
A Clustered Case Series of Mucorales Detection in Respiratory Samples from COVID-19 Patients in Intensive Care, France, August to September 2021

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Fungal PCR and Culture
2.3. Statistical Analyses
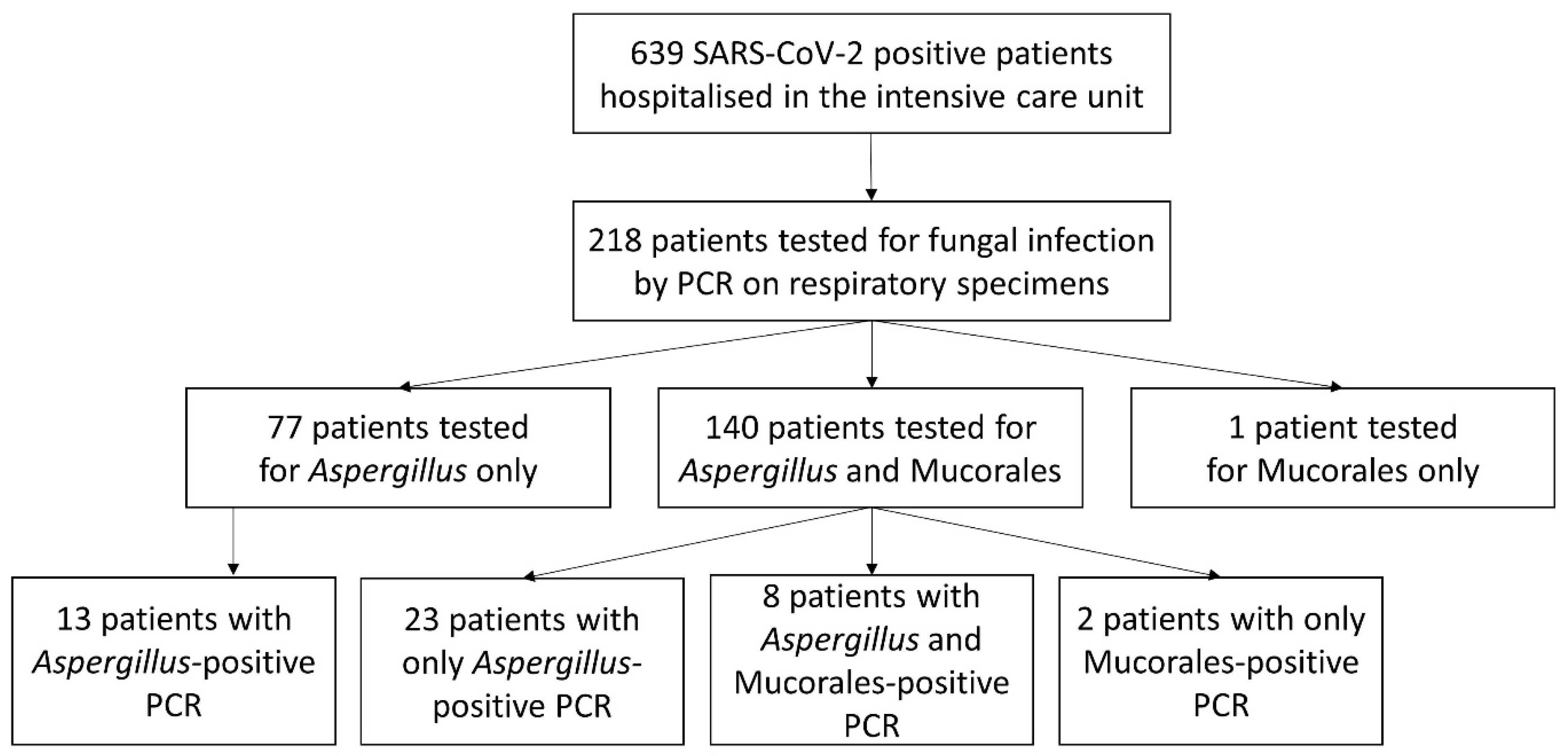
3. Results
3.1. Patients Characteristics
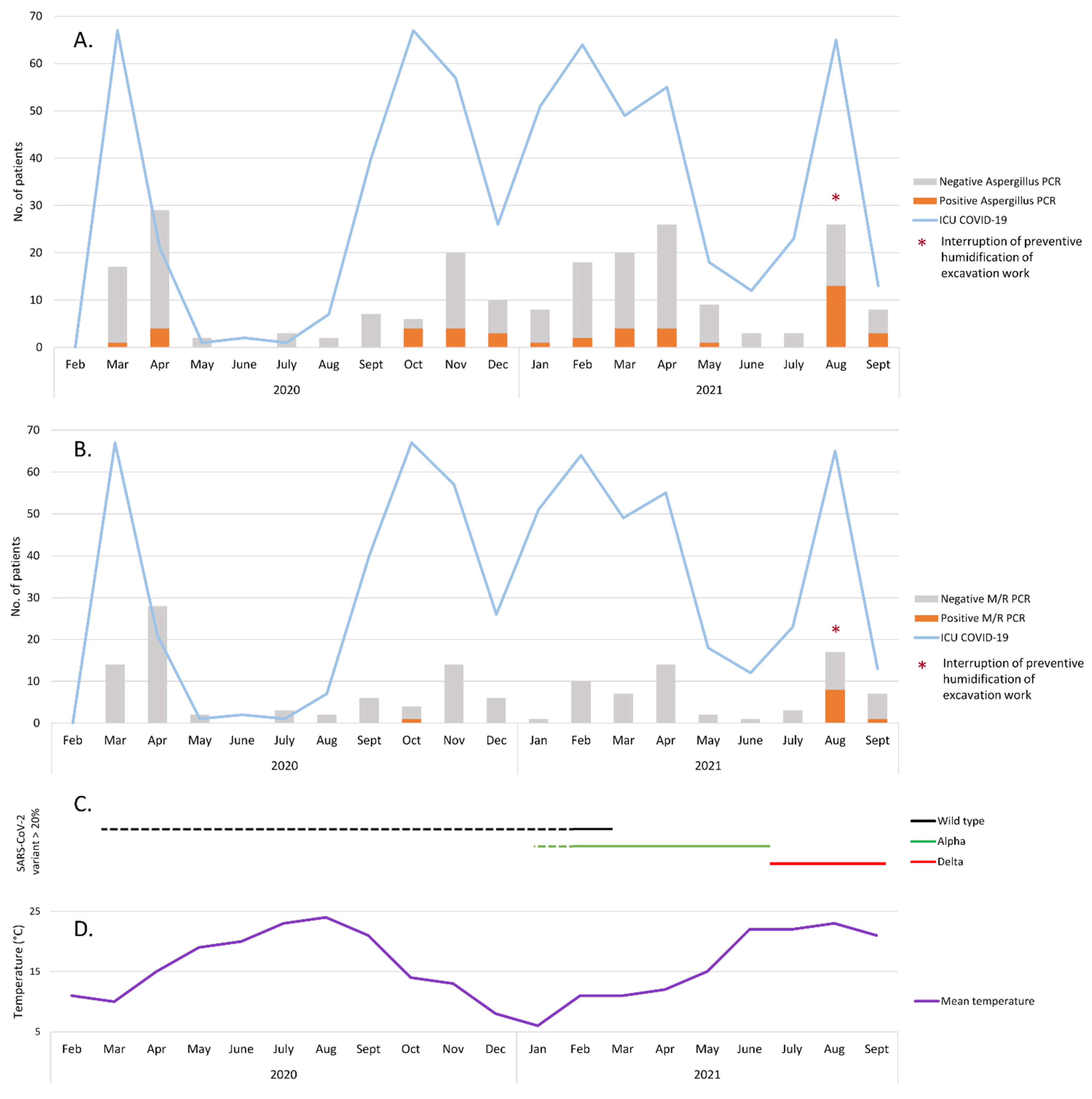
3.2. Evaluation of the Incidence of Aspergillus- and Mucorales-Positive PCRs among ICU COVID-19 Patients
3.3. Mucorales Infections among COVID-19-Patients in the ICU
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lescure, F.-X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.-H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Le Hingrat, Q.; et al. Clinical and virological data of the first cases of COVID-19 in Europe: A case series. Lancet Infect. Dis. 2020, 20, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Patel, A.; Agarwal, R.; Rudramurthy, S.M.; Shevkani, M.; Xess, I.; Sharma, R.; Savio, J.; Sethuraman, N.; Madan, S.; Shastri, P.; et al. Multicenter epidemiologic study of coronavirus disease-associated mucormycosis, India. Emerg. Infect. Dis. 2021, 27, 2349–2359. [Google Scholar] [CrossRef] [PubMed]
- Rudramurthy, S.M.; Hoenigl, M.; Meis, J.F.; Cornely, O.A.; Muthu, V.; Gangneux, J.P.; Perfect, J.; Chakrabarti, A. ECMM/ISHAM recommendations for clinical management of COVID-19 associated mucormycosis in low- and middle-income countries. Mycoses 2021, 64, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Gangneux, J.-P.; Dannaoui, E.; Fekkar, A.; Luyt, C.-E.; Botterel, F.; De Prost, N.; Tadié, J.-M.; Reizine, F.; Houzé, S.; Timsit, J.-F.; et al. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: The French multicentre MYCOVID study. Lancet Respir. Med. 2021, 10, 180–190. [Google Scholar] [CrossRef]
- de la Santé Publique, C. Décret n° 2017-884 du 9 mai 2017 modifiant certaines dispositions réglementaires relatives aux recherches impliquant la personne humaine. Article R. 2017, 1121-1-1. [Google Scholar]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in hospitalized patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Costa, C.; Costa, J.-M.; Desterke, C.; Botterel, F.; Cordonnier, C.; Bretagne, S. Real-time PCR coupled with automated DNA extraction and detection of galactomannan antigen in serum by enzyme-linked immunosorbent assay for diagnosis of invasive aspergillosis. J. Clin. Microbiol. 2002, 40, 2224–2227. [Google Scholar] [CrossRef] [Green Version]
- Millon, L.; Herbrecht, R.; Grenouillet, F.; Morio, F.; Alanio, A.; Letscher-Bru, V.; Cassaing, S.; Chouaki, T.; Kauffmann-Lacroix, C.; Poirier, P.; et al. Early diagnosis and monitoring of mucormycosis by detection of circulating DNA in serum: Retrospective analysis of 44 cases collected through the French Surveillance Network of Invasive Fungal Infections (RESSIF). Clin. Microbiol. Infect. 2016, 22, e1–e810. [Google Scholar] [CrossRef] [Green Version]
- Normand, A.C.; Becker, P.; Gabriel, F.; Cassagne, C.; Accoceberry, I.; Gari-Toussaint, M.; Hasseine, L.; De Geyter, D.; Pierard, D.; Surmont, I.; et al. Validation of a new web application for identification of fungi by use of Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry. J. Clin. Microbiol. Am. Soc. Microbiol. 2017, 55, 2661–2670. [Google Scholar] [CrossRef] [Green Version]
- Météo Toulouse (Haute-Garonne), Août 2021. Hist.-Météo. Available online: https://www.historique-meteo.net/france/midi-toulousain/toulouse/2021/08/ (accessed on 24 February 2022).
- Bellanger, A.P.; Navellou, J.C.; Lepiller, Q.; Brion, A.; Brunel, A.S.; Millon, L.; Berceanu, A. Mixed mold infection with Aspergillus fumigatus and Rhizopus microsporus in a severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) patient. Infect. Dis. Now 2021, 51, 633–635. [Google Scholar] [CrossRef]
- Buil, J.B.; van Zanten, A.R.H.; Bentvelsen, R.G.; Rijpstra, A.T.; Goorhuis, B.; van der Voort, S.; Wammes, L.J.; Janson, A.J.; Melchers, M.; Heusinkveld, M.; et al. Case series of four secondary mucormycosis infections in COVID-19 patients, the Netherlands, December 2020 to May 2021. Eurosurveillance 2021, 26, 2100510. [Google Scholar] [CrossRef] [PubMed]
- Danion, F.; Letscher-Bru, V.; Guitard, J.; Sitbon, K.; Dellière, S.; Angoulvant, A.; Desoubeaux, G.; Botterel, F.; Bellanger, A.-P.; Gargala, G.; et al. Coronavirus disease 2019-Associated Mucormycosis in France: A rare but deadly complication. Open Forum Infect. Dis. 2022, 9, ofab566. [Google Scholar] [CrossRef] [PubMed]
- Gumashta, J.; Gumashta, R. COVID19 associated mucormycosis: Is GRP78 a possible link? J. Infect. Public Health 2021, 14, 1351–1357. [Google Scholar] [CrossRef] [PubMed]
- Panagopoulou, P.; Filioti, J.; Farmaki, E.; Maloukou, A.; Roilides, E. Filamentous fungi in a tertiary care hospital: Environmental surveillance and susceptibility to antifungal drugs. Infect. Control. Hosp. Epidemiol. 2007, 28, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Athan, E.; Morrissey, C.O.; Slavin, M.A. Preventing invasive fungal infection during hospital building works. Intern. Med. J. 2008, 38, 538–541. [Google Scholar] [CrossRef]
- Kanamori, H.; Rutala, W.A.; Sickbert-Bennett, E.E.; Weber, D.J. Review of fungal outbreaks and infection prevention in healthcare settings during construction and renovation. Clin. Infect. Dis. 2015, 61, 433–444. [Google Scholar] [CrossRef]
- Salmanton-Garcia, J.; Sprute, R.; Stemler, J.; Bartoletti, M.; Dupont, D.; Valerio, M.; Garcia-Vidal, C.; Falces-Romero, I.; Machado, M.; de la Villa, S.; et al. COVID-19-Associated Pulmonary Aspergillosis, March-August 2020. Emerg. Infect. Dis. 2021, 27, 1077–1086. [Google Scholar] [CrossRef]
- Sivagnanam, S.; Sengupta, D.J.; Hoogestraat, D.; Jain, R.; Stednick, Z.; Fredricks, D.N.; Hendrie, P.; Whimbey, E.; Podczervinski, S.T.; Krantz, E.M.; et al. Seasonal clustering of sinopulmonary mucormycosis in patients with hematologic malignancies at a large comprehensive cancer center. Antimicrob. Resist. Infect. Control. 2017, 6, 123. [Google Scholar] [CrossRef] [Green Version]
- Al-Ajam, M.R.; Bizri, A.R.; Mokhbat, J.; Weedon, J.; Lutwick, L. Mucormycosis in the Eastern Mediterranean: A seasonal disease. Epidemiol. Infect. 2006, 134, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Chamilos, G.; Lewis, R.E.; Kontoyiannis, D.P. Delaying amphotericin B-based frontline therapy significantly increases mortality among patients with hematologic malignancy who have zygomycosis. Clin. Infect. Dis. 2008, 47, 503–509. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient | Period | Age | Sex | SARS-CoV-2 Variant | Underling Conditions | Dexamethasone | Tocilizumab | Serum M/R PCR | CAM Therapy | Aspergillus Associated | Death |
|---|---|---|---|---|---|---|---|---|---|---|---|
| A | October 2020 | 83 | m | Undetermined | Hypertension | Yes | No | Positive | L-AmB | Yes | Yes |
| B | August 2021 | 72 | m | Delta | No | Yes | Yes | Positive | L-AmB, PCZ | Yes | Yes |
| C | August 2021 | 58 | f | Delta | BMI > 30, ET | Yes | Yes | Positive | L-AmB, IVZ, PCZ | Yes | No |
| D | August 2021 | 68 | m | Delta | Hypertension, CRI | Yes | Yes | Negative | L-AmB | Yes | Yes |
| E | August 2021 | 39 | f | Delta | BMI > 30 | Yes | Yes | Negative | L-AmB, IVZ | No | No |
| F | August 2021 | 73 | m | Undetermined | Hypertension | Yes | Yes | Negative | L-AmB, IVZ | Yes | No |
| G | August 2021 | 52 | m | Delta | BMI > 30, hypertension | Yes | Yes | Negative | L-AmB, IVZ | Yes | No |
| H | August 2021 | 77 | m | Delta | DM, hypertension | No | No | Negative | No | No | Yes |
| I | August 2021 | 70 | m | Undetermined | DM, hypertension | Yes | No | Negative | L-AmB | Yes | Yes |
| J | September 2021 | 61 | m | Delta | No | Yes | Yes | Negative | IVZ | Yes | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guemas, E.; Cassaing, S.; Malavaud, S.; Fillaux, J.; Chauvin, P.; Lelièvre, L.; Ruiz, S.; Riu, B.; Berry, A.; Iriart, X. A Clustered Case Series of Mucorales Detection in Respiratory Samples from COVID-19 Patients in Intensive Care, France, August to September 2021. J. Fungi 2022, 8, 258. https://doi.org/10.3390/jof8030258
Guemas E, Cassaing S, Malavaud S, Fillaux J, Chauvin P, Lelièvre L, Ruiz S, Riu B, Berry A, Iriart X. A Clustered Case Series of Mucorales Detection in Respiratory Samples from COVID-19 Patients in Intensive Care, France, August to September 2021. Journal of Fungi. 2022; 8(3):258. https://doi.org/10.3390/jof8030258
Chicago/Turabian StyleGuemas, Emilie, Sophie Cassaing, Sandra Malavaud, Judith Fillaux, Pamela Chauvin, Lucie Lelièvre, Stéphanie Ruiz, Béatrice Riu, Antoine Berry, and Xavier Iriart. 2022. "A Clustered Case Series of Mucorales Detection in Respiratory Samples from COVID-19 Patients in Intensive Care, France, August to September 2021" Journal of Fungi 8, no. 3: 258. https://doi.org/10.3390/jof8030258