
Investigating the Role of Leukocyte Telomere Length in Treatment-Resistant Depression and in Response to Electroconvulsive Therapy

 , , and
, , and 
Abstract
:
1. Introduction
2. Results
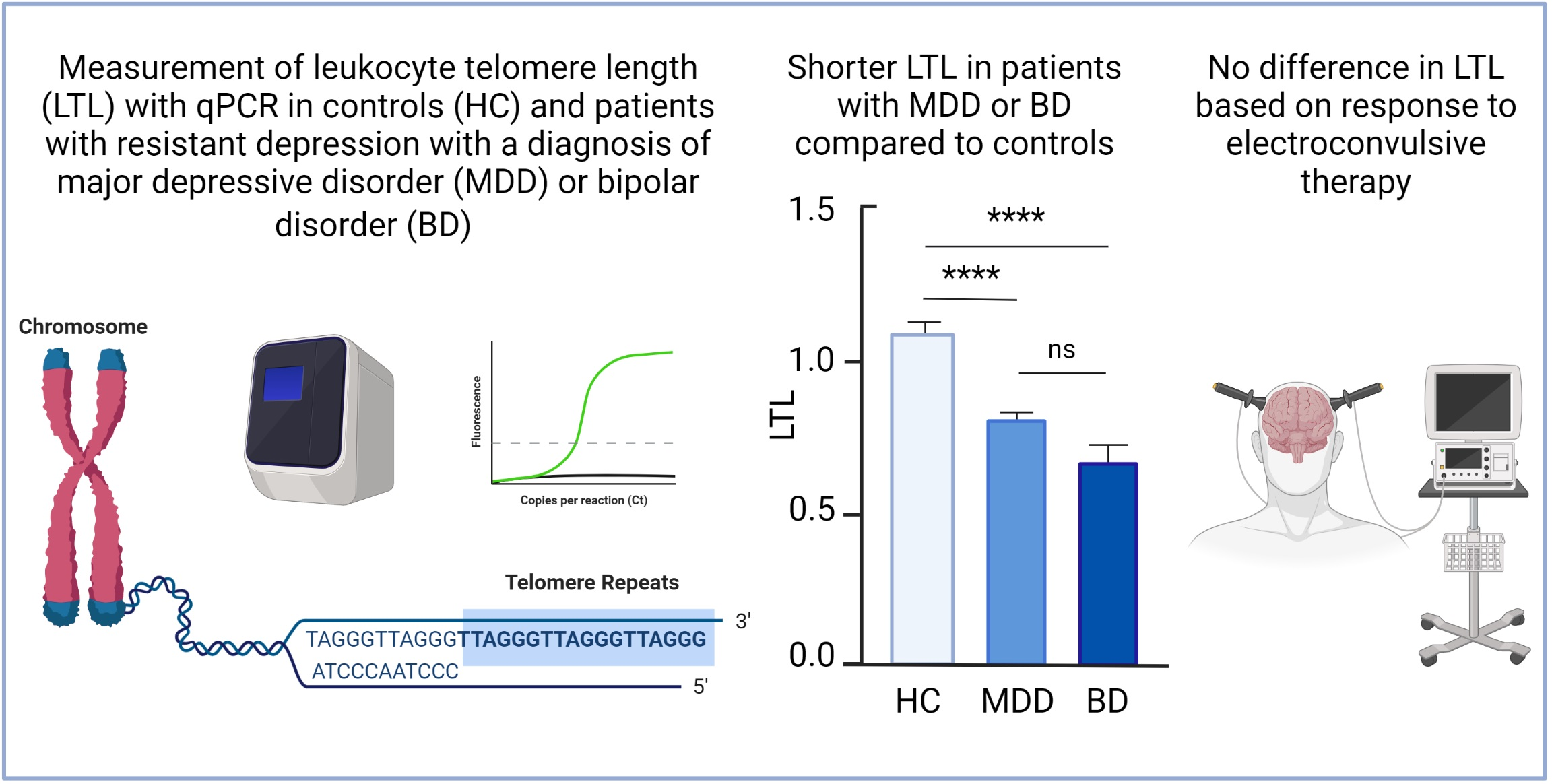
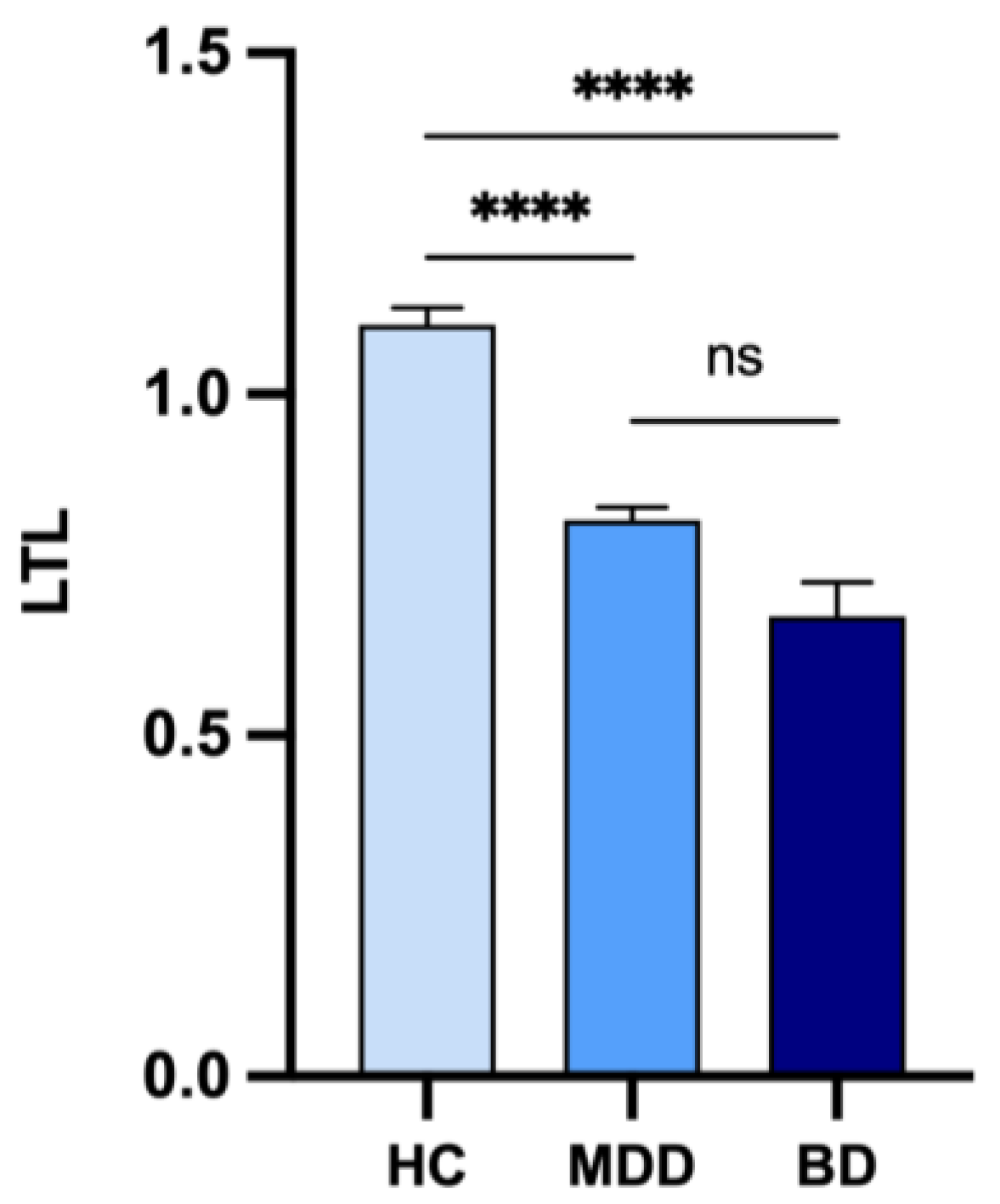
2.1. Comparison of LTL between Patients with Treatment-Resistant Depression and Controls
2.2. Association between Baseline LTL and Response to ECT
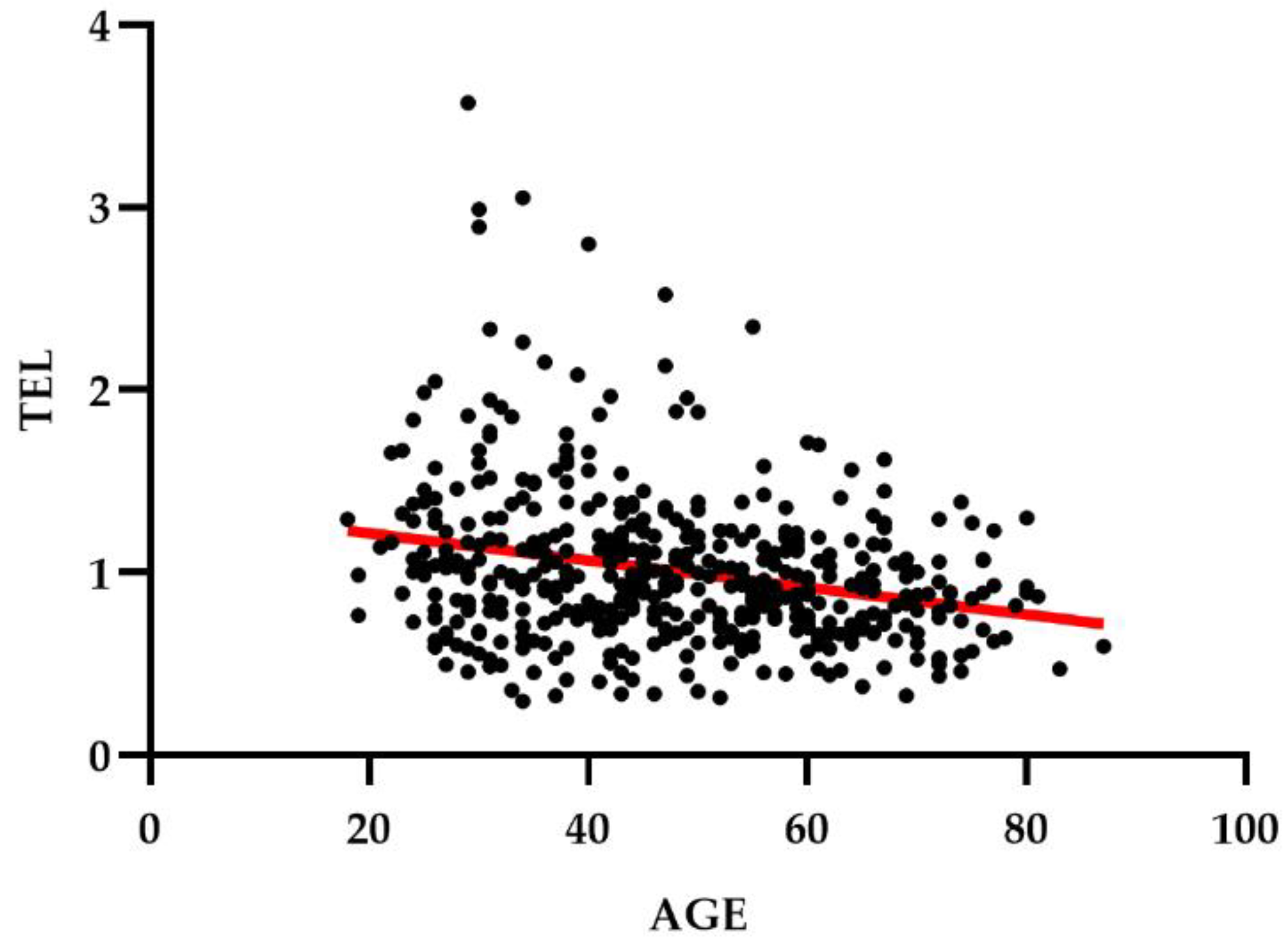
2.3. Association between LTL and other Demographic or Clinical Variables
2.4. Association between Genetic Variants, Response to ECT and LTL
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. DNA Extraction
4.3. Measurements of Leukocyte Telomere Length with Quantitative PCR
4.4. Statistical Analysis
4.5. Analysis of GWAS Data
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akvardar, Y.; Akdede, B.B.; Ozerdem, A.; Eser, E.; Topkaya, S.; Alptekin, K. Assessment of quality of life with the WHOQOL-BREF in a group of Turkish psychiatric patients compared with diabetic and healthy subjects. Psychiatry Clin. Neurosci. 2006, 60, 693–699. [Google Scholar] [CrossRef]
- Hayes, J.F.; Miles, J.; Walters, K.; King, M.; Osborn, D.P. A systematic review and meta-analysis of premature mortality in bipolar affective disorder. Acta Psychiatr. Scand. 2015, 131, 417–425. [Google Scholar] [CrossRef]
- Skevington, S.M.; McCrate, F.M. Expecting a good quality of life in health: Assessing people with diverse diseases and conditions using the WHOQOL-BREF. Health Expect. 2012, 15, 49–62. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Bromet, E.J. The epidemiology of depression across cultures. Annu. Rev. Public Health 2013, 34, 119–138. [Google Scholar] [CrossRef] [Green Version]
- Merikangas, K.R.; Jin, R.; He, J.P.; Kessler, R.C.; Lee, S.; Sampson, N.A.; Viana, M.C.; Andrade, L.H.; Hu, C.; Karam, E.G.; et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch. Gen. Psychiatry 2011, 68, 241–251. [Google Scholar] [CrossRef] [PubMed]
- De Hert, M.; Dekker, J.M.; Wood, D.; Kahl, K.G.; Holt, R.I.; Moller, H.J. Cardiovascular disease and diabetes in people with severe mental illness position statement from the European Psychiatric Association (EPA), supported by the European Association for the Study of Diabetes (EASD) and the European Society of Cardiology (ESC). Eur. Psychiatry 2009, 24, 412–424. [Google Scholar] [CrossRef] [Green Version]
- WHO Report. Available online: http://www.euro.who.int/__data/assets/pdf_file/0009/342297/Comorbidity-report_E-web.pdf (accessed on 25 April 2021).
- Gonda, X.; Pompili, M.; Serafini, G.; Montebovi, F.; Campi, S.; Dome, P.; Duleba, T.; Girardi, P.; Rihmer, Z. Suicidal behavior in bipolar disorder: Epidemiology, characteristics and major risk factors. J. Affect. Disord. 2012, 143, 16–26. [Google Scholar] [CrossRef]
- Large, M. Study on suicide risk assessment in mental illness underestimates inpatient suicide risk. BMJ 2016, 532, i267. [Google Scholar] [CrossRef]
- Tondo, L.; Pompili, M.; Forte, A.; Baldessarini, R.J. Suicide attempts in bipolar disorders: Comprehensive review of 101 reports. Acta Psychiatr. Scand. 2016, 133, 174–186. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Vieta, E.; Siamouli, M.; Valenti, M.; Magiria, S.; Oral, T.; Fresno, D.; Giannakopoulos, P.; Kaprinis, G.S. Treatment of bipolar disorder: A complex treatment for a multi-faceted disorder. Ann. Gen. Psychiatry 2007, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Geddes, J.R.; Miklowitz, D.J. Treatment of bipolar disorder. Lancet 2013, 381, 1672–1682. [Google Scholar] [CrossRef]
- Nestsiarovich, A.; Kumar, P.; Lauve, N.R.; Hurwitz, N.G.; Mazurie, A.J.; Cannon, D.C.; Zhu, Y.; Nelson, S.J.; Crisanti, A.S.; Kerner, B.; et al. Using Machine Learning Imputed Outcomes to Assess Drug-Dependent Risk of Self-Harm in Patients with Bipolar Disorder: A Comparative Effectiveness Study. JMIR Ment. Health 2021, 8, e24522. [Google Scholar] [CrossRef]
- Pacchiarotti, I.; Bond, D.J.; Baldessarini, R.J.; Nolen, W.A.; Grunze, H.; Licht, R.W.; Post, R.M.; Berk, M.; Goodwin, G.M.; Sachs, G.S.; et al. The International Society for Bipolar Disorders (ISBD) task force report on antidepressant use in bipolar disorders. Am. J. Psychiatry 2013, 170, 1249–1262. [Google Scholar] [CrossRef]
- Vazquez, G.; Tondo, L.; Baldessarini, R.J. Comparison of antidepressant responses in patients with bipolar vs. unipolar depression: A meta-analytic review. Pharmacopsychiatry 2011, 44, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Fergusson, D.; Doucette, S.; Glass, K.C.; Shapiro, S.; Healy, D.; Hebert, P.; Hutton, B. Association between suicide attempts and selective serotonin reuptake inhibitors: Systematic review of randomised controlled trials. BMJ 2005, 330, 396. [Google Scholar] [CrossRef] [Green Version]
- McElroy, S.L.; Kotwal, R.; Kaneria, R.; Keck, P.E., Jr. Antidepressants and suicidal behavior in bipolar disorder. Bipolar Disord. 2006, 8, 596–617. [Google Scholar] [CrossRef]
- InformedHealth.org. Depression: How Effective Are Antidepressants? Available online: https://www.ncbi.nlm.nih.gov/books/NBK361016/ (accessed on 1 September 2021).
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef]
- Fountoulakis, K.N. Refractoriness in bipolar disorder: Definitions and evidence-based treatment. CNS Neurosci. Ther. 2012, 18, 227–237. [Google Scholar] [CrossRef]
- Thase, M.E.; Rush, A.J. When at first you don’t succeed: Sequential strategies for antidepressant nonresponders. J. Clin. Psychiatry 1997, 58 (Suppl. 13), 23–29. [Google Scholar]
- Al-Harbi, K.S. Treatment-resistant depression: Therapeutic trends, challenges, and future directions. Patient Prefer. Adherence 2012, 6, 369–388. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.; Brown, W.A. Antidepressants versus placebo in major depression: An overview. World Psychiatry 2015, 14, 294–300. [Google Scholar] [CrossRef] [Green Version]
- Tondo, L.; Vazquez, G.H.; Baldessarini, R.J. Options for pharmacological treatment of refractory bipolar depression. Curr. Psychiatry Rep. 2014, 16, 431. [Google Scholar] [CrossRef]
- Reus, G.Z.; de Moura, A.B.; Borba, L.A.; Abelaira, H.M.; Quevedo, J. Strategies for Treatment-Resistant Depression: Lessons Learned from Animal Models. Mol. Neuropsychiatry 2019, 5, 178–189. [Google Scholar] [CrossRef]
- American Psychiatric Association. Task Force on Electroconvulsive, T. The Practice of ECT: Recommendations for Treatment, Training and Privileging. Convuls. Ther. 1990, 6, 85–120. [Google Scholar]
- O’Leary, D.; Paykel, E.; Todd, C.; Vardulaki, K. Suicide in primary affective disorders revisited: A systematic review by treatment era. J. Clin. Psychiatry 2001, 62, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, D.J.; Zhao, S.; Qi, F.; Nyakyoma, K.; Kwong, J.S.; Adams, C.E. Electroconvulsive therapy for treatment-resistant schizophrenia. Cochrane Database Syst. Rev. 2019, 3, CD011847. [Google Scholar] [CrossRef] [PubMed]
- Francis, A.; Fink, M. ECT response in catatonia. Am. J. Psychiatry 1992, 149, 581–582. [Google Scholar] [CrossRef]
- Duthie, A.C.; Perrin, J.S.; Bennett, D.M.; Currie, J.; Reid, I.C. Anticonvulsant Mechanisms of Electroconvulsive Therapy and Relation to Therapeutic Efficacy. J. ECT 2015, 31, 173–178. [Google Scholar] [CrossRef]
- Tsoukalas, I. How does ECT work? A new explanatory model and suggestions for non-convulsive applications. Med. Hypotheses 2020, 145, 110337. [Google Scholar] [CrossRef]
- Beale, M.D.; Kellner, C.H. ECT in treatment algorithms: No need to save the best for last. J. ECT 2000, 16, 1–2. [Google Scholar] [CrossRef]
- Esel, E.; Kose, K.; Hacimusalar, Y.; Ozsoy, S.; Kula, M.; Candan, Z.; Turan, T. The effects of electroconvulsive therapy on GABAergic function in major depressive patients. J. ECT 2008, 24, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Heninger, G.R.; Delgado, P.L.; Charney, D.S. The revised monoamine theory of depression: A modulatory role for monoamines, based on new findings from monoamine depletion experiments in humans. Pharmacopsychiatry 1996, 29, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Pfleiderer, B.; Michael, N.; Erfurth, A.; Ohrmann, P.; Hohmann, U.; Wolgast, M.; Fiebich, M.; Arolt, V.; Heindel, W. Effective electroconvulsive therapy reverses glutamate/glutamine deficit in the left anterior cingulum of unipolar depressed patients. Psychiatry Res. 2003, 122, 185–192. [Google Scholar] [CrossRef]
- Haskett, R.F. Electroconvulsive therapy’s mechanism of action: Neuroendocrine hypotheses. J. ECT 2014, 30, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Maffioletti, E.; Gennarelli, M.; Gainelli, G.; Bocchio-Chiavetto, L.; Bortolomasi, M.; Minelli, A. BDNF Genotype and Baseline Serum Levels in Relation to Electroconvulsive Therapy Effectiveness in Treatment-Resistant Depressed Patients. J. ECT 2019, 35, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Michael, N.; Erfurth, A.; Ohrmann, P.; Arolt, V.; Heindel, W.; Pfleiderer, B. Neurotrophic effects of electroconvulsive therapy: A proton magnetic resonance study of the left amygdalar region in patients with treatment-resistant depression. Neuropsychopharmacology 2003, 28, 720–725. [Google Scholar] [CrossRef] [Green Version]
- Zheng, W.; Cen, Q.; Nie, S.; Li, M.; Zeng, R.; Zhou, S.; Cai, D.; Jiang, M.; Huang, X. Serum BDNF levels and the antidepressant effects of electroconvulsive therapy with ketamine anaesthesia: A preliminary study. PeerJ 2021, 9, e10699. [Google Scholar] [CrossRef]
- Minelli, A.; Zanardini, R.; Abate, M.; Bortolomasi, M.; Gennarelli, M.; Bocchio-Chiavetto, L. Vascular Endothelial Growth Factor (VEGF) serum concentration during electroconvulsive therapy (ECT) in treatment resistant depressed patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 1322–1325. [Google Scholar] [CrossRef]
- Guloksuz, S.; Rutten, B.P.; Arts, B.; van Os, J.; Kenis, G. The immune system and electroconvulsive therapy for depression. J. ECT 2014, 30, 132–137. [Google Scholar] [CrossRef]
- Nobler, M.S.; Sackeim, H.A. Neurobiological correlates of the cognitive side effects of electroconvulsive therapy. J. ECT 2008, 24, 40–45. [Google Scholar] [CrossRef]
- Nordanskog, P.; Dahlstrand, U.; Larsson, M.R.; Larsson, E.M.; Knutsson, L.; Johanson, A. Increase in hippocampal volume after electroconvulsive therapy in patients with depression: A volumetric magnetic resonance imaging study. J. ECT 2010, 26, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Fink, M. Electroconvulsive Therapy; American Psychiatric Press: Washington, DC, USA, 1998. [Google Scholar]
- Vann Jones, S.; McCollum, R. Subjective memory complaints after electroconvulsive therapy: Systematic review. BJPsych Bull. 2019, 43, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Baldinger, P.; Lotan, A.; Frey, R.; Kasper, S.; Lerer, B.; Lanzenberger, R. Neurotransmitters and electroconvulsive therapy. J. ECT 2014, 30, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Gazdag, G.; Ungvari, G.S. Electroconvulsive therapy: 80 years old and still going strong. World J. Psychiatry 2019, 9, 1–6. [Google Scholar] [CrossRef]
- Belge, J.B.; van Diermen, L.; Sabbe, B.; Parizel, P.; Morrens, M.; Coppens, V.; Constant, E.; de Timary, P.; Sienaert, P.; Schrijvers, D.; et al. Inflammation, Hippocampal Volume, and Therapeutic Outcome following Electroconvulsive Therapy in Depressive Patients: A Pilot Study. Neuropsychobiology 2020, 79, 222–232. [Google Scholar] [CrossRef]
- Yrondi, A.; Sporer, M.; Peran, P.; Schmitt, L.; Arbus, C.; Sauvaget, A. Electroconvulsive therapy, depression, the immune system and inflammation: A systematic review. Brain Stimul. 2018, 11, 29–51. [Google Scholar] [CrossRef]
- Bauer, M.E.; Teixeira, A.L. Inflammation in psychiatric disorders: What comes first? Ann. N. Y. Acad. Sci. 2019, 1437, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Felger, J.C. Imaging the Role of Inflammation in Mood and Anxiety-related Disorders. Curr. Neuropharmacol. 2018, 16, 533–558. [Google Scholar] [CrossRef]
- Pfau, M.L.; Menard, C.; Russo, S.J. Inflammatory Mediators in Mood Disorders: Therapeutic Opportunities. Annu. Rev. Pharmacol. Toxicol. 2018, 58, 411–428. [Google Scholar] [CrossRef]
- Zhang, J.; Rane, G.; Dai, X.; Shanmugam, M.K.; Arfuso, F.; Samy, R.P.; Lai, M.K.; Kappei, D.; Kumar, A.P.; Sethi, G. Ageing and the telomere connection: An intimate relationship with inflammation. Ageing Res. Rev. 2016, 25, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Squassina, A.; Manchia, M.; Pisanu, C.; Ardau, R.; Arzedi, C.; Bocchetta, A.; Caria, P.; Cocco, C.; Congiu, D.; Cossu, E.; et al. Telomere attrition and inflammatory load in severe psychiatric disorders and in response to psychotropic medications. Neuropsychopharmacology 2020, 45, 2229–2238. [Google Scholar] [CrossRef]
- Blackburn, E.H. Telomere states and cell fates. Nature 2000, 408, 53–56. [Google Scholar] [CrossRef]
- Monaghan, P. Telomeres and life histories: The long and the short of it. Ann. N. Y. Acad. Sci. 2010, 1206, 130–142. [Google Scholar] [CrossRef]
- Calado, R.T. Telomeres and marrow failure. Hematol. Am. Soc. Hematol. Educ. Program 2009, 2009, 338–343. [Google Scholar] [CrossRef] [Green Version]
- Hayflick, L. Recent advances in the cell biology of aging. Mech. Ageing Dev. 1980, 14, 59–79. [Google Scholar] [CrossRef]
- Li, C.; Stoma, S.; Lotta, L.A.; Warner, S.; Albrecht, E.; Allione, A.; Arp, P.P.; Broer, L.; Buxton, J.L.; Da Silva Couto Alves, A.; et al. Genome-wide Association Analysis in Humans Links Nucleotide Metabolism to Leukocyte Telomere Length. Am. J. Hum. Genet. 2020, 106, 389–404. [Google Scholar] [CrossRef] [Green Version]
- Mangino, M.; Christiansen, L.; Stone, R.; Hunt, S.C.; Horvath, K.; Eisenberg, D.T.; Kimura, M.; Petersen, I.; Kark, J.D.; Herbig, U.; et al. DCAF4, a novel gene associated with leucocyte telomere length. J. Med. Genet. 2015, 52, 157–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Codd, V.; Nelson, C.P.; Albrecht, E.; Mangino, M.; Deelen, J.; Buxton, J.L.; Hottenga, J.J.; Fischer, K.; Esko, T.; Surakka, I.; et al. Identification of seven loci affecting mean telomere length and their association with disease. Nat. Genet. 2013, 45, 422–427, 427e1-2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, Y.B.; Martinsson, L.; Liu, J.J.; Forsell, Y.; Schalling, M.; Backlund, L.; Lavebratt, C. hTERT genetic variation in depression. J. Affect. Disord. 2016, 189, 62–69. [Google Scholar] [CrossRef]
- Aubert, G.; Lansdorp, P.M. Telomeres and aging. Physiol. Rev. 2008, 88, 557–579. [Google Scholar] [CrossRef] [PubMed]
- Manoliu, A.; Bosch, O.G.; Brakowski, J.; Bruhl, A.B.; Seifritz, E. The potential impact of biochemical mediators on telomere attrition in major depressive disorder and implications for future study designs: A narrative review. J. Affect. Disord. 2018, 225, 630–646. [Google Scholar] [CrossRef]
- Bodelon, C.; Savage, S.A.; Gadalla, S.M. Telomeres in molecular epidemiology studies. Prog. Mol. Biol. Transl. Sci. 2014, 125, 113–131. [Google Scholar] [CrossRef]
- Pisanu, C.; Tsermpini, E.E.; Skokou, M.; Kordou, Z.; Gourzis, P.; Assimakopoulos, K.; Congiu, D.; Meloni, A.; Balasopoulos, D.; Patrinos, G.P.; et al. Leukocyte telomere length is reduced in patients with major depressive disorder. Drug Dev. Res. 2020, 81, 268–273. [Google Scholar] [CrossRef]
- Simon, N.M.; Smoller, J.W.; McNamara, K.L.; Maser, R.S.; Zalta, A.K.; Pollack, M.H.; Nierenberg, A.A.; Fava, M.; Wong, K.K. Telomere shortening and mood disorders: Preliminary support for a chronic stress model of accelerated aging. Biol. Psychiatry 2006, 60, 432–435. [Google Scholar] [CrossRef]
- Tyrka, A.R.; Parade, S.H.; Price, L.H.; Kao, H.T.; Porton, B.; Philip, N.S.; Welch, E.S.; Carpenter, L.L. Alterations of Mitochondrial DNA Copy Number and Telomere Length With Early Adversity and Psychopathology. Biol. Psychiatry 2016, 79, 78–86. [Google Scholar] [CrossRef] [Green Version]
- Vance, M.C.; Bui, E.; Hoeppner, S.S.; Kovachy, B.; Prescott, J.; Mischoulon, D.; Walton, Z.E.; Dong, M.; Nadal, M.F.; Worthington, J.J.; et al. Prospective association between major depressive disorder and leukocyte telomere length over two years. Psychoneuroendocrinology 2018, 90, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Schutte, N.S.; Malouff, J.M. The association between depression and leukocyte telomere length: A meta-analysis. Depress. Anxiety 2015, 32, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Elvsashagen, T.; Vera, E.; Boen, E.; Bratlie, J.; Andreassen, O.A.; Josefsen, D.; Malt, U.F.; Blasco, M.A.; Boye, B. The load of short telomeres is increased and associated with lifetime number of depressive episodes in bipolar II disorder. J. Affect. Disord. 2011, 135, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Lima, I.M.; Barros, A.; Rosa, D.V.; Albuquerque, M.; Malloy-Diniz, L.; Neves, F.S.; Romano-Silva, M.A.; de Miranda, D.M. Analysis of telomere attrition in bipolar disorder. J. Affect. Disord. 2015, 172, 43–47. [Google Scholar] [CrossRef]
- Vasconcelos-Moreno, M.P.; Fries, G.R.; Gubert, C.; Dos Santos, B.; Fijtman, A.; Sartori, J.; Ferrari, P.; Grun, L.K.; Parisi, M.M.; Guma, F.; et al. Telomere Length, Oxidative Stress, Inflammation and BDNF Levels in Siblings of Patients with Bipolar Disorder: Implications for Accelerated Cellular Aging. Int. J. Neuropsychopharmacol. 2017, 20, 445–454. [Google Scholar] [CrossRef]
- Huang, Y.C.; Wang, L.J.; Tseng, P.T.; Hung, C.F.; Lin, P.Y. Leukocyte telomere length in patients with bipolar disorder: An updated meta-analysis and subgroup analysis by mood status. Psychiatry Res. 2018, 270, 41–49. [Google Scholar] [CrossRef]
- Martinsson, L.; Wei, Y.; Xu, D.; Melas, P.A.; Mathe, A.A.; Schalling, M.; Lavebratt, C.; Backlund, L. Long-term lithium treatment in bipolar disorder is associated with longer leukocyte telomeres. Transl. Psychiatry 2013, 3, e261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squassina, A.; Pisanu, C.; Congiu, D.; Caria, P.; Frau, D.; Niola, P.; Melis, C.; Baggiani, G.; Lopez, J.P.; Cruceanu, C.; et al. Leukocyte telomere length positively correlates with duration of lithium treatment in bipolar disorder patients. Eur. Neuropsychopharmacol. 2016, 26, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Pisanu, C.; Congiu, D.; Manchia, M.; Caria, P.; Cocco, C.; Dettori, T.; Frau, D.V.; Manca, E.; Meloni, A.; Nieddu, M.; et al. Differences in telomere length between patients with bipolar disorder and controls are influenced by lithium treatment. Pharmacogenomics 2020, 21, 533–540. [Google Scholar] [CrossRef]
- Hough, C.M.; Bersani, F.S.; Mellon, S.H.; Epel, E.S.; Reus, V.I.; Lindqvist, D.; Lin, J.; Mahan, L.; Rosser, R.; Burke, H.; et al. Leukocyte telomere length predicts SSRI response in major depressive disorder: A preliminary report. Mol. Neuropsychiatry 2016, 2, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Ryan, K.M.; McLoughlin, D.M. Telomere length in depression and association with therapeutic response to electroconvulsive therapy and cognitive side-effects. Psychol. Med. 2020, 50, 2096–2106. [Google Scholar] [CrossRef] [PubMed]
- Minelli, A.; Abate, M.; Zampieri, E.; Gainelli, G.; Trabucchi, L.; Segala, M.; Sartori, R.; Gennarelli, M.; Conca, A.; Bortolomasi, M. Seizure Adequacy Markers and the Prediction of Electroconvulsive Therapy Response. J. ECT 2016, 32, 88–92. [Google Scholar] [CrossRef]
- Muneer, A.; Minhas, F.A. Telomere Biology in Mood Disorders: An Updated, Comprehensive Review of the Literature. Clin. Psychopharmacol. Neurosci. 2019, 17, 343–363. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, N.; Boehner, M.; Groenen, F.; Kalb, R. Telomere length of patients with major depression is shortened but independent from therapy and severity of the disease. Depress. Anxiety 2010, 27, 1111–1116. [Google Scholar] [CrossRef]
- Mendes-Silva, A.P.; Vieira, E.L.M.; Xavier, G.; Barroso, L.S.S.; Bertola, L.; Martins, E.A.R.; Brietzke, E.M.; Belangero, S.I.N.; Diniz, B.S. Telomere shortening in late-life depression: A potential marker of depression severity. Brain Behav. 2021, 11, e2255. [Google Scholar] [CrossRef]
- Gao, X.; Li, S.; Dong, S.; Li, J.; Yan, Y.; Zhang, T.; Chen, W. Association between Body Weight and Telomere Length is Predominantly Mediated through C-Reactive Protein. J. Clin. Endocrinol. Metab. 2021, 106, e4634–e4640. [Google Scholar] [CrossRef]
- The Telomeres Mendelian Randomization Collaboration; Haycock, P.C.; Burgess, S.; Nounu, A.; Zheng, J.; Okoli, G.N.; Bowden, J.; Wade, K.H.; Timpson, N.J.; Evans, D.M.; et al. Association Between Telomere Length and Risk of Cancer and Non-Neoplastic Diseases: A Mendelian Randomization Study. JAMA Oncol. 2017, 3, 636–651. [Google Scholar] [CrossRef] [PubMed]
- Wium-Andersen, M.K.; Orsted, D.D.; Rode, L.; Bojesen, S.E.; Nordestgaard, B.G. Telomere length and depression: Prospective cohort study and Mendelian randomisation study in 67 306 individuals. Br. J. Psychiatry 2017, 210, 31–38. [Google Scholar] [CrossRef]
- Verhoeven, J.E.; Penninx, B.; Milaneschi, Y. Unraveling the association between depression and telomere length using genomics. Psychoneuroendocrinology 2019, 102, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Demanelis, K.; Jasmine, F.; Chen, L.S.; Chernoff, M.; Tong, L.; Delgado, D.; Zhang, C.; Shinkle, J.; Sabarinathan, M.; Lin, H.; et al. Determinants of telomere length across human tissues. Science 2020, 369, eaaz6876. [Google Scholar] [CrossRef]
- Gampawar, P.; Schmidt, R.; Schmidt, H. Leukocyte Telomere Length Is Related to Brain Parenchymal Fraction and Attention/Speed in the Elderly: Results of the Austrian Stroke Prevention Study. Front. Psychiatry 2020, 11, 100. [Google Scholar] [CrossRef] [Green Version]
- King, K.S.; Kozlitina, J.; Rosenberg, R.N.; Peshock, R.M.; McColl, R.W.; Garcia, C.K. Effect of leukocyte telomere length on total and regional brain volumes in a large population-based cohort. JAMA Neurol. 2014, 71, 1247–1254. [Google Scholar] [CrossRef] [Green Version]
- Haukvik, U.K.; Gurholt, T.P.; Nerland, S.; Elvsashagen, T.; Akudjedu, T.N.; Alda, M.; Alnaes, D.; Alonso-Lana, S.; Bauer, J.; Baune, B.T.; et al. In vivo hippocampal subfield volumes in bipolar disorder-A mega-analysis from The Enhancing Neuro Imaging Genetics through Meta-Analysis Bipolar Disorder Working Group. Hum. Brain Mapp. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fries, G.R.; Bauer, I.E.; Scaini, G.; Valvassori, S.S.; Walss-Bass, C.; Soares, J.C.; Quevedo, J. Accelerated hippocampal biological aging in bipolar disorder. Bipolar Disord. 2020, 22, 498–507. [Google Scholar] [CrossRef]
- Zhang, Y.; Wei, H.; Cronin, M.J.; He, N.; Yan, F.; Liu, C. Longitudinal atlas for normative human brain development and aging over the lifespan using quantitative susceptibility mapping. Neuroimage 2018, 171, 176–189. [Google Scholar] [CrossRef]
- Fredericks, C.A.; Brown, J.A.; Deng, J.; Kramer, A.; Ossenkoppele, R.; Rankin, K.; Kramer, J.H.; Miller, B.L.; Rabinovici, G.D.; Seeley, W.W. Intrinsic connectivity networks in posterior cortical atrophy: A role for the pulvinar? Neuroimage Clin. 2019, 21, 101628. [Google Scholar] [CrossRef] [PubMed]
- Penner, J.; Osuch, E.A.; Schaefer, B.; Theberge, J.; Neufeld, R.W.J.; Menon, R.S.; Rajakumar, N.; Bourne, J.A.; Williamson, P.C. Higher order thalamic nuclei resting network connectivity in early schizophrenia and major depressive disorder. Psychiatry Res. Neuroimaging 2018, 272, 7–16. [Google Scholar] [CrossRef]
- Yu, J.; Kanchi, M.M.; Rawtaer, I.; Feng, L.; Kumar, A.P.; Kua, E.H.; Mahendran, R. The functional and structural connectomes of telomere length and their association with cognition in mild cognitive impairment. Cortex 2020, 132, 29–40. [Google Scholar] [CrossRef]
- Cotrena, C.; Branco, L.D.; Shansis, F.M.; Fonseca, R.P. Executive function impairments in depression and bipolar disorder: Association with functional impairment and quality of life. J. Affect. Disord. 2016, 190, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, D.K.; Nurnberger, J.I., Jr. A rapid non-enzymatic method for the preparation of HMW DNA from blood for RFLP studies. Nucleic Acids Res. 1991, 19, 5444. [Google Scholar] [CrossRef] [PubMed]
- Cawthon, R.M. Telomere measurement by quantitative PCR. Nucleic Acids Res. 2002, 30, e47. [Google Scholar] [CrossRef]
- Chang, C.C.; Chow, C.C.; Tellier, L.C.; Vattikuti, S.; Purcell, S.M.; Lee, J.J. Second-generation PLINK: Rising to the challenge of larger and richer datasets. Gigascience 2015, 4, 7. [Google Scholar] [CrossRef]
- Das, S.; Forer, L.; Schonherr, S.; Sidore, C.; Locke, A.E.; Kwong, A.; Vrieze, S.I.; Chew, E.Y.; Levy, S.; McGue, M.; et al. Next-generation genotype imputation service and methods. Nat. Genet. 2016, 48, 1284–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, K.; Taskesen, E.; van Bochoven, A.; Posthuma, D. Functional mapping and annotation of genetic associations with FUMA. Nat. Commun. 2017, 8, 1826. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with TRD (n = 148) | Controls (n = 335) | Statistics | p | |
|---|---|---|---|---|
| Age, median (IQR) | 56 (20) | 43 (22) | 14,125 a | <0.0001 |
| Gender (women, %) | 67.6 | 53.1 | 8.76 b | 0.004 |
| Unadjusted Analyses | Analyses Adjusted for Age | ||||
|---|---|---|---|---|---|
| LTL, median (IQR) | U | p | Quade’s F | p | |
| Patients with TRD (n = 148) | 0.77 (0.30) | 13,015 | <0.0001 | 49.17 | <0.0001 |
| Controls (n = 335) | 1.03 (0.48) | ||||
| Unadjusted Analyses | Analyses Adjusted for Age | ||||
|---|---|---|---|---|---|
| LTL, median (IQR) | U | p | Quade’s F | p | |
| Responders at T1 (n = 119) | 0.77 (0.30) | 777 | 0.68 | 0.04 | 0.85 |
| Non-Responders at T1 (n = 14) | 0.85 (0.34) | ||||
| Responders at T2 (n = 65) | 0.77 (0.34) | 767 | 0.34 | 0.54 | 0.46 |
| Non-Responders at T2 (n = 27) | 0.88 (0.27) | ||||
| Remitters (n = 53) | 0.75 (0.32) | 769 | 0.18 | 1.50 | 0.23 |
| Non-remitters (n = 35) | 0.88 (0.29) | ||||
| Median (IQR) | Spearman’s rho | p | partial corr. coeff. | p | |
| Delta % MADRS T1-T0 | 75 (77) | −0.11 | 0.23 | −0.12 | 0.17 |
| Delta % MADRS T2-T0 | 78 (118) | −0.16 | 0.13 | −0.18 | 0.10 |
| MADRS scores at T0 | 33 (36) | 0.03 | 0.73 | 0.03 | 0.76 |
| MADRS scores at T1 | 8 (7) | 0.11 | 0.20 | 0.13 | 0.15 |
| MADRS scores at T2 | 7.5 (18) | 0.17 | 0.12 | 0.17 | 0.12 |
| Number of ECT sessions | 7 (3) | 0.03 | 0.71 | 0.02 | 0.79 |
| Unadjusted Analyses | Analyses Adjusted for Age | |||
|---|---|---|---|---|
| Variable | Statistics | p | Statistics | p |
| Years of education, median (IQR): 8 (8) | 0.14 a | 0.10 | 0.01 b | 0.90 |
| BMI, median (IQR): 26.4 (6.7) | −0.16 a | 0.067 | −0.19 b | 0.027 |
| Psychotic symptoms (70.9%) | 2162 c | 0.687 | 0.09 d | 0.76 |
| Smoking (35.1%) | 2405 c | 0.72 | 0.24 d | 0.63 |
| History of substance abuse (5.1%) | 435 c | 0.85 | 0.27 d | 0.60 |
| Comorbid alcohol abuse (2.7%) | 244 c | 0.60 | 0.10 d | 0.75 |
| Comorbid anxiety disorders (27.7%) | 2030 c | 0.48 | 1.64 d | 0.20 |
| Comorbid personality disorders (23.6%) | 1456 c | 0.019 | 2.36 d | 0.13 |
| Comorbid cardiometabolic disorders (27.0%) | 2055 c | 0.65 | 1.74 d | 0.19 |
| Unadjusted Analyses | Analyses Adjusted for Age | |||
|---|---|---|---|---|
| Variable | U | p | Quade’s F | p |
| Antipsychotics (76.2%) | 1730 | 0.30 | 0.56 | 0.46 |
| Antidepressants (95.2%) | 378 | 0.31 | 0.11 | 0.19 |
| Mood stabilizers (15.0%) | 1258 | 0.53 | 0.15 | 0.70 |
| Benzodiazepines (87.1%) | 1150 | 0.34 | 1.05 | 0.31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pisanu, C.; Vitali, E.; Meloni, A.; Congiu, D.; Severino, G.; Ardau, R.; Chillotti, C.; Trabucchi, L.; Bortolomasi, M.; Gennarelli, M.; et al. Investigating the Role of Leukocyte Telomere Length in Treatment-Resistant Depression and in Response to Electroconvulsive Therapy. J. Pers. Med. 2021, 11, 1100. https://doi.org/10.3390/jpm11111100
Pisanu C, Vitali E, Meloni A, Congiu D, Severino G, Ardau R, Chillotti C, Trabucchi L, Bortolomasi M, Gennarelli M, et al. Investigating the Role of Leukocyte Telomere Length in Treatment-Resistant Depression and in Response to Electroconvulsive Therapy. Journal of Personalized Medicine. 2021; 11(11):1100. https://doi.org/10.3390/jpm11111100
Chicago/Turabian StylePisanu, Claudia, Erika Vitali, Anna Meloni, Donatella Congiu, Giovanni Severino, Raffaella Ardau, Caterina Chillotti, Luigi Trabucchi, Marco Bortolomasi, Massimo Gennarelli, and et al. 2021. "Investigating the Role of Leukocyte Telomere Length in Treatment-Resistant Depression and in Response to Electroconvulsive Therapy" Journal of Personalized Medicine 11, no. 11: 1100. https://doi.org/10.3390/jpm11111100