Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections



1
Infectious Diseases Service and Institute of Microbiology, University Hospital of Lausanne, Lausanne University, 1011 Lausanne, Switzerland
2
Clinic of Infectious Diseases, S’Orsola-Malpighi Hospital, Department of Medical and Surgical Sciences, University of Bologna, 40126 Bologna, Italy
3
Department of Infectious Diseases, Infection Control and Employee Health, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA
*
Author to whom correspondence should be addressed.
†
Alternate corresponding author: Institute of Microbiology, Lausanne University Hospital (CHUV), Rue du Bugnon 48, 1011 Lausanne, Switzerland
J. Fungi 2021, 7(1), 17; https://doi.org/10.3390/jof7010017
Submission received: 2 December 2020
/
Revised: 18 December 2020
/
Accepted: 23 December 2020
/
Published: 30 December 2020
(This article belongs to the Special Issue Antifungal Resistance)
Abstract
:Invasive fungal infections (IFIs) are associated with high mortality rates and timely appropriate antifungal therapy is essential for good outcomes. Emerging antifungal resistance among Candida and Aspergillus spp., the major causes of IFI, is concerning and has led to the increasing incorporation of in vitro antifungal susceptibility testing (AST) to guide clinical decisions. However, the interpretation of AST results and their contribution to management of IFIs remains a matter of debate. Specifically, the utility of AST is limited by the delay in obtaining results and the lack of pharmacodynamic correlation between minimal inhibitory concentration (MIC) values and clinical outcome, particularly for molds. Clinical breakpoints for Candida spp. have been substantially revised over time and appear to be reliable for the detection of azole and echinocandin resistance and for outcome prediction, especially for non-neutropenic patients with candidemia. However, data are lacking for neutropenic patients with invasive candidiasis and some non-albicans Candida spp. (notably emerging Candida auris). For Aspergillus spp., AST is not routinely performed, but may be indicated according to the epidemiological context in the setting of emerging azole resistance among A. fumigatus. For non-Aspergillus molds (e.g., Mucorales, Fusarium or Scedosporium spp.), AST is not routinely recommended as interpretive criteria are lacking and many confounders, mainly host factors, seem to play a predominant role in responses to antifungal therapy. This review provides an overview of the pre-clinical and clinical pharmacodynamic data, which constitute the rationale for the use and interpretation of AST testing of yeasts and molds in clinical practice.
1. Introduction
Early appropriate antifungal therapy is a key determinant for the outcome of invasive fungal infections (IFIs). While first and alternative therapeutic choices have been well defined for the most frequent IFIs, such as invasive aspergillosis (IA) and invasive candidiasis (IC) [1,2,3,4,5], or other less frequent IFIs (e.g., mucormycosis, fusariosis, scedosporiosis) [6,7], much uncertainty remains about the role and interpretation of antifungal susceptibility testing (AST). For some fungal pathogens, antifungal susceptibility patterns are well known with limited intra-species variability (e.g., Scedosporium apiospermum). For others, the significance of minimal inhibitory concentration (MIC) in predicting outcome is notoriously weak and AST is not routinely recommended (e.g., Fusarium spp., Mucorales). However, for Candida spp. and Aspergillus spp., the two most frequent fungal pathogens, emergence of acquired antifungal resistance is a concern and definitions of clinical breakpoints (CBPs) are needed for the distinction between susceptible and resistant isolates in order to inform appropriate antifungal selection. Both the Clinical and Laboratory Standards Institute (CLSI) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) are working on establishing and updating CBPs for fungi. However, this task is complex, as illustrated by the reassessment and changes of CBPs over time, some discrepancy in CBP definitions between CLSI and EUCAST, and the absence of CBP definitions for some fungus/antifungal drug combinations (Table 1).
The aim of this article is to discuss the specific challenges of CBP definitions for the most relevant fungal pathogens of IFIs and to review the current evidence of MIC/outcome correlations.
2. The Challenges of Fungal Clinical Breakpoints (Cbps) Definitions
While often well established for antibacterials, CBPs for antifungals are associated with greater uncertainty. This is in part due to the relatively low prevalence of IFI (in particular mold infections) and some specific biological characteristics of fungal pathogens. In this section, we will review these specific aspects (summarized in Figure 1).
2.1. Antifungal Susceptibility Testing (AST) of Fungi
Some nuances of AST exist. First, the artificial in vitro conditions of testing by microbroth dilution method may differ considerably from the actual pathophysiological environment of IFIs. For example, invasive infections by molds affect mainly solid tissues (rather than biological fluids), have relatively low fungal inoculum (compared to the very high spore concentrations used in AST), and are often accompanied by tissue infarction and necrosis that might preclude appropriate drug penetration at the site of infection. In addition, the chemical composition of AST growth media differs from real pathogenic conditions regarding important elements for fungal growth (e.g., glucose, iron, oxygen, pH). Moreover, routine in vitro testing conditions do not take into account the possibility of biofilm formation (especially for Candida spp.).
Different AST methods are used in routine across countries or local laboratories. CLSI and EUCAST methods are recognized as the standard procedures and MICs derived from these methods are used for definitions of epidemiological cut-off values (ECVs) and CBPs [8,9,10,11]. CLSI and EUCAST procedures exhibit some notable differences (e.g., related to glucose content, spore inoculum, and reading interpretation), which may explain some differences between their respective CBPs. Moreover, these methods are manual and fastidious with an accepted margin of errors of up to ± two dilutions, which may considerably impact MIC classification and interpretation. As a consequence, many laboratories use commercially available microbroth dilution method (e.g., Sensititre YeastOneTM, Vitek-2TM) or alternative methods (E-tests, agar disk diffusion), which may result in significant differences in MIC results, despite relatively good essential agreements [12,13,14,15]. Important interlaboratory discrepancies have also been notified regarding AST of caspofungin for Candida spp., which resulted in the withdrawal of CBPs recommendations by EUCAST [16]. Another common issue with AST consists of the difficulties in MIC determination for some drug/fungus, which may lead to discrepant results as a consequence of different subjective interpretation from the reader. This is principally the case for antifungal drugs for which there is a fungistatic activity and a trailing effect (e.g., Candida spp. and azoles, Aspergillus spp. and echinocandins) or a paradoxical effect at increased concentrations (Candida spp. and Aspergillus spp. with echinocandins). Moreover, the timing of reading (24 vs. 48 h), which is not consistent across studies, may affect MIC determination.
Finally and most importantly, AST results for fungi are usually obtained after a significant delay due to their slower growth rate compared to bacteria (i.e., several days to one week). Their interpretation for patient management is not made in “real time” and their impact on outcome is therefore limited, since early and appropriate antifungal therapy is of paramount importance for success.
2.2. Animal Pharmacodynamic/Pharamacokinetic (Pk/Pd) Models
In view of the paucity of clinical data, murine Pk/Pd models are important for assessing the correlation between drug exposure/MIC and therapeutic response. These data are also taken into account for CBP definitions. However, an element of artificiality also exists in these in vivo models as it compares to the complex clinical scenarios of IFIs in humans. For example, much higher fungal inocula are administered to mice, an innately non-susceptible species to fungal diseases, and only following intensive immunosuppressive regimens (e.g., myelotoxic drugs and corticosteroids) in order to induce a quick and intense (rapidly fatal) infection. These conditions do not reflect the diversity of immunosuppressive and other co-morbid conditions in humans, the variety of IFI types and localizations (e.g., pulmonary vs. cerebral aspergillosis, candidemia vs. non-candidemic IC) and the actual timing and course of infection.
2.3. Pathophysiology of Invasive Fungal Infections (IFIs)
The distinct features of IFI (compared to bacterial infections) represent the most important aspect of interpreting MIC results for fungi. Mold pathogens are relatively infrequently isolated in culture and MICs are therefore lacking [17]. The diagnosis of IFI (in particular for molds) is complex and associated with some degree of uncertainty with a high rate of possible/probable infections and a lower rate of proven infections, which may bias outcome analyses towards later diagnosis when the fungal burden is high. The timing of diagnosis and initiation of antifungal therapy is also crucial and frequent delays in IFI diagnosis have a considerable impact on outcome. The localization and extension of infection may also affect the therapeutic response. For instance, drug penetration within the different organs commonly affected by IFI (e.g., lungs, brain, or skin for IA, blood, or peritoneal cavity for IC) may be quite different [18]. Most importantly, the outcome of IFI is highly influenced by non-pharmacologic parameters, such as host variables (type, severity and potential for recovery of underlying diseases and immunosuppression) or adjunct therapies such as surgical interventions.
The assessment of therapeutic response in IFI is also difficult. While objective criteria can be monitored in candidemia (e.g., clearance of blood cultures), the outcome evaluation of invasive mold infections essentially relies on radiological interpretation, which may be confounded by other infectious or non-infectious (e.g., sequela of surgery, inflammatory reaction) radiological patterns with frequent initial worsening of lesions at the time of neutrophil recovery. Moreover, the assessment of response for invasive mold infections requires prolonged follow-up (weeks to months) and overall survival may be affected by multiple intercurrent infections/events in these patients with severe underlying diseases, such as cancer.
The rarity of some IFIs makes that many clinical pharmacodynamic studies present very heterogeneous data pooling different type of IFI (IC, IA, and other IFIs) or different species within a same genus (e.g., Candida albicans and non-albicans Candida spp.) or different grading of IFI (proven/probable or possible, empiric treatment for suspected IFI without documentation). Moreover, uniform therapeutic approaches are needed for outcome analyses and IFIs often require multiple lines of different antifungal treatments or drug combinations. Because of the delay in culture results, initial antifungal therapy is usually empirical and then switched to targeted treatment.
3. Correlation between Mics and Outcome: Current Evidence
Determination of CBPs rely on ECVs derived from epidemiological studies, animal Pk/Pd models and, most importantly, clinical studies supporting the reliability of MIC in predicting outcomes. In this section, we will review the current evidence supporting a correlation between antifungal drugs MIC and clinical outcomes for the most frequent IFIs and for the three antifungal drug classes (polyenes, azoles, and echinocandins).
3.1. Invasive Candidiasis (IC)
IC is the most frequent IFI and consists of candidemia in a majority of cases, which means that there is a relatively robust set of data with documented pathogen/MIC and objectives parameters of outcome measurement, such as the clearance of candidemia. Based on these data, CBPs have been proposed by both CLSI and EUCAST for the most frequent antifungal drug/pathogen combinations (Table 1). However, most trials of candidemia, from which these data have been derived, have been performed in non-neutropenic patients. Data from candidemia in neutropenic hematologic cancer patients or from non-candidemic IC (e.g., hepato-splenic candidiasis, intra-abdominal candidiasis) are lacking [19].
3.2. Amphotericin B
Pk/Pd murine models of IC have shown that the Cmax/MIC ratio of amphotericin B (AMB) was the determinant predictor of outcome with a ratio ≥10 resulting in maximal fungicidal effect [20,21,22]. However, poor solubility of AMB at physiological pH and high degrees of protein binding of insoluble drug may create a low ceiling (<100 ng/mL) for concentration-dependent fungicidal activity in many tissues, resulting in accumulation of non-bioactive protein bound [23].
AMB is currently not a first-line treatment of IC. Analyses of MIC/outcome correlation are therefore scarce or relatively old. One study suggested a correlation for a MIC threshold of 1 mg/L [24], while another study derived from a large randomized controlled trial of AMB versus fluconazole did not found any correlation [25]. This lack of correlation was confirmed by a more recent study among 107 candidemic episodes [26]. The narrow range of MICs (0.25–1 mg/L) with a very limited number of cases with MIC ≥ 1 mg/L in these later studies may explain these negative results.
3.3. Azoles
Fluconazole is the most widely used azole for the treatment of IC, being recommended as first or second line treatment [1,2,5]. Other azoles are rarely used in this setting.
Murine models of C. albicans IC showed that a fluconazole AUC/MIC ratio >25–100 was the best parameter in predicting outcome [27,28]. For C. glabrata, murine models of IC showed overall reduced efficacy of fluconazole independently from MIC results [29,30]. For fluconazole, the 24-h serum AUC is roughly equivalent to the daily dose in patients with normal body habitus and renal function.
Mechanisms of azole resistance in Candida spp. are multiple and complex (e.g., mutations in ERG11 target gene, overexpression of target genes and/or drug transporters) [31], which can be associated with different levels of resistance, fitness, and virulence, and renders MIC interpretation more complex.
Several clinical studies have tried to correlate the Candida MICs or other composite pharmacodynamic parameters (dose/MIC, AUC/MIC) with outcome of IC (Table 2). Interpretation of these studies is confounded by heterogeneity according to the susceptibility testing method, the overall number of cases, and the rate of resistant isolates (i.e., their statistical power) and the outcome definitions (e.g., overall or attributable mortality, different composite scores of response to therapy), which could partly explain their discordant results. Most importantly, the differences in the proportion of C. albicans versus non-albicans Candida spp. (NAC) and the frequent pooled analysis of these cases represents the major confounding factor. It is also important to mention that the CLSI method and interpretive criteria have evolved over time, which precludes comparison between studies using the old CLSI method/criteria (before 2012) and those using the new ones with MIC cut-offs that are lower and closer to those from EUCAST [8,9,10,11,32].
The most recent and largest studies using the current methods (EUCAST, CLSI M38-A2, or Sensititre YeastOneTM) tend to confirm a CBP around 2 mg/L for C. albicans [33,34,35]. However, this MIC/outcome relationship is absent or less obvious in studies reporting both C. albicans and NAC cases [36,37]. Some studies limited to C. glabrata candidemia suggest that the dose/AUC or AUC/MIC ratio could be more relevant to predict efficacy for this pathogen exhibiting a wide range of fluconazole MIC and a dose-dependent response to azole therapy [37,38].
3.4. Echinocandins
The three echinocandins (caspofungin, anidulafungin, and micafungin) currently represent the first choice treatment of IC [1,2,5].
The parameters best predicting efficacy of echinocandins in murine models of IC were the Cmax/MIC and AUC/MIC ratios [44,45,46]. Caspofungin exhibits an important post-antifungal effect with persistent therapeutic concentrations in tissues [46]. The AUC/MIC targets were found to be similar for the three echinocandins when considering the free drug concentration (because of the high rate of protein binding of these drugs), but notably higher for C. albicans compared to C. glabrata or C. parapsilosis (ratios of 20 vs. 7, respectively) [47]. There is some controversy about the appropriateness of the currently recommended dosing regimens, which could not be sufficient to achieve the targeted AUC/MIC ratios, in particular, among critically-ill or neutropenic patients or in case of high body mass index [48,49,50].
For echinocandins, treatment failure has been clearly correlated to the presence of FKS hotspot mutations conferring non-susceptibility across all echinocandins, which is currently observed in about 5–10% of C. glabrata and 1–5% of C. albicans bloodstream isolates in US [51,52,53]. Overall, the rates of echinocandin treatment failure for candidemia due to FKS-mutant Candida spp. ranges from 60 to 90% [51,52,54,55], while the usual failure rate of echinocandins in the big trials of candidemia is around 10 to 30% [56,57,58,59].
Clinical studies of MIC/outcome correlation for echinocandins are shown in Table 3. Analyses derived from the caspofungin clinical trial database including several phase II and III trials of IC and Candida esophagitis did not find any correlation between echinocandin MICs and outcome [60,61]. However, these studies have been performed before the emergence of echinocandin resistance and included Candida isolates with a low and narrow MIC range. One study considering two clinical trials of micafungin for IC (total 493 cases) showed a correlation between clinical/mycological response and outcome according to the AUC/MIC ratio (cut-off 3000) and showed a trend towards improved mycological response for a micafungin MIC cut-off of <0.5 mg/L (p = 0.07) [62]. The most recent studies, including a substantial proportion of FKS mutant isolates and limited to C. glabrata (i.e., the species for which these mutations are more frequent), showed some association between MIC and outcome [51,52,55,63,64] (Table 3).
Overall, these MIC cut-offs are close to the actual CLSI CBPs, which demonstrated a good accuracy in identifying FKS mutant isolates [55,65]. Shields et al. showed that CLSI breakpoints of non-susceptibility for anidulafungin (≥0.25 mg/L) and micafungin (≥0.12 mg/L) were highly specific for the identification of FKS-mutant C. glabrata isolates and predicted treatment failure with 23–27% sensitivity and 89–98% specificity [55]. However, caspofungin CBPs appear as less reliable predictor of FKS mutations, which may be related to some methodological testing issue and interlaboratory variability of MIC results [16,55].
Whether higher echinocandin doses can overcome resistance in FKS-mutant strains remains a debated question with controversial results in murine models, suggesting that the effect could be strain-dependent and/or related to the type of mutation [66,67,68]. It is noteworthy that such FKS mutations may occur with a consequent fitness cost, which may result in decreased virulence and lower AUC/MIC ratio for efficacy in murine models [50,66,69].
In addition to the phenomenon of acquired FKS mutations among C. albicans and C. glabrata, decreased echinocandin susceptibility is observed in C. parapsilosis, which has a natural mutation at codon A661 of FKS1. However, echinocandin therapy demonstrated a global response of 60–90% for C. parapsilosis IC in large prospective comparative trials, which did not differ from that of IC due to other Candida spp. [56,57,58,59]. Finally, Fernandez-Ruiz et al. observed that initial echinocandin treatment had no impact on clinical failure among 194 cases of C. parapsilosis candidemia of a Spanish cohort [70]. One pharmacodynamic analysis showed a trend towards improved mycological response of C. parapsilosis IC to micafungin for an AUC/MIC ratio ≥285, which was about 7-fold lower than for C. albicans [62]. This might be explained by the fact that C. parapsilosis is considered as a less-virulent Candida species associated with catheter infection and for which adequate source control by catheter removal may be sufficient for clearance of the infection.
3.5. Current Issues/Pitfalls for Candida spp. AST
CLSI and EUCAST have now harmonized their CBPs for Candida spp. and azoles (Table 1). Relative robust data support the C. albicans CBP for fluconazole, while it seems less evident for NAC, in particular for C. glabrata, for which both CLSI and EUCAST abstain from a clear categorization and consider most isolates to fall in the susceptible-dose dependent or intermediate category.
For echinocandins, there is robust evidence of the association of FKS mutations among C. albicans/glabrata and failure of therapy. CLSI CBPs display acceptable reliability for their identification. Discrepancies between CLSI and EUCAST CBPs, which can be attributed to differences in testing methods, remain an important issue (Table 1). Microbiology laboratories should be aware to use the appropriate CBPs according to their testing method, in particular, regarding the widely used commercial kit Sensititre YeastOneTM, for which CLSI CBPs are recommended. Use of EUCAST criteria with this method would result in overestimation of echinocandin resistance. The role of caspofungin AST and its interpretation is still a matter of debate, and both CLSI and EUCAST recommend to rely on anidulafungin/micafungin MICs for interpretation.
The role and interpretation of AST in NAC other than C. glabrata still remain unclear. In particular, there is currently no established CBPs for emerging Candida auris, which exhibit a large variability of MIC values and a remarkable ability to rapidly induce resistance to all three antifungal drug classes [71,72]. These isolates should be tested and results interpreted using CBPs derived from other Candida spp. [72], but their actual relevance should be investigated in clinical studies.
3.6. Invasive Aspergillosis (IA)
IA and invasive mold infections in general are challenging for the assessment of CBPs because of their frequent lack of microbiological documentation and therefore of MIC data. Over 50% of IA are nowadays diagnosed on the basis of a positive galactomannan only, without recovery of the mold in culture [73]. Currently, AST is not routinely recommended for all Aspergillus isolates [4]. However, emerging pan-azole resistance among A. fumigatus makes that this practice is encouraged for documented IA [4] and raises the need to better correlate the results of AST testing with response to therapy.
3.7. Amphotericin B
Amphotericin B (AMB) formulations are still widely used for the treatment of IA, in particular, as initial pre-emptive therapy and/or in the setting of breakthrough to azole prophylaxis [3,4,74]. With the exception of A. terreus exhibiting innate resistance to AMB, and to a lesser extent A. flavus, the other common pathogenic Aspergillus spp. including A. fumigatus exhibit low and narrow ranges of MICs [75]. Acquired AMB resistance among A. fumigatus seems to be extremely rare, as it is associated with fitness cost, and its mechanisms are not well understood [76].
The Cmax/MIC was the best parameter predicting response to therapy in mice with an optimal ratio at 2.4 [77]. All formulations of AMB induce a dose-dependent response that can also be linked to the AUC/MIC, but there is very distinct concentration-response and AUC-response profiles between the three AMB formulations (deoxycholate, liposomal, and lipid complex) [78,79].
3.8. Azoles
Voriconazole is the first-line treatment of IA, while the novel triazoles isavuconazole and posaconazole represent alternative therapeutic options [3,4]. A. fumigatus, the most common cause of IA, and other pathogenic Aspergillus spp. exhibit low and narrow MIC ranges to these drugs [95,96,97].
Acquired azole resistance among A. fumigatus is an emerging issue, which is currently observed at variable incidence around the world, from <1% to 15% (e.g., in the Netherlands) [98,99]. Isolates harboring the typical TR34/L98H mutation in the cyp51A gene usually display pan-azole resistance with high MIC values (≥8 µg/mL for voriconazole) [98,100]. Other mutations have been described, with variable levels of resistance [101]. One study suggests that the proportion of A. fumigatus cyp51A-mutant isolates becomes significant (≥10%) among isolates with a MIC ≥2 mg/L for voriconazole and ≥0.5 mg/L for posaconazole [100]. Acquired azole resistance is much less frequently reported among the other common pathogenic Aspergillus spp. (A. flavus, A. niger, A. terreus), but could be an underrecognized issue [102].
In murine Pk-Pd models of IA, the AUC/MIC ratio is the most reliable index for exposure-response analyses [103,104,105,106,107,108]. A standard dosing regimen is expected to achieve appropriate exposure for efficacy against A. fumigatus isolates with a MIC ≤1 or 2 mg/L for voriconazole, ≤0.25 mg/L for posaconazole and ≤2 mg/L for isavuconazole [103,104,105,106,107,108]. These values are close to the established epidemiological cut-off values (ECVs) [95,96,97]. Pk-Pd murine models showed that the efficacy of triazoles was significantly decreased against cyp51A-mutant isolates, but could be improved with escalating doses [104,105,106,107,108].
Most clinical pharmacodynamic studies of azoles and IA have assessed the correlation between pharmacologic parameters and outcome, instead of MIC/outcome. Effectively, MIC documentation is lacking in many IA cases and, before the recent emergence of azole resistance, most A. fumigatus isolates exhibited a low and narrow range of MICs. On the contrary, azole drugs (mainly voriconazole and to some degree posaconazole) display important pharmacokinetic inter- and intra-individual variability. As the trough concentration (Ctrough) correlates with AUC [109], it can be easily monitored in clinical practice. These studies showed an association between a voriconazole Ctrough ≥1 to 2 mg/L, or a Ctrough/MIC ratio >2 to 10 and therapeutic success, but are hampered by their very heterogeneous dataset including all types of IFI (usually a mix of IA and IC) [90,91,92,93,94]. These results are however supported by an in vitro model of IA using cell culture of the human alveolus and mimicking voriconazole pharmacokinetics in humans suggesting that a Ctrough/MIC ratio of 1 to 2 is a predictor of success [104].
Studies correlating MIC/outcome and limited to IA are scarce, but are actually needed with the raising concern of emerging azole resistance. Their results are controversial (Table 4), which is mainly due to the low proportion of cyp51A mutant isolates (affecting their actual statistical power) and the confounding factor of non-azole drugs (in particular, use of amphotericin B among patients infected with azole-resistant isolates, which represents an important bias in outcome analyses). The most relevant results have been recently reported in a large Dutch cohort of IA including a high proportion of cyp51A mutant isolates and in which the majority of patients have received initial voriconazole therapy [87]. In this study, a voriconazole MIC cut-off >2 mg/L was associated with a higher mortality rate (47% vs. 24% for MIC ≤2 mg/L, p = 0.02).
The efficacy of increased azole doses for the treatment of cyp51A-mutant isolates is still an open question. One study reported an overall good response to high-dose posaconazole (targeted Ctrough > 3 mg/L) in a series of 7 IA with resistant isolates (MIC ≥ 16 mg/L, most of them with documented cyp51A mutations) [110].
In addition to acquired resistance among A. fumigatus, some rare cryptic Aspergillus spp. (e.g., A. calidoustus, A. lentulus) intrinsically exhibit decreased susceptibility to azoles [111,112,113]. Limited data are available regarding the efficacy of azoles against these cryptic Aspergillus spp. Voriconazole displayed similar efficacy than amphotericin B against Aspergillus calidoustus in a Galleria mellonella model of infection and in an retrospective outcome analysis of clinical cases, while this species usually exhibits high MICs to voriconazole (4–8 mg/L) [112,114].
3.9. Echinocandins
Echinocandins only have fungistatic activity against Aspergillus spp. and are considered as second-line or third-line therapy of IA in case of intolerance or failure of azoles or amphotericin B [3,4]. In vitro, the fungistatic effect is observed at relatively low concentrations with a very narrow range of minimal effective concentrations (MEC). Variable ECVs have been reported across studies, which actually reflects variations in methods and reading interpretation [115,116,117]. Acquired echinocandin resistance among Aspergillus spp. can result from mutation in the target gene (FKS1) and seems to be an extremely rare event as the cost of such mutations may be an important loss of fitness [118,119]. The effect of echinocandins against A. fumigatus is dose-dependent, but caspofungin may have a paradoxical effect in vitro (i.e., initial dose-dependent effect followed by loss of activity at increasing concentrations), which was also observed in murine models [120,121,122]. In a murine Pk/Pd model of IA, the caspofungin Cmax/MEC ratio appeared as the most reliable indicator with optimal efficacy at 10–20 [122].
There are no data correlating echinocandins MICs and IA outcome. Considering the narrow MIC distribution and the extreme rarity of acquired echinocandin resistance among A. fumigatus, it is unlikely that such analyses would provide any relevant conclusions.
3.10. Current Issues/Pitfalls for Aspergillus spp. AST
The MIC interpretation and CBP definitions for Aspergillus spp. continue to be a matter of uncertainty. While EUCAST has defined clinical CBPs for azoles and amphotericin B, CLSI abstains from a susceptibility/resistance categorization and only provides ECVs (Table 1). Although there is good agreement between these CBP/ECV values, some issues should be outlined.
For amphotericin B, the very narrow interval of categorization proposed by EUCAST (i.e., ≤1 mg/L susceptible, 2 mg/L intermediate and ≥4 mg/L resistant) is concerning. Effectively, these CBPs fall within the narrow range of MIC distribution of A. fumigatus (1 to 4 mg/L), and a single-dilution difference could be not significant, considering the acceptable technical variability of ± two dilutions for AST testing of molds. The concept of defining CBPs for amphotericin B and A. fumigatus is debated in the absence of established and clinically-relevant mechanisms of resistance to this drug. MIC differences in this setting are more likely to reflect technical variability.
For azoles, there is relatively good evidence to suggest that voriconazole therapy is appropriate for isolates with MIC ≤2 mg/L, provided appropriate monitoring of voriconazole concentrations for a targeted Ctrough ≥2 mg/L. Presence of cyp51A mutation actually represents the most reliable predictor of failure of azole therapy and these isolates usually exhibit high MICs (≥8 mg/L), which can be easily identified. Because therapeutic options of azole-resistant IA are very limited, the potential role of higher azole doses for a dose-dependent effect should be further investigated. However, the relatively narrow therapeutic range of azoles, especially voriconazole, represents a limitation to this approach.
For echinocandins, current data do not support a recommendation for AST and MIC interpretation. The fact that widely used commercial kits (e.g., Sensititre YeastOneTM) include echinocandin testing in their panel could be confusing for the clinicians, in particular, because of the low MICs of Aspergillus spp., which actually correspond to MECs and cannot be translated in good efficacy.
Regarding the testing methods, there is an increased use of more convenient and less time-consuming approaches, such as E-test. It should be outlined that E-test for Aspergillus spp. usually provide lower MICs (in particular for posaconazole) compared to those obtained by standard CLSI or EUCAST microbroth dilution methods [14].
3.11. Non-Aspergillus Invasive Mold Infections (NAIMIs)
NAIMIs consist mainly of invasive mucormycosis (IM), followed by disseminated fusariosis and scedosporiosis. Fungal pathogens causing these infections share the characteristics of resistance or decreased susceptibility to at least one or two of the currently available antifungal drug classes and are considered as “difficult to treat”. Some of them have a highly predictable antifungal susceptibility profile (e.g., Scedosporium spp.), but others exhibit a wide range of MIC distribution. This is notably the case for species of the order Mucorales (causal agents of IM) with respect to the broad-spectrum azoles (posaconazole and isavuconazole) and for Fusarium spp. (causal agents of fusariosis) and voriconazole [123,124,125]. To a lesser extent, variable MICs to amphotericin B are also observed for these mold species [124,125]. Despite these observations, mechanisms of acquired resistance remain largely unknown among non-Aspergillus molds.
Murine models are scarce and have failed to demonstrate a correlation between MICs and outcome for IM and fusariosis [126,127,128]. This lack of association could be partly explained by the overall poor efficacy of antifungals in these models and/or by the narrow MIC ranges of the tested strains. For Scedosporium apiospermum infection, one study in mice suggested a correlation between voriconazole MICs >2 mg/L and failure [129].
Clinical pharmacodynamic studies for NAIMIs are quasi-absent because of the rarity of the disease and the frequent lack of positive culture results, in particular for IM. One retrospective small-series of NAIMIs (consisting mainly of mucormycosis) suggested a correlation between amphotericin B MIC >0.5 mg/L and failure of therapy [130]. For fusariosis, voriconazole, despite its wide MIC distribution and frequent high MIC values (≥8 mg/L), was found to be equally effective than lipid formulations of amphotericin B (exhibiting overall lower MICs) [131,132].
Most importantly, the studies reporting factors associated with NAIMI outcomes demonstrated that non-pharmacologic factors, such as the type and duration of immunosuppression, the localization and extension of disease, the timing of appropriate antifungal therapy, and surgical interventions actually represented the best predictors of outcome [132,133,134,135].
3.12. Current Issues/Pitfalls for Non-Aspergillus Molds AST
There is no recommendation of AST testing for non-Aspergillus molds as MICs are considered as unreliable predictors of outcome and actual mechanisms of acquired resistance are unknown. Nonetheless, a wide range of MIC distribution is frequently observed, in particular for Mucorales and posaconazole/isavuconazole, and for Fusarium spp. and voriconazole. A better understanding of the causes and actual significance of these MIC variations is needed.
4. Conclusions and Perspectives
The assessment of CBPs for fungi remains a difficult task, as illustrated by the ongoing processes of revision and harmonization of the CLSI and EUCAST criteria. AST is recommended for Candida spp. (azoles and echinocandins) and Aspergillus fumigatus (azoles) isolated in invasive diseases. Notably, the mechanisms of resistance for these antifungals/pathogens are well-described (i.e., acquired mutations) and the performance of CBPs or ECVs seems acceptable for their identification with a high probability of failure of therapy. For Candida/echinocandins and Aspergillus/azoles, a single mechanism of resistance (i.e., mutations in hotspots of the target gene) seems to be by far the most clinically relevant. Therefore, genotypic rather than phenotypic characterization of the isolates might be a most reliable indicator to guide therapeutic choices. Direct identification of these mutations by PCR tools has also the considerable advantage to provide more rapid results compared to AST that requires initial positive cultures and subcultures resulting in important delays. Several PCR kits have been developed for the rapid and accurate identification of FKS mutations (for Candida spp.) or cyp51A mutations (for Aspergillus spp.) on cultures or directly on the clinical samples [136,137,138]. Albeit promising, these molecular diagnostic tools might be more costly with limited availability. Therefore, AST is expected to remain an important pillar for resistance detection.
Because of the heterogeneity of AST methods, the area of technical uncertainty and the difficulties in MIC interpretation (as mentioned above), input by mycology experts is required for the interface between the laboratory and beside in order to avoid misinterpretation. Indications for AST should also be clearly delineated and each request of fungal AST falling outside these indications should be carefully evaluated and discussed with the clinicians. Systematic AST may have an interest for epidemiological purposes and monitoring of resistance, but can also be confusing for the clinicians in the absence of expert guidance for interpretation.
The significance of MIC results should always be interpreted in a global context, taking into account the multiple parameters that can affect outcome, including host factors, the pathogenesis of the disease, the drug bioavailability, and non-pharmacologic interventions. Lack of response to therapy despite a susceptible fungal pathogen and an appropriate therapy remains a relatively frequent situation. On the contrary, a favorable response despite apparently high MIC of the fungus to the ongoing antifungal drug can also be observed. Several mechanisms that can influence clinical response (Figure 1) and that are not reflected by MIC may occur. For instance, acquired mutations of resistance are often associated with a fitness loss and decreased virulence. Heteroresistance can also occur with an undetected subpopulation of resistant clones despite apparent low MIC. Such phenomenon might be observed in patients with sanctuary sites and poor drug penetration (e.g., intra-abdominal IC, aspergilloma, or large necrotic mass in IA or IM).
Finally, several priority axes of research in this complex topic can be highlighted. On the molecular laboratory side, there is a need to improve our understanding of the clinically-relevant mechanisms of acquired resistance, in particular regarding azole resistance other than cyp51A mutations in Aspergillus and the still largely unknown mechanisms of resistance in non-Aspergillus molds. On the clinical microbiology laboratory side, efforts should be pursued for more uniform practices and interpretive criteria. On the clinical side, studies of MCI/outcome correlation should be undertaken in large multicenter cohorts of relatively homogenous patient populations, allowing for integration of potential confounding factors in multivariate analyses.
Author Contributions
Conceptualization: D.P.K. and F.L. Figure design: R.E.L. Writing: original draft preparation: F.L. Writing: review and editing: D.P.K., R.E.L. All authors have read and agreed to the published version of the manuscript.
Funding
Supported in part by the Robert C Hickey Chair in Clinical Care endowment to D.P.K. F.L. is supported by the Swiss National Science Foundation (310030_192611/1) and by the Santos-Suarez Foundation.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
D.P.K. reports honoraria, research support from Gilead Sciences; consultant fees from Astellas Pharma and Mayne, Inc and he is member of the Darrta Review Committee of Cidara Therapeutics. R.E.L. has received research support from Merck & Co and has served on advisory boards for Astellas Pharma and Cidara Therapeutics. FL has received research support from Novartis and has served on advisory boards for Gilead.
References
- Cornely, O.A.; Bassetti, M.; Calandra, T.; Garbino, J.; Kullberg, B.J.; Lortholary, O.; Meersseman, W.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S.; et al. ESCMID guideline for the diagnosis and management of Candida diseases 2012: Non-neutropenic adult patients. Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 19–37. [Google Scholar] [CrossRef] [Green Version]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R., 3rd; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Florl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24 (Suppl. 1), e1–e38. [Google Scholar] [CrossRef] [Green Version]
- Ullmann, A.J.; Akova, M.; Herbrecht, R.; Viscoli, C.; Arendrup, M.C.; Arikan-Akdagli, S.; Bassetti, M.; Bille, J.; Calandra, T.; Castagnola, E.; et al. ESCMID guideline for the diagnosis and management of Candida diseases 2012: Adults with haematological malignancies and after haematopoietic stem cell transplantation (HCT). Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 53–67. [Google Scholar] [CrossRef] [Green Version]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the european confederation of medical mycology in cooperation with the mycoses study group education and research consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Tortorano, A.M.; Richardson, M.; Roilides, E.; van Diepeningen, A.; Caira, M.; Munoz, P.; Johnson, E.; Meletiadis, J.; Pana, Z.D.; Lackner, M.; et al. Escmid and ecmm joint guidelines on diagnosis and management of hyalohyphomycosis: Fusarium spp., scedosporium spp. and others. Clin. Microbiol. Infect. 2014, 20 (Suppl. 3), 27–46. [Google Scholar] [CrossRef] [Green Version]
- CLSI. M59ed2e: Epidemiological Cut off Values for Antifungal Susceptibility Testing, 2nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- EUCAST. Mic and Zone Diameter Distributions and Ecoffs. 2018. Available online: Http://www.Eucast.Org/mic_distributions_and_ecoffs/ (accessed on 1 October 2020).
- CLSI. M60ed1e: Performance Standards for Antifungal Susceptibility Testing of Yeasts, 2nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Fourth International Supplement; CLSI Document m27-4; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2012; p. 32. [Google Scholar]
- Cuenca-Estrella, M.; Gomez-Lopez, A.; Mellado, E.; Rodriguez-Tudela, J.L. Correlation between the procedure for antifungal susceptibility testing for Candida spp. of the european committee on antibiotic susceptibility testing (eucast) and four commercial techniques. Clin. Microbiol. Infect. 2005, 11, 486–492. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Turnidge, J.; Alastruey-Izquierdo, A.; Botterel, F.; Canton, E.; Castro, C.; Chen, Y.C.; Chen, Y.; Chryssanthou, E.; Dannaoui, E.; et al. Method-dependent epidemiological cutoff values for detection of triazole resistance in candida and aspergillus species for the sensititre yeastone colorimetric broth and etest agar diffusion methods. Antimicrob. Agents Chemother. 2018, 63, e01651-18. [Google Scholar] [CrossRef] [Green Version]
- Lamoth, F.; Alexander, B.D. Comparing etest and broth microdilution for antifungal susceptibility testing of the most-relevant pathogenic molds. J. Clin. Microbiol. 2015, 53, 3176–3181. [Google Scholar] [CrossRef] [Green Version]
- Meletiadis, J.; Geertsen, E.; Curfs-Breuker, I.; Meis, J.F.; Mouton, J.W. Intra- and interlaboratory agreement in assessing the in vitro activity of micafungin against common and rare candida species with the eucast, clsi, and etest methods. Antimicrob. Agents Chemother. 2016, 60, 6173–6178. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Arendrup, M.C.; Pfaller, M.A.; Bonfietti, L.X.; Bustamante, B.; Canton, E.; Chryssanthou, E.; Cuenca-Estrella, M.; Dannaoui, E.; Fothergill, A.; et al. Interlaboratory variability of caspofungin mics for candida spp. Using clsi and eucast methods: Should the clinical laboratory be testing this agent? Antimicrob. Agents Chemother. 2013, 57, 5836–5842. [Google Scholar] [CrossRef] [Green Version]
- Tarrand, J.J.; Lichterfeld, M.; Warraich, I.; Luna, M.; Han, X.Y.; May, G.S.; Kontoyiannis, D.P. Diagnosis of invasive septate mold infections. A correlation of microbiological culture and histologic or cytologic examination. Am. J. Clin. Pathol. 2003, 119, 854–858. [Google Scholar] [CrossRef]
- Felton, T.; Troke, P.F.; Hope, W.W. Tissue penetration of antifungal agents. Clin. Microbiol. Rev. 2014, 27, 68–88. [Google Scholar] [CrossRef] [Green Version]
- Colombo, A.L.; Agnelli, C.; Kontoyiannis, D.P. Knowledge gaps in candidaemia/invasive candidiasis in haematological cancer patients. J. Antimicrob. Chemother. 2020. [Google Scholar] [CrossRef]
- Andes, D.; Safdar, N.; Marchillo, K.; Conklin, R. Pharmacokinetic-pharmacodynamic comparison of amphotericin b (amb) and two lipid-associated amb preparations, liposomal amb and amb lipid complex, in murine candidiasis models. Antimicrob. Agents Chemother. 2006, 50, 674–684. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Stamsted, T.; Conklin, R. Pharmacodynamics of amphotericin b in a neutropenic-mouse disseminated-candidiasis model. Antimicrob. Agents Chemother. 2001, 45, 922–926. [Google Scholar] [CrossRef] [Green Version]
- Takemoto, K.; Yamamoto, Y.; Ueda, Y. Evaluation of antifungal pharmacodynamic characteristics of ambisome against candida albicans. Microbiol. Immunol. 2006, 50, 579–586. [Google Scholar] [CrossRef]
- Bekersky, I.; Fielding, R.M.; Dressler, D.E.; Lee, J.W.; Buell, D.N.; Walsh, T.J. Plasma protein binding of amphotericin b and pharmacokinetics of bound versus unbound amphotericin b after administration of intravenous liposomal amphotericin b (ambisome) and amphotericin b deoxycholate. Antimicrob. Agents Chemother. 2002, 46, 834–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, M.H.; Clancy, C.J.; Yu, V.L.; Yu, Y.C.; Morris, A.J.; Snydman, D.R.; Sutton, D.A.; Rinaldi, M.G. Do in vitro susceptibility data predict the microbiologic response to amphotericin b? Results of a prospective study of patients with candida fungemia. J. Infect. Dis. 1998, 177, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Rex, J.H.; Pfaller, M.A.; Barry, A.L.; Nelson, P.W.; Webb, C.D. Antifungal susceptibility testing of isolates from a randomized, multicenter trial of fluconazole versus amphotericin b as treatment of nonneutropenic patients with candidemia. Niaid mycoses study group and the candidemia study group. Antimicrob. Agents Chemother. 1995, 39, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Park, B.J.; Arthington-Skaggs, B.A.; Hajjeh, R.A.; Iqbal, N.; Ciblak, M.A.; Lee-Yang, W.; Hairston, M.D.; Phelan, M.; Plikaytis, B.D.; Sofair, A.N.; et al. Evaluation of amphotericin b interpretive breakpoints for candida bloodstream isolates by correlation with therapeutic outcome. Antimicrob. Agents Chemother. 2006, 50, 1287–1292. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; van Ogtrop, M. Characterization and quantitation of the pharmacodynamics of fluconazole in a neutropenic murine disseminated candidiasis infection model. Antimicrob. Agents Chemother. 1999, 43, 2116–2120. [Google Scholar] [CrossRef] [Green Version]
- Louie, A.; Drusano, G.L.; Banerjee, P.; Liu, Q.F.; Liu, W.; Kaw, P.; Shayegani, M.; Taber, H.; Miller, M.H. Pharmacodynamics of fluconazole in a murine model of systemic candidiasis. Antimicrob. Agents Chemother. 1998, 42, 1105–1109. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, B.A.; Bouthet, C.; Bocanegra, R.; Correa, A.; Luther, M.F.; Graybill, J.R. Comparison of fluconazole, amphotericin b and flucytosine in treatment of a murine model of disseminated infection with candida glabrata in immunocompromised mice. J. Antimicrob Chemother. 1995, 35, 631–640. [Google Scholar] [CrossRef]
- Marine, M.; Serena, C.; Fernandez-Torres, B.; Pastor, F.J.; Guarro, J. Activities of flucytosine, fluconazole, amphotericin b, and micafungin in a murine model of disseminated infection by candida glabrata. Antimicrob. Agents Chemother. 2005, 49, 4757–4759. [Google Scholar] [CrossRef] [Green Version]
- Whaley, S.G.; Berkow, E.L.; Rybak, J.M.; Nishimoto, A.T.; Barker, K.S.; Rogers, P.D. Azole antifungal resistance in candida albicans and emerging non-albicans candida species. Front. Microbiol. 2016, 7, 2173. [Google Scholar] [CrossRef] [Green Version]
- Clinical and Laboratory Standards Institute. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Approved Standard m27-a3; Clinical and laboratory standards institute: Wayne, PA, USA, 2008. [Google Scholar]
- Brosh-Nissimov, T.; Ben-Ami, R. Differential association of fluconazole dose and dose/mic ratio with mortality in patients with candida albicans and non-albicans bloodstream infection. Clin. Microbiol. Infect. 2015, 21, 1011–1017. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Tudela, J.L.; Almirante, B.; Rodriguez-Pardo, D.; Laguna, F.; Donnelly, J.P.; Mouton, J.W.; Pahissa, A.; Cuenca-Estrella, M. Correlation of the mic and dose/mic ratio of fluconazole to the therapeutic response of patients with mucosal candidiasis and candidemia. Antimicrob. Agents Chemother. 2007, 51, 3599–3604. [Google Scholar] [CrossRef] [Green Version]
- van Hal, S.J.; Chen, S.C.; Sorrell, T.C.; Ellis, D.H.; Slavin, M.; Marriott, D.M. Support for the eucast and revised clsi fluconazole clinical breakpoints by sensititre(r) yeastone(r) for candida albicans: A prospective observational cohort study. J. Antimicrob. Chemother. 2014, 69, 2210–2214. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Ruiz, M.; Guinea, J.; Lora-Pablos, D.; Zaragoza, O.; Puig-Asensio, M.; Almirante, B.; Cuenca-Estrella, M.; Aguado, J.M.; Project, C.; Geih, G.; et al. Impact of fluconazole susceptibility on the outcome of patients with candidaemia: Data from a population-based surveillance. Clin. Microbiol. Infect. 2017, 23, 672.e1–672.e11. [Google Scholar] [CrossRef] [Green Version]
- Ghanem-Zoubi, N.; Qasum, M.; Khoury, J.; Zorbavel, D.; Arnon, M.; Geffen, Y.; Paul, M. The association between fluconazole dose and mic with mortality and persistence in candidemia. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1773–1780. [Google Scholar] [CrossRef]
- Eschenauer, G.A.; Carver, P.L.; Lin, S.W.; Klinker, K.P.; Chen, Y.C.; Potoski, B.A.; Shields, R.K.; Clancy, C.J.; Nguyen, M.H.; Lam, S.W. Fluconazole versus an echinocandin for candida glabrata fungaemia: A retrospective cohort study. J. Antimicrob. Chemother. 2013, 68, 922–926. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.C.; Fung, C.P.; Huang, J.S.; Tsai, C.J.; Chen, K.S.; Chen, H.Y.; Lee, N.; See, L.C.; Shieh, W.B. Clinical correlates of antifungal macrodilution susceptibility test results for non-aids patients with severe candida infections treated with fluconazole. Antimicrob. Agents Chemother. 2000, 44, 2715–2718. [Google Scholar] [CrossRef] [Green Version]
- Kovacicova, G.; Krupova, Y.; Lovaszova, M.; Roidova, A.; Trupl, J.; Liskova, A.; Hanzen, J.; Milosovic, P.; Lamosova, M.; Macekova, L.; et al. Antifungal susceptibility of 262 bloodstream yeast isolates from a mixed cancer and non-cancer patient population: Is there a correlation between in-vitro resistance to fluconazole and the outcome of fungemia? J. Infect. Chemother. 2000, 6, 216–221. [Google Scholar] [CrossRef]
- Clancy, C.J.; Yu, V.L.; Morris, A.J.; Snydman, D.R.; Nguyen, M.H. Fluconazole mic and the fluconazole dose/mic ratio correlate with therapeutic response among patients with candidemia. Antimicrob. Agents Chemother. 2005, 49, 3171–3177. [Google Scholar] [CrossRef] [Green Version]
- Pai, M.P.; Turpin, R.S.; Garey, K.W. Association of fluconazole area under the concentration-time curve/mic and dose/mic ratios with mortality in nonneutropenic patients with candidemia. Antimicrob. Agents Chemother. 2007, 51, 35–39. [Google Scholar] [CrossRef] [Green Version]
- Baddley, J.W.; Patel, M.; Bhavnani, S.M.; Moser, S.A.; Andes, D.R. Association of fluconazole pharmacodynamics with mortality in patients with candidemia. Antimicrob. Agents Chemother. 2008, 52, 3022–3028. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Diekema, D.J.; Pfaller, M.A.; Prince, R.A.; Marchillo, K.; Ashbeck, J.; Hou, J. In vivo pharmacodynamic characterization of anidulafungin in a neutropenic murine candidiasis model. Antimicrob. Agents Chemother. 2008, 52, 539–550. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.R.; Diekema, D.J.; Pfaller, M.A.; Marchillo, K.; Bohrmueller, J. In vivo pharmacodynamic target investigation for micafungin against candida albicans and c. Glabrata in a neutropenic murine candidiasis model. Antimicrob. Agents Chemother. 2008, 52, 3497–3503. [Google Scholar] [CrossRef] [Green Version]
- Louie, A.; Deziel, M.; Liu, W.; Drusano, M.F.; Gumbo, T.; Drusano, G.L. Pharmacodynamics of caspofungin in a murine model of systemic candidiasis: Importance of persistence of caspofungin in tissues to understanding drug activity. Antimicrob. Agents Chemother. 2005, 49, 5058–5068. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Diekema, D.J.; Pfaller, M.A.; Bohrmuller, J.; Marchillo, K.; Lepak, A. In vivo comparison of the pharmacodynamic targets for echinocandin drugs against candida species. Antimicrob. Agents Chemother. 2010, 54, 2497–2506. [Google Scholar] [CrossRef] [Green Version]
- Howard, S.J.; Livermore, J.; Sharp, A.; Goodwin, J.; Gregson, L.; Alastruey-Izquierdo, A.; Perlin, D.S.; Warn, P.A.; Hope, W.W. Pharmacodynamics of echinocandins against candida glabrata: Requirement for dosage escalation to achieve maximal antifungal activity in neutropenic hosts. Antimicrob. Agents Chemother. 2011, 55, 4880–4887. [Google Scholar] [CrossRef] [Green Version]
- Jullien, V.; Azoulay, E.; Schwebel, C.; Le Saux, T.; Charles, P.E.; Cornet, M.; Souweine, B.; Klouche, K.; Jaber, S.; Trouillet, J.L.; et al. Population pharmacokinetics of micafungin in icu patients with sepsis and mechanical ventilation. J. Antimicrob. Chemother. 2017, 72, 181–189. [Google Scholar] [CrossRef]
- Lepak, A.; Castanheira, M.; Diekema, D.; Pfaller, M.; Andes, D. Optimizing echinocandin dosing and susceptibility breakpoint determination via in vivo pharmacodynamic evaluation against candida glabrata with and without fks mutations. Antimicrob. Agents Chemother. 2012, 56, 5875–5882. [Google Scholar] [CrossRef] [Green Version]
- Alexander, B.D.; Johnson, M.D.; Pfeiffer, C.D.; Jimenez-Ortigosa, C.; Catania, J.; Booker, R.; Castanheira, M.; Messer, S.A.; Perlin, D.S.; Pfaller, M.A. Increasing echinocandin resistance in candida glabrata: Clinical failure correlates with presence of fks mutations and elevated minimum inhibitory concentrations. Clin. Infect. Dis. 2013, 56, 1724–1732. [Google Scholar] [CrossRef] [Green Version]
- Beyda, N.D.; John, J.; Kilic, A.; Alam, M.J.; Lasco, T.M.; Garey, K.W. Fks mutant candida glabrata: Risk factors and outcomes in patients with candidemia. Clin. Infect. Dis. 2014, 59, 819–825. [Google Scholar] [CrossRef] [Green Version]
- Shields, R.K.; Nguyen, M.H.; Press, E.G.; Cumbie, R.; Driscoll, E.; Pasculle, A.W.; Clancy, C.J. Rate of fks mutations among consecutive candida isolates causing bloodstream infection. Antimicrob. Agents Chemother. 2015, 59, 7465–7470. [Google Scholar] [CrossRef] [Green Version]
- Coste, A.T.; Kritikos, A.; Li, J.; Khanna, N.; Goldenberger, D.; Garzoni, C.; Zehnder, C.; Boggian, K.; Neofytos, D.; Riat, A.; et al. Emerging echinocandin-resistant candida albicans and glabrata in switzerland. Infection 2020, 48, 761–766. [Google Scholar] [CrossRef]
- Shields, R.K.; Nguyen, M.H.; Press, E.G.; Updike, C.L.; Clancy, C.J. Anidulafungin and micafungin mic breakpoints are superior to that of caspofungin for identifying fks mutant candida glabrata strains and echinocandin resistance. Antimicrob. Agents Chemother. 2013, 57, 6361–6365. [Google Scholar] [CrossRef] [Green Version]
- Kuse, E.R.; Chetchotisakd, P.; da Cunha, C.A.; Ruhnke, M.; Barrios, C.; Raghunadharao, D.; Sekhon, J.S.; Freire, A.; Ramasubramanian, V.; Demeyer, I.; et al. Micafungin versus liposomal amphotericin b for candidaemia and invasive candidosis: A phase iii randomised double-blind trial. Lancet 2007, 369, 1519–1527. [Google Scholar] [CrossRef]
- Mora-Duarte, J.; Betts, R.; Rotstein, C.; Colombo, A.L.; Thompson-Moya, L.; Smietana, J.; Lupinacci, R.; Sable, C.; Kartsonis, N.; Perfect, J.; et al. Comparison of caspofungin and amphotericin b for invasive candidiasis. N. Engl. J. Med. 2002, 347, 2020–2029. [Google Scholar] [CrossRef]
- Pappas, P.G.; Rotstein, C.M.; Betts, R.F.; Nucci, M.; Talwar, D.; De Waele, J.J.; Vazquez, J.A.; Dupont, B.F.; Horn, D.L.; Ostrosky-Zeichner, L.; et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin. Infect. Dis. 2007, 45, 883–893. [Google Scholar] [CrossRef] [Green Version]
- Reboli, A.C.; Rotstein, C.; Pappas, P.G.; Chapman, S.W.; Kett, D.H.; Kumar, D.; Betts, R.; Wible, M.; Goldstein, B.P.; Schranz, J.; et al. Anidulafungin versus fluconazole for invasive candidiasis. N. Engl. J. Med. 2007, 356, 2472–2482. [Google Scholar] [CrossRef] [Green Version]
- Kartsonis, N.; Killar, J.; Mixson, L.; Hoe, C.M.; Sable, C.; Bartizal, K.; Motyl, M. Caspofungin susceptibility testing of isolates from patients with esophageal candidiasis or invasive candidiasis: Relationship of mic to treatment outcome. Antimicrob. Agents Chemother. 2005, 49, 3616–3623. [Google Scholar] [CrossRef] [Green Version]
- Pfaller, M.A.; Diekema, D.J.; Ostrosky-Zeichner, L.; Rex, J.H.; Alexander, B.D.; Andes, D.; Brown, S.D.; Chaturvedi, V.; Ghannoum, M.A.; Knapp, C.C.; et al. Correlation of mic with outcome for candida species tested against caspofungin, anidulafungin, and micafungin: Analysis and proposal for interpretive mic breakpoints. J. Clin. Microbiol. 2008, 46, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Ambrose, P.G.; Hammel, J.P.; Van Wart, S.A.; Iyer, V.; Reynolds, D.K.; Buell, D.N.; Kovanda, L.L.; Bhavnani, S.M. Use of pharmacokinetic-pharmacodynamic analyses to optimize therapy with the systemic antifungal micafungin for invasive candidiasis or candidemia. Antimicrob. Agents Chemother. 2011, 55, 2113–2121. [Google Scholar] [CrossRef] [Green Version]
- Farmakiotis, D.; Tarrand, J.J.; Kontoyiannis, D.P. Drug-resistant candida glabrata infection in cancer patients. Emerg. Infect. Dis. 2014, 20, 1833–1840. [Google Scholar] [CrossRef] [Green Version]
- Shields, R.K.; Nguyen, M.H.; Press, E.G.; Updike, C.L.; Clancy, C.J. Caspofungin mics correlate with treatment outcomes among patients with candida glabrata invasive candidiasis and prior echinocandin exposure. Antimicrob. Agents Chemother. 2013, 57, 3528–3535. [Google Scholar] [CrossRef] [Green Version]
- Kritikos, A.; Neofytos, D.; Khanna, N.; Schreiber, P.W.; Boggian, K.; Bille, J.; Schrenzel, J.; Muhlethaler, K.; Zbinden, R.; Bruderer, T.; et al. Accuracy of sensititre yeastone echinocandins epidemiological cut-off values for identification of fks mutant candida albicans and candida glabrata: A ten year national survey of the fungal infection network of switzerland (funginos). Clin. Microbiol. Infect. 2018, 24, 1214.e1–1214.e4. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Perlin, D.S.; Jensen, R.H.; Howard, S.J.; Goodwin, J.; Hope, W. Differential in vivo activities of anidulafungin, caspofungin, and micafungin against candida glabrata isolates with and without fks resistance mutations. Antimicrob. Agents Chemother. 2012, 56, 2435–2442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slater, J.L.; Howard, S.J.; Sharp, A.; Goodwin, J.; Gregson, L.M.; Alastruey-Izquierdo, A.; Arendrup, M.C.; Warn, P.A.; Perlin, D.S.; Hope, W.W. Disseminated candidiasis caused by candida albicans with amino acid substitutions in fks1 at position ser645 cannot be successfully treated with micafungin. Antimicrob. Agents Chemother. 2011, 55, 3075–3083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiederhold, N.P.; Najvar, L.K.; Bocanegra, R.A.; Kirkpatrick, W.R.; Patterson, T.F. Caspofungin dose escalation for invasive candidiasis due to resistant candida albicans. Antimicrob. Agents Chemother. 2011, 55, 3254–3260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Ami, R.; Garcia-Effron, G.; Lewis, R.E.; Gamarra, S.; Leventakos, K.; Perlin, D.S.; Kontoyiannis, D.P. Fitness and virulence costs of candida albicans fks1 hot spot mutations associated with echinocandin resistance. J. Infect. Dis. 2011, 204, 626–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Ruiz, M.; Aguado, J.M.; Almirante, B.; Lora-Pablos, D.; Padilla, B.; Puig-Asensio, M.; Montejo, M.; Garcia-Rodriguez, J.; Peman, J.; Ruiz Perez de Pipaon, M.; et al. Initial use of echinocandins does not negatively influence outcome in candida parapsilosis bloodstream infection: A propensity score analysis. Clin. Infect. Dis. 2014, 58, 1413–1421. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F.; Kontoyiannis, D.P. The candida auris alert: Facts and perspectives. J. Infect. Dis. 2018, 217, 516–520. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous emergence of multidrug-resistant candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin. Infect. Dis. 2017, 64, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Steinbach, W.J.; Marr, K.A.; Anaissie, E.J.; Azie, N.; Quan, S.P.; Meier-Kriesche, H.U.; Apewokin, S.; Horn, D.L. Clinical epidemiology of 960 patients with invasive aspergillosis from the path alliance registry. J. Infect. 2012, 65, 453–464. [Google Scholar] [CrossRef]
- Lionakis, M.S.; Lewis, R.E.; Kontoyiannis, D.P. Breakthrough invasive mold infections in the hematology patient: Current concepts and future directions. Clin. Infect. Dis. 2018, 67, 1621–1630. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A.; Cuenca-Estrella, M.; Fothergill, A.; Fuller, J.; Ghannoum, M.; Johnson, E.; Pelaez, T.; Pfaller, M.A.; Turnidge, J. Wild-type mic distributions and epidemiological cutoff values for amphotericin b and Aspergillus spp. for the clsi broth microdilution method (m38-a2 document). Antimicrob. Agents Chemother. 2011, 55, 5150–5154. [Google Scholar] [CrossRef] [Green Version]
- Chamilos, G.; Kontoyiannis, D.P. Update on antifungal drug resistance mechanisms of aspergillus fumigatus. Drug. Resist. Updat. 2005, 8, 344–358. [Google Scholar] [CrossRef]
- Wiederhold, N.P.; Tam, V.H.; Chi, J.; Prince, R.A.; Kontoyiannis, D.P.; Lewis, R.E. Pharmacodynamic activity of amphotericin b deoxycholate is associated with peak plasma concentrations in a neutropenic murine model of invasive pulmonary aspergillosis. Antimicrob. Agents Chemother. 2006, 50, 469–473. [Google Scholar] [CrossRef] [Green Version]
- Al-Nakeeb, Z.; Petraitis, V.; Goodwin, J.; Petraitiene, R.; Walsh, T.J.; Hope, W.W. Pharmacodynamics of amphotericin b deoxycholate, amphotericin b lipid complex, and liposomal amphotericin b against aspergillus fumigatus. Antimicrob. Agents Chemother. 2015, 59, 2735–2745. [Google Scholar] [CrossRef] [Green Version]
- Lestner, J.M.; Howard, S.J.; Goodwin, J.; Gregson, L.; Majithiya, J.; Walsh, T.J.; Jensen, G.M.; Hope, W.W. Pharmacokinetics and pharmacodynamics of amphotericin b deoxycholate, liposomal amphotericin b, and amphotericin b lipid complex in an in vitro model of invasive pulmonary aspergillosis. Antimicrob. Agents Chemother. 2010, 54, 3432–3441. [Google Scholar] [CrossRef] [Green Version]
- Johnson, E.M.; Oakley, K.L.; Radford, S.A.; Moore, C.B.; Warn, P.; Warnock, D.W.; Denning, D.W. Lack of correlation of in vitro amphotericin b susceptibility testing with outcome in a murine model of aspergillus infection. J. Antimicrob. Chemother. 2000, 45, 85–93. [Google Scholar] [CrossRef]
- Manavathu, E.K.; Cutright, J.L.; Chandrasekar, P.H. In vivo resistance of a laboratory-selected aspergillus fumigatus isolate to amphotericin b. Antimicrob. Agents Chemother. 2005, 49, 428–430. [Google Scholar] [CrossRef] [Green Version]
- Verweij, P.E.; Oakley, K.L.; Morrissey, J.; Morrissey, G.; Denning, D.W. Efficacy of ly303366 against amphotericin b-susceptible and -resistant aspergillus fumigatus in a murine model of invasive aspergillosis. Antimicrob. Agents Chemother. 1998, 42, 873–878. [Google Scholar] [CrossRef] [Green Version]
- Lass-Florl, C.; Kofler, G.; Kropshofer, G.; Hermans, J.; Kreczy, A.; Dierich, M.P.; Niederwieser, D. In-vitro testing of susceptibility to amphotericin b is a reliable predictor of clinical outcome in invasive aspergillosis. J. Antimicrob. Chemother. 1998, 42, 497–502. [Google Scholar] [CrossRef] [Green Version]
- Lionakis, M.S.; Lewis, R.E.; Chamilos, G.; Kontoyiannis, D.P. Aspergillus susceptibility testing in patients with cancer and invasive aspergillosis: Difficulties in establishing correlation between in vitro susceptibility data and the outcome of initial amphotericin b therapy. Pharmacotherapy 2005, 25, 1174–1180. [Google Scholar] [CrossRef]
- Heo, S.T.; Tatara, A.M.; Jimenez-Ortigosa, C.; Jiang, Y.; Lewis, R.E.; Tarrand, J.; Tverdek, F.; Albert, N.D.; Verweij, P.E.; Meis, J.F.; et al. Changes in in vitro susceptibility patterns of aspergillus to triazoles and correlation with aspergillosis outcome in a tertiary care cancer center, 1999–2015. Clin. Infect. Dis. 2017, 65, 216–225. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.R.; Ghannoum, M.A.; Mukherjee, P.K.; Kovanda, L.L.; Lu, Q.; Jones, M.E.; Santerre Henriksen, A.; Lademacher, C.; Hope, W.W. Outcomes by mic values for patients treated with isavuconazole or voriconazole for invasive aspergillosis in the phase 3 secure and vital trials. Antimicrob. Agents Chemother. 2018, 63, e01634-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lestrade, P.P.; Bentvelsen, R.G.; Schauwvlieghe, A.; Schalekamp, S.; van der Velden, W.; Kuiper, E.J.; van Paassen, J.; van der Hoven, B.; van der Lee, H.A.; Melchers, W.J.G.; et al. Voriconazole resistance and mortality in invasive aspergillosis: A multicenter retrospective cohort study. Clin. Infect. Dis. 2019, 68, 1463–1471. [Google Scholar] [CrossRef] [Green Version]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised definitions of invasive fungal disease from the european organization for research and treatment of cancer/invasive fungal infections cooperative group and the national institute of allergy and infectious diseases mycoses study group (eortc/msg) consensus group. Clin. Infect. Dis. 2008, 46, 1813–1821. [Google Scholar] [PubMed]
- Blot, S.I.; Taccone, F.S.; Van den Abeele, A.M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Wang, T.; Wang, Y.; Yang, Q.; Xie, J.; Li, Y.; Lei, J.; Wang, X.; Xing, J.; Dong, Y.; et al. Optimization of voriconazole dosage regimen to improve the efficacy in patients with invasive fungal disease by pharmacokinetic/pharmacodynamic analysis. Fundam. Clin. Pharmacol. 2016, 30, 459–465. [Google Scholar] [CrossRef]
- Dolton, M.J.; Ray, J.E.; Chen, S.C.; Ng, K.; Pont, L.G.; McLachlan, A.J. Multicenter study of voriconazole pharmacokinetics and therapeutic drug monitoring. Antimicrob. Agents Chemother. 2012, 56, 4793–4799. [Google Scholar] [CrossRef] [Green Version]
- Pascual, A.; Calandra, T.; Bolay, S.; Buclin, T.; Bille, J.; Marchetti, O. Voriconazole therapeutic drug monitoring in patients with invasive mycoses improves efficacy and safety outcomes. Clin. Infect. Dis. 2008, 46, 201–211. [Google Scholar] [CrossRef] [Green Version]
- Pascual, A.; Csajka, C.; Buclin, T.; Bolay, S.; Bille, J.; Calandra, T.; Marchetti, O. Challenging recommended oral and intravenous voriconazole doses for improved efficacy and safety: Population pharmacokinetics-based analysis of adult patients with invasive fungal infections. Clin. Infect. Dis. 2012, 55, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Troke, P.F.; Hockey, H.P.; Hope, W.W. Observational study of the clinical efficacy of voriconazole and its relationship to plasma concentrations in patients. Antimicrob. Agents Chemother. 2011, 55, 4782–4788. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Chowdhary, A.; Gonzalez, G.M.; Lass-Florl, C.; Martin-Mazuelos, E.; Meis, J.; Pelaez, T.; Pfaller, M.A.; Turnidge, J. Multicenter study of isavuconazole mic distributions and epidemiological cutoff values for Aspergillus spp. for the clsi m38-a2 broth microdilution method. Antimicrob. Agents Chemother. 2013, 57, 3823–3828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinel-Ingroff, A.; Diekema, D.J.; Fothergill, A.; Johnson, E.; Pelaez, T.; Pfaller, M.A.; Rinaldi, M.G.; Canton, E.; Turnidge, J. Wild-type mic distributions and epidemiological cutoff values for the triazoles and six Aspergillus spp. for the clsi broth microdilution method (m38-a2 document). J. Clin. Microbiol. 2010, 48, 3251–3257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfaller, M.A.; Diekema, D.J.; Ghannoum, M.A.; Rex, J.H.; Alexander, B.D.; Andes, D.; Brown, S.D.; Chaturvedi, V.; Espinel-Ingroff, A.; Fowler, C.L.; et al. Wild-type mic distribution and epidemiological cutoff values for aspergillus fumigatus and three triazoles as determined by the clinical and laboratory standards institute broth microdilution methods. J. Clin. Microbiol. 2009, 47, 3142–3146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lestrade, P.P.A.; Buil, J.B.; van der Beek, M.T.; Kuijper, E.J.; van Dijk, K.; Kampinga, G.A.; Rijnders, B.J.A.; Vonk, A.G.; de Greeff, S.C.; Schoffelen, A.F.; et al. Paradoxal trends in azole-resistant aspergillus fumigatus in a national multicenter surveillance program, the netherlands, 2013–2018. Emerg. Infect. Dis. 2020, 26, 1447–1455. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, J.W.; Arendrup, M.C.; Warris, A.; Lagrou, K.; Pelloux, H.; Hauser, P.M.; Chryssanthou, E.; Mellado, E.; Kidd, S.E.; Tortorano, A.M.; et al. Prospective multicenter international surveillance of azole resistance in aspergillus fumigatus. Emerg. Infect. Dis. 2015, 21, 1041–1044. [Google Scholar] [CrossRef] [PubMed]
- Buil, J.B.; Hagen, F.; Chowdhary, A.; Verweij, P.E.; Meis, J.F. Itraconazole, voriconazole, and posaconazole clsi mic distributions for wild-type and azole-resistant aspergillus fumigatus isolates. J. Fungi 2018, 4, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhary, A.; Sharma, C.; Meis, J.F. Azole-resistant aspergillosis: Epidemiology, molecular mechanisms, and treatment. J. Infect. Dis. 2017, 216, S436–S444. [Google Scholar] [CrossRef] [Green Version]
- Perez-Cantero, A.; Lopez-Fernandez, L.; Guarro, J.; Capilla, J. Azole resistance mechanisms in aspergillus: Update and recent advances. Int. J. Antimicrob. Agents 2020, 55, 105807. [Google Scholar] [CrossRef]
- Howard, S.J.; Lestner, J.M.; Sharp, A.; Gregson, L.; Goodwin, J.; Slater, J.; Majithiya, J.B.; Warn, P.A.; Hope, W.W. Pharmacokinetics and pharmacodynamics of posaconazole for invasive pulmonary aspergillosis: Clinical implications for antifungal therapy. J. Infect. Dis. 2011, 203, 1324–1332. [Google Scholar] [CrossRef] [Green Version]
- Jeans, A.R.; Howard, S.J.; Al-Nakeeb, Z.; Goodwin, J.; Gregson, L.; Majithiya, J.B.; Lass-Florl, C.; Cuenca-Estrella, M.; Arendrup, M.C.; Warn, P.A.; et al. Pharmacodynamics of voriconazole in a dynamic in vitro model of invasive pulmonary aspergillosis: Implications for in vitro susceptibility breakpoints. J. Infect. Dis. 2012, 206, 442–452. [Google Scholar] [CrossRef] [Green Version]
- Lepak, A.J.; Marchillo, K.; Vanhecker, J.; Andes, D.R. Posaconazole pharmacodynamic target determination against wild-type and cyp51 mutant isolates of aspergillus fumigatus in an in vivo model of invasive pulmonary aspergillosis. Antimicrob. Agents Chemother. 2013, 57, 579–585. [Google Scholar] [CrossRef] [Green Version]
- Mavridou, E.; Bruggemann, R.J.; Melchers, W.J.; Mouton, J.W.; Verweij, P.E. Efficacy of posaconazole against three clinical aspergillus fumigatus isolates with mutations in the cyp51a gene. Antimicrob. Agents Chemother. 2010, 54, 860–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavridou, E.; Bruggemann, R.J.; Melchers, W.J.; Verweij, P.E.; Mouton, J.W. Impact of cyp51a mutations on the pharmacokinetic and pharmacodynamic properties of voriconazole in a murine model of disseminated aspergillosis. Antimicrob. Agents Chemother. 2010, 54, 4758–4764. [Google Scholar] [CrossRef] [Green Version]
- Seyedmousavi, S.; Bruggemann, R.J.; Meis, J.F.; Melchers, W.J.; Verweij, P.E.; Mouton, J.W. Pharmacodynamics of isavuconazole in an aspergillus fumigatus mouse infection model. Antimicrob. Agents Chemother. 2015, 59, 2855–2866. [Google Scholar] [CrossRef] [Green Version]
- Driscoll, T.A.; Frangoul, H.; Nemecek, E.R.; Murphey, D.K.; Yu, L.C.; Blumer, J.; Krance, R.A.; Baruch, A.; Liu, P. Comparison of pharmacokinetics and safety of voriconazole intravenous-to-oral switch in immunocompromised adolescents and healthy adults. Antimicrob. Agents Chemother. 2011, 55, 5780–5789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schauwvlieghe, A.; Buil, J.B.; Verweij, P.E.; Hoek, R.A.S.; Cornelissen, J.J.; Blijlevens, N.M.A.; Henriet, S.S.V.; Rijnders, B.J.A.; Bruggemann, R.J.M. High-dose posaconazole for azole-resistant aspergillosis and other difficult-to-treat mould infections. Mycoses 2020, 63, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Alastruey-Izquierdo, A.; Alcazar-Fuoli, L.; Cuenca-Estrella, M. Antifungal susceptibility profile of cryptic species of aspergillus. Mycopathologia 2014, 178, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Glampedakis, E.; Cassaing, S.; Fekkar, A.; Dannaoui, E.; Bougnoux, M.E.; Bretagne, S.; Neofytos, D.; Schreiber, P.W.; Hennequin, C.; Morio, F.; et al. Invasive aspergillosis due to aspergillus section usti: A multicenter retrospective study. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F. Aspergillus fumigatus-related species in clinical practice. Front. Microbiol. 2016, 7, 683. [Google Scholar] [CrossRef] [Green Version]
- Glampedakis, E.; Coste, A.T.; Aruanno, M.; Bachmann, D.; Delarze, E.; Erard, V.; Lamoth, F. Efficacy of antifungal monotherapies and combinations against aspergillus calidoustus. Antimicrob. Agents Chemother. 2018, 62, e01137-18. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Fothergill, A.; Fuller, J.; Johnson, E.; Pelaez, T.; Turnidge, J. Wild-type mic distributions and epidemiological cutoff values for caspofungin and Aspergillus spp. for the clsi broth microdilution method (m38-a2 document). Antimicrob. Agents Chemother. 2011, 55, 2855–2859. [Google Scholar] [CrossRef] [Green Version]
- Pfaller, M.A.; Boyken, L.; Hollis, R.J.; Kroeger, J.; Messer, S.A.; Tendolkar, S.; Diekema, D.J. In vitro susceptibility of clinical isolates of aspergillus spp. To anidulafungin, caspofungin, and micafungin: A head-to-head comparison using the clsi m38-a2 broth microdilution method. J. Clin. Microbiol. 2009, 47, 3323–3325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfaller, M.A.; Boyken, L.; Hollis, R.J.; Kroeger, J.; Messer, S.A.; Tendolkar, S.; Diekema, D.J. Wild-type minimum effective concentration distributions and epidemiologic cutoff values for caspofungin and Aspergillus spp. as determined by clinical and laboratory standards institute broth microdilution methods. Diagn Microbiol. Infect. Dis. 2010, 67, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Ortigosa, C.; Moore, C.; Denning, D.W.; Perlin, D.S. Emergence of echinocandin resistance due to a point mutation in the fks1 gene of aspergillus fumigatus in a patient with chronic pulmonary aspergillosis. Antimicrob. Agents Chemother. 2017, 61, e01277-17. [Google Scholar] [CrossRef] [Green Version]
- Lewis, R.E.; Liao, G.; Hou, J.; Prince, R.A.; Kontoyiannis, D.P. Comparative in vivo dose-dependent activity of caspofungin and anidulafungin against echinocandin-susceptible and -resistant aspergillus fumigatus. J. Antimicrob. Chemother. 2011, 66, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Aruanno, M.; Glampedakis, E.; Lamoth, F. Echinocandins for the treatment of invasive aspergillosis: From laboratory to bedside. Antimicrob. Agents Chemother. 2019, 63, e00399-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, R.E.; Albert, N.D.; Kontoyiannis, D.P. Comparison of the dose-dependent activity and paradoxical effect of caspofungin and micafungin in a neutropenic murine model of invasive pulmonary aspergillosis. J. Antimicrob. Chemother. 2008, 61, 1140–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiederhold, N.P.; Kontoyiannis, D.P.; Chi, J.; Prince, R.A.; Tam, V.H.; Lewis, R.E. Pharmacodynamics of caspofungin in a murine model of invasive pulmonary aspergillosis: Evidence of concentration-dependent activity. J. Infect. Dis. 2004, 190, 1464–1471. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Jensen, R.H.; Meletiadis, J. In vitro activity of isavuconazole and comparators against clinical isolates of the mucorales order. Antimicrob. Agents Chemother. 2015, 59, 7735–7742. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Chakrabarti, A.; Chowdhary, A.; Cordoba, S.; Dannaoui, E.; Dufresne, P.; Fothergill, A.; Ghannoum, M.; Gonzalez, G.M.; Guarro, J.; et al. Multicenter evaluation of mic distributions for epidemiologic cutoff value definition to detect amphotericin b, posaconazole, and itraconazole resistance among the most clinically relevant species of mucorales. Antimicrob. Agents Chemother. 2015, 59, 1745–1750. [Google Scholar] [CrossRef] [Green Version]
- Espinel-Ingroff, A.; Colombo, A.L.; Cordoba, S.; Dufresne, P.J.; Fuller, J.; Ghannoum, M.; Gonzalez, G.M.; Guarro, J.; Kidd, S.E.; Meis, J.F.; et al. International evaluation of mic distributions and epidemiological cutoff value (ecv) definitions for fusarium species identified by molecular methods for the clsi broth microdilution method. Antimicrob. Agents Chemother. 2016, 60, 1079–1084. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.S.; Gebremariam, T.; Schwartz, J.A.; Edwards, J.E., Jr.; Spellberg, B. Posaconazole mono- or combination therapy for treatment of murine zygomycosis. Antimicrob. Agents Chemother. 2009, 53, 772–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro-Rodriguez, P.; Guevara-Suarez, M.; Paredes, K.; Celis, A.; Guarro, J.; Capilla, J. Lack of correlation of ecv and outcome in an in vivo murine model of systemic fusariosis. Diagn Microbiol. Infect. Dis. 2018, 92, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Salas, V.; Pastor, F.J.; Calvo, E.; Alvarez, E.; Sutton, D.A.; Mayayo, E.; Fothergill, A.W.; Rinaldi, M.G.; Guarro, J. In vitro and in vivo activities of posaconazole and amphotericin b in a murine invasive infection by mucor circinelloides: Poor efficacy of posaconazole. Antimicrob. Agents Chemother. 2012, 56, 2246–2250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Vicente, A.; Guarro, J.; Gonzalez, G.M.; Lass-Florl, C.; Lackner, M.; Capilla, J. Voriconazole mics are predictive for the outcome of experimental disseminated scedosporiosis. J. Antimicrob. Chemother. 2017, 72, 1118–1122. [Google Scholar] [CrossRef]
- Lamoth, F.; Damonti, L.; Alexander, B.D. Role of antifungal susceptibility testing in non-aspergillus invasive mold infections. J. Clin. Microbiol. 2016, 54, 1638–1640. [Google Scholar] [CrossRef] [Green Version]
- Lortholary, O.; Obenga, G.; Biswas, P.; Caillot, D.; Chachaty, E.; Bienvenu, A.L.; Cornet, M.; Greene, J.; Herbrecht, R.; Lacroix, C.; et al. International retrospective analysis of 73 cases of invasive fusariosis treated with voriconazole. Antimicrob. Agents Chemother. 2010, 54, 4446–4450. [Google Scholar] [CrossRef] [Green Version]
- Nucci, M.; Marr, K.A.; Vehreschild, M.J.; de Souza, C.A.; Velasco, E.; Cappellano, P.; Carlesse, F.; Queiroz-Telles, F.; Sheppard, D.C.; Kindo, A.; et al. Improvement in the outcome of invasive fusariosis in the last decade. Clin. Microbiol. Infect. 2014, 20, 580–585. [Google Scholar] [CrossRef] [Green Version]
- Lamoth, F.; Kontoyiannis, D.P. Therapeutic challenges of non-aspergillus invasive mold infections in immunosuppressed patients. Antimicrob. Agents Chemother. 2019, 63, e01244-19. [Google Scholar] [CrossRef] [Green Version]
- Lanternier, F.; Dannaoui, E.; Morizot, G.; Elie, C.; Garcia-Hermoso, D.; Huerre, M.; Bitar, D.; Dromer, F.; Lortholary, O.; French Mycosis Study, G. A global analysis of mucormycosis in france: The retrozygo study (2005–2007). Clin. Infect. Dis. 2012, 54 (Suppl. 1), S35–S43. [Google Scholar] [CrossRef] [Green Version]
- Skiada, A.; Pagano, L.; Groll, A.; Zimmerli, S.; Dupont, B.; Lagrou, K.; Lass-Florl, C.; Bouza, E.; Klimko, N.; Gaustad, P.; et al. Zygomycosis in europe: Analysis of 230 cases accrued by the registry of the european confederation of medical mycology (ecmm) working group on zygomycosis between 2005 and 2007. Clin. Microbiol. Infect. 2011, 17, 1859–1867. [Google Scholar] [CrossRef] [Green Version]
- Chong, G.L.; van de Sande, W.W.; Dingemans, G.J.; Gaajetaan, G.R.; Vonk, A.G.; Hayette, M.P.; van Tegelen, D.W.; Simons, G.F.; Rijnders, B.J. Validation of a new aspergillus real-time pcr assay for direct detection of aspergillus and azole resistance of aspergillus fumigatus on bronchoalveolar lavage fluid. J. Clin. Microbiol. 2015, 53, 868–874. [Google Scholar] [CrossRef] [Green Version]
- Chong, G.M.; van der Beek, M.T.; von dem Borne, P.A.; Boelens, J.; Steel, E.; Kampinga, G.A.; Span, L.F.; Lagrou, K.; Maertens, J.A.; Dingemans, G.J.; et al. Pcr-based detection of aspergillus fumigatus cyp51a mutations on bronchoalveolar lavage: A multicentre validation of the aspergenius assay(r) in 201 patients with haematological disease suspected for invasive aspergillosis. J. Antimicrob. Chemother. 2016, 71, 3528–3535. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Nagasaki, Y.; Kordalewska, M.; Press, E.G.; Shields, R.K.; Nguyen, M.H.; Clancy, C.J.; Perlin, D.S. Rapid detection of fks-associated echinocandin resistance in candida glabrata. Antimicrob. Agents Chemother. 2016, 60, 6573–6577. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Challenges and pitfalls in the assessment of clinical breakpoints for fungi and antifungal drugs.
Figure 1.
Challenges and pitfalls in the assessment of clinical breakpoints for fungi and antifungal drugs.


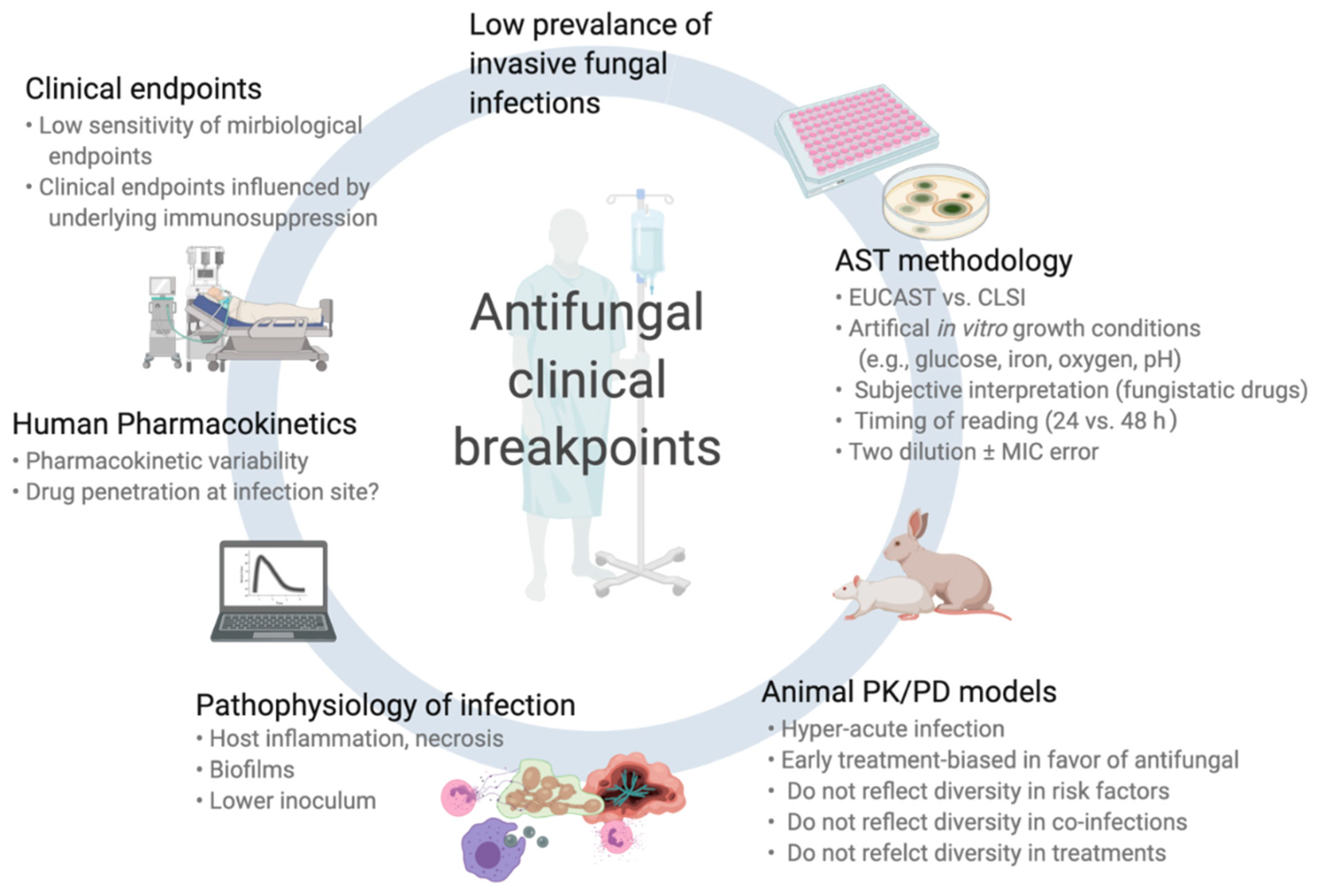{kind=link}
Table 1.
Comparison of CLSI and EUCAST clinical breakpoints of antifungal drugs for most relevant Candida and Aspergillus spp. according to CLSI and EUCAST.
Table 1.
Comparison of CLSI and EUCAST clinical breakpoints of antifungal drugs for most relevant Candida and Aspergillus spp. according to CLSI and EUCAST.
| Species | AMB | FLC | VRC | POS | CAS | AND | MCF | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C. albicans | ND | 1 | 2 (8) | 2 (8) | 0.12 (1) | 0.06 (0.5) | ND | 0.06 | 0.25 (1) | ND | 0.25 (1) | 0.03 | 0.25 (1) | 0.016 |
| C. tropicalis | ND | 1 | 2 (8) | 2 (8) | 0.12 (1) | 0.12 (0.5) | ND | 0.06 | 0.25 (1) | ND | 0.25 (1) | 0.06 | 0.25 (1) | ND |
| C. parapsilosis | ND | 1 | 2 (8) | 2 (8) | 0.12 (1) | 0.12 (0.5) | ND | 0.06 | 2 (8) | ND | 2 (8) | 0.002 (8) | 2 (8) | 0.002 (4) |
| C. glabrata | ND | 1 | 32 (SDD) (64) | 0.002 (64) | ND | ND | ND | ND | 0.12 (0.5) | ND | 0.12 (0.5) | 0.06 | 0.06 (0.25) | 0.032 |
| C. krusei | ND | 1 | (R) | (R) | 0.5 (2) | ND | ND | ND | 0.25 (1) | ND | 0.25 (1) | 0.06 | 0.25 (1) | ND |
| A. fumigatus | ND | 1 (4) | (R) | (R) | ND | 1 (4) | ND | 0.125 (0.5) | ND | ND | ND | ND | ND | ND |
| A. flavus | ND | ND | (R) | (R) | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND |
| A. niger | ND | 1 (4) | (R) | (R) | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND |
| A. terreus | (R) | (R) | (R) | (R) | ND | ND | ND | 0.125 (0.5) | ND | ND | ND | ND | ND | ND |
Clinical breakpoints (CBPs) of the Clinical and Laboratory Standards Institute (CLSI, left column) and European Committee on Antimicrobial Susceptibility Testing (EUCAST, right column). The numbers indicate the CBP [mg/L] for the distinction between susceptible “S” (≤the indicated value) vs. non-susceptible. If an intermediate “I” or “susceptible dose-dependent” (SDD) category has been defined, the resistance “R” cut-off (≥the indicated value) is mentioned in brackets. ND: no defined CBP (insufficient evidence), (R): the species is considered as intrinsically resistant (susceptibility testing not recommended).
Table 2.
Clinical studies correlating fluconazole minimal inhibitory concentrations (MIC) and outcome of invasive candidiasis (IC).
Table 2.
Clinical studies correlating fluconazole minimal inhibitory concentrations (MIC) and outcome of invasive candidiasis (IC).
| Study (First Author, Year, Reference) | N Cases | Type of IC (Patients) | Candida spp. | AST Method | Outcome Indicator | Correlation MIC/Outcome 1 | MIC Cut-Off for Success |
|---|---|---|---|---|---|---|---|
| Rex (1995) | 232 | Candidemia (non-neutropenic) | C. albicans 56% NAC 44% | NCCLS (M27-P) | Clinical response 2 | No | - |
| Lee (2000) [39] | 32 | All IC (mainly non-neutropenic) | C. albicans 53% NAC 47% | NCCLS (M27-A) | Clinical response 2 | Trend | MIC ≤ 8 mg/L |
| Kovacicova (2000) [40] | 161 | Candidemia (mixed) | C. albicans and NAC (NS) | Disk diffusion (some E-test) | Attributable mortality | Yes | “susceptible” |
| Clancy (2005) [41] | 32 | Candidemia (mixed) | C. albicans 37% NAC 63% | NCCLS (M27-A) | Clinical response 2 | Yes | MIC ≤ 8 mg/L Dose/MIC > 50 |
| Pai (2007) [42] | 77 | Candidemia (non-neutropenic) | C. albicans 64% NAC 36% | CLSI (M27-A2) | Overall mortality (hospital discharge) | Trend (MIC alone) Yes (ratios) | MIC ≤ 8 mg/L Dosewn/MIC > 12 AUC/MIC > 55 |
| Rodriguez-Tudela (2007) [34] | 126 | Candidemia (mainly non-neutropenic) | C. albicans 58% NAC 42% | EUCAST | Clinical response 2 | Yes | MIC ≤ 2 mg/L Dose/MIC ≥ 33.5 |
| Baddley (2008) [43] | 84 | Candidemia (mainly non-neutropenic) | C. albicans 44% NAC 56% | CLSI (M27-A2) | Overall mortality (week 6) | Yes | MIC ≤ 32 mg/L AUC/MIC ≥ 11.5 Dose/MIC ≥ 12.5 |
| Eschenauer (2013) [38] | 122 | Candidemia (mainly non-neutropenic) | C. glabrata | CLSI (M27-A3) | Clinical response (day 14) | Yes | Dose/MIC > 12.5 |
| Van Hal (2014) [35] | 217 | Candidemia (mainly non-neutropenic) | C. albicans | SYO | Attributable mortality (day 30) | Yes | MIC ≤1 mg/L |
| Brosh-Nissimov (2015) [33] | 75 | Candidemia (mainly non-neutropenic) | C. albicans 48% NAC 52% | E-test | Overall mortality (day 30) | Yes (C. albicans) No (NAC) | MIC ≤ 2 mg/L Dose/MIC > 400 AUC/MIC > 400 - |
| Fernandez-Ruiz (2017) [36] | 257 | Candidemia (mainly non-neutropenic) | C. albicans 54% NAC 46% | CLSI (M27-A3) EUCAST | Clinical response 2 | Trend | MIC ≤ 0.25 mg/L (CLSI) |
| Ghanem-Zoubi (2019) [37] | 158 | Candidemia (mainly non-neutropenic) | C. albicans 42% NAC 58% | E-test Vitek-2 | Overall mortality (day 30) Clinical response (day 14) | No (all species) Trend (C. glabrata) No | - AUC/MIC ≥ 400 |
IC: invasive candidiasis, AST: antifungal susceptibility testing, MIC: minimal inhibitory concentration, NAC: non-albicans Candida spp., NCCLS: National Committee for Clinical Laboratory Standards, CLSI: Clinical and Laboratory Standards Institute (former NCCLS), EUCAST: European Committee on Antimicrobial Susceptibility testing, SYO: Sensititre YeastOneTM, AUC = area under the time-concentration curve, Dosewn = dose normalized to weight, NS: not specified. 1 Assessment of correlation MIC/outcome: Yes (p < 0.05)/Trend (p < 0.2)/No (p ≥ 0.2). 2 Clinical response was usually assessed with composite parameters including clinical response, microbiological cure, overall mortality, relapsing candidemia.
Table 3.
Clinical studies correlating echinocandin minimal inhibitory concentrations (MIC) and outcome of invasive candidiasis (IC).
Table 3.
Clinical studies correlating echinocandin minimal inhibitory concentrations (MIC) and outcome of invasive candidiasis (IC).
| Study (First Author, Year, Reference) | N Cases | Type of IC (Patients) | Candida spp. | Echinocandin | AST Method | Outcome Indicator | Correlation MIC/Outcome 1 | MIC Cut-Off for Success |
|---|---|---|---|---|---|---|---|---|
| Kartsonis (2005) [60] | 114 | All IC (~70% non-neutropenic) | C. albicans 38% NAC 62% | CSF | NCCLS (M27-A) | Clinical response 2 | No | - |
| Andes (2011) [62] | 493 | All IC (~90% non-neutropenic) | C. albicans 44% NAC 56% | MCF | CLSI (M27-A) | Clinical response 2 | Yes | AUC/MIC > 3000 |
| Shields (2013) [55,64] | 66 | All IC (NS) | C. glabrata | CSF (N = 63) | CLSI (M27-A3) | Clinical response 2 | Yes Trend Trend | AND MIC ≤ 0.12 mg/L MCF MIC ≤ 0.06 mg/L CSF MIC ≤ 0.5 mg/L |
| Alexander (2013) [51] | 155 | Candidemia (mainly non-neutropenic) | C. glabrata | CSF and MCF | CLSI (M27-A3) | Clinical response 2 (day 10) | No | - |
| Farmakiotis (2014) [63] | 93 | Candidemia (~60% non-neutropenic) | C. glabrata | All (NS) | CLSI (M27-A2) | Overall mortality (day 28) | Yes | CSF MIC ≤ 0.25 mg/L |
| Beyda (2014) [52] | 57 | Candidemia (NS) | C. glabrata | MCF | SYO | Clinical response 2 (day 14) | Yes | CSF MIC ≤ 0.12 mg/L |
IC: invasive candidiasis, AST: antifungal susceptibility testing, MIC: minimal inhibitory concentration, NAC: non-albicans Candida spp., NCCLS: National Committee for Clinical Laboratory Standards, CLSI: Clinical and Laboratory Standards Institute (former NCCLS), SYO: Sensititre YeastOneTM, AND: anidulafungin, CSF: caspofungin, MCF: micafungin, NS: not specified. 1 Assessment of correlation MIC/outcome: Yes (p < 0.05)/Trend (p < 0.2)/No (p ≥ 0.2). 2 Clinical response was usually assessed with composite parameters including clinical response, microbiological cure, overall mortality, relapsing candidemia.
Table 4.
Clinical studies correlating antifungal minimal inhibitory concentrations (MIC) and outcome of invasive aspergillosis (IA).
Table 4.
Clinical studies correlating antifungal minimal inhibitory concentrations (MIC) and outcome of invasive aspergillosis (IA).
| Study (First Author, Year, Reference) | N Cases | Type of IA (Patients) | Aspergillus spp. | AF Drug | AST Method | Outcome Indicator | Correlation MIC/Outcome 1 | MIC Cut-Off for Success |
|---|---|---|---|---|---|---|---|---|
| Azoles MIC/outcomes | ||||||||
| Heo (2017) [85] | 107 | Proven/probable 2 (HEM) | A. fumigatus 49% (no cyp51A mutations 3) Others: 51% | VRC (44%) L-AmB (54%) | CLSI (M38-A2) | Overall mortality (day 42) | No | - |
| Andes (2019) [86] | 22 | Proven/probable 2 (mainly HEM) | NS | VRC | CLSI (M38-A2) EUCAST | Overall mortality (day 42) Clinical response | No | - |
| Lestrade (2019) [87] | 196 | Proven/probable or putative 2 (HEM 53%) | A. fumigatus (32 with cyp51A mutations 3) | VRC (79%) 4 | EUCAST | Overall mortality (day 42 and 90) | Yes | MIC ≤ 2 mg/L |
| Andes (2019) [86] | 49 | Proven/probable 2 (mainly HEM) | NS | ISA | CLSI (M38-A2) EUCAST | Overall mortality (day 42) Clinical response | No | - |
| Amphotericin B MIC/outcomes | ||||||||
| Lass-Flörl (1998) [83] | 29 | Proven/probable 2 (HEM) | A. flavus (12), A. terreus (9), A. fumigatus (8) | d-AmB | NCCLS (M27-P) | Overall mortality | Yes | MIC ≤ 1 mg/L |
| Lionakis (2005) [84] | 18 | Proven/probable 2 (mainly HEM) | A. terreus 33% Others: NS | L-AmB | NCCLS (M38-A) | Clinical response (day 14) | No | - |
MIC: minimal inhibitory concentration, IA: invasive aspergillosis, AF: antifungal, AST: antifungal susceptibility testing, HEM: hematologic cancer patients, VRC: voriconazole, ISA: isavuconazole, d-AmB: deoxycholate amphotericin B, L-AmB: lipid formulation of amphotericin B, EUCAST: European Committee on Antimicrobial Susceptibility testing, NCCLS: National Committee for Clinical Laboratory Standards, CLSI: Clinical and Laboratory Standards Institute (former NCCLS), NS: not specified. 1 Assessment of correlation MIC/outcome: Yes (p < 0.05)/Trend (p < 0.2)/No (p ≥ 0.2). 2 IA classification: proven/probable according to EORTC-MSG criteria (or equivalent) for immunocompromised patients [88], proven/putative according to the AspICU algorithm for intensive care units patients [89]. 3 No mutations known to be associated with azole resistance (in particular TR34/L98H or TR46/Y121F/T289A). 4 Voriconazole was the first-line AF in 79% of cases. N.B.: Only studies limited to IA are mentioned in this Table. Pharmacodynamics studies including a mix of different invasive fungal infections [90,91,92,93,94] have not been included in this Table.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lamoth, F.; Lewis, R.E.; Kontoyiannis, D.P. Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections. J. Fungi 2021, 7, 17. https://doi.org/10.3390/jof7010017
AMA Style
Lamoth F, Lewis RE, Kontoyiannis DP. Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections. Journal of Fungi. 2021; 7(1):17. https://doi.org/10.3390/jof7010017
Chicago/Turabian StyleLamoth, Frederic, Russell E. Lewis, and Dimitrios P. Kontoyiannis. 2021. "Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections" Journal of Fungi 7, no. 1: 17. https://doi.org/10.3390/jof7010017
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.