 222.35 (60.97) 1 | 0.55 2 | 252.50 (66.30) 1 | 256.22 (74.41) 1 | 0.82 2 |
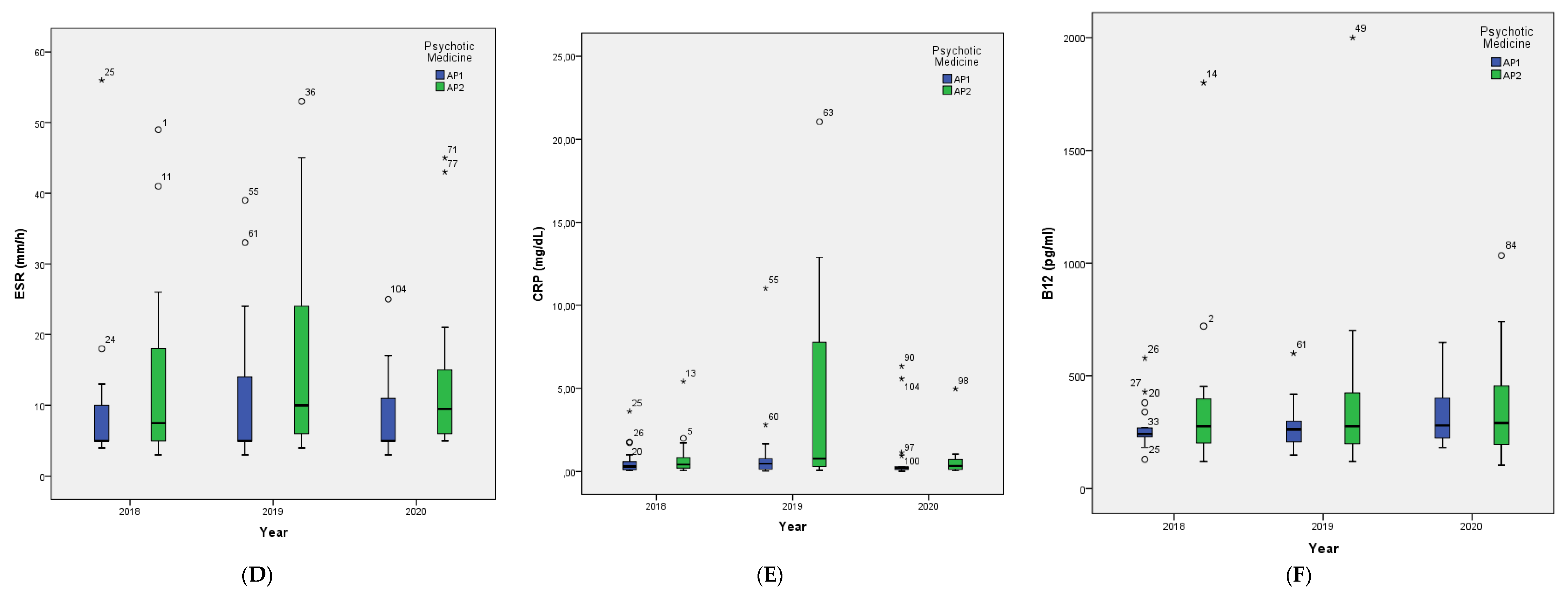
| ESR (mm/h) | 5.00 (7.00) | 7.00 (16.00) | 0.11 | 5.00 (5.50) | 5.00 (11.00) | 0.68 | 7.50 (13.50) | 10.00 (21.80) | 0.06 |
| CRP (mg/dL) | 0.40 (0.70) | 0.51 (2.64) | 0.01 | 0.30 (0.70) | 0.48 (0.76) | 0.33 | 0.43 (0.67) | 0.78 (7.56) | 0.01 |
| B12 (pg/mL) | 250.00 (167.00) | 270.00 (181.00) | 0.13 | 243.00 (95.00) | 278.82 (111.03) 1 | 0.32 2 | 276.00 (206.00) | 276.00 (229.00) | 0.25 |
| Folicacid (ng/mL) | 4.00 (3.10) | 3.90 (2.80) | 0.79 | 4.40 (3.20) | 4.00 (4.70) | 0.87 | 3.95 (1.80) | 3.70 (2.10) | 0.47 |
| (B) | |||||||||
| Variables | Total T2 | Total T3 | p-Value | AP1 T2 | AP1 T3 | p-Value | AP2 T2 | AP2 T3 | p-Value |
| Weight (kg) | 86.37 (16.40) 1 | 85.34 (16.41) 1 | 0.19 | 88.82 (18.74) 1 | 86.53 (19.34) 1 | 0.10 | 84.06 (14.00) 1 | 84.22 (13.57) 1 | 0.93 2 |
| BMI (kg/m2) | 29.42 (5.88) 1 | 29.04 (5.75) 1 | 0.20 | 30.84 (6.59) 1 | 30.01 (6.79) 1 | 0.12 | 28.07 (4.95) 1 | 28.11 (4.56) 1 | 0.95 2 |
| Glucose (mg/dL) | 94.00 (24.00) | 95.00 (16.00) | 0.30 | 94.00 (26.00) | 95.00 (15.00) | 0.33 | 94.50 (27.00) | 94.50 (22.00) | 0.47 |
| Cholesterol (mg/dL) | 171.11 (38.81) 1 | 164.34 (35.30) 1 | 0.75 | 164.65 (43.55) 1 | 159.18 (29.52) 1 | 0.86 | 177.22 (33.86) 1 | 160.50 (60.00) | 0.57 |
| Triglyce-rides (mg/dL) | 108.00 (126.00) | 153.46 (105.00) | 0.17 | 119.82 (76.89) 1 | 108.00 (40.95) 1 | 0.55 | 121.50 (228.00) | 110.50 (151.00) | 0.01 |
| HDL (mg/dL) | 41.77 (12.01) 1 | 39.71 (10.48) 1 | 0.084 2 | 42.06 (9.83) | 40.24 (9.69) | 0.03 | 41.50 (14.06) | 39.22 (11.43) | 0.21 2 |
| LDL (mm Hg) | 98.91 (31.76) 1 | 95.29 (30.57) 1 | 0.90 | 99.12 (37.69) 1 | 96.12 (22.07) 1 | 0.51 | 98.72 (26.07) 1 | 86.50 (59.00) | 0.51 |
| Systolic BP (mm Hg) | 123.94 (14.85) 1 | 126.86 (21.12) 1 | 0.44 | 125.12 (17.00) 1 | 128.00 (23.00) | 0.64 | 122.83 (12.89) 1 | 119.50 (25.00) | 0.70 2 |
| Diastolic BP (mm Hg) | 79.63 (11.67) 1 | 79.00 (16.00) | 0.44 | 80.06 (14.76) 1 | 83.82 (11.32) 1 | 0.66 | 79.22 (8.17) 1 | 76.72 (7.40) 1 | 0.09 2 |
| WBC (103/L) | 8.65 (2.58) 1 | 8.57 (2.40) 1 | 0.86 2 | 7.62 (2.29) 1 | 7.16 (1.60) 1 | 0.87 | 9.62 (2.51) 1 | 9.91 (2.29) 1 | 0.63 |
| PLT (103/L) | 239.77 (69.37) 1 | 251.66 (68.74) 1 | 0.01 | 222.35 (60.97) 1 | 238.88 (74.27) 1 | 0.07 2 | 256.22 (74.41) 1 | 263.72 (62.78) 1 | 0.07 |
| ESR (mm/h) | 7.00 (16.00) | 8.00 (8.00) | 0.05 | 5.00 (11.00) | 5.00 (6.00) | 0.20 | 10.00 (21.80) | 9.50 (10.50) | 0.13 |
| CRP (mg/dL) | 0.51 (2.64) | 0.25 (0.60) | <0.01 | 0.48 (0.76) | 0.21 (0.51) | 0.34 | 0.78 (7.56) | 0.34 (0.61) | <0.01 |
| B12 (pg/mL) | 270.00 (181.00) | 290.00 (225.00) | 0.10 | 278.82 (111.03) 1 | 331.82 (144.31) 1 | 0.04 | 276.00 (229.00) | 359.39 (232.18) 1 | 0.73 |
| Folicacid (ng/mL) | 3.90 (2.80) | 4.10 (9.10) | 0.16 | 4.00 (4.70) | 3.80 (13.20) | 0.30 | 3.70 (2.10) | 4.20 (5.40) | 0.44 |
| (C) | |||||||||
| Variables | Total T1 | Total T3 | p-Value | AP1 T1 | AP1 T3 | p-Value | AP2 T1 | AP2 T3 | p-Value |
| Weight (kg) | 85.26 (15.59) 1 | 85.34 (16.41) 1 | 0.84 | 86.47 (18.54) 1 | 86.53 (19.34) 1 | 0.98 2 | 84.11 (12.64) 1 | 84.22 (13.57) 1 | 0.95 2 |
| BMI (kg/m2) | 29.09 (6.05) 1 | 29.04 (5.75) 1 | 0.82 | 30.10 (7.09) 1 | 30.01 (6.79) 1 | 0.93 2 | 28.14 (4.88) 1 | 28.11 (4.56) 1 | 0.96 2 |
| Glucose (mg/dL) | 94.00 (13.00) | 95.00 (16.00) | 0.31 | 94.00 (12.00) | 95.00 (15.00) | 0.31 | 97.17 (11.32) | 94.50 (22.00) | 0.67 |
| Cholesterol (mg/dL) | 174.71 (36.18) 1 | 164.34 (35.30) 1 | 0.16 2 | 166.00 (31.77) 1 | 159.18 (29.52) 1 | 0.31 | 182.94 (38.99) 1 | 160.50 (60.00) | 0.31 |
| Triglyce-rides (mg/dL) | 109.00 (69.00) | 153.46 (105.00) | 0.59 | 100.00 (58.00) | 108.00 (40.95) 1 | 1.00 | 122.00 (110.00) | 110.50 (151.00) | 0.57 |
| HDL (mg/dL) | 45.03 (12.48) 1 | 39.71 (10.48) 1 | <0.01 2 | 46.47 (11.17) | 40.24 (9.69) | <0.01 2 | 43.67 (13.78) | 39.22 (11.43) | 0.08 2 |
| LDL (mm Hg) | 97.23 (32.24) 1 | 95.29 (30.57) 1 | 0.73 2 | 94.06 (28.17) 1 | 96.12 (22.07) 1 | 0.73 2 | 100.22 (36.22) 1 | 86.50 (59.00) | 0.56 2 |
| Systolic BP (mm Hg) | 121.23 (12.93) 1 | 126.86 (21.12) 1 | 0.08 | 120.71 (15.34) 1 | 128.00 (23.00) | 0.09 | 121.72 (10.59) 1 | 119.50 (25.00) | 0.33 2 |
| Diastolic BP (mm Hg) | 78.26 (11.91) 1 | 79.00 (16.00) | 0.40 | 78.00 (15.17) 1 | 83.82 (11.32) 1 | 0.10 2 | 78.50 (8.18) 1 | 76.72 (7.40) 1 | 0.13 2 |
| WBC (103/L) | 8.75 (2.57) 1 | 8.57 (2.40) 1 | 0.66 2 | 7.35 (1.91) 1 | 7.16 (1.60) 1 | 0.72 2 | 9.56 (3.47) | 9.91 (2.29) 1 | 0.80 2 |
| PLT (103/L) | 240.51 (61.17) 1 | 251.66 (68.74) 1 | 0.11 2 | 227.82 (54.31) 1 | 238.88 (74.27) 1 | 0.29 2 | 252.50 (66.30) 1 | 263.72 (62.78) 1 | 0.25 2 |
| ESR (mm/h) | 5.00 (7.00) | 8.00 (8.00) | 0.45 | 5.00 (5.50) | 5.00 (6.00) | 0.61 | 7.50 (13.50) | 9.50 (10.50) | 0.15 |
| CRP (mg/dL) | 0.40 (0.70) | 0.25 (0.60) | 0.46 | 0.30 (0.70) | 0.21 (0.51) | 0.96 | 0.43 (0.67) | 0.34 (0.61) | 0.31 |
| B12 (pg/mL) | 250.00 (167.00) | 290.00 (225.00) | 0.05 2 | 243.00 (95.00) | 331.82 (144.31) 1 | 0.04 | 276.00 (206.00) | 359.39 (232.18) 1 | 0.57 |
| Folicacid (ng/mL) | 4.00 (3.10) | 4.10 (9.10) | 0.11 | 4.40 (3.20) | 3.80 (13.20) | 0.09 | 3.95 (1.80) | 4.20 (5.40) | 0.51 |
| Variable | T1 | T2 | T3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| AP1 | AP2 | p-Value | AP1 | AP2 | p-Value | AP1 | AP2 | p-Value | |
| Weight (kg) | 86.47 (18.54) 1 | 84.11 (12.64) 1 | 0.66 2 | 88.82 (18.74) 1 | 84.06 (14.00) 1 | 0.39 2 | 86.53 (19.34) 1 | 84.22 (13.57) 1 | 0.68 2 |
| BMI (kg/m2) | 30.10 (7.09) 1 | 28.14 (4.88) 1 | 0.34 2 | 30.84 (6.59) 1 | 28.07 (4.95) 1 | 0.16 2 | 30.01 (6.79) 1 | 28.11 (4.56) 1 | 0.33 2 |
| Glucose (mg/dL) | 94.00 (12.00) | 97.17 (11.32) | 0.80 | 94.00 (26.00) | 94.50 (27.00) | 0.98 | 95.00 (15.00) | 94.50 (22.00) | 0.76 |
| Cholesterol (mg/dL) | 166.00 (31.77) 1 | 182.94 (38.99) 1 | 0.17 2 | 164.65 (43.55) 1 | 177.22 (33.86) 1 | 0.34 2 | 159.18 (29.52) 1 | 160.50 (60.00) | 0.96 |
| Triglycerides (mg/dL) | 100.00 (58.00) | 122.00 (110.00) | 0.11 | 119.82 (76.89) 1 | 121.50 (228.00) | 0.11 | 108.00 (40.95) 1 | 110.50 (151.00) | 0.32 |
| HDL (mg/dL) | 46.47 (11.17) | 43.67 (13.78) | 0.51 2 | 42.06 (9.83) | 41.50 (14.06) | 0.89 2 | 40.24 (9.69) | 39.22 (11.43) | 0.78 2 |
| LDL (mm Hg) | 94.06 (28.17) 1 | 100.22 (36.22) 1 | 0.58 | 99.12 (37.69) 1 | 98.72 (26.07) 1 | 0.97 | 96.12 (22.07) 1 | 86.50 (59.00) | 0.64 |
| Systolic BP (mm Hg) | 120.71 (15.34) 1 | 121.72 (10.59) 1 | 0.82 2 | 125.12 (17.00) 1 | 122.83 (12.89) 1 | 0.65 2 | 128.00 (23.00) | 119.50 (25.00) | 0.64 |
| Diastolic BP (mm Hg) | 78.00 (15.17) 1 | 78.50 (8.18) 1 | 0.90 2 | 80.06 (14.76) 1 | 79.22 (8.17) 1 | 0.84 2 | 83.82 (11.32) 1 | 76.72 (7.40) 1 | 0.03 2 |
| WBC 103/L) | 7.35 (1.91) 1 | 9.56 (3.47) | <0.01 | 7.62 (2.29) 1 | 9.62 (2.51) 1 | 0.01 2 | 7.16 (1.60) 1 | 9.91 (2.29) 1 | <0.01 2 |
| PLT (103/L) | 227.82 (54.31) 1 | 252.50 (66.30) 1 | 0.24 2 | 222.35 (60.97) 1 | 256.22 (74.41) 1 | 0.15 2 | 238.88 (74.27) 1 | 263.72 (62.78) 1 | 0.29 2 |
| ESR (mm/h) | 5.00 (5.50) | 7.50 (13.50) | 0.40 | 5.00 (11.00) | 10.00 (21.80) | 0.08 | 5.00 (6.00) | 9.50 (10.50) | 0.06 |
| CRP (mg/dL) | 0.30 (0.70) | 0.43 (0.67) | 0.25 | 0.48 (0.76) | 0.78 (7.56) | 0.11 | 0.21 (0.51) | 0.34 (0.61) | 0.35 |
| B12 (pg/mL) | 243.00 (95.00) | 276.00 (206.00) | 0.33 | 278.82 (111.03) 1 | 276.00 (229.00) | 0.48 | 331.82 (144.31) 1 | 359.39 (232.18) 1 | 0.67 |
| Folic Acid (ng/mL) | 4.40 (3.20) | 3.95 (1.80) | 0.71 | 4.00 (4.70) | 3.70 (2.10) | 0.57 | 3.80 (13.20) | 4.20 (5.40) | 0.81 |
| Variables | T1 | T2 | T3 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | AP1 | AP2 | p-Value | Total | AP1 | AP2 | p-Value | Total | AP1 | AP2 | p-Value | |
| WC (cm)2 | N/A | N/A | N/A | - | N/A | N/A | N/A | - | 12 (34.3%) | 7 (41.2%) | 5 (27.8%) | 0.40 1 |
| Triglycerides (mg/dL) | 8 (22.9%) | 3 (17.6%) | 5 (27.8%) | 0.69 | 12 (34.3%) | 4 (23.5%) | 8 (44.4%) | 0.19 1 | 9 (25.7%) | 2 (11.8%) | 7 (38.9%) | 0.12 |
| HDL (mg/dL) | 10 (28.6%) | 3 (17.6%) | 7 (38.9%) | 0.26 | 18 (51.4%) | 8 (47.1%) | 10 (55.6%) | 0.61 1 | 19 (54.3%) | 8 (47.1%) | 11 (61.1%) | 0.40 1 |
| Systolic BP (mm Hg) | 8 (22.9%) | 5 (29.4%) | 3 (8.6%) | 0.44 | 13 (37.1%) | 8 (47.1%) | 5 (27.8%) | 0.24 1 | 15 (42.9%) | 8 (47.1%) | 7 (38.9%) | 0.62 1 |
| Diastolic BP (mm Hg) | 10 (28.6%) | 5 (29.4%) | 5 (27.8%) | 1.00 | 11 (31.4%) | 6 (35.3%) | 5 (27.8%) | 0.63 1 | 12 (34.3%) | 9 (52.9%) | 3 (16.7%) | 0.02 1 |
| Glucose (mg/dL) | 6 (17.1%) | 3 (17.6%) | 3 (16.7%) | 1.00 | 9 (25.7%) | 5 (29.4%) | 4 (22.2%) | 0.71 | 7 (20%) | 3 (17.6%) | 4 (22.2%) | 1.00 |
| Metabolic Syndrome | 10 (28.6%) | 5 (29.4%) | 5 (27.8%) | 1.00 | 12 (34.3%) | 6 (35.3%) | 6 (33.3%) | 0.90 1 | 9 (25.7%) | 5 (29.4%) | 4 (22.2%) | 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassilopoulou, E.; Efthymiou, D.; Papatriantafyllou, E.; Markopoulou, M.; Sakellariou, E.-M.; Popescu, A.C. Long Term Metabolic and Inflammatory Effects of Second-Generation Antipsychotics: A Study in Mentally Disordered Offenders. J. Pers. Med. 2021, 11, 1189. https://doi.org/10.3390/jpm11111189
Vassilopoulou E, Efthymiou D, Papatriantafyllou E, Markopoulou M, Sakellariou E-M, Popescu AC. Long Term Metabolic and Inflammatory Effects of Second-Generation Antipsychotics: A Study in Mentally Disordered Offenders. Journal of Personalized Medicine. 2021; 11(11):1189. https://doi.org/10.3390/jpm11111189
Chicago/Turabian StyleVassilopoulou, Emilia, Dimitris Efthymiou, Evangelia Papatriantafyllou, Maria Markopoulou, Efthymia-Maria Sakellariou, and Alina Codruta Popescu. 2021. "Long Term Metabolic and Inflammatory Effects of Second-Generation Antipsychotics: A Study in Mentally Disordered Offenders" Journal of Personalized Medicine 11, no. 11: 1189. https://doi.org/10.3390/jpm11111189