
Acceptability of a Patient Portal (Opal) in HIV Clinical Care: A Feasibility Study

 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Sites
2.3. Study Design and Participant Eligibility
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Smart Device Ownership and Experience and Comfort Using Healthcare Applications
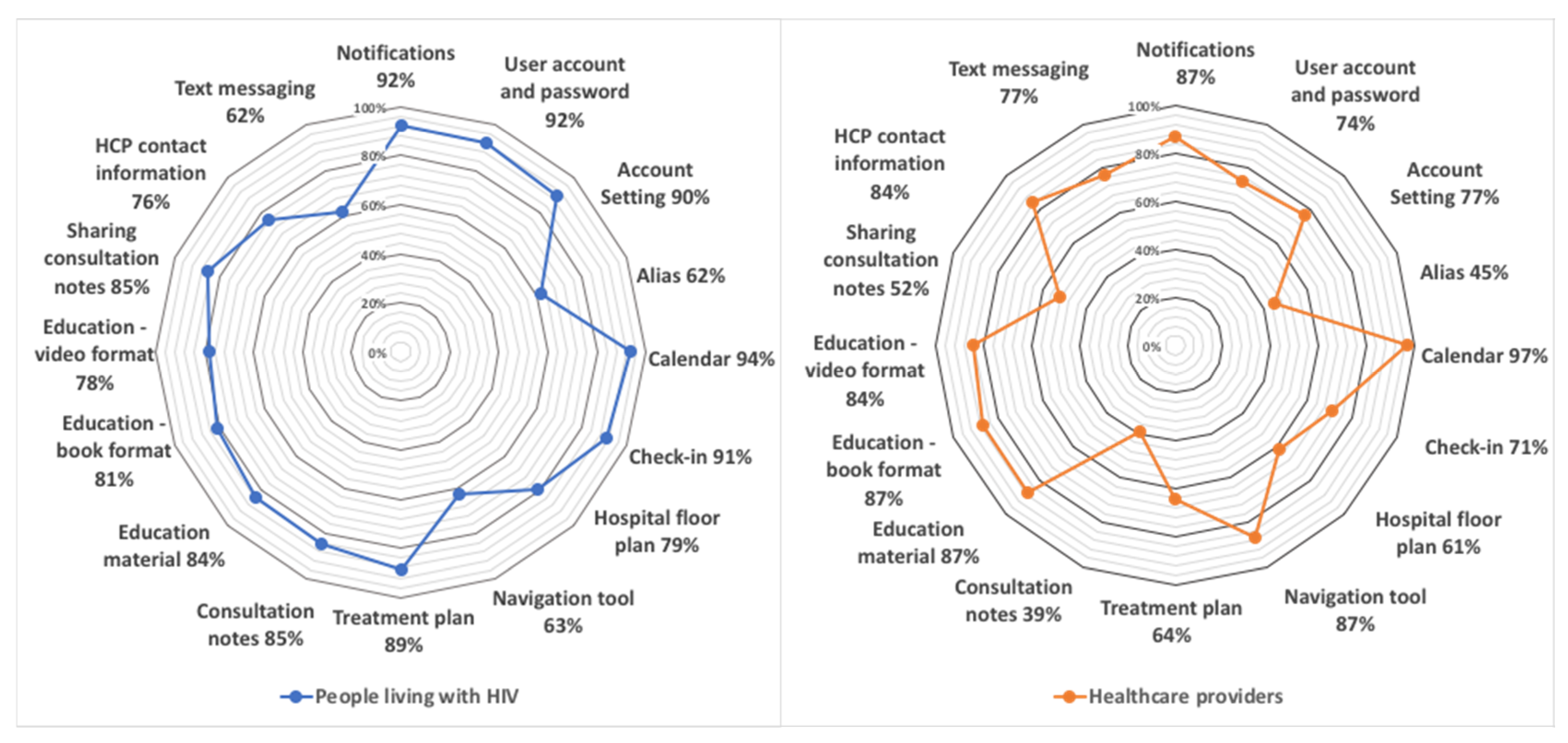
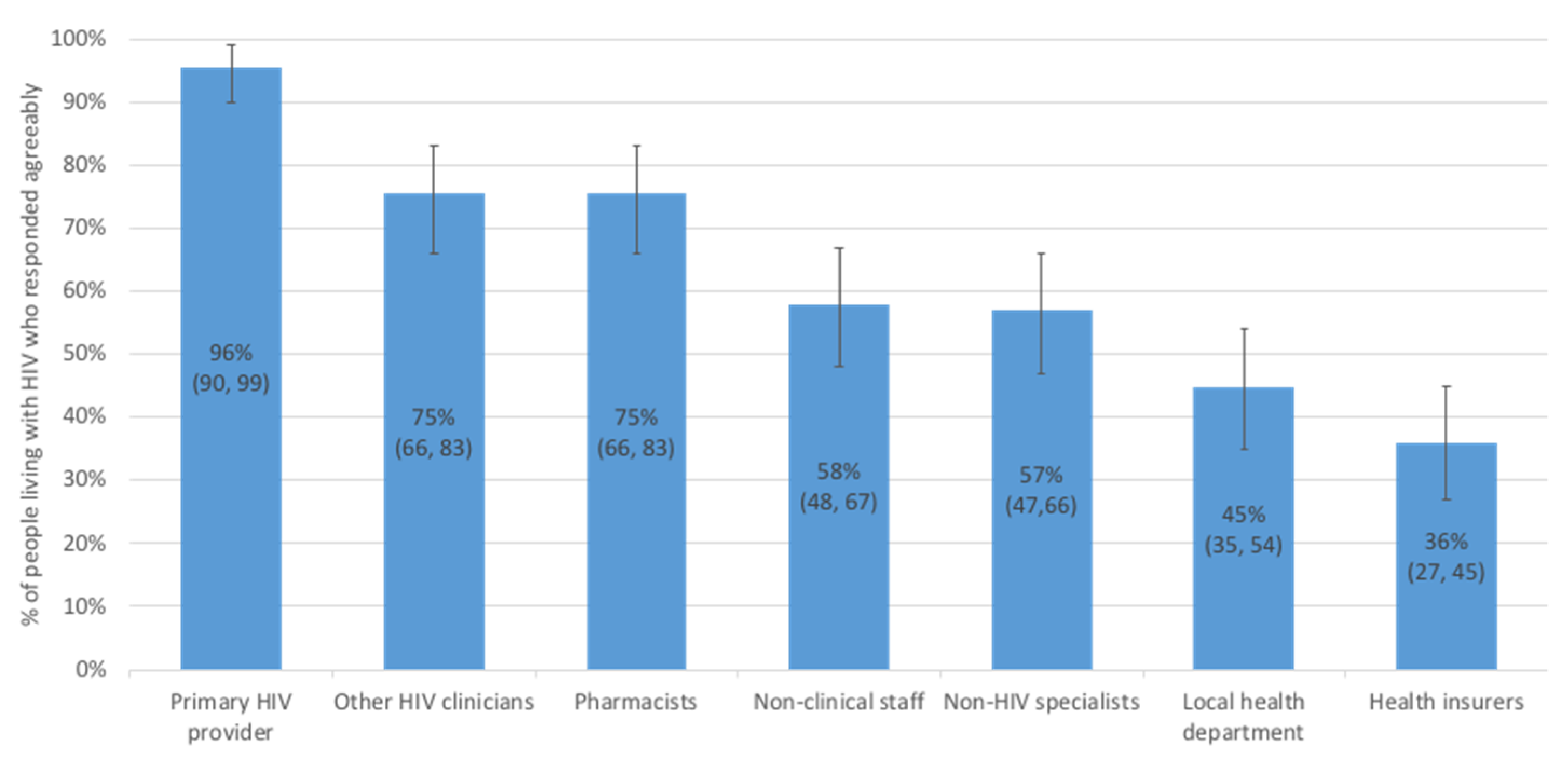
3.3. Interest in Opal Functions and Preferences for Sharing Personal Health Information
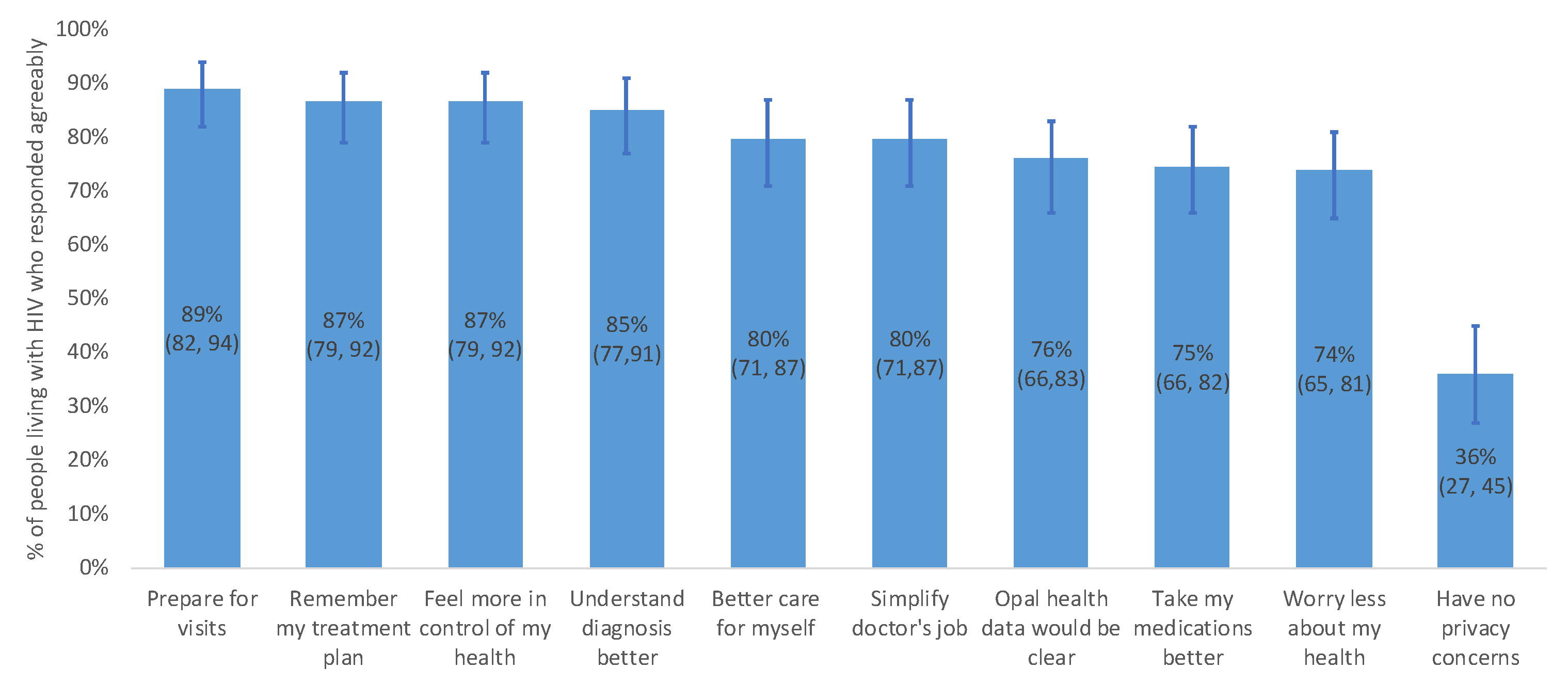
3.4. Anticipated Benefits and Inconveniences of Opal
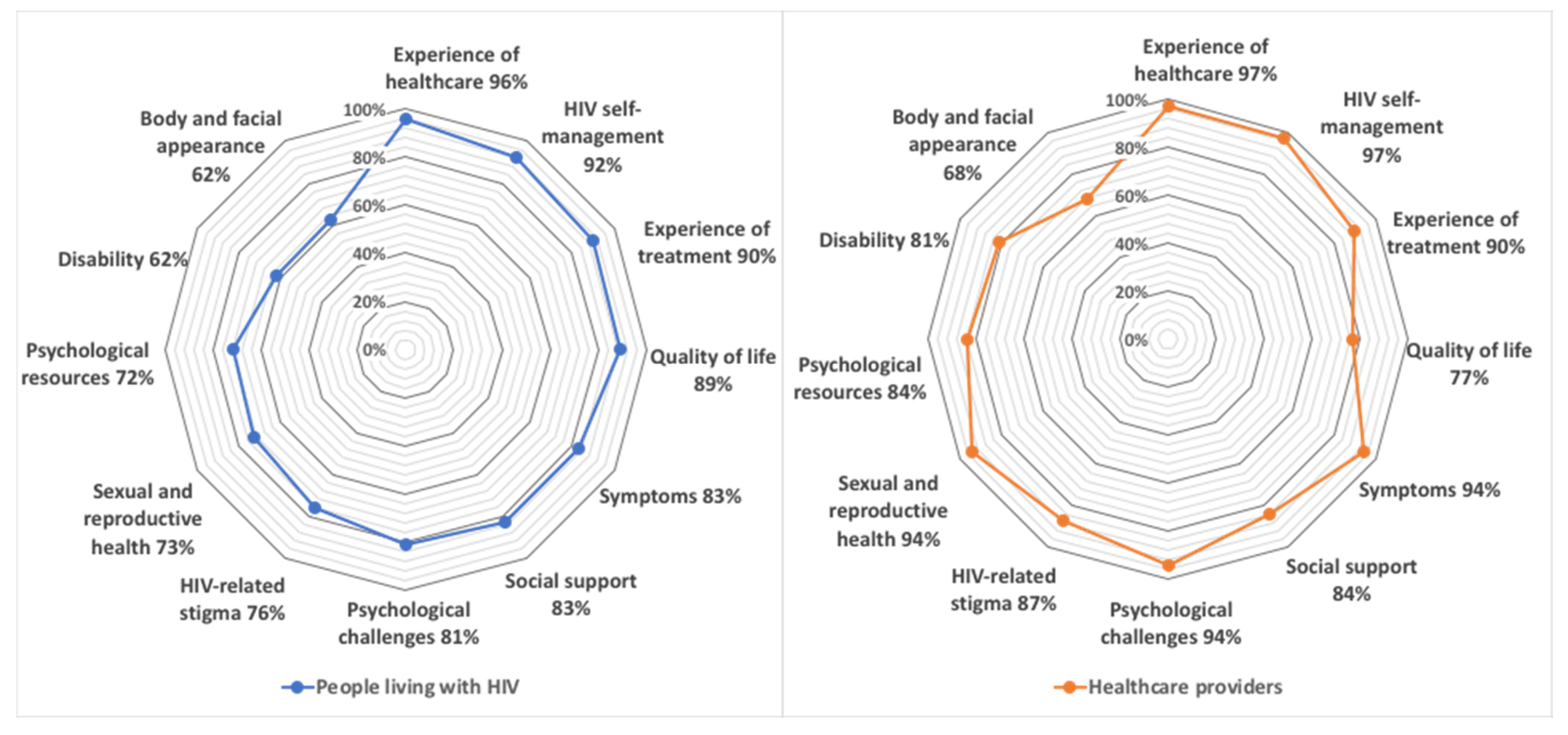
3.5. Interest in Different Patient-Reported Outcome Measures
4. Discussion
4.1. Smart Device Ownership, Experience with Healthcare Applications, and Health Info Preferences
4.2. Interest in Opal’s Functions
4.3. Anticipated Benefits and Inconveniences of Opal
4.4. Interest in Different Types of PROMs
4.5. Limitations
4.6. Future Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goodman, R.A.; Posner, S.F.; Huang, E.S.; Parekh, A.K.; Koh, H.K. Defining and measuring chronic conditions: Imperatives for research, policy, program, and practice. Prev. Chronic Dis. 2013, 10, E66. [Google Scholar] [CrossRef] [Green Version]
- Lowther, K.; Selman, L.; Harding, R.; Higginson, I.J. Experience of persistent psychological symptoms and perceived stigma among people with HIV on antiretroviral therapy (ART): A systematic review. Int. J. Nurs. Stud. 2014, 51, 1171–1189. [Google Scholar] [CrossRef] [PubMed]
- Engler, K.; Lenart, A.; Lessard, D.; Toupin, I.; Lebouche, B. Barriers to antiretroviral therapy adherence in developed countries: A qualitative synthesis to develop a conceptual framework for a new patient-reported outcome measure. AIDS Care 2018, 30, 17–28. [Google Scholar] [CrossRef]
- Mills, E.J.; Nachega, J.B.; Buchan, I.; Orbinski, J.; Attaran, A.; Singh, S.; Rachlis, B.; Wu, P.; Cooper, C.; Thabane, L.; et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: A meta-analysis. JAMA 2006, 296, 679–690. [Google Scholar] [CrossRef]
- Lessard, D.; Toupin, I.; Engler, K.; Lenart, A.; Team, I.S.C.; Lebouche, B. HIV-Positive Patients’ Perceptions of Antiretroviral Therapy Adherence in Relation to Subjective Time: Imprinting, Domino Effects, and Future Shadowing. J. Int. Assoc. Provid. AIDS Care 2018, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kildea, J.; Battista, J.; Cabral, B.; Hendren, L.; Herrera, D.; Hijal, T.; Joseph, A. Design and Development of a Person-Centered Patient Portal Using Participatory Stakeholder Co-Design. J. Med. Internet Res. 2019, 21, e11371. [Google Scholar] [CrossRef]
- Williams, E.C.; Achtmeyer, C.E.; Thomas, R.M.; Grossbard, J.R.; Lapham, G.T.; Chavez, L.J.; Ludman, E.J.; Berger, D.; Bradley, K.A. Factors Underlying Quality Problems with Alcohol Screening Prompted by a Clinical Reminder in Primary Care: A Multi-site Qualitative Study. J. Gen. Intern Med. 2015, 30, 1125–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, M.; Jackson, R.; Guillaume, L.; Meier, P.; Goyder, E. Barriers and facilitators to implementing screening and brief intervention for alcohol misuse: A systematic review of qualitative evidence. J. Public Health 2010, 33, 412–421. [Google Scholar] [CrossRef] [Green Version]
- Oster, N.V.; Jackson, S.L.; Dhanireddy, S.; Mejilla, R.; Ralston, J.D.; Leveille, S.; Delbanco, T.; Walker, J.D.; Bell, S.K.; Elmore, J.G. Patient Access to Online Visit Notes: Perceptions of Doctors and Patients at an Urban HIV/AIDS Clinic. J. Int. Assoc. Provid. AIDS Care 2015, 14, 306–312. [Google Scholar] [CrossRef] [Green Version]
- Fredericksen, R.; Crane, P.K.; Tufano, J.; Ralston, J.; Schmidt, S.; Brown, T.; Layman, D.; Harrington, R.D.; Dhanireddy, S.; Stone, T.; et al. Integrating a web-based, patient-administered assessment into primary care for HIV-infected adults. J. AIDS HIV Res. 2012, 4, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammenwerth, E.; Schnell-Inderst, P.; Hoerbst, A. The impact of electronic patient portals on patient care: A systematic review of controlled trials. J. Med. Internet Res. 2012, 14, e162. [Google Scholar] [CrossRef] [PubMed]
- Ryan, B.L.; Brown, J.B.; Terry, A.; Cejic, S.; Stewart, M.; Thind, A. Implementing and Using a Patient Portal: A qualitative exploration of patient and provider perspectives on engaging patients. J. Innov. Health Inform. 2016, 23, 848. [Google Scholar] [CrossRef] [PubMed]
- Irizarry, T.; DeVito Dabbs, A.; Curran, C.R. Patient Portals and Patient Engagement: A State of the Science Review. J. Med. Internet Res. 2015, 17, e148. [Google Scholar] [CrossRef] [Green Version]
- Kruse, C.S.; Bolton, K.; Freriks, G. The effect of patient portals on quality outcomes and its implications to meaningful use: A systematic review. J. Med. Internet Res. 2015, 17, e44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.T.; Wittevrongel, L.; Moore, L.; Beaty, B.L.; Ross, S.E. An Internet-based patient-provider communication system: Randomized controlled trial. J. Med. Internet Res. 2005, 7, e47. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.Y.; Garrido, T.; Chin, H.L.; Wiesenthal, A.M.; Liang, L.L. Patient access to an electronic health record with secure messaging: Impact on primary care utilization. Am. J. Manag. Care 2007, 13, 418–424. [Google Scholar]
- Osborn, C.Y.; Mayberry, L.S.; Wallston, K.A.; Johnson, K.B.; Elasy, T.A. Understanding patient portal use: Implications for medication management. J. Med. Internet Res. 2013, 15, e133. [Google Scholar] [CrossRef]
- Baudendistel, I.; Winkler, E.; Kamradt, M.; Langst, G.; Eckrich, F.; Heinze, O.; Bergh, B.; Szecsenyi, J.; Ose, D. Personal electronic health records: Understanding user requirements and needs in chronic cancer care. J. Med. Internet Res. 2015, 17, e121. [Google Scholar] [CrossRef]
- Deshpande, P.R.; Rajan, S.; Sudeepthi, B.L.; Abdul Nazir, C.P. Patient-reported outcomes: A new era in clinical research. Perspect. Clin. Res. 2011, 2, 137–144. [Google Scholar] [CrossRef]
- Boyce, M.B.; Browne, J.P. Does providing feedback on patient-reported outcomes to healthcare professionals result in better outcomes for patients? A systematic review. Qual. Life Res. 2013, 22, 2265–2278. [Google Scholar] [CrossRef]
- Bristowe, K.; Clift, P.; James, R.; Josh, J.; Platt, M.; Whetham, J.; Nixon, E.; Post, F.A.; McQuillan, K.; Ni Cheallaigh, C.; et al. Towards person-centred care for people living with HIV: What core outcomes matter, and how might we assess them? A cross-national multi-centre qualitative study with key stakeholders. HIV Med. 2019, 20, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Edelman, E.J.; Gordon, K.; Justice, A.C. Patient and provider-reported symptoms in the post-cART era. AIDS Behav. 2011, 15, 853–861. [Google Scholar] [CrossRef] [Green Version]
- CBC News. ’She’s Still Living, in Some Sense’: Woman’s App for Patients Wins Award, Days after Her Death. Available online: https://www.cbc.ca/news/canada/montreal/opal-app-cancer-patients-laurie-hendren-1.5161267 (accessed on 4 June 2019).
- van Limburg, M.; Wentzel, J.; Sanderman, R.; van Gemert-Pijnen, L. Business Modeling to Implement an eHealth Portal for Infection Control: A Reflection on Co-Creation with Stakeholders. JMIR Res. Protoc. 2015, 4, e104. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Hinder, S.; Stramer, K.; Bratan, T.; Russell, J. Adoption, non-adoption, and abandonment of a personal electronic health record: Case study of HealthSpace. BMJ 2010, 341, c5814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldridge, S.M.; Lancaster, G.A.; Campbell, M.J.; Thabane, L.; Hopewell, S.; Coleman, C.L.; Bond, C.M. Defining Feasibility and Pilot Studies in Preparation for Randomised Controlled Trials: Development of a Conceptual Framework. PLoS ONE 2016, 11, e0150205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiner, B.J.; Lewis, C.C.; Stanick, C.; Powell, B.J.; Dorsey, C.N.; Clary, A.S.; Boynton, M.H.; Halko, H. Psychometric assessment of three newly developed implementation outcome measures. Implement. Sci. 2017, 12, 108. [Google Scholar] [CrossRef]
- Engler, K.; Lessard, D.; Toupin, I.; Lènàrt, A.; Lebouché, B. Engaging Stakeholders into an Electronic Patient-Reported Outcome Development Study: On Making an HIV-Specific e-PRO Patient-Centered. Health Policy Technol. 2017, 6, 59–66. [Google Scholar] [CrossRef]
- République Française. Décret No. 2017-884 du 9 mai 2017 Modifiant Certaines Dispositions Réglementaires Relatives aux Recherches Impliquant la Personne Humaine Paris: LegiFrance. 2017. Available online: https://www.legifrance.gouv.fr/eli/decret/2017/5/9/2017-884/jo/texte (accessed on 28 January 2021).
- Engler, K.; Lessard, D.; Lebouche, B. A Review of HIV-Specific Patient-Reported Outcome Measures. Patient 2017, 10, 187–202. [Google Scholar] [CrossRef]
- Leveille, S.G.; Walker, J.; Ralston, J.D.; Ross, S.E.; Elmore, J.G.; Delbanco, T. Evaluating the impact of patients’ online access to doctors’ visit notes: Designing and executing the OpenNotes project. BMC Med. Inform. Decis. Mak. 2012, 12, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maiorana, A.; Steward, W.T.; Koester, K.A.; Pearson, C.; Shade, S.B.; Chakravarty, D.; Myers, J.J. Trust, confidentiality, and the acceptability of sharing HIV-related patient data: Lessons learned from a mixed methods study about Health Information Exchanges. Implement. Sci. 2012, 7, 34. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.S.; Ko, M.; Warren, J.; Carpenter, D. Healthcare Technology Self-Efficacy (HTSE) and its influence on individual attitude: An empirical study. Comput. Hum. Behav. 2016, 58, 12–24. [Google Scholar] [CrossRef]
- Moore, G.C.; Benbasat, I. Development of an instrument to measure the perceptions of adopting an information technology innovation. Inf. Syst. Res. 1991, 2, 192–222. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Foundation for Statistical Computing. R: A Language and Environment for Statistical Computing, 1.2; R Core Team: Vienna, Austria, 2020. [Google Scholar]
- Bate, P.; Robert, G. Experience-based design: From redesigning the system around the patient to co-designing services with the patient. Qual. Saf. Health Care 2006, 15, 307–310. [Google Scholar] [CrossRef] [Green Version]
- Ancker, J.S.; Osorio, S.N.; Cheriff, A.; Cole, C.L.; Silver, M.; Kaushal, R. Patient activation and use of an electronic patient portal. Inform. Health Soc. Care 2015, 40, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Gordon, N.P.; Hornbrook, M.C. Differences in Access to and Preferences for Using Patient Portals and Other eHealth Technologies Based on Race, Ethnicity, and Age: A Database and Survey Study of Seniors in a Large Health Plan. J. Med. Internet Res. 2016, 18, e50. [Google Scholar] [CrossRef] [PubMed]
- Latulipe, C.; Gatto, A.; Nguyen, H.T.; Miller, D.P.; Quandt, S.A.; Bertoni, A.G.; Smith, A.; Arcury, T.A. Design Considerations for Patient Portal Adoption by Low-Income, Older Adults. Proc. SIGCHI Conf. Hum. Factor Comput. Syst. 2015, 2015, 3859–3868. [Google Scholar] [CrossRef] [Green Version]
- Franklin, P.; Chenok, K.; Lavalee, D.; Love, R.; Paxton, L.; Segal, C.; Holve, E. Framework to Guide the Collection and Use of Patient-Reported Outcome Measures in the Learning Healthcare System. EGEMS 2017, 5, 17. [Google Scholar] [CrossRef]
- McInnes, D.K.; Solomon, J.L.; Bokhour, B.G.; Asch, S.M.; Ross, D.; Nazi, K.M.; Gifford, A.L. Use of electronic personal health record systems to encourage HIV screening: An exploratory study of patient and provider perspectives. BMC Res. Notes 2011, 4, 295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Garrido, T.; Chock, D.; Okawa, G.; Liang, L. The Kaiser Permanente Electronic Health Record: Transforming and streamlining modalities of care. Health Aff. (Millwood) 2009, 28, 323–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, R.; Bryce, C.L.; Paone, S.; Fischer, G.; McTigue, K.M.; Olshansky, E.; Zickmund, S.; Fitzgerald, K.; Siminerio, L. Exploring challenges and potentials of personal health records in diabetes self-management: Implementation and initial assessment. Telemed. J. E Health 2007, 13, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Lingg, M.; Lutschg, V. Health System Stakeholders’ Perspective on the Role of Mobile Health and Its Adoption in the Swiss Health System: Qualitative Study. JMIR Mhealth Uhealth 2020, 8, e17315. [Google Scholar] [CrossRef]
- Zettel-Watson, L.; Tsukerman, D. Adoption of online health management tools among healthy older adults: An exploratory study. Health Inform. J. 2016, 22, 171–183. [Google Scholar] [CrossRef]
- Lober, W.B.; Zierler, B.; Herbaugh, A.; Shinstrom, S.E.; Stolyar, A.; Kim, E.H.; Kim, Y. Barriers to the use of a personal health record by an elderly population. In AMIA Annual Symposium Proceedings; American Medical Informatics Association: Bethesda, MD, USA, 2006; p. 514. [Google Scholar]
- Schnipper, J.L.; Gandhi, T.K.; Wald, J.S.; Grant, R.W.; Poon, E.G.; Volk, L.A.; Businger, A.; Siteman, E.; Buckel, L.; Middleton, B. Design and implementation of a web-based patient portal linked to an electronic health record designed to improve medication safety: The Patient Gateway medications module. Inform. Prim. Care 2008, 16, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerai, P.; Wood, P.; Martin, M. A pilot study on the views of elderly regional Australians of personally controlled electronic health records. Int. J. Med. Inform. 2014, 83, 201–209. [Google Scholar] [CrossRef]
- Hourcade, J.P.; Chrischilles, E.A.; Gryzlak, B.M.; Hanson, B.M.; Dunbar, D.E.; Eichmann, D.A.; Lorentzen, R.R. Design Lessons for Older Adult Personal Health Records Software from Older Adults; Springer: Berlin/Heidelberg, Germany; pp. 176–185.
- Price, M.M.; Pak, R.; Müller, H.; Stronge, A. Older adults’ perceptions of usefulness of personal health records. Univers. Access Inf. Soc. 2013, 12, 191–204. [Google Scholar] [CrossRef]
- Rueda, S.; Mitra, S.; Chen, S.; Gogolishvili, D.; Globerman, J.; Chambers, L.; Wilson, M.; Logie, C.H.; Shi, Q.; Morassaei, S.; et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: A series of meta-analyses. BMJ Open 2016, 6, e011453. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| People Living with HIV (n = 114) Mean (SD) or % | Healthcare Providers (n = 31) Mean (SD) or % | |
|---|---|---|
| Age (years) | 47.8 (12.4) | 46.5 (11.4) |
| Range | 27, 74 | 25, 68 |
| Gender | ||
| Male | 74 | 32 |
| Female | 24 | 65 |
| Other/Transgender | 2 | 3 |
| Sexual orientation | ||
| Heterosexual | 48 | N/A |
| Men who have sex with men | 41 | |
| Bisexual | 9 | |
| Unsure or other | 2 | |
| Marital status | ||
| Single | 47 | N/A |
| Married | 38 | |
| Divorced or widow(er) | 15 | |
| Level of education | ||
| University or higher | 36 | N/A |
| CEGEP *, trade/vocational school, or high school | 53 | |
| Up to high school | 11 | |
| Paid work | ||
| Student | 8 | N/A |
| Part-time | 14 | |
| Full-time | 35 | |
| Unemployed, retired, or disabled | 43 | |
| Income (CAD) | ||
| 1 to 19 999 | 33 | N/A |
| 20 000 to 39 999 | 29 | |
| 40 000 to 59 999 | 15 | |
| >60 000 | 14 | |
| None or missing | 9 | |
| Ethnicity | ||
| Caucasian or White | 36 | N/A |
| Black, African, or Carribean | 31 | |
| Latino, Latin American, or South American | 20 | |
| North African or Middle Eastern | 6 | |
| Asian or Pacific Islander | <5 | |
| Indian or South Asian | <5 | |
| Other | <5 | |
| Aboriginal, First Nations, or Métis | --- | |
| Occupation | ||
| Physician | N/A | 42 |
| Pharmacist | 26 | |
| Nurse | 19 | |
| Social worker | 6 | |
| Administrative staff | 6 | |
| Smart devices owned | ||
| Smartphone | 90 | 87 |
| Computer (desktop or laptop) | 65 | 84 |
| Tablet | 39 | 29 |
| iPod or phablet | 8 | 19 |
| Smartwatch | <5 | 10 |
| Other | <5 | <5 |
| None | <5 | --- |
| People living with HIV (n = 114) % | Healthcare providers (n = 31) % | |
|---|---|---|
| Healthcare application experience | ||
| None to very little | 82 | 61 |
| Moderate to extensive | 18 | 35 |
| Willing to use a patient portal | ||
| Yes | 74 | 68 |
| No | 22 | 10 |
| Uncertain | 4 | 19 |
| Access to medical records | ||
| Immediate access | 61 | N/A |
| Following physician review | 25 | |
| No access | 10 | |
| Only need-to-know information | 4 | |
| Healthcare application self-efficacy | ||
| Capacity to use healthcare applications | 90 | 90 |
| Comfortable using healthcare applications | 77 | 81 |
| Ease of healthcare application use | 76 | 77 |
| Confidence pressing the right buttons to promote health | 73 | 84 |
| Acceptability of the proposed Opal patient portal | ||
| Opal is appealing | 90 | 97 |
| Opal has my approval | 89 | 87 |
| I would welcome Opal in HIV care | 89 | 81 |
| I like Opal | 76 | 81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, D.; Schuster, T.; Lessard, D.; Mate, K.; Engler, K.; Ma, Y.; Abulkhir, A.; Arora, A.; Long, S.; de Pokomandy, A.; et al. Acceptability of a Patient Portal (Opal) in HIV Clinical Care: A Feasibility Study. J. Pers. Med. 2021, 11, 134. https://doi.org/10.3390/jpm11020134
Chu D, Schuster T, Lessard D, Mate K, Engler K, Ma Y, Abulkhir A, Arora A, Long S, de Pokomandy A, et al. Acceptability of a Patient Portal (Opal) in HIV Clinical Care: A Feasibility Study. Journal of Personalized Medicine. 2021; 11(2):134. https://doi.org/10.3390/jpm11020134
Chicago/Turabian StyleChu, Dominic, Tibor Schuster, David Lessard, Kedar Mate, Kim Engler, Yuanchao Ma, Ayoub Abulkhir, Anish Arora, Stephanie Long, Alexandra de Pokomandy, and et al. 2021. "Acceptability of a Patient Portal (Opal) in HIV Clinical Care: A Feasibility Study" Journal of Personalized Medicine 11, no. 2: 134. https://doi.org/10.3390/jpm11020134