
Performance of a Real Time PCR for Pneumocystis jirovecii Identification in Induced Sputum of AIDS Patients: Differentiation between Pneumonia and Colonization

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. DNA Extractions and PCR Assays
2.3. 1,3-β-D-Glucan Assay
2.4. Statistical Analysis
3. Results
3.1. Efficiency and Analytical Sensitivity of the qPCR Assay
3.2. Patients Enrolled
3.3. qPCR Assay vs. Patients’ Clinical, Laboratory and Radiology Characteristics
3.4. qPCR vs. cPCR
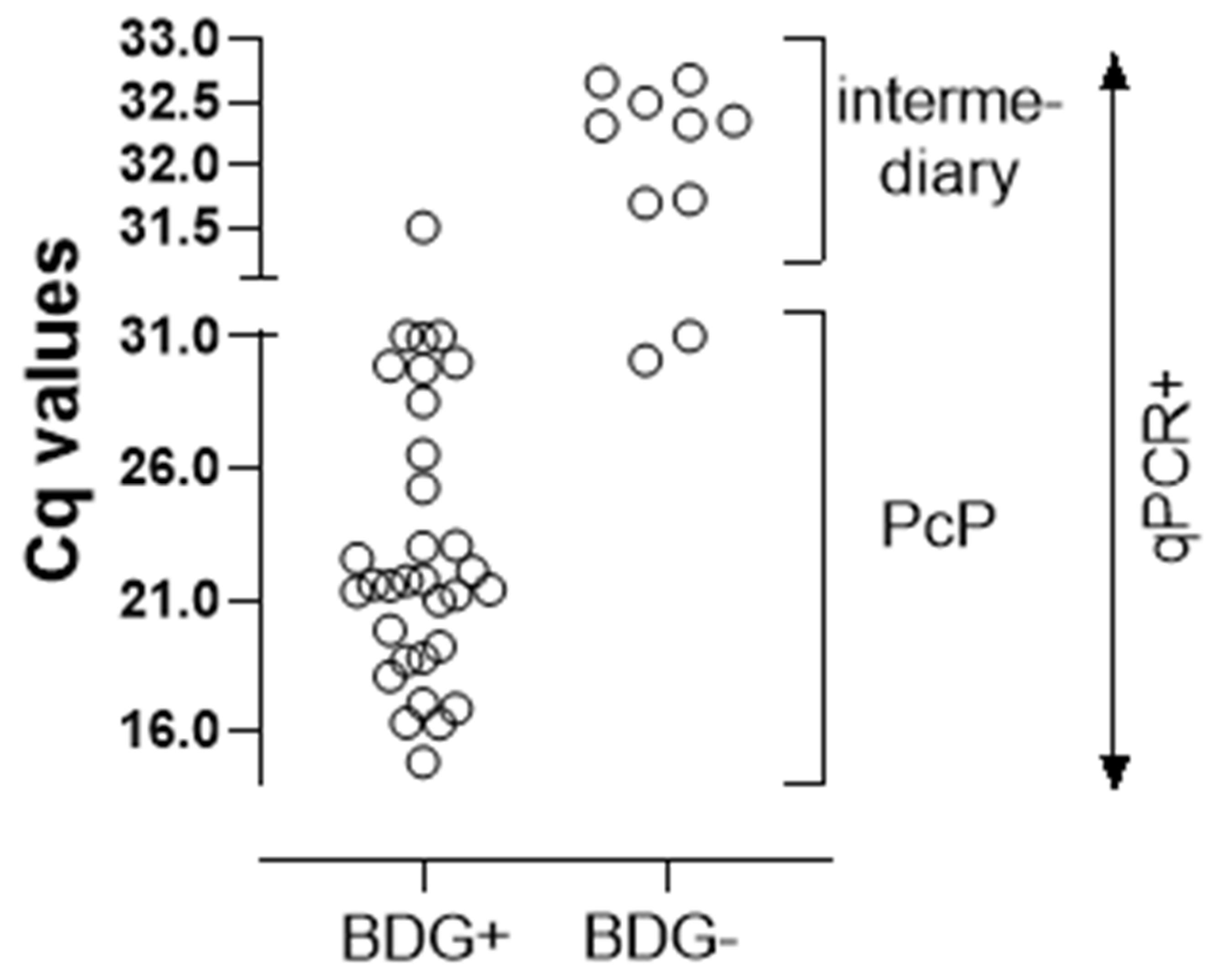
3.5. qPCR vs. BDG
3.6. Clinical, Laboratory and Radiology Characteristics of the Three Patients’ Groups Defined by the qPCR
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ford, N.; Shubber, Z.; Meintjes, G.; Grinsztejn, B.; Eholie, S.; Mills, E.J.; Davies, M.-A.; Vitoria, M.; Penazzato, M.; Nsanzimana, S.; et al. Causes of Hospital Admission among People Living with HIV Worldwide: A Systematic Review and Meta-Analysis. Lancet HIV 2015, 2, e438–e444. [Google Scholar] [CrossRef]
- Kaplan, J.E.; Hanson, D.; Dworkin, M.S.; Frederick, T.; Bertolli, J.; Lindegren, M.L.; Holmberg, S.; Jones, J.L. Epidemiology of Human Immunodeficiency Virus-Associated Opportunistic Infections in the United States in the Era of Highly Active Antiretroviral Therapy. Clin. Infect. Dis. 2000, 30, S5–S14. [Google Scholar] [CrossRef] [Green Version]
- Barbier, F.; Coquet, I.; Legriel, S.; Pavie, J.; Darmon, M.; Mayaux, J.; Molina, J.-M.; Schlemmer, B.; Azoulay, É. Etiologies and Outcome of Acute Respiratory Failure in HIV-Infected Patients. Intensive Care Med. 2009, 35, 1678–1686. [Google Scholar] [CrossRef]
- Wei, C.; Xiaojing, S.; Yanling, L.; Zhifeng, Q.; Jing, X.; Yang, H.; Wei, L. Clinical characteristics of 297 newly diagnosed Chinese HIV/AIDS patients. Chin. J. Intern. Med. 2014, 53, 537–541. [Google Scholar] [CrossRef]
- Rojanawiwat, A.; Tsuchiya, N.; Pathipvanich, P.; Pumpradit, W.; Schmidt, W.-P.; Honda, S.; Auwanit, W.; Sawanpanyalert, P.; Ariyoshi, K. Impact of the National Access to Antiretroviral Program on the Incidence of Opportunistic Infections in Thailand. Int. Health 2011, 3, 101–107. [Google Scholar] [CrossRef]
- Kaur, R.; Wadhwa, A.; Bhalla, P.; Dhakad, M.S. Pneumocystis Pneumonia in HIV Patients: A Diagnostic Challenge till Date. Med. Mycol. 2015, 53, 587–592. [Google Scholar] [CrossRef] [Green Version]
- Babic-Erceg, A.; Vilibic-Cavlek, T.; Erceg, M.; Mlinaric-Missoni, E.; Begovac, J. Prevalence of Pneumocystis jirovecii Pneumonia (2010–2013): The First Croatian Report. Acta Microbiol. Immunol. Hung. 2014, 61, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Coelho, L.; Veloso, V.G.; Grinsztejn, B.; Luz, P.M. Trends in Overall Opportunistic Illnesses, Pneumocystis Carinii Pneumonia, Cerebral Toxoplasmosis and Mycobacterium Avium Complex Incidence Rates over the 30 Years of the HIV Epidemic: A Systematic Review. Braz. J. Infect. Dis. 2014, 18, 196–210. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, L.C.; Hahn, R.C.; Favalessa, O.C.; Tadano, T.; Fontes, C.J.F. Micoses sistêmicas: Fatores associados ao óbito em pacientes com infecção pelo vírus da imunodeficiência humana, Cuiabá, Estado de Mato Grosso, 2005–2008. Rev. Soc. Bras. Med. Trop. 2009, 42, 698–705. [Google Scholar] [CrossRef] [Green Version]
- Prado, M.; da Silva, M.B.; Laurenti, R.; Travassos, L.R.; Taborda, C.P. Mortality due to systemic mycoses as a primary cause of death or in association with AIDS in Brazil: A review from 1996 to 2006. Mem. Inst. Oswaldo Cruz 2009, 104, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Nucci, M.; Queiroz-Telles, F.; Tobón, A.M.; Restrepo, A.; Colombo, A.L. Epidemiology of Opportunistic Fungal Infections in Latin America. Clin. Infect. Dis. 2010, 51, 561–570. [Google Scholar] [CrossRef]
- Ramos-e-Silva, M.; Lima, C.M.O.; Schechtman, R.C.; Trope, B.M.; Carneiro, S. Systemic Mycoses in Immunodepressed Patients (AIDS). Clin. Dermatol. 2012, 30, 616–627. [Google Scholar] [CrossRef]
- López-Sánchez, C.; Falcó, V.; Burgos, J.; Navarro, J.; Martín, M.T.; Curran, A.; Miguel, L.; Ocaña, I.; Ribera, E.; Crespo, M.; et al. Epidemiology and Long-Term Survival in HIV-Infected Patients with Pneumocystis jirovecii Pneumonia in the HAART Era: Experience in a University Hospital and Review of the Literature. Medicine 2015, 94, e681. [Google Scholar] [CrossRef]
- de Oliveira, R.B.; Atobe, J.H.; Souza, S.A.; de Castro Lima Santos, D.W. Epidemiology of Invasive Fungal Infections in Patients with Acquired Immunodeficiency Syndrome at a Reference Hospital for Infectious Diseases in Brazil. Mycopathologia 2014, 178, 71–78. [Google Scholar] [CrossRef]
- Focaccia, R.; Ribeiro, M.L.A.; Cossich, A.C.C.; de Andrade, R.F.L.; Carbonari, K.F.B.S.D.F.; Kallouf, G.A.; Vieira, R.M.R.; Gemha, J.P.L.; De Castro, A.A.; de Oliveira, J.P.C.; et al. Clinical and epidemiology evaluation of Aids-infected patients hospitalized between 2011 and 2016 in the Santos region of Brazil. Rev. Soc. Bras. Med. Trop. 2019, 52, e20180126. [Google Scholar] [CrossRef]
- Guerro, A.C.; Andretta, I.B.; Bello, S.L.; Trevisol, D.J.; Schuelter-Trevisol, F. Causes of Hospital Admission of AIDS Patients in Southern Brazil, 2007 to 2012. Rev. Soc. Bras. Med. Trop. 2014, 47, 632–636. [Google Scholar] [CrossRef] [Green Version]
- Pecego, A.; Amâncio, R.; Costa, D.; Bozza, F.; Siqueira, M.; Oliveira, M.; Cerbino-Neto, J.; Japiassu, A. Etiology, Clinical, and Epidemiological Characteristics of Severe Respiratory Infection in People Living with HIV. Int. J. STD AIDS 2020, 31, 100–108. [Google Scholar] [CrossRef]
- Dias, R.F.G.; Bento, L.O.; Tavares, C.; Ranes Filho, H.; da Silva, M.A.C.; Moraes, L.C.; Freitas-Vilela, A.A.; Moreli, M.L.; Cardoso, L.P.V. Epidemiological and Clinical Profile of HIV-Infected Patients from Southwestern Goias State, Brazil. Rev. Inst. Med. Trop. S. Paulo 2018, 60, e34. [Google Scholar] [CrossRef] [Green Version]
- Soares, V.Y.R.; Filho, C.E.P.L.; de Carvalho, L.I.M.; Silva, A.M.M.D.M.E.; Eulálio, K.D. Clinical and Epidemiological Analysis of Patients with HIV/AIDS Admitted to a Reference Hospital in the Northeast Region of Brazil. Rev. Inst. Med. Trop. S. Paulo 2008, 50, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo-Mello, C.; Naucler, P.; Negra, M.D.; Levin, A.S. Prospective Etiological Investigation of Community-Acquired Pulmonary Infections in Hospitalized People Living with HIV. Medicine 2017, 96, e5778. [Google Scholar] [CrossRef]
- Fungal Disease Frequency—Gaffi | Gaffi—Global Action for Fungal Infections. Available online: https://gaffi.org/why/fungal-disease-frequency/ (accessed on 30 January 2022).
- Rolston, K.V.; Rodriguez, S.; McRory, L.; Uribe-Botero, G.; Morice, R.; Mansell, P.W. Diagnostic Value of Induced Sputum in Patients with the Acquired Immunodeficiency Syndrome. Am. J. Med. 1988, 85, 269. [Google Scholar] [CrossRef]
- Miller, R.F.; Kocjan, G.; Buckland, J.; Holton, J.; Malin, A.; Semple, S.J. Sputum Induction for the Diagnosis of Pulmonary Disease in HIV Positive Patients. J. Infect. 1991, 23, 5–15. [Google Scholar] [CrossRef]
- Fortun, J.; Navas, E.; Marti-Belda, P.; Montilla, P.; Hermida, J.M.; Perez-Elias, M.J.; Buzon, L.; Guerrero, A. Pneumocystis Carinii Pneumonia in HIV-Infected Patients: Diagnostic Yield of Induced Sputum and Immunofluorescent Stain with Monoclonal Antibodies. Eur. Respir. J. 1992, 5, 665–669. [Google Scholar] [PubMed]
- Kovacs, J.A.; Ng, V.L.; Masur, H.; Leoung, G.; Hadley, W.K.; Evans, G.; Lane, H.C.; Ognibene, F.P.; Shelhamer, J.; Parrillo, J.E. Diagnosis of Pneumocystis Carinii Pneumonia: Improved Detection in Sputum with Use of Monoclonal Antibodies. N. Engl. J. Med. 1988, 318, 589–593. [Google Scholar] [CrossRef]
- Kroe, D.M.; Kirsch, C.M.; Jensen, W.A. Diagnostic Strategies for Pneumocystis Carinii Pneumonia. Semin. Respir. Infect. 1997, 12, 70–78. [Google Scholar]
- Linder, J.; Radio, S.J. Immunohistochemistry of Pneumocystis Carinii. Semin. Diagn. Pathol. 1989, 6, 238–244. [Google Scholar]
- Scheicher, M.E.; Terra Filho, J.; Vianna, E.O. Sputum Induction: Review of Literature and Proposal for a Protocol. Sao Paulo Med. J. 2003, 121, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Guegan, H.; Robert-Gangneux, F. Molecular Diagnosis of Pneumocystis Pneumonia in Immunocompromised Patients. Curr. Opin. Infect. Dis. 2019, 32, 314–321. [Google Scholar] [CrossRef]
- Lipschik, G.Y.; Andrawis, V.A.; Ognibene, F.P.; Kovacs, J.A.; Gill, V.J.; Nelson, N.A.; Lundgren, J.D.; Nielsen, J.O. Improved Diagnosis of Pneumocystis Carinii Infection by Polymerase Chain Reaction on Induced Sputum and Blood. Lancet 1992, 340, 203–206. [Google Scholar] [CrossRef]
- Sing, A.; Trebesius, K.; Roggenkamp, A.; Rüssmann, H.; Tybus, K.; Pfaff, F.; Bogner, J.R.; Emminger, C.; Heesemann, J. Evaluation of Diagnostic Value and Epidemiological Implications of PCR for Pneumocystis Carinii in Different Immunosuppressed and Immunocompetent Patient Groups. J. Clin. Microbiol. 2000, 38, 1461–1467. [Google Scholar] [CrossRef] [Green Version]
- Torres, J.; Goldman, M.; Wheat, L.J.; Tang, X.; Bartlett, M.S.; Smith, J.W.; Allen, S.D.; Lee, C.H. Diagnosis of Pneumocystis Carinii Pneumonia in Human Immunodeficiency Virus-Infected Patients with Polymerase Chain Reaction: A Blinded Comparison to Standard Methods. Clin. Infect. Dis. 2000, 30, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Meliani, L.; Develoux, M.; Marteau-Miltgen, M.; Magne, D.; Barbu, V.; Poirot, J.-L.; Roux, P. Real Time Quantitative PCR Assay for Pneumocystis jirovecii Detection. J. Eukaryotic. Microbiol. 2003, 50, 651. [Google Scholar] [CrossRef] [PubMed]
- Zingale, A.; Carrera, P.; Lazzarin, A.; Scarpellini, P. Detection of Pneumocystis Carinii and Characterization of Mutations Associated with Sulfa Resistance in Bronchoalveolar Lavage Samples from Human Immunodeficiency Virus-Infected Subjects. J. Clin. Microbiol. 2003, 41, 2709–2712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latouche, S.; Lacube, P.; Maury, E.; Bolognini, J.; Develoux, M.; Girard, P.; Godet, C.; Lebrette, M.; Mayaud, C.; Guillot, J.; et al. Pneumocystis jirovecii Dihydropteroate Synthase Genotypes in French Patients with Pneumocystosis: A 1998–2001 Prospective Study. Med. Mycol. 2003, 41, 533–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flori, P. Comparison between Real-Time PCR, Conventional PCR and Different Staining Techniques for Diagnosing Pneumocystis Jiroveci Pneumonia from Bronchoalveolar Lavage Specimens. J. Med. Microbiol. 2004, 53, 603–607. [Google Scholar] [CrossRef]
- Huggett, J.F.; Taylor, M.S.; Kocjan, G.; Evans, H.E.; Morris-Jones, S.; Gant, V.; Novak, T.; Costello, A.M.; Zumla, A.; Miller, R.F. Development and Evaluation of a Real-Time PCR Assay for Detection of Pneumocystis jirovecii DNA in Bronchoalveolar Lavage Fluid of HIV-Infected Patients. Thorax 2007, 63, 154–159. [Google Scholar] [CrossRef] [Green Version]
- Fan, L.-C.; Lu, H.-W.; Cheng, K.-B.; Li, H.-P.; Xu, J.-F. Evaluation of PCR in Bronchoalveolar Lavage Fluid for Diagnosis of Pneumocystis jirovecii Pneumonia: A Bivariate Meta-Analysis and Systematic Review. PLoS ONE 2013, 8, e73099. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Ling, G.; Qiang, C.; Ming, Q.; Wu, C.; Wang, K.; Ying, Z. PCR Diagnosis of Pneumocystis Pneumonia: A Bivariate Meta-Analysis. J. Clin. Microbiol. 2011, 49, 4361–4363. [Google Scholar] [CrossRef] [Green Version]
- Gits-Muselli, M.; White, P.L.; Mengoli, C.; Chen, S.; Crowley, B.; Dingemans, G.; Fréalle, E.; Gorton, R.; Guiver, M.; Hagen, F.; et al. The Fungal PCR Initiative’s Evaluation of in-House and Commercial Pneumocystis jirovecii QPCR Assays: Toward a Standard for a Diagnostics Assay. Med. Mycol. 2020, 58, 779–788. [Google Scholar] [CrossRef]
- Medrano, F.J.; Montes-Cano, M.; Conde, M.; de la Horra, C.; Respaldiza, N.; Gasch, A.; Perez-Lozano, M.J.; Varela, J.M.; Calderon, E.J. Pneumocystis jirovecii in General Population. Emerg. Infect. Dis. 2005, 11, 245–250. [Google Scholar] [CrossRef]
- Leigh, T.R.; Gazzard, B.G. DNA Amplification by the Polymerase Chain Reaction to Detect Sub-Clinical Pneumocystis Cauinil’ Colonization in HIV-Positive and HIV-Negative Male Homosexuals with and without Respiratory Symptoms. Respir. Med. 1993, 87, 525–529. [Google Scholar] [CrossRef]
- Rabodonirina, M.; Raffenot, D.; Cotte, L.; Boibieux, A.; Mayençon, M.; Bayle, G.; Persat, F.; Rabatel, F.; Trepo, C.; Peyramond, D.; et al. Rapid Detection of Pneumocystis Carinii in Bronchoalveolar Lavage Specimens from Human Immunodeficiency Virus-Infected Patients: Use of a Simple DNA Extraction Procedure and Nested PCR. J. Clin. Microbiol. 1997, 35, 2748–2751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matos, O.; Costa, M.; Lundgren, B.; Caldeira, L.; Aguiar, P.; Antunes, F. Effect of Oral Washes on the Diagnosis of Pneumocystis Carinii Pneumonia with a Low Parasite Burden and on Detection of Organisms in Subclinical Infections. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 573–575. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, A.E.; Lindley, A.R.; Ambrose, H.E.; Denis, C.; Miller, R.F. Limited Asymptomatic Carriage of Pneumocystis Jiroveci in Human Immunodeficiency Virus–Infected Patients. J. Infect. Dis. 2003, 187, 901–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maskell, N.A. Asymptomatic Carriage of Pneumocystis Jiroveci in Subjects Undergoing Bronchoscopy: A Prospective Study. Thorax 2003, 58, 594–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calderón, E.; Regordán, C.; Medrano, F.; Ollero, M.; Varela, J. Pneumocystis Carinii Infection in Patients with Chronic Bronchial Disease. Lancet 1996, 347, 977. [Google Scholar] [CrossRef]
- Respaldiza, N.; Montes-Cano, M.A.; Dapena, F.J.; de la Horra, C.; Mateos, I.; Medrano, F.J.; Calderon, E.; Varela, J.M. Prevalence of Colonisation and Genotypic Characterisation of Pneumocystis jirovecii among Cystic Fibrosis Patients in Spain. Clin. Microbiol. Infect. 2005, 11, 1012–1015. [Google Scholar] [CrossRef] [Green Version]
- Vidal, S.; de la Horra, C.; Martín, J.; Montes-Cano, M.A.; Rodríguez, E.; Respaldiza, N.; Rodríguez, F.; Varela, J.M.; Medrano, F.J.; Calderón, E.J. Pneumocystis jirovecii Colonisation in Patients with Interstitial Lung Disease. Clin. Microbiol. Infect. 2006, 12, 231–235. [Google Scholar] [CrossRef] [Green Version]
- Calderon, E.J.; Rivero, L.; Respaldiza, N.; Morilla, R.; Montes-Cano, M.A.; Friaza, V.; Munoz-Lobato, F.; Varela, J.M.; Medrano, F.J.; de la Horra, C. Systemic Inflammation in Patients with Chronic Obstructive Pulmonary Disease Who Are Colonized with Pneumocystis Jiroveci. Clin. Infect. Dis. 2007, 45, e17–e19. [Google Scholar] [CrossRef] [Green Version]
- Morris, A.; Wei, K.; Afshar, K.; Huang, L. Epidemiology and Clinical Significance of Pneumocystis Colonization. J. Infect. Dis. 2008, 197, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Matsumura, Y.; Ito, Y.; Iinuma, Y.; Yasuma, K.; Yamamoto, M.; Matsushima, A.; Nagao, M.; Takakura, S.; Ichiyama, S. Quantitative Real-Time PCR and the (1 → 3)-β-d-Glucan Assay for Differentiation between Pneumocystis jirovecii Pneumonia and Colonization. Clin. Microbiol. Infect. 2012, 18, 591–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alanio, A.; Desoubeaux, G.; Sarfati, C.; Hamane, S.; Bergeron, A.; Azoulay, E.; Molina, J.M.; Derouin, F.; Menotti, J. Real-Time PCR Assay-Based Strategy for Differentiation between Active Pneumocystis jirovecii Pneumonia and Colonization in Immunocompromised Patients. Clin. Microbiol. Infect. 2011, 17, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.R.; Marston, B.J.; Sangrujee, N.; DuPlessis, D.; Park, B. Cost-Effectiveness Analysis of Diagnostic Options for Pneumocystis Pneumonia (PCP). PLoS ONE 2011, 6, e23158. [Google Scholar] [CrossRef] [Green Version]
- Maillet, M.; Maubon, D.; Brion, J.P.; François, P.; Molina, L.; Stahl, J.P.; Epaulard, O.; Bosseray, A.; Pavese, P. Pneumocystis jirovecii (Pj) Quantitative PCR to Differentiate Pj Pneumonia from Pj Colonization in Immunocompromised Patients. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Onishi, A.; Sugiyama, D.; Kogata, Y.; Saegusa, J.; Sugimoto, T.; Kawano, S.; Morinobu, A.; Nishimura, K.; Kumagai, S. Diagnostic Accuracy of Serum 1,3-β-d-Glucan for Pneumocystis Jiroveci Pneumonia, Invasive Candidiasis, and Invasive Aspergillosis: Systematic Review and Meta-Analysis. J. Clin. Microbiol. 2012, 50, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Juniper, T.; Eades, C.P.; Gil, E.; Fodder, H.; Quinn, K.; Morris-Jones, S.; Gorton, R.L.; Wey, E.Q.; Post, F.A.; Miller, R.F. Use of β-D-Glucan in Diagnosis of Suspected Pneumocystis jirovecii Pneumonia in Adults with HIV Infection. Int. J. STD AIDS 2021, 095646242110222. [Google Scholar] [CrossRef]
- Esteves, F.; Lee, C.-H.; de Sousa, B.; Badura, R.; Seringa, M.; Fernandes, C.; Gaspar, J.F.; Antunes, F.; Matos, O. (1–3)-Beta-D-Glucan in Association with Lactate Dehydrogenase as Biomarkers of Pneumocystis Pneumonia (PcP) in HIV-Infected Patients. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1173–1180. [Google Scholar] [CrossRef]
- Cilloniz, C.; Torres, A.; Polverino, E.; Gabarrus, A.; Amaro, R.; Moreno, E.; Villegas, S.; Ortega, M.; Mensa, J.; Marcos, M.A.; et al. Community-Acquired Lung Respiratory Infections in HIV-Infected Patients: Microbial Aetiology and Outcome. Eur. Respir. J. 2014, 43, 1698–1708. [Google Scholar] [CrossRef] [Green Version]
- Bigby, T.D. Diagnosis of Pneumocystis Carinii Pneumonia. How Invasive? Chest 1994, 105, 650–652. [Google Scholar] [CrossRef]
- Chouaid, C.; Housset, B.; Lebeau, B. Cost-Analysis of Four Diagnostic Strategies for Pneumocystis Carinii Pneumonia in HIV-Infected Subjects. Eur. Respir. J. 1995, 8, 1554–1558. [Google Scholar]
- O’Brien, R.F.; Quinn, J.L.; Miyahara, B.T.; Lepoff, R.B.; Cohn, D.L. Diagnosis of Pneumocystis Carinii Pneumonia by Induced Sputum in a City with Moderate Incidence of AIDS. Chest 1989, 95, 136–138. [Google Scholar] [CrossRef] [PubMed]
- Metersky, M.L.; Aslenzadeh, J.; Stelmach, P. A Comparison of Induced and Expectorated Sputum for the Diagnosis of Pneumocystis Carinii Pneumonia. Chest 1998, 113, 1555–1559. [Google Scholar] [CrossRef] [PubMed]
- Chanez, P.; Holz, O.; Ind, P.W.; Djukanovic, R.; Maestrelli, P.; Sterk, P.J. Sputum Induction. Eur. Respir. J. 2002, 20, 3S–8S. [Google Scholar] [CrossRef]
- Khan, M.A.; Farrag, N.; Butcher, P. Diagnosis of Pneumocystis Carinii Pneumonia: Immunofluorescence Staining, Simple PCR or NPCR. J. Infect. 1999, 39, 77–80. [Google Scholar] [CrossRef]
- Del Corpo, O.; Butler-Laporte, G.; Sheppard, D.C.; Cheng, M.P.; McDonald, E.G.; Lee, T.C. Diagnostic Accuracy of Serum (1-3)-β-D-Glucan for Pneumocystis jirovecii Pneumonia: A Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2020, 26, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 20 November 2021).
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moodley, B.; Tempia, S.; Frean, J.A. Comparison of Quantitative Real-Time PCR and Direct Immunofluorescence for the Detection of Pneumocystis Jirovecii. PLoS ONE 2017, 12, e0180589. [Google Scholar] [CrossRef] [PubMed]
- Valero, C.; Buitrago, M.J.; Gits-Muselli, M.; Benazra, M.; Sturny-Leclère, A.; Hamane, S.; Guigue, N.; Bretagne, S.; Alanio, A. Copy Number Variation of Mitochondrial DNA Genes in Pneumocystis jirovecii According to the Fungal Load in BAL Specimens. Front. Microbiol. 2016, 7, 1413. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, A.E.; Pixley, F.J.; Banerji, S.; Sinclair, K.; Moxon, E.R.; Miller, R.F.; Hopkin, J.M. Detection of Pneumocystis Carinii with DNA Amplification. Lancet 1990, 336, 451–453. [Google Scholar] [CrossRef]
- Azoulay, E.; Bergeron, A.; Chevret, S.; Bele, N.; Schlemmer, B.; Menotti, J. Polymerase Chain Reaction for Diagnosing Pneumocystis Pneumonia in Non-HIV Immunocompromised Patients with Pulmonary Infiltrates. Chest 2009, 135, 655–661. [Google Scholar] [CrossRef]
- Phipps, L.M.; Chen, S.C.-A.; Kable, K.; Halliday, C.L.; Firacative, C.; Meyer, W.; Wong, G.; Nankivell, B.J. Nosocomial Pneumocystis jirovecii Pneumonia: Lessons from a Cluster in Kidney Transplant Recipients. Transplantation 2011, 92, 1327–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Prüller, F.; Raggam, R.; Divjak, M.K.; Kurath-Koller, S.; Lackner, H.; Urban, C.; Strenger, V. False Positive Serum Levels of (1-3)-ß-D-Glucan after Infusion of Intravenous Immunoglobulins and Time to Normalisation. J. Infect. 2018, 76, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Metan, G.; Koc, A.N.; Ağkuş, Ç.; Kaynar, L.G.; Alp, E.; Eser, B. Can Bacteraemia Lead to False Positive Results in 1,3-Beta-D-Glucan Test? Analysis of 83 Bacteraemia Episodes in High-Risk Patients for Invasive Fungal Infections. Rev. Iberoam. Micol. 2012, 29, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Kanamori, H.; Kanemitsu, K.; Miyasaka, T.; Ameku, K.; Endo, S.; Aoyagi, T.; Inden, K.; Hatta, M.; Yamamoto, N.; Kunishima, H.; et al. Measurement of (1-3)-Beta-D-Glucan Derived from Different Gauze Types. Tohoku. J. Exp. Med. 2009, 217, 117–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, M.; Nozu, R.; Kuramochi, T.; Eguchi, N.; Suzuki, S.; Hioki, K.; Itoh, T.; Ikeda, F. Prophylactic Effect of FK463, a Novel Antifungal Lipopeptide, against Pneumocystis Carinii Infection in Mice. Antimicrob. Agents Chemother. 2000, 44, 2259–2262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Racil, Z.; Kocmanova, I.; Lengerova, M.; Weinbergerova, B.; Buresova, L.; Toskova, M.; Winterova, J.; Timilsina, S.; Rodriguez, I.; Mayer, J. Difficulties in Using 1,3-{beta}-D-Glucan as the Screening Test for the Early Diagnosis of Invasive Fungal Infections in Patients with Haematological Malignancies--High Frequency of False-Positive Results and Their Analysis. J. Med. Microbiol. 2010, 59, 1016–1022. [Google Scholar] [CrossRef] [Green Version]
- Rogina, P.; Skvarc, M. Diagnostic Accuracy of (1→3)-β-D-Glucan to Predict Pneumocystis jirovecii Pneumonia in Non-HIV-Infected Patients. Radiol. Oncol. 2020, 54, 221–226. [Google Scholar] [CrossRef]
- Kuang, J.; Yan, X.; Genders, A.J.; Granata, C.; Bishop, D.J. An Overview of Technical Considerations When Using Quantitative Real-Time PCR Analysis of Gene Expression in Human Exercise Research. PLoS ONE 2018, 13, e0196438. [Google Scholar] [CrossRef]
- Bhat, J.; Rao, V.; Muniyandi, M.; Yadav, R.; Karforma, C.; Luke, C. Impact of Sputum Quality and Quantity on Smear and Culture Positivity: Findings from a Tuberculosis Prevalence Study in Central India. Trans. R. Soc. Trop. Med. Hyg. 2014, 108, 55–56. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| A Cq ≤ 31 (n = 32) | B 31 > Cq < 33 (n = 9) | C Cq ≥ 33 (n = 45) | p Value | |
|---|---|---|---|---|
| Male/Female | 27/5 | 6/3 | 33/12 | 0.4 |
| Age (years) | 38 ± 2.3 | 34 ± 3.7 | 41 ± 3.9 | 0.15 |
| Dry cough | 60% | 11% | 25% | A × B: 0.02 A × C: 0.004 |
| Productive cough | 40% | 89% | 75% | A × B: 0.02 A × C: 0.004 |
| Fever | 78% | 77% | 73% | 0.88 |
| PcP treatment | 90% | 11% | 28% | A × B: <0.001 A × C: <0.001 |
| Tuberculosis * | 18% | 11% | 37% | 0.09 |
| Presumed pulmonary CMV * | 25% | 0% | 11% | 0.052 |
| Presumed CABP * | 68% | 33% | 42% | A × B: 0.054 A × C: 0.027 |
| Respiratory frequency > 24 bim | 84% | 44% | 57% | A × B: 0.014 A × C: 0.013 |
| Interstitial infiltrate on X-ray | 93% | 66% | 61% | A × B: 0.028 A × C: 0.001 |
| Ground-grass on CT-scan | 93% | 42% | 38% | A × B: 0.001 A × C: <0.001 |
| beta-D-glucan > 150 pg/mL | 93% | 11% | 11% | A × B: <0.001 A × C: <0.001 |
| Days with symptoms | 43 ± 9 | 41 ± 15 | 43 ± 15 | 0.98 |
| O2 saturation (%) | 88 ± 1.5 | 91 ± 2.4 | 93 ± 2.5 | A × C: 0.01 |
| Lactic dehydrogenase (U/L) | 488 ± 49 | 219 ± 78 | 324 ± 81 | A × B: 0.004 A × C: 0.004 |
| TCD4 cells/mm3 | 40 ± 15 | 86 ± 28 | 75 ± 28 | A × C: 0.01 A × B: 0.07 |
| HIV viral load (copies/mL) | 780,289 ± 207,058 | 117,728 ± 386,509 | 304,545 ± 394,559 | A × C: 0.02 A × B: 0.07 |
| BDG (pg/mL) | 441 ± 29 | 76.3 ± 46 | 62.2 ± 48 | A × B: <0.001 A × C: <0.001 |
| PcP clinical index | 5 (4 − 5) | 1 (1 − 2) | 2 (1 − 3) | A × B: <0.001 A × C: <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chagas, O.J.; Nagatomo, P.P.; Pereira-Chioccola, V.L.; Gava, R.; Buccheri, R.; Del Negro, G.M.B.; Benard, G. Performance of a Real Time PCR for Pneumocystis jirovecii Identification in Induced Sputum of AIDS Patients: Differentiation between Pneumonia and Colonization. J. Fungi 2022, 8, 222. https://doi.org/10.3390/jof8030222
Chagas OJ, Nagatomo PP, Pereira-Chioccola VL, Gava R, Buccheri R, Del Negro GMB, Benard G. Performance of a Real Time PCR for Pneumocystis jirovecii Identification in Induced Sputum of AIDS Patients: Differentiation between Pneumonia and Colonization. Journal of Fungi. 2022; 8(3):222. https://doi.org/10.3390/jof8030222
Chicago/Turabian StyleChagas, Oscar José, Priscila Paiva Nagatomo, Vera Lucia Pereira-Chioccola, Ricardo Gava, Renata Buccheri, Gilda Maria Barbaro Del Negro, and Gil Benard. 2022. "Performance of a Real Time PCR for Pneumocystis jirovecii Identification in Induced Sputum of AIDS Patients: Differentiation between Pneumonia and Colonization" Journal of Fungi 8, no. 3: 222. https://doi.org/10.3390/jof8030222