The Application of Deep Convolutional Neural Networks to Brain Cancer Images: A Survey

 , ,
, ,
Abstract
:1. Introduction
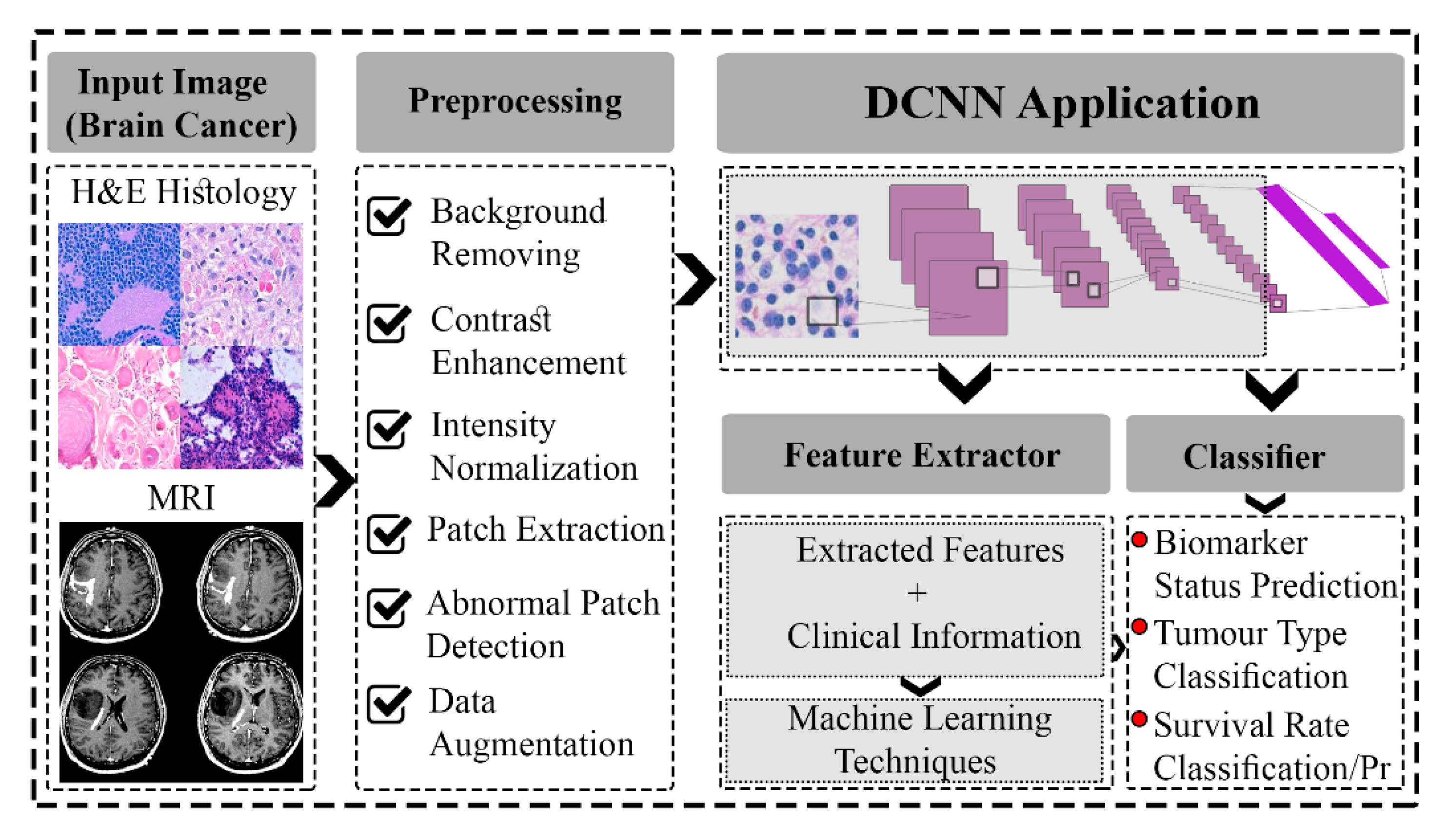
2. DCNNs Application in the Classification of Brain Cancer Images
2.1. DCNNs Application in the Classification of Brain Cancer H&E Histology Images
2.2. DCNNs Application in the Classification of Brain Cancer MR Images
2.3. DCNNs Application in the Classification of Brain Cancer H&E Histology and MR Images
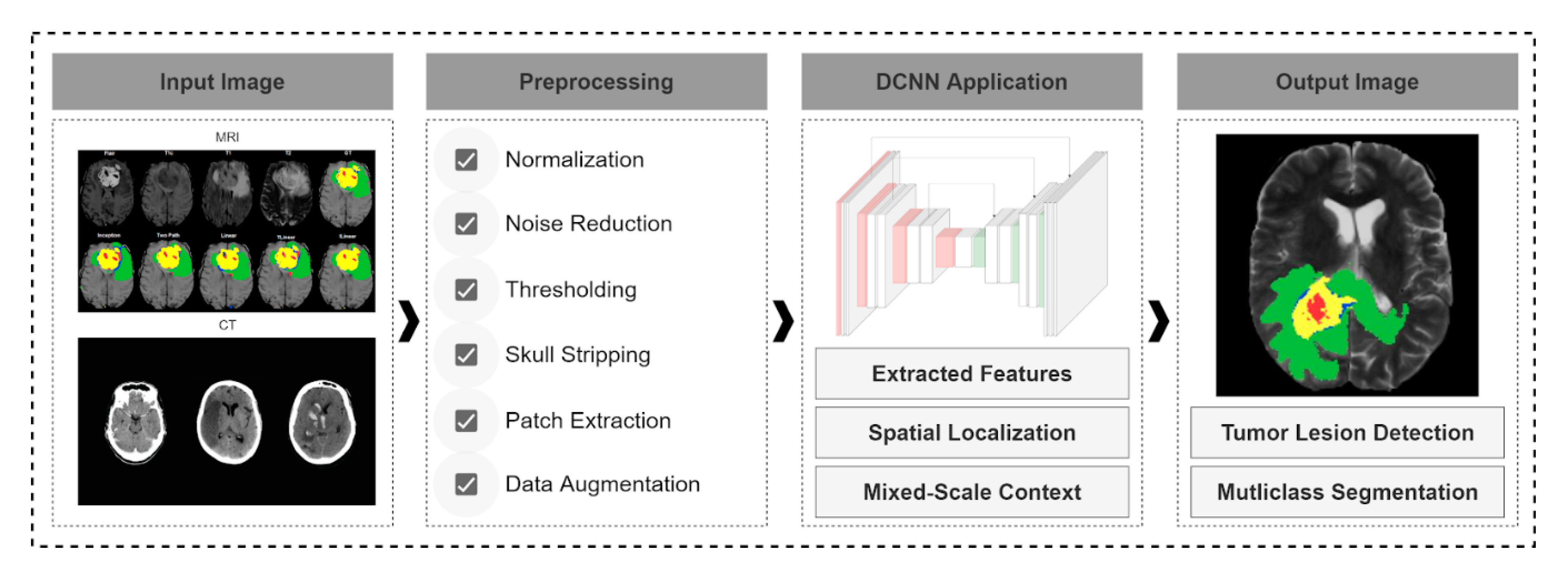
3. DCNNs Application in the Segmentation of Brain Cancer Images
3.1. DCNNs Application in the Segmentation of Brain Cancer MR Images
3.2. DCNNs Application in the Segmentation of Brain Cancer CT Images
3.3. DCNNs Application in the Segmentation of Brain Cancer H&E Histology Images
4. Discussion
5. Challenges and Future Considerations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| ANN | Artificial Neural Network |
| APSO | Adaptive Particle Swarm Optimization |
| AUC | Area Under the Curve |
| BraTS-xxxx | Brain Tumour Segmentation Challenge-year |
| CapsNets | Capsule Networks |
| CLAHE | Contrast Adaptive Histogram Equalization |
| CRF | Conditional Random Forest |
| CT | Computed Tomography |
| DCNN | Deep Convolutional Neural Network |
| DenseNet | Densely Connected Convolutional Networks |
| DMD | Dense Micro-block Difference |
| DNN | Deep (Artificial) Neural Network |
| DWT | Discrete Wavelet Transform |
| ELM | Extreme Learning Machines |
| FA | False Alarm |
| FC | Fully Connected |
| FLAIR | T2-Weighted Fluid-Attenuated Inversion Recovery |
| GAN | Generative Adversarial Networks |
| GBM | Glioblastoma |
| GCNN | Growing Convolution Neural Network |
| GD | Gradient Descent |
| GLCM | Grey Level Co-occurrence Matrix |
| H&E | Haematoxylin and Eosin |
| HCNN | Heterogenous Convolution Neural Network |
| HGG | High-Grade Glioma |
| IDH | Isocitrate Dehydrogenase |
| LBP | Local Binary Pattern |
| LGG | Low-Grade Glioma |
| LoG | Laplacian of Gaussian |
| LRF | Local Receptive Fields |
| LSTM | Long Short-Term Memory |
| MA | Missed Alarm |
| MC-Net | Model Cascade Net |
| ML | Machine Learning |
| MR | Magnetic Resonance |
| M-SVM | Multiclass-Support Vector Machine |
| N/A | Not Available |
| OM-Net | One-Pass Multi-Task Net |
| PCA | Principal Component Analysis |
| Pr | Predictive Model |
| ResNet | Residual Network |
| RNN | Recurrent Neural Network |
| RoI | Region of Interest |
| RRNN | Recurrent Regression-based Neural Networks |
| SVC | Support Vector Classifier |
| SWT | Stationary Wavelet Transform |
| T1 (T1-Weighted) | Longitudinal Relaxation Time |
| T1c | T1-Weighted Post-Contrast |
| T1-Gado | Gadolinium contrast medium in MR images |
| T2 (T2-Weighted) | Transverse Relaxation Time |
| TBI | Traumatic Brain Injury |
| TCGA | The Cancer Genome Atlas |
| TCIA | The Cancer Imaging Archive |
| WBA | The Whole-Brain Atlas |
| WSI | Whole Slide Image |
| xD | x Dimensional |
References
- Shirazi, A.Z.; Mohammadi, Z. A hybrid intelligent model combining ANN and imperialist competitive algorithm for prediction of corrosion rate in 3C steel under seawater environment. Neural Comput. Appl. 2017, 28, 3455–3464. [Google Scholar]
- Shirazi, A.Z.; Hatami, M.; Yaghoobi, M.; Chabok, S.J.S.M. An intelligent approach to predict vibration rate in a real gas turbine. Intell. Ind. Syst. 2016, 2, 253–267. [Google Scholar]
- Shirazi, A.Z.; Tofighi, M.; Ganjefar, S.; Mahdavi, S.J.S. An optimized adaptive-neuro fuzzy inference system (ANFIS) for reliable prediction of entrance length in pipes. Int. J. Enhanc. Res. Sci. Technol. Eng. 2014, 3, 79–89. [Google Scholar]
- Yavuz, E.; Eyupoglu, C. An effective approach for breast cancer diagnosis based on routine blood analysis features. Med. Biol. Eng. Comput. 2020, 58, 1583–1601. [Google Scholar]
- Becker, A. Artificial intelligence in medicine: What is it doing for us today? Health Policy Technol. 2019, 8, 198–205. [Google Scholar]
- Shirazi, A.Z.; Fornaciari, E.; Gomez, G.A. Deep learning in precision medicine. In Artificial Intelligence in Precision Health; Elsevier: Amsterdam, The Netherlands, 2020; pp. 61–90. [Google Scholar]
- Shirazi, A.Z.; Chabok, S.J.S.M.; Mohammadi, Z. A novel and reliable computational intelligence system for breast cancer detection. Med. Biol. Eng. Comput. 2018, 56, 721–732. [Google Scholar]
- Zhu, W.; Xie, L.; Han, J.; Guo, X. The Application of Deep Learning in Cancer Prognosis Prediction. Cancers 2020, 12, 603. [Google Scholar]
- Coccia, M. Deep learning technology for improving cancer care in society: New directions in cancer imaging driven by artificial intelligence. Technol. Soc. 2020, 60, 101198. [Google Scholar]
- Huang, Z.; Johnson, T.S.; Han, Z.; Helm, B.; Cao, S.; Zhang, C.; Salama, P.; Rizkalla, M.; Yu, C.Y.; Cheng, J.; et al. Deep learning-based cancer survival prognosis from RNA-seq data: Approaches and evaluations. BMC Med. Genom. 2020, 13, 1–12. [Google Scholar]
- Baptista, D.; Ferreira, P.G.; Rocha, M. Deep learning for drug response prediction in cancer. Brief. Bioinform. 2020. [Google Scholar] [CrossRef]
- Shao, L.; Shum, H.P.; Hospedales, T. Special Issue on Machine Vision with Deep Learning. Int. J. Comput. Vis. 2020, 128, 771–772. [Google Scholar] [CrossRef] [Green Version]
- Gour, M.; Jain, S.; Kumar, T.S. Residual learning based CNN for breast cancer histopathological image classification. Int. J. Imaging Syst. Technol. 2020, 30, 621–635. [Google Scholar] [CrossRef]
- Chen, X.; Men, K.; Chen, B.; Tang, Y.; Zhang, T.; Wang, S.; Li, Y.; Dai, J. CNN-Based Quality Assurance for Automatic Segmentation of Breast Cancer in Radiotherapy. Front. Oncol. 2020, 10, 524. [Google Scholar] [CrossRef] [PubMed]
- Duran-Lopez, L.; Dominguez-Morales, J.P.; Conde-Martin, A.F.; Vicente-Diaz, S.; Linares-Barranco, A. PROMETEO: A CNN-Based Computer-Aided Diagnosis System for WSI Prostate Cancer Detection. IEEE Access 2020, 8, 128613–128628. [Google Scholar] [CrossRef]
- Liu, Z.; Yang, C.; Huang, J.; Liu, S.; Zhuo, Y.; Lu, X. Deep learning framework based on integration of S-Mask R-CNN and Inception-v3 for ultrasound image-aided diagnosis of prostate cancer. Future Gener. Comput. Syst. 2020, 114, 358–367. [Google Scholar] [CrossRef]
- Meng, J.; Xue, L.; Chang, Y.; Zhang, J.; Chang, S.; Liu, K.; Liu, S.; Wang, B.; Yang, K. Automatic detection and segmentation of adenomatous colorectal polyps during colonoscopy using Mask R-CNN. Open Life Sci. 2020, 15, 588–596. [Google Scholar] [CrossRef]
- Fonollà, R.; van der Zander, Q.E.; Schreuder, R.M.; Masclee, A.A.; Schoon, E.J.; van der Sommen, F. A CNN CADx System for Multimodal Classification of Colorectal Polyps Combining WL, BLI, and LCI Modalities. Appl. Sci. 2020, 10, 5040. [Google Scholar]
- Takahashi, M.; Kameya, Y.; Yamada, K.; Hotta, K.; Takahashi, T.; Sassa, N.; Iwano, S.; Yamamoto, T. An empirical study on the use of visual explanation in kidney cancer detection. In Proceedings of the Twelfth International Conference on Digital Image Processing (ICDIP 2020), Osaka, Japan, 19–22 May 2020; International Society for Optics and Photonics: Bellingham, WA, USA, 2020. [Google Scholar]
- Vasanthselvakumar, R.; Balasubramanian, M.; Sathiya, S. Automatic Detection and Classification of Chronic Kidney Diseases Using CNN Architecture. In Data Engineering and Communication Technology; Springer: Berlin/Heidelberg, Germany, 2020; pp. 735–744. [Google Scholar]
- Hashemzehi, R.; Mahdavi, S.J.S.; Kheirabadi, M.; Kamel, S.R. Detection of brain tumors from MRI images base on deep learning using hybrid model CNN and NADE. Biocybern. Biomed. Eng. 2020, 40, 1225–1232. [Google Scholar] [CrossRef]
- Mzoughi, H.; Njeh, I.; Wali, A.; Slima, M.B.; BenHamida, A.; Mhiri, C.; Mahfoudhe, K.B. Deep Multi-Scale 3D Convolutional Neural Network (CNN) for MRI Gliomas Brain Tumor Classification. J. Digit. Imaging 2020, 33, 903–915. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Amin, Z.S.; Fornaciari, E.; Ebert, L.M.; Koszyca, B.; Gomez, G.A. DeepSurvNet: Deep survival convolutional network for brain cancer survival rate classification based on histopathological images. Med. Biol. Eng. Comput. 2020, 58, 1031–1045. [Google Scholar]
- Perrin, S.L.; Samuel, M.S.; Koszyca, B.; Brown, M.P.; Ebert, L.M.; Oksdath, M.; Gomez, G.A. Glioblastoma heterogeneity and the tumour microenvironment: Implications for preclinical research and development of new treatments. Biochem. Soc. Trans. 2019, 47, 625–638. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, K.; Khan, S.; Ser, J.D.; de Albuquerque, V.H.C. Deep learning for multigrade brain tumor classification in smart healthcare systems: A prospective survey. IEEE Trans. Neural Netw. Learn. Syst. 2020. [Google Scholar] [CrossRef] [PubMed]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015. [Google Scholar]
- Liu, S.; Shah, Z.; Sav, A.; Russo, C.; Berkovsky, S.; Qian, Y.; Coiera, E.; Di Ieva, A. Isocitrate dehydrogenase (iDH) status prediction in histopathology images of gliomas using deep learning. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sumi, P.S.; Delhibabu, R. Glioblastoma Multiforme Classification On High Resolution Histology Image Using Deep Spatial Fusion Network. In Proceedings of the CEUR Workshop, Como, Italy, 9–11 September 2019; pp. 109–120. [Google Scholar]
- Yonekura, A.; Kawanaka, H.; Prasath, V.S.; Aronow, B.J.; Takase, H. Automatic disease stage classification of glioblastoma multiforme histopathological images using deep convolutional neural network. Biomed. Eng. Lett. 2018, 8, 321–327. [Google Scholar] [CrossRef]
- LeCun, Y.; Bottou, L.; Bengio, Y.; Haffner, P. Gradient-based learning applied to document recognition. Proc. IEEE 1998, 86, 2278–2324. [Google Scholar] [CrossRef] [Green Version]
- Zeiler, M.D.; Fergus, R. Visualizing and understanding convolutional networks. In European Conference on Computer Vision; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Fukuma, R.; Yanagisawa, T.; Kinoshita, M.; Shinozaki, T.; Arita, H.; Kawaguchi, A.; Takahashi, M.; Narita, Y.; Terakawa, Y.; Tsuyuguchi, N.; et al. Prediction of IDH and TERT promoter mutations in low-grade glioma from magnetic resonance images using a convolutional neural network. Sci. Rep. 2019, 9, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.; Bai, H.X.; Zhou, H.; Su, C.; Bi, W.L.; Agbodza, E.; Kavouridis, V.K.; Senders, J.T.; Boaro, A.; Beers, A.; et al. Residual convolutional neural network for the determination of IDH status in low-and high-grade gliomas from MR imaging. Clin. Cancer Res. 2018, 24, 1073–1081. [Google Scholar] [CrossRef] [Green Version]
- Alqudah, A.M.; Alquraan, H.; Qasmieh, I.A.; Alqudah, A.; Al-Sharu, W. Brain Tumor Classification Using Deep Learning Technique—A Comparison between Cropped, Uncropped, and Segmented Lesion Images with Different Sizes. arXiv 2020, arXiv:2001.08844. [Google Scholar] [CrossRef]
- Kalaiselvi, T.; Padmapriya, T.; Sriramakrishnan, P.; Priyadharshini, V. Development of automatic glioma brain tumor detection system using deep convolutional neural networks. Int. J. Imaging Syst. Technol. 2020, 30, 926–938. [Google Scholar] [CrossRef]
- Badža, M.M.; Barjaktarović, M.Č. Classification of Brain Tumors from MRI Images Using a Convolutional Neural Network. Appl. Sci. 2020, 10, 1999. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Liu, Y.; Dong, L. G-ResNet: Improved ResNet for brain tumor classification. In International Conference on Neural Information Processing; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Hemanth, D.J.; Anitha, J.; Naaji, A.; Geman, O.; Popescu, D.E.; Son, L.H.; Hoang, L. A modified deep convolutional neural network for abnormal brain image classification. IEEE Access 2018, 7, 4275–4283. [Google Scholar] [CrossRef]
- Afshar, P.; Plataniotis, K.N.; Mohammadi, A. Capsule networks for brain tumor classification based on MRI images and coarse tumor boundaries. In ICASSP 2019—2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP); IEEE: Piscataway Township, NJ, USA, 2019. [Google Scholar]
- Seetha, J.; Raja, S.S. Brain tumor classification using convolutional neural networks. Biomed. Pharmacol. J. 2018, 11, 1457. [Google Scholar] [CrossRef]
- Pashaei, A.; Sajedi, H.; Jazayeri, N. Brain tumor classification via convolutional neural network and extreme learning machines. In 2018 8th International Conference on Computer and Knowledge Engineering (ICCKE); IEEE: Piscataway Township, NJ, USA, 2018. [Google Scholar]
- Zhou, Y.; Li, Z.; Zhu, H.; Chen, C.; Gao, M.; Xu, K.; Xu, J. Holistic brain tumor screening and classification based on densenet and recurrent neural network. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Mohsen, H.; El-Dahshan, E.S.A.; El-Horbaty, E.S.M.; Salem, A.B.M. Classification using deep learning neural networks for brain tumors. Future Comput. Inform. J. 2018, 3, 68–71. [Google Scholar] [CrossRef]
- Ari, A.; Hanbay, D. Deep learning based brain tumor classification and detection system. Turk. J. Electr. Eng. Comput. Sci. 2018, 26, 2275–2286. [Google Scholar] [CrossRef]
- Suter, Y.; Jungo, A.; Rebsamen, M.; Knecht, U.; Herrmann, E.; Wiest, R.; Reyes, M. Deep learning versus classical regression for brain tumor patient survival prediction. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Banerjee, S.; Mitra, S.; Masulli, F.; Rovetta, S. Brain tumor detection and classification from multi-sequence MRI: Study using convnets. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Afshar, P.; Mohammadi, A.; Plataniotis, K.N. Brain tumor type classification via capsule networks. In 2018 25th IEEE International Conference on Image Processing (ICIP); IEEE: Piscataway, NJ, USA, 2018. [Google Scholar]
- Bagari, A.; Kumar, A.; Kori, A.; Khened, M.; Krishnamurthi, G. A combined Radio-Histological Approach for Classification of Low Grade Gliomas. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Sajjad, M.; Khan, S.; Muhammad, K.; Wu, W.; Ullah, A.; Baik, S.W. Multi-grade brain tumor classification using deep CNN with extensive data augmentation. J. Comput. Sci. 2019, 30, 174–182. [Google Scholar] [CrossRef]
- Cheng, J.; Huang, W.; Cao, S.; Yang, R.; Yang, W.; Yun, Z.; Wang, Z.; Feng, Q. Enhanced performance of brain tumor classification via tumor region augmentation and partition. PLoS ONE 2015, 10, e0140381. [Google Scholar] [CrossRef]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [Green Version]
- Menze, B.H.; Jakab, A.; Bauer, S.; Kalpathy-Cramer, J.; Farahani, K.; Kirby, J.; Burren, Y.; Porz, N.; Slotboom, J.; Wiest, R.; et al. The multimodal brain tumor image segmentation benchmark (BRATS). IEEE Trans. Med. Imaging 2014, 34, 1993–2024. [Google Scholar] [CrossRef]
- Vidoni, E.D. The Whole Brain Atlas: Www. med. harvard. edu/aanlib. J. Neurol. Phys. Ther. 2012, 36, 108. [Google Scholar]
- Caldairou, B.; Passat, N.; Habas, P.A.; Studholme, C.; Rousseau, F. A non-local fuzzy segmentation method: Application to brain MRI. Pattern Recognit. 2011, 44, 1916–1927. [Google Scholar]
- Cancer Genome Atlas Research Network; Weinstein, J.N.; Collisson, E.A.; Mills, G.B.; Shaw, K.R.; Ozenberger, B.A.; Ellrott, K.; Shmulevich, I.; Sander, C.; Stuart, J.M. The cancer genome atlas pan-cancer analysis project. Nat. Genet. 2013, 45, 1113. [Google Scholar] [PubMed]
- Brain Tumor Dataset. Available online: https://figshare.com/articles/brain_tumor_dataset/1512427/5 (accessed on 10 September 2020).
- BraTS2013. Available online: https://qtim-lab.github.io/ (accessed on 10 September 2020).
- The Whole Brain Atlas. Available online: http://www.med.harvard.edu/AANLIB/ (accessed on 10 September 2020).
- BraTS2018. Available online: https://www.med.upenn.edu/sbia/brats2018/data.html (accessed on 10 September 2020).
- Devaki Scans & Diagnostics. Available online: https://www.medindia.net/labs/devaki-scans-diagnostics-madurai-tamil-nadu-1680-1.htm (accessed on 10 September 2020).
- Radiopaedia. Available online: https://radiopaedia.org/ (accessed on 10 September 2020).
- BraTS2015. Available online: https://www.smir.ch/BRATS/Start2015 (accessed on 10 September 2020).
- Suhag, S.; Saini, L.M. Automatic brain tumor detection and classification using svm classifier. In Proceedings of the ISER 2nd International Conference, Singapore, 20–21 September 2015. [Google Scholar]
- Kwan, R.-S.; Evans, A.C.; Pike, G.B. MRI simulation-based evaluation of image-processing and classification methods. IEEE Trans. Med. Imaging 1999, 18, 1085–1097. [Google Scholar] [PubMed]
- Scarpace, L.; Mikkelsen, L.; Cha, T.; Rao, S.; Tekchandani, S.; Gutman, S.; Pierce, D. Radiology data from the cancer genome atlas glioblastoma multiforme [TCGA-GBM] collection. Cancer Imaging Arch. 2016, 11, 1. [Google Scholar]
- Pedano, N.; Flanders, A.E.; Scarpace, L.; Mikkelsen, T.; Eschbacher, J.M.; Hermes, B.; Ostrom, Q. Radiology data from the cancer genome atlas low grade glioma [TCGA-LGG] collection. Cancer Imaging Arch. 2016, 2. [Google Scholar]
- Ismael, S.A.A.; Mohammed, A.; Hefny, H. An enhanced deep learning approach for brain cancer MRI images classification using residual networks. Artif. Intell. Med. 2020, 102, 101779. [Google Scholar]
- Maharjan, S.; Alsadoon, A.; Prasad, P.W.C.; Al-Dalain, T.; Alsadoon, O.H. A novel enhanced softmax loss function for brain tumour detection using deep learning. J. Neurosci. Methods 2020, 330, 108520. [Google Scholar]
- Vijh, S.; Sharma, S.; Gaurav, P. Brain Tumor Segmentation Using OTSU Embedded Adaptive Particle Swarm Optimization Method and Convolutional Neural Network. In Data Visualization and Knowledge Engineering; Springer: Berlin/Heidelberg, Germany, 2020; pp. 171–194. [Google Scholar]
- Rani, N.S.; Karthik, U.; Ranjith, S. Extraction of Gliomas from 3D MRI Images using Convolution Kernel Processing and Adaptive Thresholding. Procedia Comput. Sci. 2020, 167, 273–284. [Google Scholar]
- Deng, W.; Shi, Q.; Wang, M.; Zheng, B.; Ning, N. Deep Learning-Based HCNN and CRF-RRNN Model for Brain Tumor Segmentation. IEEE Access 2020, 8, 26665–26675. [Google Scholar]
- Deng, W.; Shi, Q.; Luo, K.; Yang, Y.; Ning, N. Brain tumor segmentation based on improved convolutional neural network in combination with non-quantifiable local texture feature. J. Med. Syst. 2019, 43, 152. [Google Scholar] [CrossRef] [PubMed]
- Kumar, G.A.; Sridevi, P. Intensity Inhomogeneity Correction for Magnetic Resonance Imaging of Automatic Brain Tumor Segmentation. In Microelectronics, Electromagnetics and Telecommunications; Springer: Berlin/Heidelberg, Germany, 2019; pp. 703–711. [Google Scholar]
- Mittal, M.; Goyal, L.M.; Kaur, S.; Kaur, I.; Verma, A.; Jude Hemanth, D. Hemanth Deep learning based enhanced tumor segmentation approach for MR brain images. Appl. Soft Comput. 2019, 78, 346–354. [Google Scholar]
- Mittal, A.; Kumar, D. AiCNNs (Artificially-integrated Convolutional Neural Networks) for Brain Tumor Prediction. Eai Endorsed Trans. Pervasive Health Technol. 2019, 5, 346–354. [Google Scholar] [CrossRef]
- Thillaikkarasi, R.; Saravanan, S. An enhancement of deep learning algorithm for brain tumor segmentation using kernel based CNN with M-SVM. J. Med. Syst. 2019, 43, 84. [Google Scholar] [CrossRef]
- Sharma, A.; Kumar, S.; Singh, S.N. Brain tumor segmentation using DE embedded OTSU method and neural network. Multidimens. Syst. Signal Process. 2019, 30, 1263–1291. [Google Scholar] [CrossRef]
- Kong, X.; Sun, G.; Wu, Q.; Liu, J.; Lin, F. Hybrid pyramid u-net model for brain tumor segmentation. In International Conference on Intelligent Information Processing; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Benson, E.; Pound, M.P.; French, A.P.; Jackson, A.S.; Pridmore, T.P. Deep hourglass for brain tumor segmentation. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Zhou, C.; Chen, S.; Ding, C.; Tao, D. Learning contextual and attentive information for brain tumor segmentation. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Dai, L.; Li, T.; Shu, H.; Zhong, L.; Shen, H.; Zhu, H. Automatic brain tumor segmentation with domain adaptation. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Kermi, A.; Mahmoudi, I.; Khadir, M.T. Deep convolutional neural networks using U-Net for automatic brain tumor segmentation in multimodal MRI volumes. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Mlynarski, P.; Delingette, H.; Criminisi, A.; Ayache, N. Deep learning with mixed supervision for brain tumor segmentation. J. Med. Imaging 2019, 6, 034002. [Google Scholar] [CrossRef]
- Wang, G.; Li, W.; Zuluaga, M.A.; Pratt, R.; Patel, P.A.; Aertsen, M.; Doel, T.; David, A.L.; Deprest, J.; Ourselin, S.; et al. Interactive medical image segmentation using deep learning with image-specific fine tuning. IEEE Trans. Med. Imaging 2018, 37, 1562–1573. [Google Scholar] [CrossRef]
- Monteiro, M.; Newcombe, V.F.; Mathieu, F.; Adatia, K.; Kamnitsas, K.; Ferrante, E.; Das, T.; Whitehouse, D.; Rueckert, D.; Menon, D.K. Multiclass semantic segmentation and quantification of traumatic brain injury lesions on head CT using deep learning: An algorithm development and multicentre validation study. Lancet Digit. Health 2020, 2, 314–322. [Google Scholar] [CrossRef]
- Xu, Y.; Jia, Z.; Ai, Y.; Zhang, F.; Lai, M.; Eric, I.; Chang, C. Deep convolutional activation features for large scale brain tumor histopathology image classification and segmentation. In 2015 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP); IEEE: Piscataway Township, NJ, USA, 2015. [Google Scholar]
- Internet Brain Segmentation Repository. Available online: https://datamed.org/display-item.php?repository=0058&id=590247f25152c6571cff8916&query= (accessed on 11 November 2020).
- CENTER-TBI. Available online: https://www.center-tbi.eu/data (accessed on 10 September 2020).
- CQ500 Dataset. Available online: http://headctstudy.qure.ai/dataset (accessed on 10 September 2020).
- DICOM Image Sample Sets. Available online: https://www.osirix-viewer.com/resources/dicom-image-library/ (accessed on 10 September 2020).
- BraTS2017. Available online: https://www.med.upenn.edu/sbia/brats2017/data.html (accessed on 10 September 2020).
- MICCAI 2014 Boston. Available online: http://miccai2014.org/ (accessed on 10 September 2020).
- Wang, Q.; Hu, B.; Hu, X.; Kim, H.; Squatrito, M.; Scarpace, L.; Decarvalho, A.C.; Lyu, S.; Li, P.; Li, Y.; et al. Tumor evolution of glioma-intrinsic gene expression subtypes associates with immunological changes in the microenvironment. Cancer Cell 2017, 32, 42–56.e6. [Google Scholar]



{kind=link}
{kind=link}
| Ref. | Year | Task | Tumor Type | Image Type | Model Name | Model Desc. | Software | Hardware | Dataset | Instances/ Cases | Perf. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [26] ** | 2020 | Classification |
| MRI | Six DCNN Architectures * | A prospective survey on Deep Learning techniques applied for Multigrade Brain Tumor Classification |
| NVidia TITAN X (Pascal) |
|
| |
| [24] ** | 2020 | Classification |
| H&E Histology | DeepSurvNet | Brain cancer patients’ survival rate classification by using deep convolutional neural network |
| 4xNVidia 1080 Ti GPU |
|
|
|
| [28] ** | 2020 | Prediction |
| H&E Histology | GAN-based ResNet50 * | Gliomas’ IDH status prediction by using the GAN model for data augmentation and Resnet50 as a predictive model |
| N/A |
|
|
|
| [36] | 2020 | Classification |
| MR (T1 weighted contrast-enhanced) | 18 layers DCNN * | Meningioma, glioma, and pituitary tumors classification by using 18 layers DCNN-based model on MR images | N/A |
| Brain tumor public dataset [58] | 3064 |
|
| [38] | 2020 | Classification |
| MR (T1 weighted contrast-enhanced) | 22 layers DCNN * | Meningioma, glioma, and pituitary tumors classification by using 22 layers DCNN-based model based on MR images | MATLAB R2018a | NVidia 1050 Ti GPU | Brain tumor public dataset [58] | 3064 | Accuracy: 0.96 |
| [37] ** | 2020 | Classification |
| MR (T2 weighted) | FLSCBN | Tumor vs non-tumor classification by using a five layers DCNN-based model on MR images |
|
|
|
| |
| [22] ** | 2020 | Classification |
| MR (T1-Gado or T1-weighted) | 3-D DCNN | 11 layers 3-D DCNN-based model to classify glioma tumors into LGG and HGG using the T1-weighted MR images |
|
| BraTS2018 [61] | 351 | Accuracy: 0.96 |
| [34] ** | 2019 | Classification | Glioma | MRI | AlexNet; Linear Support Vector Machine | Identify IDH and pTERT mutations using age, radiomic features, and tumor texture features | Caffe | N/A | Not Publicly Available | 164 | Accuracy: 63.1% |
| [29] | 2019 | Classification |
| H&E Histology | INRV2-based deep spatial fusion network * | A mixed DCNN architecture combining InceptionResNetV2 and deep spatial fusion network to classify four different kinds of brain tumors based on H&E images | PyTorch | NVidia 1080 Ti GPU | TCGA [57] TCIA [53] |
|
|
| [39] | 2019 | Classification |
| MR (T1 weighted contrast-enhanced) | G-ResNet | Meningioma, glioma, and pituitary tumors classification by using a ResNet34-based model with global average pooling and modified loss function based on MR images | PyTorch | NVidia 1080 Ti GPU | Brain tumor public dataset [58] | 3064 | Accuracy: 0.95 |
| [40] | 2019 | Classification |
| MR (T1, T2, and T2 flair) | MDCNN | Metastasis, Meningioma, Glioma and Astrocytoma tumors classification using a modified DCNN with reduced computational complexity based on MR images | N/A | N/A | Brain tumor private dataset [62] | 220 | Accuracy: 0.96 |
| [30] | 2018 | Classification |
| H&E Histology | Deep CNN | GBM and LGG classification by using DCNN-based model based on H&E Histological images |
|
| TCGA [57] | 200 | Accuracy: 0.96 |
| [50] | 2018 | Classification |
| H&E Histology; MR FLAIR, T1, T1C, and T2 images | A combined DCNNs-based network * | Astrocytoma and Oligodendroglioma classification by using DCNN-based model based on both MR and Histological images | N/A | N/A | Private dataset | 50 | Accuracy: 0.90 |
| [43] | 2018 | Classification |
| MR (T1 weighted contrast-enhanced) | KE-CNN | Meningioma, glioma, and pituitary tumors classification by using a mixed approach of DCNN and extreme learning based on MR images | N/A | N/A | Brain tumor public dataset [58] | 3064 | Accuracy: 0.93 |
| [44] | 2018 | Classification | Public dataset:
|
| DenseNet-LSTM |
|
| Nvidia Titan Xp GPU |
|
|
|
| [41] | 2018 | Classification |
| MR (T1 weighted contrast-enhanced) | CapsNet | Meningioma, Glioma, and Pituitary tumors classification by using a developed CapsNet architecture based on MR images |
| N/A | Brain tumor public dataset [58] | 3064 | Accuracy: 0.91 |
| [49] | 2018 | Classification |
| MR (T1 weighted contrast-enhanced) | CapsNet | Meningioma, Glioma, and Pituitary tumors classification by using a developed CapsNet architecture based on MR images | N/A | N/A | Brain tumor public dataset [58] | 3064 | Accuracy: 0.86 |
| [42] | 2018 | Classification |
| MR | Pre-trained DCNN | Brian tumors vs nontumors classification by using a pretrained DCNN based on MR images | Python | N/A | N/A | Accuracy: 0.97 | |
| [45] | 2018 | Classification |
| MR (T2 weighted) | DWT-DNN * | Normal lesion and GBM, Sarcoma, and Metastasis tumors classification by using DWT-DNN based on MR images |
| N/A | Public dataset [65] | 66 |
|
| [46] | 2018 | Classification |
| MR (T1 weighted) | DCNN vs ELM-LRF * | Benign vs malignant tumors classification by using DCNN and ELM-LRF models on MR images | MATLAB R2015a | N/A | Public dataset [66] | 16 |
|
| [47] ** | 2018 | Prediction | GBM | MR (T1-weighted, T1c, T2-weighted, FLAIR) | SVC Ensemble | GBM patient survival rate classification by using two different DCNN models based on MR images | Python | Nvidia Titan Xp GPU | BraTS2018 [61] | 293 | Accuracy: 0.42 |
| [48] | 2018 | Classification |
| MR (T1-weighted, T1c, T2-weighted, FLAIR) |
| GBM and LGG classification by using DCNN-based models based on MR images |
|
| 461 | Accuracy: 0.97 | |
| [35] ** | 2018 | Classification | Glioma | MRI | ResNet50 | Identify IDH1/2 mutations in glioma grades II-IV using ResNet50 |
| N/A | From Hospital of the University of Pennsylvania, Brigham and Women’s Hospital, The Cancer Imaging Center, Dana-Farber/Brigham and Women’s Cancer Center | 603, 414, 471 (With respect to sources) | Accuracy: 85.7% |
| Ref | Year | Tumor Type | Task | Model Name | Image Type | Model Desc. | Software | Hardware | Dataset | Instances | Performance |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [70] ** | 2020 | Glioma, Meningioma, Pituitary | Segmentation | ELM-LRF | MRI | Implemented an enhanced softmax loss function that is more suitable for multiclass applications. | Python 3.6; Keras |
| Brain Tumor Dataset [58] | 3064 | 99.54%, 98.14%, 98.67% (Per Tumor Type) |
| [69] | 2020 | Glioma, Meningioma, Pituitary | Segmentation | ResNet50 | MRI | Glioma, meningioma, and pituitary tumor segmentation with the ResNet50 architecture. |
|
| Brain Tumor Dataset [58] | 3064 | 99% |
| [73] | 2020 | Glioma | Segmentation | HCNN; CRF-RRNN | MRI | The composite architecture of HCNN to capture mixed scale context and CRF-RRNN reconstruct a global segmentation. | N/A | N/A | 220 HGG; 50 LGG | 98.6% | |
| [74] | 2019 | Glioma | Segmentation | FCNN; DMD | MRI | Enhanced FCNN with batch normalization and DMD features to provide spatial consistency. Fisher vector encoding method for texture invariance to scale and rotation. | Caffe |
| BraTS2015 [64] | 220 HGG; 50 LGG | 91% |
| [86] ** | 2018 | Glioma | Segmentation | P-Net; PC-Net | MRI | Addresses zero-shot learning by taking user input bounding boxes and scribbles to fine-tune segmentations. | Caffe |
| BraTS2015 [64] | 220 HGG; 50 LGG | 86.29% |
| [75] | 2019 | Glioma | Segmentation | FCNN | MRI | A novel N3T-spline utilizes is used to preprocess 3D input images. GLCM extracts feature vectors and are inputs into a CNN. | MATLAB R2017a | N/A | BraTS2015 [64] | 220 HGG; 50 LGG | N/A |
| [71] | 2020 | N/A | Segmentation | 3-layer DCNN * | MRI | Utilized Otsu thresholding to create a novel skull stripping algorithm. GLCM and a three-layer CNN segments the stripped images. | MATLAB R2018b | N/A | IBSR [89] | 18 | 98% |
| [72] | 2020 | Glioma | Segmentation | Automatic Detection and Segmentation of Tumor (ADST) * | 3D MRI | Region Growing and Local Binary Pattern (LBP) operators are used to build a feature vector that is then segmented | N/A | N/A | BraTS2018 [61] | 210 HGG; 75 LGG | 87.20% for HGG; 83.77 for LGG (Average Jaccard) |
| [81] ** | 2019 | Glioma | Segmentation | Hourglass Net | MRI | Enhanced Hourglass Network with added residual blocks and novel concatenation layers. | N/A | NVIDIA TITAN X GPU | BraTS2018 [61] | 210 HGG; 75 LGG | 92% |
| [83] ** | 2019 | Glioma | Segmentation | XGBoost; U-Net; DAU-Net (Domain Adaptive U-Net) * | MRI | Implementation of a U-Net variation using instance normalization to boost domain adaptation. | PyTorch | 4 NVIDIA Titan Xp GPU cards | BraTS2018 [61] | 210 HGG; 75 LGG | 91% (Whole Tumor) |
| [82] | 2019 | Glioma | Segmentation | MC-Net; OM-Net | MRI | Ensemble network of several MC-Net and OM-Net variations. Attention mechanisms are added to increases sensitivity to relevant channel-wise interdependencies | N/A | N/A | BraTS2018 [61] | 210 HGG; 75 LGG | 90% (Whole Tumor) |
| [84] ** | 2019 | Glioma | Segmentation | U-Net | MRI | The U-Net variation that uses batch normalization and residual blocks to improve performance on neurological images. | N/A |
| BraTS2018 [61] | 210 HGG; 75 LGG | 86.8% (Whole Tumor) |
| [85] | 2019 | Glioma | Segmentation | U-Net | MRI | Extension of the U-Net to train with “mixed supervision”, meaning both pixel-wise & image-level ground truths to achieve superior performance. | N/A | N/A | BraTS2018 [61] | 210 HGG; 75 LGG | N/A for the entire dataset |
| [77] | 2019 | Glioma, Meningioma, Pituitary, and Negative | Classification |
| MRI | Several of the pre-trained models (simple CNNs, Xception, VGG16, and VGG19) were fused together in a composite architecture. | Keras | N/A | N/A | 1167 | 98.89% |
| [87] ** | 2020 | TBI (Traumatic Brain Injury) | Segmentation | CNN | CT | 3D CNN architecture to create voxel-wise segmentation of TBI CT scans. | N/A | N/A | CENTER-TBI (Datasets 1 & 2) [90]; CQ500 [91] | 539; 500 (Patients) | 94% |
| [78] | 2019 | N/A | Segmentation | M-SVM; CNN | MRI | SGLDM and M-SVM are applied to extract and classify MRI scans. CNN is then applied to segment the extracted feature vectors. | N/A | N/A | N/A | 40 | 84% |
| [76] | 2019 | N/A | Segmentation | SWT; GCNN | MRI | Dataset is preprocessed with a novel skull stripping. Features are extracted with SWT, classified with a Random Forest implementation and finally segmented with GCNN. | N/A | N/A | BRAINIX [92] | 2457 | 98.6% (SSIM Score) |
| [80] ** | 2018 | Glioma | Segmentation | U-Net | MRI | HPU-Net enhances the traditional U-Net with multiscale images and image pyramids. | Keras; Tensorflow | NVIDIA Titan X GPU | 430 HGG; 145 LGG | 71% and 80% (Respective to dataset) | |
| [88] ** | 2015 | Glioma | Segmentation | ImageNet LSVRC 2013 | H&E Histology | Patches are extracted from large histopathology scans and passed into ImageNet LSVRC 2013 architecture. Linear SVM classifier pools extracted feature vectors. | N/A | N/A | MICCAI 2014 [94] | 35 | 84% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zadeh Shirazi, A.; Fornaciari, E.; McDonnell, M.D.; Yaghoobi, M.; Cevallos, Y.; Tello-Oquendo, L.; Inca, D.; Gomez, G.A. The Application of Deep Convolutional Neural Networks to Brain Cancer Images: A Survey. J. Pers. Med. 2020, 10, 224. https://doi.org/10.3390/jpm10040224
Zadeh Shirazi A, Fornaciari E, McDonnell MD, Yaghoobi M, Cevallos Y, Tello-Oquendo L, Inca D, Gomez GA. The Application of Deep Convolutional Neural Networks to Brain Cancer Images: A Survey. Journal of Personalized Medicine. 2020; 10(4):224. https://doi.org/10.3390/jpm10040224
Chicago/Turabian StyleZadeh Shirazi, Amin, Eric Fornaciari, Mark D. McDonnell, Mahdi Yaghoobi, Yesenia Cevallos, Luis Tello-Oquendo, Deysi Inca, and Guillermo A. Gomez. 2020. "The Application of Deep Convolutional Neural Networks to Brain Cancer Images: A Survey" Journal of Personalized Medicine 10, no. 4: 224. https://doi.org/10.3390/jpm10040224