
Impact of MAFLD on HBV-Related Stage 0/A Hepatocellular Carcinoma after Curative Resection

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Ethics
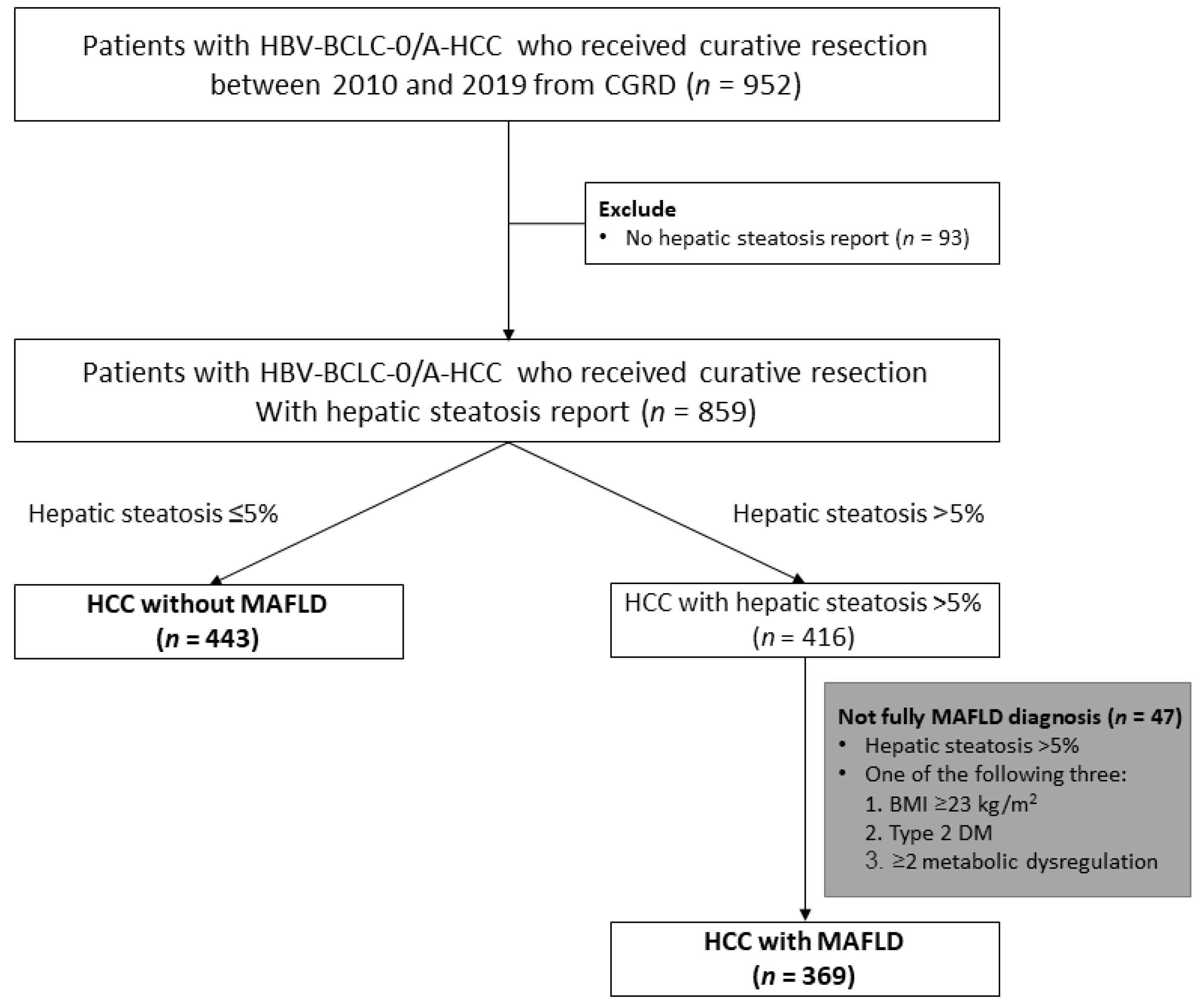
2.2. Study Population
2.3. Data Collection
2.4. Study Outcomes
2.5. Definition
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
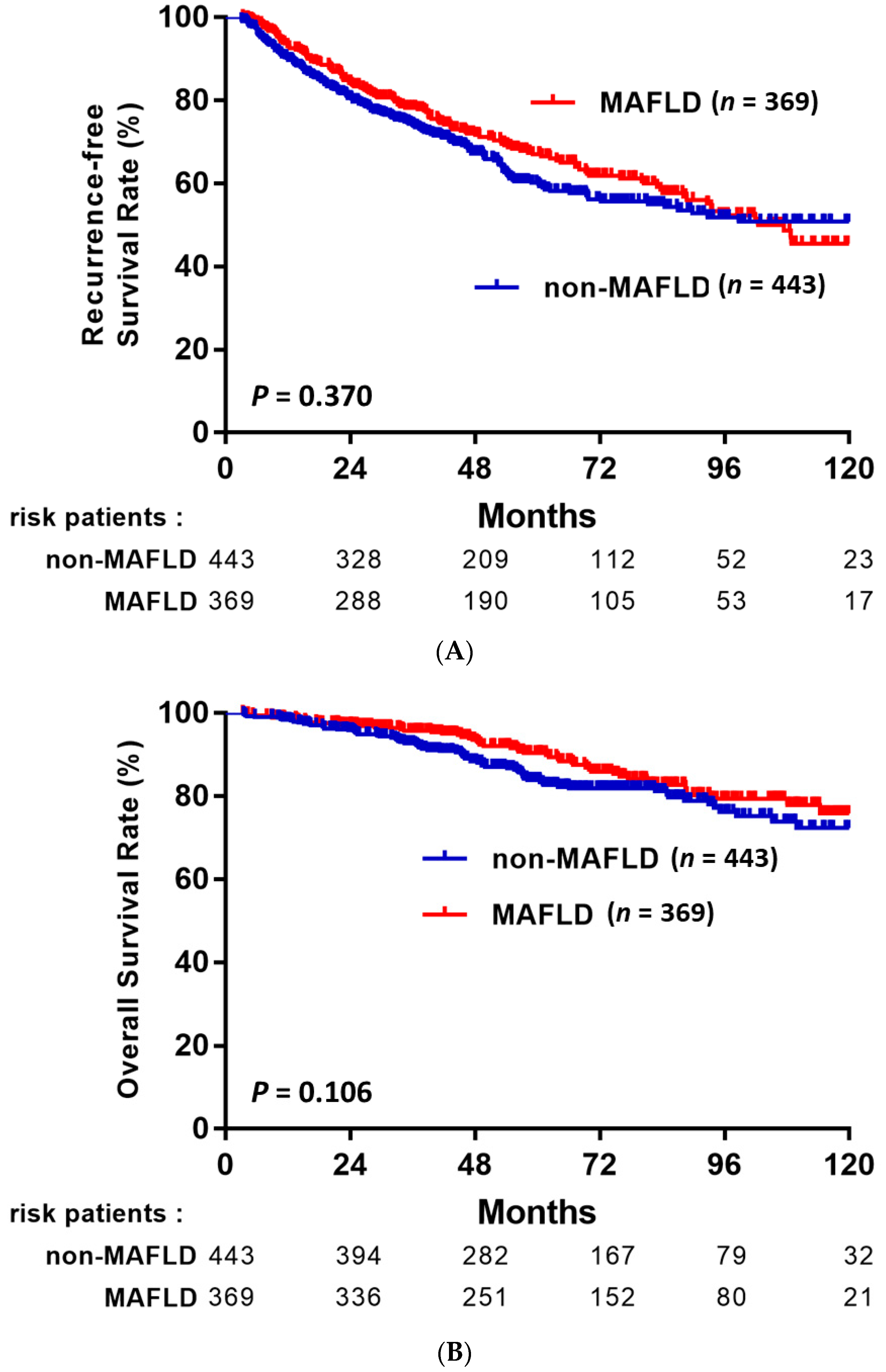
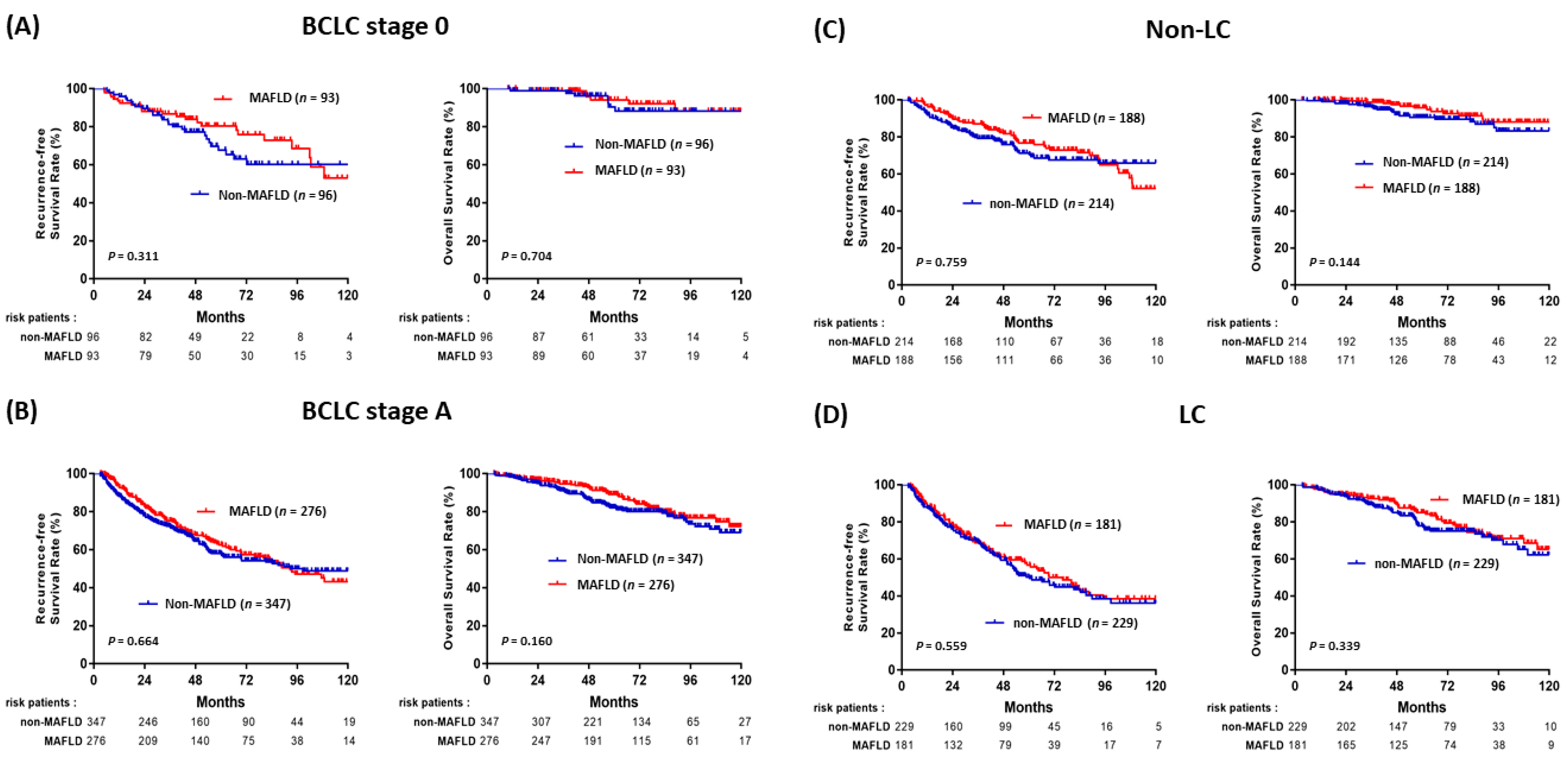
3.2. Impact of MAFLD on the Outcomes of HBV-HCC
3.3. Factors Associated with HCC Recurrence
3.4. Factors Associated with Overall Survival
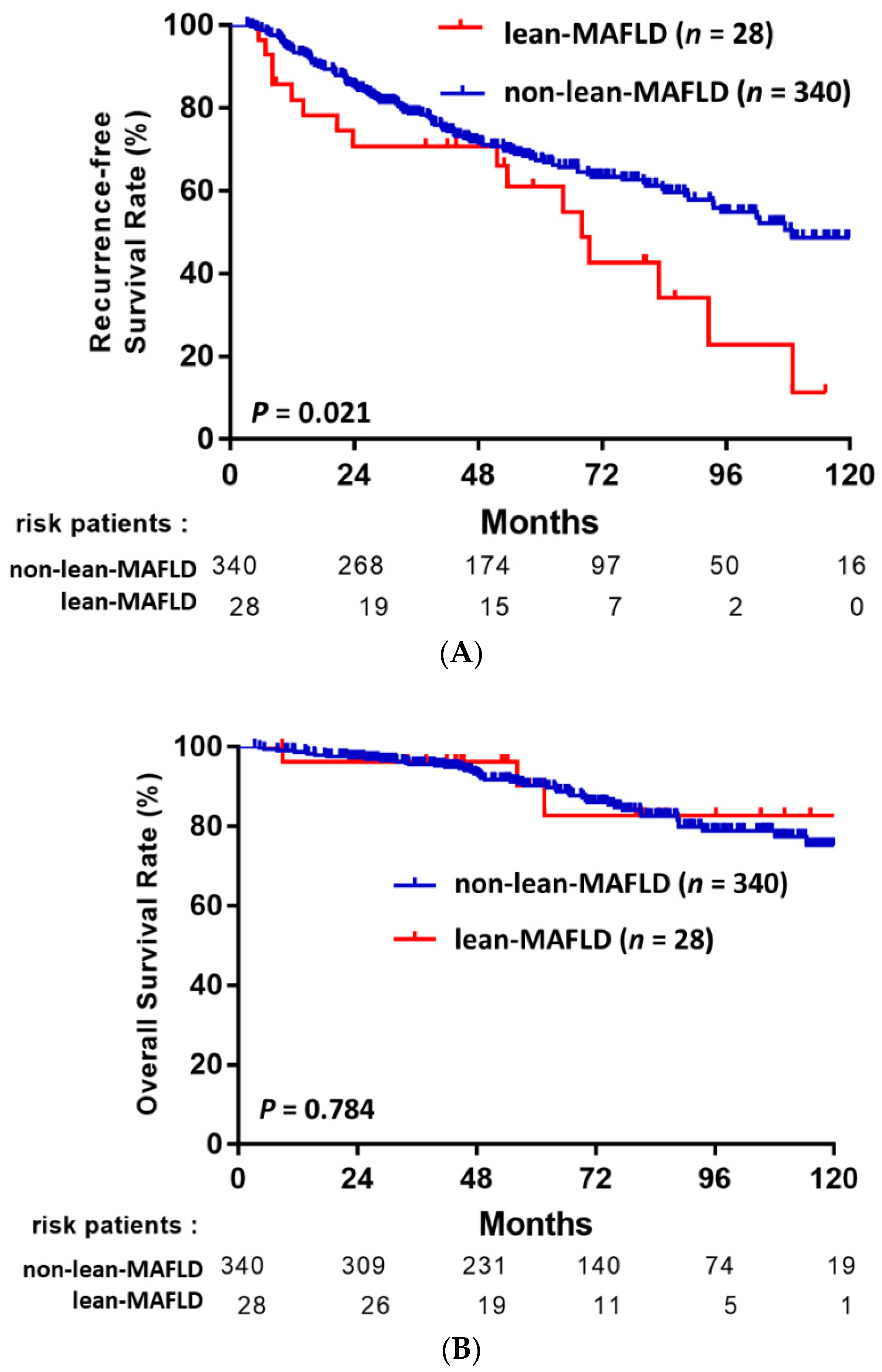
3.5. MAFLD Subgroup Analysis: Lean-MAFLD Is a Risk Factor
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MAFLD | metabolic-associated fatty liver disease |
| HCC | hepatocellular carcinoma |
| BCLC | Barcelona Clinic Liver Cancer |
| OS | overall survival |
| RFS | recurrence-free survival |
| HR | hazard ratio |
| HBV | Hepatitis B virus |
| AFP | alpha-fetoprotein |
| HBsAg | hepatitis B surface antigen |
| HBeAg | hepatitis B e antigen |
| BMI | body mass index |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Erratum: Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2020, 70, 313. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An up-date. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [PubMed]
- Tabrizian, P.; Jibara, G.; Shrager, B.; Schwartz, M.; Roayaie, S. Recurrence of hepatocellular cancer after resection: Patterns, treatments, and prognosis. Ann. Surg. 2015, 261, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Ercolani, G.; Grazi, G.L.; Ravaioli, M.; Del Gaudio, M.; Gardini, A.; Cescon, M.; Varotti, G.; Cetta, F.; Cavallari, A. Liver resection for hepatocellular carcinoma on cirrhosis: Univariate and multivariate analysis of risk factors for intrahepatic recurrence. Ann. Surg. 2003, 237, 536–543. [Google Scholar] [CrossRef]
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef]
- Huang, Y.H.; Wu, J.C.; Chen, C.H.; Chang, T.T.; Lee, P.C.; Chau, G.Y.; Lui, W.Y.; Chang, F.Y.; Lee, S.D. Comparison of recurrence after hepatic resection in patients with hepatitis B vs. hepatitis C-related small hepatocellular carcinoma in hepatitis B virus endemic area. Liver Int. 2005, 25, 236–241. [Google Scholar] [CrossRef]
- Hirokawa, F.; Hayashi, M.; Asakuma, M.; Shimizu, T.; Inoue, Y.; Uchiyama, K. Risk factors and patterns of early recurrence after curative hepatectomy for hepatocellular carcinoma. Surg. Oncol. 2016, 25, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Kuk, D.; Gonen, M.; Balachandran, V.P.; Kingham, T.P.; Allen, P.J.; D’Angelica, M.I.; Jarnagin, W.R.; DeMatteo, R.P. Actual 10-Year Survivors After Resection of Hepatocellular Carcinoma. Ann. Surg. Oncol. 2017, 24, 1358–1366. [Google Scholar] [CrossRef]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Powell, E.E.; Wong, V.W.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- White, D.L.; Kanwal, F.; El-Serag, H.B. Association between nonalcoholic fatty liver disease and risk for hepatocellular cancer, based on systematic review. Clin. Gastroenterol. Hepatol. 2012, 10, 1342–1359.e1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.; Stepanova, M.; Ong, J.P.; Jacobson, I.M.; Bugianesi, E.; Duseja, A.; Eguchi, Y.; Wong, V.W.; Negro, F.; Yilmaz, Y.; et al. Nonalcoholic Steatohepatitis Is the Fastest Growing Cause of Hepatocellular Carcinoma in Liver Transplant Candidates. Clin. Gastroenterol. Hepatol. 2019, 17, 748–755.e743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [CrossRef] [PubMed]
- Wong, V.W.; Chan, W.K.; Chitturi, S.; Chawla, Y.; Dan, Y.Y.; Duseja, A.; Fan, J.; Goh, K.L.; Hamaguchi, M.; Hashimoto, E.; et al. Asia-Pacific Working Party on Non-alcoholic Fatty Liver Disease guidelines 2017-Part 1: Definition, risk factors and assessment. J. Gastroenterol. Hepatol. 2018, 33, 70–85. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An inter-national expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; International Consensus, P. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1991. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Huang, J.; Wang, M.; Kumar, R.; Liu, Y.; Liu, S.; Wu, Y.; Wang, X.; Zhu, Y. Comparison of MAFLD and NAFLD diagnostic criteria in real world. Liver Int. 2020, 40, 2082–2089. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef] [Green Version]
- Xie, D.Y.; Ren, Z.G.; Zhou, J.; Fan, J.; Gao, Q. 2019 Chinese clinical guidelines for the management of hepatocellular car-cinoma: Updates and insights. Hepatobiliary Surg. Nutr. 2020, 9, 452–463. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and diagnosis of diabetes. Diabetes Care 2015, 38 (Suppl. S1), S8–S16. [Google Scholar] [CrossRef] [Green Version]
- Buzova, D.; Maugeri, A.; Liguori, A.; Napodano, C.; Lo Re, O.; Oben, J.; Alisi, A.; Gasbarrini, A.; Grieco, A.; Cerveny, J.; et al. Circulating histone signature of human lean metabolic-associated fatty liver disease (MAFLD). Clin. Epigenetics 2020, 12, 126. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Cho, Y.; Jeong, S.W.; Kim, S.U.; Lee, J.W.; Korean, N.S.G. From nonalcoholic fatty liver disease to metabol-ic-associated fatty liver disease: Big wave or ripple? Clin. Mol. Hepatol. 2021, 27, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.C.; Su, H.J.; Kao, J.H.; Tseng, T.C.; Yang, H.C.; Su, T.H.; Chen, P.J.; Liu, C.J. Clinical and Histologic Features of Patients with Biopsy-Proven Metabolic Dysfunction-Associated Fatty Liver Disease. Gut Liver 2021, 15, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.F.; Wan, B.; Wu, Y.L.; Huang, J.F.; Zhu, Y.Y.; Li, Y.B. Clinic-pathological features of metabolic associated fatty liver disease with hepatitis B virus infection. World J. Gastroenterol. 2021, 27, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.S.; Lee, H.Y.; Chung, S.W.; Kim, S.W.; Chang, Y.; Lee, Y.B.; Cho, E.J.; Lee, J.H.; Yu, S.J.; Kim, H.; et al. Prognostic impact of concurrent nonalcoholic fatty liver disease in patients with chronic hepatitis B-related hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2020, 35, 1960–1968. [Google Scholar] [CrossRef]
- Myers, S.; Neyroud-Caspar, I.; Spahr, L.; Gkouvatsos, K.; Fournier, E.; Giostra, E.; Magini, G.; Frossard, J.L.; Bascaron, M.E.; Vernaz, N.; et al. NAFLD and MAFLD as emerging causes of HCC: A populational study. JHEP Rep. 2021, 3, 100231. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Chan, Z.; Magkos, F. Lean, but not healthy: The ‘metabolically obese, normal-weight’ phenotype. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 408–417. [Google Scholar] [CrossRef]
- Cruz, A.D.; Bugianesi, E.; George, J.; Day, C.; Liaquat, H.; Charatcharoenwitthaya, P.; Mills, P.; Dam-Larsen, S.; Bjornsson, E.; Haflidadottir, S.; et al. 379 Characteristics and Long-Term Prognosis of Lean Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2014, 5, S-909. [Google Scholar] [CrossRef]
- Hagstrom, H.; Nasr, P.; Ekstedt, M.; Hammar, U.; Stal, P.; Hultcrantz, R.; Kechagias, S. Risk for development of severe liver disease in lean patients with nonalcoholic fatty liver disease: A long-term follow-up study. Hepatol. Commun. 2018, 2, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.M.; Kao, J.H.; Wang, C.C. The metabolic profiles and body composition of lean metabolic associated fatty liver disease. Hepatol. Int. 2021, 15, 405–412. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 812) | HCC with MAFLD (n = 369) | HCC without MAFLD (n = 443) | p-Value | |
|---|---|---|---|---|
| Age (years), mean ± SD | 56.2 ± 10.7 | 56.2 ± 10.2 | 56.2 ± 11.1 | 0.312 |
| Male gender, n (%) | 693 (85.3) | 320 (86.7) | 373 (84.2) | 0.908 |
| Body mass index (kg/m2), mean ± SD | 25.2 ± 3.2 | 26.7 ± 3.3 | 23.9 ± 3.4 | <0.001 |
| DM, n (%) | 199 (24.6) | 117 (31.7) | 82 (18.6) | <0.001 |
| Hypertension, n (%) | 269 (33.1) | 149 (40.4) | 120 (27.1) | <0.001 |
| Family history of HCC, n (%) | 130 (16) | 56 (15.2) | 74 (16.7) | 0.545 |
| Alcohol drinking | 0.744 | |||
| Never, n (%) | 596 (73.5) | 273 (74.0) | 323 (73.7) | |
| Current, n (%) | 95 (11.7) | 45 (12.2) | 50 (11.3) | |
| Quit, n (%) | 120 (14.8) | 51 (13.8) | 69 (15.6) | |
| Smoking | 0.227 | |||
| Never, n (%) | 536 (66.1) | 229 (64.8) | 297 (67.2) | |
| Current, n (%) | 160 (19.7) | 82 (22.2) | 78 (17.6) | |
| Quit, n (%) | 115 (14.2) | 48 (13.0) | 67 (15.2) | |
| Platelets (<150 × 109/L), n (%) | 309 (39.4) | 113 (31.3) | 196 (46.3) | <0.001 |
| AST (U/L), mean ± SD | 36.8 ± 20.7 | 37.7 ± 20.6 | 36.0 ± 20.7 | 0.244 |
| ALT (U/L), mean ± SD | 42.5 ± 34.4 | 46.9 ± 37.8 | 38.9 ± 30.8 | 0.001 |
| Total bilirubin (mg/dL), mean ± SD | 0.8 ± 0.4 | 0.7 ± 0.4 | 0.8 ± 0.3 | 0.403 |
| Albumin (g/dL), mean ± SD | 4.2 ± 0.5 | 4.3 ± 0.5 | 4.2 ± 0.5 | 0.773 |
| Creatinine (mg/dL), mean ± SD | 1.1 ± 3.0 | 1.1 ± 4.1 | 1.1 ± 1.3 | 0.653 |
| eGFR (mL/min/1.732), mean ± SD | 92.9 ± 24.4 | 94.2 ± 21.8 | 91.9 ± 26.4 | 0.185 |
| AFP (>20 ng/mL), n (%) | 344 (43.4) | 138 (38.1) | 206 (47.9) | 0.006 |
| AFP (>200 ng/mL), n (%) | 170 (21.5) | 62 (17.1) | 108 (25.1) | 0.006 |
| Child–Pugh grade (A/B), n (%) | 766/8 (99/1) | 353/3 (99.2/0.8) | 413/5 (98.8/1.2) | 0.628 |
| ALBI grade(I/II/III), n (%) | 621/148/4 (80.3/19.1/0.6) | 298/55/2 (83.9/15.5/0.6) | 323/93/2 (77.3/22.2/0.5) | 0.059 |
| HBeAg positive, n (%) | 83 (13.1) | 33 (12) | 50 (14) | 0.428 |
| HBV DNA | 0.139 | |||
| Undetectable, n (%) | 146 (43.1) | 66 (49.6) | 80 (38.8) | |
| Detectable, n (%) | 193 (56.9) | 67 (50.4) | 126 (61.2) | |
| NUCs treatment, n (%) | 368 (45.3) | 150 (40.7) | 218 (49.2) | 0.015 |
| Ishak score, mean ± SD | 4.1 ± 1.9 | 4.2 ± 1.7 | 4.0 ± 2.0 | 0.154 |
| Liver cirrhosis, n (%) | 410 (50.5) | 181 (49.1) | 229 (51.7) | 0.453 |
| BCLC stage 0/A, n (%) | 189/623 (23.3/76.7) | 93/276 (25.2/74.8) | 96 / 347 (21.7/78.3) | 0.236 |
| Tumor size (cm) a, mean ± SD | 2.7 ± 1.0 | 2.7 ± 1.1 | 2.7 ± 1.0 | 0.695 |
| Multiple tumors, n (%) | 96 (11.8) | 49 (13.3) | 47 (10.6) | 0.241 |
| Histological grade | <0.001 | |||
| Well-differentiated, n (%) | 146 (18.0) | 86 (23.4) | 60 (13.6) | |
| Moderately differentiated, n (%) | 511 (63.2) | 191 (52) | 320 (72.4) | |
| Poorly differentiated, n (%) | 152 (18.8) | 90 (24.5) | 62 (14) | |
| Microvascular invasion, n (%) | 250 (30.8) | 90 (24.5) | 160 (36.1) | <0.001 |
| Capsule invasion, n (%) | 654 (80.5) | 296 (80.2) | 358 (80.8) | 0.543 |
| Satellite nodules, n (%) | 24 (3.0) | 13 (3.6) | 11 (2.5) | 0.376 |
| Follow-up (months), mean ± SD | 65.1 ± 32.8 | 67.2 ± 32.6 | 63.4 ± 33.0 | 0.102 |
| Univariate | Multivariate | ||||
|---|---|---|---|---|---|
| Variable | Comparison | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Age (years) | Per one-year increase | 1.016 (1.006–1.027) | 0.003 | 1.023 (1.003–1.042) | 0.020 |
| Sex | Male vs. Female | 1.201 (0.858–1.908) | 0.286 | ||
| DM | Yes vs. No | 1.492 (1.166–1.908) | 0.001 | ||
| Hypertension | Yes vs. No | 1.148 (0.907–1.454) | 0.251 | ||
| Alcohol drinking | Current vs. Never/Past | 1.106 (0.863–1.418) | 0.426 | ||
| Smoking | Current vs. Never/Past | 1.168 (0.924–1.477) | 0.195 | ||
| HCC family history | Yes vs. No | 1.153 (0.864–1.539) | 0. 332 | ||
| HBeAg | Positive vs. Negative | 1.278 (0.889–1.839) | 0.186 | ||
| HBV DNA (IU/mL) | Detectable vs. Undetectable | 1.071 (0.737–1.555) | 0.720 | ||
| NUCs treatment | Yes vs. No | 1.056 (0.837–1.333) | 0.664 | ||
| AST (U/L) | >40 vs. ≤40 | 1.462 (1.142–1.874) | 0.003 | ||
| ALT (U/L) | >40 vs. ≤40 | 1.301 (1.029–1.647) | 0.028 | ||
| Platelets (109/L) | <150 vs. ≥150 | 1.524 (1.208–1.922) | <0.001 | ||
| AFP (ng/mL) | >200 vs. ≤200 | 1.028 (0.776–1.361) | 0.847 | ||
| Albumin (mg/dL) | Per 1 unit decrease | 1.295 (1.093–1.757) | 0.007 | ||
| Child–Pugh class | B vs. A | 1.209 (0.387–3.775) | 0.744 | ||
| ALBI grade | II/III vs. I | 1.166 (0.878–1.548) | 0.289 | ||
| Liver cirrhosis | Yes vs. No | 2.117 (1.673–2.679) | <0.001 | 2.178 (1.146–3.282) | <0.001 |
| BCLC stage | A vs. 0 | 1.615 (1.195–2.182) | 0.002 | ||
| Tumor no. | Multiple vs. Single | 1.339 (0.985–1.819) | 0.062 | ||
| Tumor diameter (cm) | Per 1 cm increase | 1.218 (1.090–1.361) | <0.001 | ||
| Histological grade | Poor/Moderate vs. Well | 1.230 (0.908–1.667) | 0.181 | ||
| Microvascular invasion | Yes vs. No | 1.150 (0.902–1.467) | 0.258 | ||
| Capsule invasion | Yes vs. No | 1.022 (0.766–1.363) | 0.883 | ||
| Satellite nodules | Yes vs. No | 2.418 (1.437–4.060) | 0.001 | ||
| MAFLD | Yes vs. No | 0.902 (0.719–1.131) | 0.370 | ||
| Univariate | Multivariate | ||||
|---|---|---|---|---|---|
| Variable | Comparison | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Age (years) | Per one-year increase | 1.017 (1.000–1.034) | 0.051 | ||
| Sex | Male vs Female | 1.188 (0.702–2.009) | 0.521 | ||
| DM | Yes vs. No | 1.215 (0.815–1.812) | 0.339 | ||
| Hypertension | Yes vs. No | 1.183 (0.817–1.712) | 0.374 | ||
| Alcohol drinking | Current vs. Never/Past | 1.357 (0.934–1.971) | 0.109 | 1.830 (1.032–3.244) | 0.039 |
| Smoking | Current vs. Never/Past | 1.438 (1.004–2.059) | 0.048 | ||
| HCC family history | Yes vs. No | 0.840 (0.515–1.370) | 0.485 | ||
| HBeAg | Positive vs. Negative | 1.208 (0.685–2.128) | 0.514 | ||
| HBV DNA (IU/mL) | Detectable vs. Undetectable | 1.553 (0.903–2.670) | 0.112 | ||
| NUCs treatment | Yes vs. No | 0.852 (0.735–1.143) | 0.452 | ||
| AST (U/L) | >40 vs. ≤40 | 1.417 (0.965–2.080) | 0.075 | ||
| ALT (U/L) | >40 vs. ≤40 | 1.197 (0.825–1.736) | 0.343 | ||
| Platelets (109/L) | <150 vs. ≥150 | 2.096 (1.448–3.033) | <0.001 | ||
| AFP (ng/mL) | >200 vs. ≤200 | 1.003 (0.645–1.558) | 0.990 | ||
| Albumin (mg/dL) | Per 1 unit decrease | 1.536 (1.063–2.222) | 0.023 | ||
| Child–Pugh class | B vs. A | 3.332 (1.056–10.509) | 0.040 | ||
| ALBI grade | II/III vs. I | 1.286 (0.834–1.985) | 0.255 | ||
| Liver cirrhosis | Yes vs. No | 2.708 (1.823–4.023) | <0.001 | 4.273 (1.934–9.439) | <0.001 |
| BCLC stage | A vs. 0 | 2.460 (1.384–4.373) | 0.002 | ||
| Tumor no. | Multiple vs. Single | 1.053 (0.638–1.738) | 0.840 | ||
| Tumor diameter (cm) | Per 1 cm increase | 1.458 (1.239–1.716) | <0.001 | 1.515 (1.309–1.945) | <0.001 |
| Histological grade | Poor/Moderate vs Well | 1.193 (0.739–1.926) | 0.471 | ||
| Microvascular invasion | Yes vs. No | 1.728 (1.204–2.479) | 0.003 | ||
| Capsule invasion | Yes vs. No | 1.362 (0.826–2.246) | 0.226 | ||
| Satellite nodules | Yes vs. No | 2.957 (1.442–6.062) | 0.003 | ||
| MAFLD | Yes vs. No | 0.743 (0.518–1.006) | 0.107 | ||
| Univariate | Multivariate | ||||
|---|---|---|---|---|---|
| Variable | Comparison | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Age(year) | Per one-year increase | 1.007 (0.991–1.023) | 0.402 | ||
| Sex | Male vs. Female | 1.253 (0.741–2.118) | 0.400 | ||
| DM | Yes vs. No | 1.274 (0.894–1.816) | 0.180 | ||
| Hypertension | Yes vs. No | 1.167 (0.829–1.642) | 0.377 | ||
| Alcohol drinking | Current vs. Never/Past | 0.981 (0.667–1.443) | 0.922 | ||
| Smoking | Current vs. Never/Past | 1.256 (0.888–1.777) | 0.197 | ||
| HCC family history | Yes vs. No | 1.382 (0.906–2.109) | 0. 134 | ||
| HBeAg | Positive vs. Negative | 1.103 (0.603–2.015) | 0.751 | ||
| HBV DNA (IU/mL) | Detectable vs. Undetectable | 1.376 (0.747–2.536) | 0.306 | ||
| NUCs treatment | Yes vs. No | 1.091 (0.903–1.846) | 0.662 | ||
| AST (U/L) | >40 vs. ≤40 | 1.522 (1.056–2.194) | 0.024 | ||
| ALT (U/L) | >40 vs. ≤40 | 1.269 (0.896–1.798) | 0.180 | ||
| Platelets (109/L) | <150 vs. ≥150 | 1.314 (0.914–1.890) | 0.140 | ||
| AFP (ng/mL) | >5 vs. ≤5 | 1.383 (0.954–2.004) | 0.087 | ||
| Albumin (mg/dL) | Per 1 unit decrease | 1.245 (0.862–1.799) | 0.242 | ||
| Child–Pugh class | B vs. A | 1.537 (0.214–11.031) | 0.669 | ||
| ALBI grade | II/III vs. I | 1.039 (0.650–1.662) | 0.873 | ||
| Liver cirrhosis | Yes vs. No | 2.168 (1.527–3.077) | <0.001 | 2.300 (1.572–3.366) | <0.001 |
| BCLC stage | A vs. 0 | 1.777 (1.134–2.786) | 0.012 | 2.005 (1.238–3.247) | 0.005 |
| Tumor no. | Multiple vs. Single | 1.524 (1.004–2.314) | 0.048 | ||
| Tumor diameter (cm) | Per 1 cm increase | 1.145 (0.964–1.361) | 0.123 | ||
| Histological grade | Poor/Moderate vs. Well | 1.134 (0.757–1.698) | 0.542 | ||
| Microvascular invasion | Yes vs. No | 1.185 (0.802–1.751) | 0.394 | ||
| Capsule invasion | Yes vs. No | 1.069 (0.696–1.641) | 0.760 | ||
| Satellite nodules | Yes vs. No | 4.481 (2.337–8.592) | <0.001 | 4.239 (2.044–8.794) | <0.001 |
| Lean-MAFLD | Yes vs. No | 1.834 (1.087–3.095) | 0.023 | 2.030 (1.117–3.690) | 0.020 |
| Lean-MAFLD (n = 28) | Non-Lean-MAFLD (n = 340) | p-Value | |
|---|---|---|---|
| Age (years), mean ± SD | 60.7 ± 9.2 | 55.8 ± 10.2 | 0.015 |
| Male gender, n (%) | 21 (75) | 299 (87.9) | 0.051 |
| Body mass index (kg/m2), mean ± SD | 21.4 ± 1.4 | 27.1 ± 3.0 | <0.001 |
| DM, n (%) | 19 (67.9) | 98 (28.8) | <0.001 |
| Hypertension, n (%) | 14 (50) | 135 (39.7) | 0.286 |
| Family history of HCC, n (%) | 4 (14.3) | 52 (15.3) | 0.886 |
| Platelets (<150 109/L), n (%) | 9 (33.3) | 104 (31.2) | 0.821 |
| AST (U/L), mean ± SD | 32.3 ± 15.0 | 38.2 ± 20.9 | 0.153 |
| ALT (U/L), mean ± SD | 33.2 ± 15.7 | 48.1 ± 38.9 | 0.048 |
| Total bilirubin (mg/dL), mean ± SD | 0.8 ± 0.4 | 0.7 ± 0.4 | 0.484 |
| Albumin (g/dL), mean ± SD | 4.1 ± 0.6 | 4.3 ± 0.4 | 0.162 |
| Creatinine (mg/dL), mean ± SD | 1.1 ± 4.1 | 1.1 ± 1.3 | 0.653 |
| eGFR (ml/min/1.732), mean ± SD | 94.2 ± 21.8 | 91.9 ± 26.4 | 0.185 |
| AFP (>20 ng/mL), n (%) | 9 (33.3) | 128 (38.3) | 0.607 |
| Child–Pugh grade (A/B), n (%) | 28/0 (100/0) | 325/3 (99.1/0.9) | 0.618 |
| ALBI grade (I/II/III), n (%) | 19/8/0 (70.4/29.6/0) | 278/47/2 (85/14.4/0.6) | 0.103 |
| Liver cirrhosis, n (%) | 10 (35.7) | 171 (50.3) | 0.138 |
| BCLC stage 0/A, n (%) | 5/23 (17.9/82.1) | 87/253 (25.6/74.4) | 0.364 |
| Tumor diameter (cm), mean ± SD | 2.6 ± 1.0 | 2.7 ± 1.1 | 0.768 |
| Multiple tumors, n (%) | 3 (10.7) | 46 (13.5) | 0.673 |
| Histological grade | 0.529 | ||
| Well differentiated, n (%) | 5 (18.5) | 8 (23.6) | |
| Moderately differentiated, n (%) | 13 (48.1) | 178 (52.5) | |
| Poorly differentiated, n (%) | 9 (33.3) | 81 (23.9) | |
| Microvascular invasion, n (%) | 5 (17.9) | 85 (25.1) | 0.394 |
| Capsule invasion, n (%) | 24 (85.7) | 271 (79.9) | 0.460 |
| Satellite nodule, n (%) | 13 (3.6) | 11 (2.5) | 0.376 |
| Follow-up (months), mean ± SD | 65.3 ± 30.4 | 67.2 ± 32.7 | 0.764 |
| Recurrence, n (%) | 16 (57.1) | 119 (35.0) | 0.019 |
| Death or liver transplantation, n (%) | 3 (10.7) | 46 (13.5) | 0.673 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-P.; Lin, S.-H.; Wang, C.-C.; Lin, C.-C.; Chen, D.-W.; Chuang, C.-H.; Huang, P.-Y.; Hung, C.-H.; Yang, S.-Y.; Cho, W.-R.; et al. Impact of MAFLD on HBV-Related Stage 0/A Hepatocellular Carcinoma after Curative Resection. J. Pers. Med. 2021, 11, 684. https://doi.org/10.3390/jpm11080684
Lin Y-P, Lin S-H, Wang C-C, Lin C-C, Chen D-W, Chuang C-H, Huang P-Y, Hung C-H, Yang S-Y, Cho W-R, et al. Impact of MAFLD on HBV-Related Stage 0/A Hepatocellular Carcinoma after Curative Resection. Journal of Personalized Medicine. 2021; 11(8):684. https://doi.org/10.3390/jpm11080684
Chicago/Turabian StyleLin, Yen-Po, Shu-Hsien Lin, Chih-Chi Wang, Chih-Che Lin, Ding-Wei Chen, Ching-Hui Chuang, Pao-Yuan Huang, Chao-Hung Hung, Shih-Yu Yang, Wei-Ru Cho, and et al. 2021. "Impact of MAFLD on HBV-Related Stage 0/A Hepatocellular Carcinoma after Curative Resection" Journal of Personalized Medicine 11, no. 8: 684. https://doi.org/10.3390/jpm11080684