Association of Sepsis Mortality with Specific Cancer Sites and Treatment Type: The Multiethnic Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Case Ascertainment
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics and Mortality Summary
3.2. Association of Sepsis Mortality with Baseline Factors
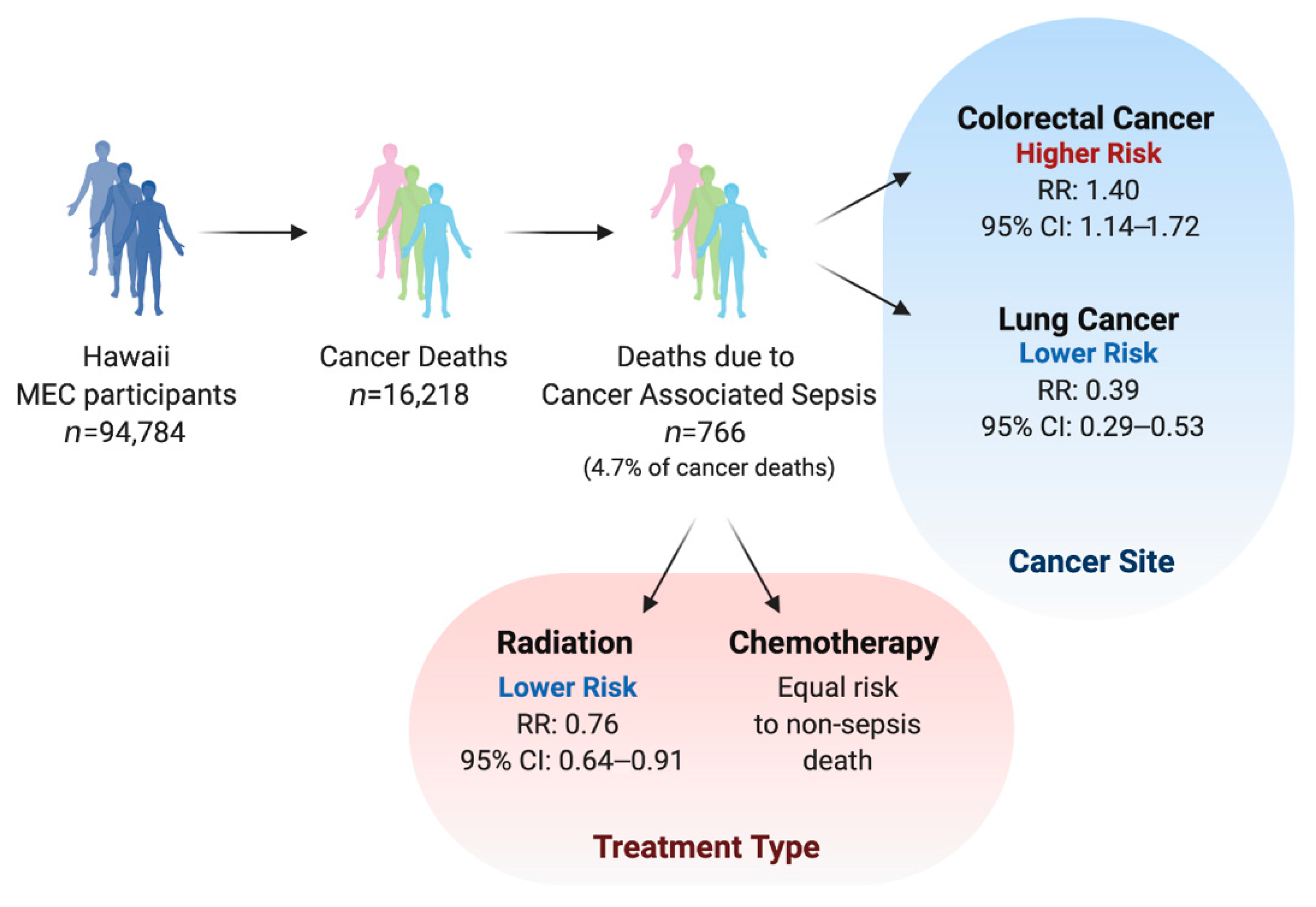
3.3. Association of Sepsis Mortality with Cancer Sites
3.4. Association of Sepsis Mortality with Cancer Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.L.; Slutsky, A.S. Sepsis and Endothelial Permeability. N. Engl. J. Med. 2010, 363, 689–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann, M.C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Mayr, F.B.; Yende, S.; Angus, D.C. Epidemiology of severe sepsis. Virulence 2014, 5, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagher, G.A.; El Khuri, C.; Chehadeh, A.A.-H.; Chami, A.; Bachir, R.; Zebian, D.; Chebl, R.B. Are patients with cancer with sepsis and bacteraemia at a higher risk of mortality? A retrospective chart review of patients presenting to a tertiary care centre in Lebanon. BMJ Open 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Williams, M.D.; Braun, L.A.; Cooper, L.M.; Johnston, J.; Weiss, R.V.; Qualy, R.L.; Linde-Zwirble, W. Hospitalized cancer patients with severe sepsis: Analysis of incidence, mortality, and associated costs of care. Crit. Care 2004, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef]
- Danai, P.A.; Moss, M.; Mannino, D.M.; Martin, G.S. The Epidemiology of Sepsis in Patients With Malignancy. Chest 2006, 129, 1432–1440. [Google Scholar] [CrossRef]
- Melamed, A.; Sorvillo, F.J. The burden of sepsis-associated mortality in the United States from 1999 to 2005: An analysis of multiple-cause-of-death data. Crit. Care 2009, 13, R28. [Google Scholar] [CrossRef] [Green Version]
- Matter, M.L.; Shvetsov, Y.B.; Dugay, C.; Haiman, C.A.; Le Marchand, L.; Wilkens, L.R.; Maskarinec, G. High mortality due to sepsis in Native Hawaiians and African Americans: The Multiethnic Cohort. PLoS ONE 2017, 12, 4–11. [Google Scholar] [CrossRef]
- Kolonel, L.N.; Henderson, B.E.; Hankin, J.H.; Nomura, A.M.; Wilkens, L.R.; Pike, M.C.; Stram, D.O.; Monroe, K.R.; Earle, M.E.; Nagamine, F.S. A Multiethnic Cohort in Hawaii and Los Angeles: Baseline Characteristics. Am. J. Epidemiol. 2000, 151, 346–357. [Google Scholar] [CrossRef]
- World Health Organization (WHO). International Statistical Classification of Diseases and Related Health Problems. Available online: http://apps.who.int/classifications/icd10/browse/2010/en (accessed on 20 December 2020).
- Centers for Disease Control and Prevention (CDC). International Classification of Diseases, 9th Revision. Available online: ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Publications/ICD9-CM/2009/ (accessed on 20 December 2020).
- Lunn, M.; McNeil, D. Applying Cox Regression to Competing Risks. Biometrics 1995, 51, 524–532. [Google Scholar] [CrossRef]
- Wang, M.; Spiegelman, D.; Kuchiba, A.; Lochhead, P.; Kim, S.; Chan, A.T.; Poole, E.M.; Tamimi, R.M.; Tworoger, S.S.; Giovannucci, E.; et al. Statistical methods for studying disease subtype heterogeneity. Stat. Med. 2016, 35, 782–800. [Google Scholar] [CrossRef]
- Grambsch, P.M.; Therneau, T.M. Proportional Hazards Tests and Diagnostics Based on Weighted Residuals. Biometrika 1994, 81, 515–526. [Google Scholar] [CrossRef]
- Angus, D.C.; Van Der Poll, T. Severe Sepsis and Septic Shock. N. Engl. J. Med. 2013, 369, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Mahale, P.; Engels, E. Sepsis and Risk of Cancer Among Elderly Adults in the United States. Clin. Infect. Dis. 2019, 68, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Mayr, F.B.; Yende, S.; Linde-Zwirble, W.T.; Peck-Palmer, O.M.; Barnato, A.E.; Weissfeld, L.A.; Angus, D.C. Infection Rate and Acute Organ Dysfunction Risk as Explanations for Racial Differences in Severe Sepsis. JAMA 2010, 303, 2495–2503. [Google Scholar] [CrossRef]
- Sullivan, A.; Edlund, C.; Nord, C.E. Effect of antimicrobial agents on the ecological balance of human microflora. Lancet Infect. Dis. 2001, 1, 101–114. [Google Scholar] [CrossRef]
- Dalhoff, A.; Shalit, I. Immunomodulatory effects of quinolones. Lancet Infect. Dis. 2003, 3, 359–371. [Google Scholar] [CrossRef]
- Rashid, M.-U.; Weintraub, A.; Nord, C.E. Effect of new antimicrobial agents on the ecological balance of human microflora. Anaerobe 2012, 18, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C.; Wax, R.S. Epidemiology of sepsis: An update. Crit. Care Med. 2001, 29, S109–S116. [Google Scholar] [CrossRef] [PubMed]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of clinical criteria for sepsis for the third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Kempker, J.A.; Martin, G.S. The Changing Epidemiology and Definitions of Sepsis. Clin. Chest Med. 2016, 37, 165–179. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Men | Women | |
|---|---|---|
| Baseline characteristics | N = 45,314 | N = 49,470 |
| Age at cohort entry (years) a | 59.3 ± 9.2 | 59.0 ± 9.1 |
| Mean follow-up (person-years) a | 18.0 ± 5.8 | 19.3 ± 4.7 |
| Total follow-up (person-years) | 814,432 | 954,829 |
| Race/ethnicity (%) | ||
| Native Hawaiian | 13.0 | 14.8 |
| Japanese American | 43.2 | 43.5 |
| White | 35.1 | 30.6 |
| Other | 8.7 | 11.1 |
| Body mass index (kg/m2, %) b | ||
| < 22 | 11.3 | 29.0 |
| 22– < 25 | 29.1 | 28.1 |
| 25– < 30 | 43.6 | 27.1 |
| ≥30 | 15.8 | 14.6 |
| Education completed (%) b | ||
| high school or less | 10.0 | 10.6 |
| some college | 54.2 | 58.4 |
| college or higher | 35.1 | 30.1 |
| Smoking status (%) b | ||
| Never smoker | 30.6 | 56.8 |
| Past smoker | 50.5 | 27.7 |
| Current smoker | 17.1 | 13.9 |
| Pack-years of cigarette smoking a,c | 17.7 ± 15.6 | 13.9 ± 13.6 |
| History of diabetes (%) | 10.3 | 8.7 |
| History of heart attack (%) | 9.3 | 4.2 |
| History of high blood pressure (%) | 38.8 | 33.1 |
| History of stroke (%) | 2.9 | 1.8 |
| Physical activity >2.5 h/wk (%) | 11.3 | 8.0 |
| Alcohol intake (g/day) a | 15.5 ± 31.4 | 4.5 ± 14.9 |
| Any-Cause Deaths | Cancer Deaths 1,2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | N | Sepsis as | Sepsis as | Percent | N | N | Sepsis | Sepsis as | Percent | |
| Sex/Ethnicity | Participants | Deaths | Primary | Contributing | Sepsis-Rel. | Cancer Cases | Deaths | as Primary | Contributing | Sepsis-Rel. |
| All participants | 103,898 | 37,386 | 462 | 1356 | 4.86 | 29,255 | 16,218 | 147 | 619 | 4.72 |
| Men | 48,937 | 20,722 | 264 | 727 | 4.78 | 14,992 | 9194 | 81 | 347 | 4.66 |
| Native Hawaiian | 6228 | 2835 | 49 | 116 | 5.82 | 1882 | 1207 | 15 | 54 | 5.72 |
| Japanese American | 20,871 | 8922 | 108 | 350 | 5.13 | 6719 | 4174 | 35 | 166 | 4.82 |
| White | 17,733 | 7446 | 80 | 189 | 3.61 | 5329 | 3224 | 25 | 96 | 3.75 |
| Other | 4105 | 1519 | 27 | 72 | 6.52 | 1062 | 589 | 6 | 31 | 6.28 |
| Women | 54,961 | 16,664 | 198 | 629 | 4.96 | 14263 | 7024 | 66 | 272 | 4.81 |
| Native Hawaiian | 8118 | 2875 | 40 | 153 | 6.71 | 2401 | 1283 | 14 | 62 | 5.92 |
| Japanese American | 23,642 | 6832 | 79 | 269 | 5.09 | 6164 | 2890 | 29 | 115 | 4.98 |
| White | 17,310 | 5518 | 59 | 148 | 3.75 | 4359 | 2221 | 18 | 65 | 3.74 |
| Other | 5891 | 1439 | 20 | 59 | 5.49 | 1339 | 630 | 5 | 30 | 5.56 |
| Men and Women | Men | Women | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sepsis | Other-Cause | Relative Risk Ratio | Sepsis | Other-Cause | Relative Risk Ratio | Sepsis | Other-Cause | Relative Risk Ratio | ||||||||
| Characteristic/Level | HR | HR | HR | LCL | UCL | HR | HR | HR | LCL | UCL | HR | HR | HR | LCL | UCL | |
| BMI | ||||||||||||||||
| <22 | 1.20 | 1.24 | 1.55 | 1.30 | 0.99 | 1.21 | ||||||||||
| 22–24.9 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| 25–29.9 | 1.04 | 1.01 | 1.11 | 1.00 | 0.93 | 1.03 | ||||||||||
| 30 or higher | 1.93 | 1.30 | 1.48 | 1.03 | 2.11 | 1.87 | 1.32 | 1.87 | 1.15 | 3.04 | 1.94 | 1.23 | 1.17 | 0.69 | 2.01 | |
| Education | ||||||||||||||||
| High school or less | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Some college | 1.03 | 0.93 | 0.99 | 0.92 | 1.10 | 0.95 | ||||||||||
| College degree or higher | 0.70 | 0.77 | 1.01 | 0.76 | 1.35 | 0.70 | 0.75 | 1.01 | 0.69 | 1.48 | 0.73 | 0.82 | 1.04 | 0.67 | 1.60 | |
| Tobacco smoking | ||||||||||||||||
| Never smoker | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Past smoker | 1.11 | 1.29 | 1.13 | 1.31 | 1.09 | 1.29 | ||||||||||
| Current smoker | 2.21 | 2.42 | 0.79 | 0.63 | 0.99 | 2.36 | 2.43 | 0.84 | 0.60 | 1.17 | 2.00 | 2.40 | 0.71 | 0.51 | 0.98 | |
| Alcohol drinking (g/d) | ||||||||||||||||
| None | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| <14 | 0.71 | 0.86 | 0.72 | 0.86 | 0.69 | 0.86 | ||||||||||
| 14 or more | 0.91 | 0.93 | 0.81 | 0.65 | 1.01 | 0.94 | 0.94 | 0.84 | 0.63 | 1.12 | 0.77 | 0.87 | 0.70 | 0.47 | 1.05 | |
| Physical activity (AC mets/d) | ||||||||||||||||
| <2.5 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| ≥2.5 | 0.88 | 0.88 | 1.01 | 0.86 | 1.17 | 0.80 | 0.87 | 0.92 | 0.75 | 1.12 | 1.02 | 0.87 | 1.17 | 0.92 | 1.49 | |
| History of diabetes | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 2.11 | 1.86 | 1.14 | 0.99 | 1.30 | 2.04 | 1.76 | 1.16 | 0.97 | 1.39 | 2.17 | 2.01 | 1.08 | 0.88 | 1.31 | |
| History of heart disease | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 1.34 | 1.57 | 0.86 | 0.73 | 1.01 | 1.35 | 1.56 | 0.86 | 0.71 | 1.05 | 1.33 | 1.60 | 0.84 | 0.63 | 1.10 | |
| History of hypertension | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 1.31 | 1.26 | 1.05 | 0.94 | 1.16 | 1.20 | 1.25 | 0.96 | 0.83 | 1.11 | 1.45 | 1.24 | 1.17 | 1.00 | 1.38 | |
| History of stroke | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 1.59 | 1.64 | 0.97 | 0.76 | 1.23 | 1.40 | 1.57 | 0.89 | 0.65 | 1.22 | 1.97 | 1.80 | 1.09 | 0.76 | 1.57 | |
| Cancer at any site | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 3.39 | 3.51 | 1.01 | 0.91 | 1.12 | 3.26 | 3.38 | 1.00 | 0.87 | 1.15 | 3.55 | 3.73 | 0.99 | 0.85 | 1.16 | |
| Men and Women | Men | Women | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sepsis | Other-Cause | Relative Risk Ratio | Sepsis | Other-Cause | Relative Risk Ratio | Sepsis | Other-Cause | Relative Risk Ratio | ||||||||
| Characteristic/Level | HR | HR | HR | LCL | UCL | HR | HR | HR | LCL | UCL | HR | HR | HR | LCL | UCL | |
| BMI | ||||||||||||||||
| <22 | 0.98 | 1.16 | 1.02 | 1.19 | 0.99 | 1.14 | ||||||||||
| 22–24.9 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| 25–29.9 | 0.98 | 1.04 | 0.98 | 1.02 | 0.95 | 1.10 | ||||||||||
| 30 or higher | 1.43 | 1.22 | 0.93 | 0.52 | 1.65 | 1.28 | 1.26 | 0.85 | 0.39 | 1.83 | 1.62 | 1.17 | 1.04 | 0.42 | 2.57 | |
| Education | ||||||||||||||||
| High school or less | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Some college | 1.04 | 0.92 | 0.97 | 0.91 | 1.17 | 0.92 | ||||||||||
| College degree or higher | 0.70 | 0.77 | 1.02 | 0.62 | 1.69 | 0.70 | 0.76 | 0.98 | 0.51 | 1.87 | 0.71 | 0.80 | 1.14 | 0.51 | 2.56 | |
| Tobacco smoking | ||||||||||||||||
| Never smoker | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Past smoker | 0.91 | 1.35 | 1.06 | 1.42 | 0.75 | 1.27 | ||||||||||
| Current smoker | 1.63 | 2.33 | 0.48 | 0.33 | 0.69 | 1.98 | 2.43 | 0.61 | 0.35 | 1.05 | 1.33 | 2.29 | 0.34 | 0.19 | 0.61 | |
| Alcohol drinking (g/d) | ||||||||||||||||
| None | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| <14 | 0.83 | 0.94 | 0.88 | 0.95 | 0.79 | 0.94 | ||||||||||
| 14 or more | 1.04 | 0.98 | 0.94 | 0.66 | 1.35 | 1.08 | 1.00 | 1.00 | 0.62 | 1.60 | 0.83 | 0.90 | 0.77 | 0.40 | 1.48 | |
| Physical activity (AC mets/d) | ||||||||||||||||
| <2.5 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| ≥2.5 | 1.03 | 0.92 | 1.12 | 0.88 | 1.43 | 0.88 | 0.91 | 0.97 | 0.71 | 1.32 | 1.35 | 0.94 | 1.44 | 0.99 | 2.11 | |
| History of diabetes | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 1.58 | 1.41 | 1.12 | 0.87 | 1.43 | 1.70 | 1.41 | 1.21 | 0.88 | 1.67 | 1.37 | 1.40 | 0.98 | 0.66 | 1.46 | |
| History of heart disease | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 1.26 | 1.25 | 1.00 | 0.75 | 1.35 | 1.35 | 1.30 | 1.03 | 0.73 | 1.46 | 1.03 | 1.15 | 0.90 | 0.51 | 1.58 | |
| History of hypertension | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 0.99 | 1.11 | 0.89 | 0.75 | 1.07 | 0.85 | 1.11 | 0.77 | 0.61 | 0.97 | 1.22 | 1.11 | 1.10 | 0.84 | 1.46 | |
| History of stroke | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 1.40 | 1.36 | 1.03 | 0.64 | 1.66 | 1.49 | 1.23 | 1.21 | 0.70 | 2.10 | 1.14 | 1.77 | 0.64 | 0.23 | 1.77 | |
| Colorectal cancer | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 1.06 | 0.79 | 1.40 | 1.14 | 1.72 | 1.07 | 0.76 | 1.43 | 1.10 | 1.86 | 1.00 | 0.81 | 1.33 | 0.95 | 1.87 | |
| Lung cancer | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 1.22 | 3.00 | 0.39 | 0.29 | 0.53 | 1.42 | 3.08 | 0.44 | 0.31 | 0.63 | 0.86 | 2.87 | 0.27 | 0.15 | 0.48 | |
| Skin cancer | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 0.59 | 0.80 | 0.68 | 0.39 | 1.16 | 0.50 | 0.80 | 0.64 | 0.33 | 1.26 | 0.76 | 0.79 | 0.77 | 0.31 | 1.90 | |
| Breast cancer | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 0.54 | 0.60 | 0.89 | 0.70 | 1.13 | N/A | N/A | 0.55 | 0.61 | 0.90 | 0.69 | 1.17 | ||||
| Prostate cancer | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 0.55 | 0.54 | 1.00 | 0.80 | 1.25 | 0.52 | 0.52 | 0.97 | 0.76 | 1.22 | N/A | N/A | ||||
| Chemotherapy | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 1.31 | 1.21 | 1.12 | 0.94 | 1.32 | 1.52 | 1.39 | 1.12 | 0.89 | 1.42 | 1.12 | 1.03 | 1.14 | 0.89 | 1.47 | |
| Radiation | ||||||||||||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||||||||||||
| Yes | 0.90 | 1.16 | 0.76 | 0.64 | 0.91 | 0.95 | 1.20 | 0.81 | 0.65 | 1.01 | 0.82 | 1.12 | 0.70 | 0.53 | 0.92 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shvetsov, Y.B.; Ogino, M.H.; Glibetic, N.; Asato, C.B.; Wilkens, L.R.; Le Marchand, L.; Matter, M.L. Association of Sepsis Mortality with Specific Cancer Sites and Treatment Type: The Multiethnic Cohort Study. J. Pers. Med. 2021, 11, 146. https://doi.org/10.3390/jpm11020146
Shvetsov YB, Ogino MH, Glibetic N, Asato CB, Wilkens LR, Le Marchand L, Matter ML. Association of Sepsis Mortality with Specific Cancer Sites and Treatment Type: The Multiethnic Cohort Study. Journal of Personalized Medicine. 2021; 11(2):146. https://doi.org/10.3390/jpm11020146
Chicago/Turabian StyleShvetsov, Yurii B., Mari H. Ogino, Natalija Glibetic, Chloe B. Asato, Lynne R. Wilkens, Loïc Le Marchand, and Michelle L. Matter. 2021. "Association of Sepsis Mortality with Specific Cancer Sites and Treatment Type: The Multiethnic Cohort Study" Journal of Personalized Medicine 11, no. 2: 146. https://doi.org/10.3390/jpm11020146