
Pneumocystis Pneumonia in Solid-Organ Transplant Recipients

 and
and
Abstract
:1. Introduction
2. Epidemiology of SOT Recipients
2.1. Incidence

{kind=link}
| Organ Transplanted | Patients not Receiving Prophylaxis | Patients Receiving Prophylaxis * | ||
|---|---|---|---|---|
| Attack Rate (%) | Reference | Attack Rate (%) | Reference | |
| Kidney | 0.6–14 | [30,32,33,34] | 0.4–2.2 a | [16,24,25,27] |
| Liver | 3–11 | [35,36,37] | 1.1–3.7 | [16,25,27,38] |
| Heart | 2–41 | [30,39,40,41] | 2–5.1 | [16,27] |
| Heart–lung/lung | 6.5–43 | [39,42] | 5–5.8 | [16,25] |
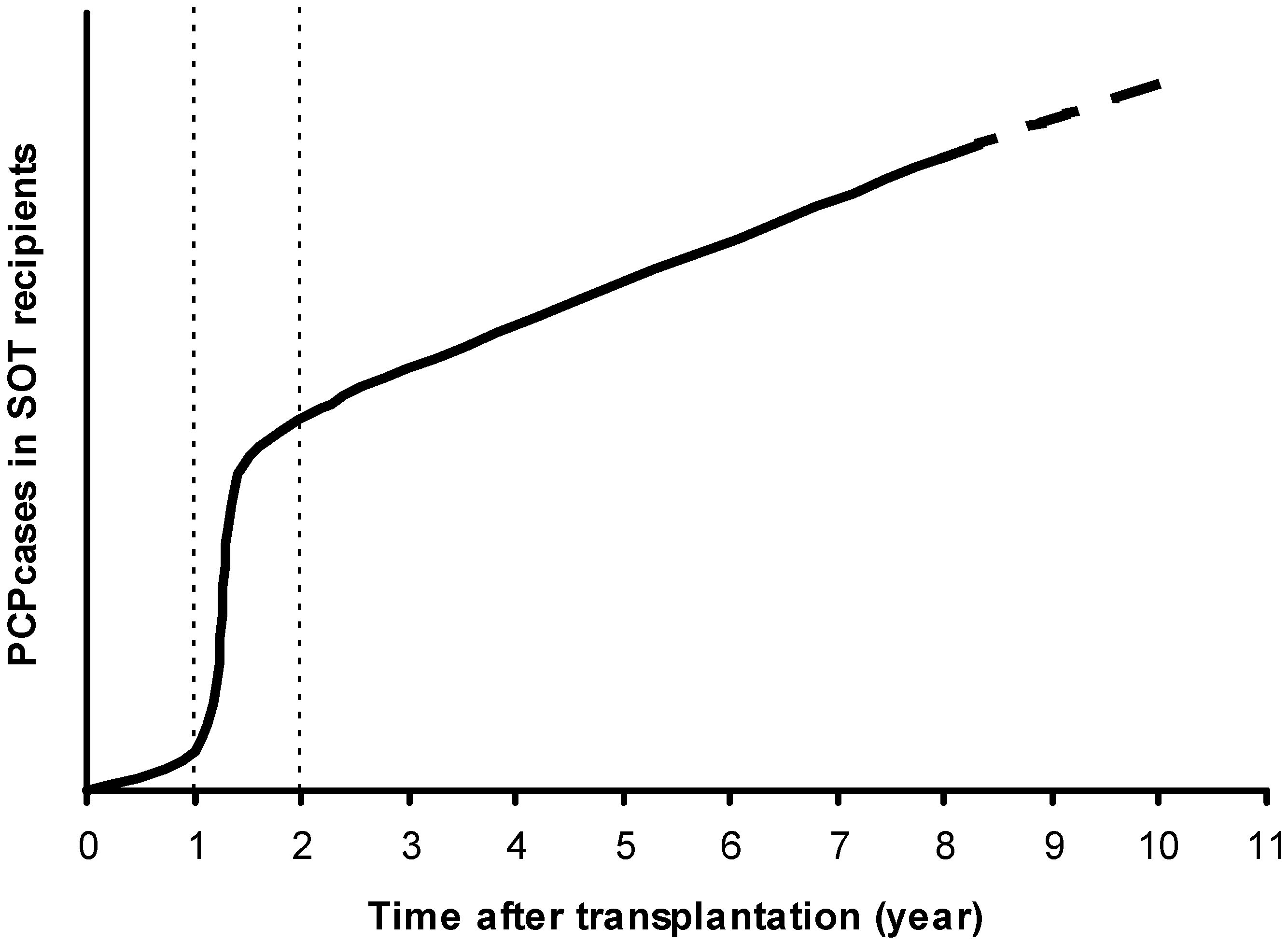
2.2. The High-Risk Period for PCP Development

2.3. Seasonal Incidence
2.4. Nosocomial Outbreaks
3. Risk Factors
3.1. Immunosuppressive Regimens
| N | PCP (%) | Controls (%) | p-Value; OR (95%CI) |
|---|---|---|---|
| 142 | 32,615 | - | |
| Induction Therapy | |||
| None | 33 (23.2) | 5922 (18.2) | 0.12 |
| Thymoglobulin | 29 (20.4) | 7783 (23.9) | 0.37 |
| IL-2 receptor antibody | 52 (36.6) | 12,389 (38.0) | 0.79 |
| Alemtuzumab | 2 (1.4) | 476 (1.5) | 0.96 |
| Discharge Immunosuppression | |||
| Tacrolimus | 79 (55.6) | 18,878 (57.9) | 0.61 |
| Cyclosporine (Neoral) | 48 (33.8) | 8755 (26.8) | 0.07 |
| Mycophenolate mofetil | 96 (67.6) | 25,415 (77.9) | 0.004 |
| Mycophenolate sodium | 0 (0) | 89 (0.3) | 0.68 |
| Azathioprine | 7 (4.9) | 900 (2.8) | 0.12 |
| Sirolimus | 41 (28.9) | 4857 (14.9) | <0.001 |
| Steroids | 124 (87.3) | 28,916 (88.7) | 0.61 |
| Discharge Immunosuppression by Combinations b | |||
| Tacrolimus and mycophenolate mofetil | 39 (27.5) | 14,715 (45.1) | Reference 1.0 |
| Tacrolimus and sirolimus | 21 (14.8) | 1861 (5.7) | <0.001; 4.26 (2.50–7.25) |
| Cyclosporine (Neoral) and mycophenolate mofetil | 39 (27.5) | 6762 (20.7) | 0.001; 2.18 (1.40–3.40) |
| Sirolimus and mycophenolate mofetil | 12 (8.5) | 1544 (4.7) | 0.001; 2.90 (1.53–5.61) |
| All other combinations | 31 (21.8) | 7733 (23.7) | 0.09; 1.51(0.94–2.42) |
3.1.1. Polyclonal/Monoclonal Antibodies
3.1.2. Corticosteroids
3.1.3. Mycophenolate Acid
3.1.4. Calcineurin Inhibitors
3.1.5. mTOR Inhibitors
3.1.6. Combinations
3.2. Acute Rejection
| Study | Prophylaxis | PCP Patients, n | Timing of Rejection (Post-Transplantation-Day) | Evaluated Criteria | Statistical Analysis | OR (95%CI) |
|---|---|---|---|---|---|---|
| Arend et al. 1996 [50] | No | 15 | 1st episode: 20 2nd episode: 34 3rd episode: 57 | No. of rejection treatment | Trend in relative risk (p = 0.002) | For 3 or more: 9.5 (1.6–56.4) |
| Radisic et al. 2003 [43] | 1 year | 17 | 1st episode: 8 2nd episode: 49 3rd episode: 62 | Rejection episode | Univ (p = 0.02) | NA |
| No. of rejection treatment | Trend in relative risk (p = 0.021) | For 3 or more: 6.3 (NA–NA) | ||||
| Type of rejection (steroid resistant) | Univ (p = 0.019) | 4.3 (1.04–18.9) | ||||
| De Castro et al. 2010 [86] | 3 months | 11 | NA | Rejection episode | Univ (p = 0.002) Multiv (p = 0.017) | 14.4 (2.1-inf) 8.7 (1.2-inf) |
| Eitner et al. 2011 [79] | No | 60 | NA | Biopsy-proven acute rejection episode | Univ (p = 0.0029) | NA |
| De Boer et al. 2011 [26] | No | 50 | 1st episode: 16 Last episode: 48 | Rejection treatment | Multiv (p = 0.002) | 5.8 (1.9–17.5) |
| No. of rejection treatment | Univ (p = 0.001) | For 3 or more: 12.9 (3.0–56.3) |
3.3. Comorbidity Conditions and Co-Infections
| Study | Prophylaxis | PCP Patients, n | Evaluated Criteria | CMV in PCP Cases, % | CMV in Controls, % | Statistical Analyses | OR (95%CI) |
|---|---|---|---|---|---|---|---|
| Arend et al. 1996 [50] | No | 15 | CMV infection | 53.3% | 18.8% | Univ (p < 0.05) | 5.0 (1.6–15.8) |
| Multiv (p < 0.05) | |||||||
| Radisic et al. 2003 [43] | 1 year | 17 | CMV infection | 52.9% | 23.5% | Univ (p = 0.036) | NA |
| Neff et al. 2009 [71] | NA | 142 | CMV disease | 20.4% | 8.8% | Univ (p < 0.001) | - |
| Multiv: NS | |||||||
| de Boer et al. 2011 [26] | No | 50 | CMV infection | NA | NA | Univ (p = 0.02) | 2.7 (1.2–6.2) |
| Multiv (p < 0.05) | 3.0 (1.2–7.9) | ||||||
| Phipps et al. 2011 [65] | 6 months | 14 | CMV disease | 35.7% | 0.6% | Univ (p < 0.001) | 65.9 (7.9–550) |
| Multiv (p < 0.001) | |||||||
| Pliquett et al. 2012 [98] | No | 29 | CMV infection and disease | 41.4% | 3.4% | Univ (p ≤ 0.05) | NA |
| Rostved et al. 2013 [94] | No a | 16 | CMV infection | 31% b 29% c | 6% b 0% c | Univ (p = 0.03) b | NA |
| Univ (p = 0.009) c | |||||||
| Iriart et al. 2015 [27] | 6 months | 33 | CMV infection | 51.5% | 18.2% | Univ (p < 0.001) | 5.2 (1.8–14.7) |
| Multiv (p = 0.002) |
3.4. Blood Parameters
3.5. Risk Period for PCP in SOT Recipients
3.6. Nosocomial Risk
3.7. Characteristics of SOT Recipients
3.8. Strategies to Target Patients at Risk for PCP
4. Clinical Manifestations and Outcomes
4.1. Clinical Manifestations
| Clinical Criteria | Reference | Frequency (%) |
|---|---|---|
| Clinical Presentation | ||
| Cough | [29,86] | 78%–100% |
| Fever | [29,86] | 67%–100% |
| Dyspnea | [29,86] | 73%–100% |
| Acute respiratory failure | [24,29,86] | 22%–69% |
| Radiological Findings | ||
| Bilateral interstitial infiltrates | [29,86] | 89%–100% |
| Unilateral infiltrate | [29] | 11% |
| Outcome | ||
| ICU admission | [26,65,79] | 8%–71% |
| Mechanical ventilation | [26,65,79] | 8%–71% |
| Death | [24,26,29,65,79,86,94] | 0%–27% |
| Death (total from all the studies) | [24,26,29,65,79,86,94] | 25/173 (14%) |
4.2. Outcomes
5. Microbiological and Radiological Diagnoses
5.1. Radiological Diagnosis
5.2. Microbiological Diagnosis
5.2.1. Samples
| Type of Sample | Reference | PCP Diagnosed (%) |
|---|---|---|
| Routine sputum | [114,135] | Poor |
| Induced sputum | [136,137] | 30–55 |
| Bronchoalveolar lavage | [137,138] | 80–95 |
| Bronchoalveolar lavage and transbronchial biopsy | [137,139] | >95 |
| Open-lung biopsy | [140] | >95 |
5.2.2. Traditional Diagnostic Methods
5.2.3. Diagnoses with the Polymerase Chain Reaction
| Study | Target Gene | Specimen (No.) | No. PCP Episodes | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|---|
| Flori et al. [146] | mtLSU rRNA | BAL (173) | 11 | 100 | 87 | NA | NA |
| Dini et al. [155] | mtLSU rRNA | Respiratory tract (932) | 150 | 100 | 83 a | 78.1 a | 100 a |
| Hauser et al. [156] | mtLSU rRNA | Respiratory tract (110) BAL (101) | 14 | 93 | 90–91 | 59–65 | 98–99 |
| Alanio et al. [152] | mtLSU rRNA | BAL (163) IS (115) | 16 | 100 | 85.7 | 72.4 a | 100 |
| Flori et al. [146] | MSG | BAL (173) | 11 | 100 | 98.6 | 84.6 a | 100 a |
| Alvarez-Martinez et al. [157] | MSG | BAL, IS (213) | 111 | 100 | 90.2 a | 82 a | 100 a |
| Fillaux et al. [153] | MSG | BAL (400) | 66 | 100 | 90.5 | 47 | 100 |
| Chumpitazi et al. [151] | MSG | BAL (66) | 18 | 100 | 97.7 | 95.5 | 100 |
6. Plasmatic Markers
7. Prophylaxis
7.1. General Considerations
7.2. Trimethoprim-Sulfamethoxazole (TMP-SMX)
| Drug | Prophylactic Regimen | Curative Regimen | Comments |
|---|---|---|---|
| Trimethoprim—sulfamethoxazole | TMP: 80–160 mg—SMX: 400–800 mg, daily p.o. or IV TMP: 160 mg—SMX: 800 mg, 3 times weekly p.o. or IV | TMP: 15–20 mg/kg—SMX: 75–100 mg/kg, IV or p.o., divided into 3–4 doses daily | Contraindication in cases of allergy to sulfa drugs. Adverse effects: Cytopenia, skin reactions, hepatitis, pancreatitis, gastrointestinal disturbance, renal insufficiency, hyperkalemia, anaphylaxis. Interaction with cyclosporine: increase of creatinine level with possible decrease of cyclosporine plasmatic concentrations. |
| Dapsone | 50–100 mg, daily p.o. | - | Contraindication in cases of G6PD deficiency. Possible cross-reaction with sulfa allergy. Adverse effects: methemoglobinemia, anemia, skin rash, gastrointestinal disturbance, agranulocytosis |
| Atovaquone | 750 mg, 2 times daily p.o. | 750 mg, 2–3 times daily p.o. | Variable oral absorption. Adverse effects: skin rash, fever, gastrointestinal disturbance, hepatitis |
| Pentamidine | 300 mg, monthly administered through aerosolized nebulizer | 4 mg/kg, daily IV | Adverse effects: pancreatitis, hypo- or hyperglycemia, bone-marrow suppression, renal insufficiency, cardiac arrhythmias, electrolyte disorders, hypotension, hepatitis. Interaction with others nephrotoxic drugs, increasing renal toxicity, particularly cyclosporine or tacrolimus |
| Dapsone + trimethoprime | - | Dapsone: 100 mg, daily p.o. Trimethoprime: 5 mg/kg, 3 times daily | Contraindication in cases of G6PD deficiency. Possible cross-reaction with sulfa allergy. Adverse effects : methemoglobinemia, skin rash, fever, gastrointestinal disturbance |
| Clindamycin + primaquine | - | Clindamycin: 600 mg, 4 times daily IV or 350–400 mg, 4 times daily p.o. Primaquine: 15–30 mg daily p.o. | Contraindication in cases of G6PD deficiency. Adverse effects: skin rash, fever, neutropenia, gastrointestinal disturbance, methemoglobinemia. Interaction with cyclosporine: possible decrease of cyclosporine plasmatic concentrations. |
7.3. Other Chemoprophylactic Agents
7.3.1. Dapsone
7.3.2. Atovaquone
7.3.3. Pentamidine
7.3.4. Other Agents or Combinations
7.4. Prophylaxis and Nosocomial Infections
8. Treatments
8.1. Anti-Pneumocystis Agents
8.1.1. Trimethoprim-Sulfamethoxazole (TMP-SMX)
8.1.2. Other Agents
8.2. Adjuvant Corticosteroids
8.3. Reduction in Immunosuppressive Medications
9. Conclusions
Acknowledgments
Conflicts of Interest
References
- Roblot, F.; Godet, C.; le Moal, G.; Garo, B.; Faouzi Souala, M.; Dary, M.; de Gentile, L.; Gandji, J.A.; Guimard, Y.; Lacroix, C.; et al. Analysis of underlying diseases and prognosis factors associated with Pneumocystis carinii pneumonia in immunocompromised HIV-negative patients. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 523–531. [Google Scholar] [PubMed]
- Sepkowitz, K.A. Opportunistic infections in patients with and patients without Acquired Immunodeficiency Syndrome. Clin. Infect. Dis. 2002, 34, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Chabe, M.; Durand-Joly, I.; Dei-Cas, E. Transmission of Pneumocystis infection in humans. Med. Sci 2012, 28, 599–604. [Google Scholar]
- Hughes, W.T. Natural mode of acquisition for de novo infection with Pneumocystis carinii. J. Infect. Dis. 1982, 145, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Cushion, M.T.; Linke, M.J.; Ashbaugh, A.; Sesterhenn, T.; Collins, M.S.; Lynch, K.; Brubaker, R.; Walzer, P.D. Echinocandin treatment of Pneumocystis pneumonia in rodent models depletes cysts leaving trophic burdens that cannot transmit the infection. PLoS ONE 2010, 5, e8524. [Google Scholar] [CrossRef] [PubMed]
- Martinez, A.; Halliez, M.C.; Aliouat el, M.; Chabe, M.; Standaert-Vitse, A.; Frealle, E.; Gantois, N.; Pottier, M.; Pinon, A.; Dei-Cas, E.; et al. Growth and airborne transmission of cell-sorted life cycle stages of Pneumocystis carinii. PLoS ONE 2013, 8, e79958. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.F.; Ambrose, H.E.; Wakefield, A.E. Pneumocystis carinii f. sp. hominis DNA in immunocompetent health care workers in contact with patients with P. carinii pneumonia. J. Clin. Microbiol. 2001, 39, 3877–3882. [Google Scholar]
- Manoloff, E.S.; Francioli, P.; Taffe, P.; Van Melle, G.; Bille, J.; Hauser, P.M. Risk for Pneumocystis carinii transmission among patients with pneumonia: A molecular epidemiology study. Emerg. Infect. Dis. 2003, 9, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Nevez, G.; Raccurt, C.; Jounieaux, V.; Dei-Cas, E.; Mazars, E. Pneumocystosis versus pulmonary Pneumocystis carinii colonization in HIV-negative and HIV-positive patients. AIDS 1999, 13, 535–536. [Google Scholar] [CrossRef] [PubMed]
- Keely, S.P.; Stringer, J.R.; Baughman, R.P.; Linke, M.J.; Walzer, P.D.; Smulian, A.G. Genetic variation among Pneumocystis carinii hominis isolates in recurrent pneumocystosis. J. Infect. Dis. 1995, 172, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Mansharamani, N.G.; Garland, R.; Delaney, D.; Koziel, H. Management and outcome patterns for adult Pneumocystis carinii pneumonia, 1985 to 1995: Comparison of HIV-associated cases to other immunocompromised states. Chest 2000, 118, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Nuesch, R.; Bellini, C.; Zimmerli, W. Pneumocystis carinii pneumonia in human immunodeficiency virus (HIV)-positive and HIV-negative immunocompromised patients. Clin. Infect. Dis. 1999, 29, 1519–1523. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Vidal-Petiot, E.; Osman, D.; Hamzaoui, O.; Durrbach, A.; Goujard, C.; Miceli, C.; Bouree, P.; Richard, C. Critical care management and outcome of severe Pneumocystis pneumonia in patients with and without HIV infection. Crit. Care 2008, 12, R28. [Google Scholar] [CrossRef] [PubMed]
- Mikaelsson, L.; Jacobsson, G.; Andersson, R. Pneumocystis pneumonia—A retrospective study 1991–2001 in Gothenburg; Sweden. J. Infect. 2006, 53, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Teichtahl, A.J.; Morrisroe, K.; Ciciriello, S.; Jennens, I.; Tadros, S.; Wicks, I. Pneumocystis jirovecci pneumonia in connective tissue diseases. Comparison with other immunocompromised patients. Semin. Arthritis Rheum. 2015, 45, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Gordon, S.M.; LaRosa, S.P.; Kalmadi, S.; Arroliga, A.C.; Avery, R.K.; Truesdell-LaRosa, L.; Longworth, D.L. Should prophylaxis for Pneumocystis carinii pneumonia in solid organ transplant recipients ever be discontinued? Clin. Infect. Dis. 1999, 28, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Bourbigot, B.; Bensoussan, T.; Garo, B.; Islam, M.S.; Hardy, E.; Moal, M.C.; Garre, M. CD4 T-lymphocyte counts as predictors of pneumonia after kidney transplantation. Transplant. Proc. 1993, 25, 1491–1492. [Google Scholar] [PubMed]
- Pareja, J.G.; Garland, R.; Koziel, H. Use of adjunctive corticosteroids in severe adult non-HIV Pneumocystis carinii pneumonia. Chest 1998, 113, 1215–1224. [Google Scholar] [CrossRef] [PubMed]
- Adler, D.; Chenivesse, C.; Similowski, T.; Soccal, P.M. Pneumocystis pneumonia in patients with immunosuppression other than HIV infection (in French). Rev. Med. Suisse 2008, 4, 2525–2526; 2528–2530. [Google Scholar] [PubMed]
- Iriart, X.; Witkowski, B.; Cassaing, S.; Abbes, S.; Menard, S.; Fillaux, J.; Valentin, A.; Linas, M.D.; Tkaczuk, J.; Huget, F.; et al. Alveolar and blood T lymphocyte profiles in Pneumocystis jirovecii-positive patients: Effects of HIV status. J. Infect. Dis. 2011, 204, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Magne, D.; Angoulvant, A.; Botterel, F.; Bouges-Michel, C.; Bougnoux, M.E.; Bouree, P.; Chochillon, C.; Cornet, M.; Dannaoui, E.; Fekkar, A.; et al. Pneumocystosis: A network survey in the Paris area 2003–2008. Eur. J. Clin. Microbiol Infect. Dis. 2011, 30, 673–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roux, A.; Canet, E.; Valade, S.; Gangneux-Robert, F.; Hamane, S.; Lafabrie, A.; Maubon, D.; Debourgogne, A.; le Gal, S.; Dalle, F.; et al. Pneumocystis jirovecii pneumonia in patients with or without AIDS, France. Emerg. Infect. Dis. 2014, 20, 1490–1497. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Samaniego, M.; Kaul, D.R. Pneumocystis jirovecii pneumonia is rare in renal transplant recipients receiving only one month of prophylaxis. Transpl. Infect. Dis. 2011, 13, 570–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borstnar, S.; Lindic, J.; Tomazic, J.; Kandus, A.; Pikelj, A.; Prah, J.; Skvarc, M.; Godnov, U.; Kovac, D. Pneumocystis jirovecii pneumonia in renal transplant recipients: A national center experience. Transplant. Proc. 2013, 45, 1614–1617. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.H.; Partovi, N.; Levy, R.D.; Shapiro, R.J.; Yoshida, E.M.; Greanya, E.D. Pneumocystis pneumonia in solid organ transplant recipients: Not yet an infection of the past. Transpl. Infect. Dis. 2012, 14, 519–525. [Google Scholar] [CrossRef] [PubMed]
- De Boer, M.G.; Kroon, F.P.; le Cessie, S.; de Fijtrer, J.W.; van Dissel, J.T. Risk factors for Pneumocystis jirovecii pneumonia in kidney transplant recipients and appraisal of strategies for selective use of chemoprophylaxis. Transpl. Infect. Dis. 2011, 13, 559–569. [Google Scholar] [CrossRef] [PubMed]
- Iriart, X.; Challan Belval, T.; Fillaux, J.; Esposito, L.; Lavergne, R.A.; Cardeau-Desangles, I.; Roques, O.; Del Bello, A.; Cointault, O.; Lavayssiere, L.; et al. Risk factors of Pneumocystis pneumonia in solid organ recipients in the era of the common use of posttransplantation prophylaxis. Am. J. Transplant. 2015, 15, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Fishman, J.A. Prevention of infection due to Pneumocystis carinii. Antimicrob. Agents Chemother. 1998, 42, 995–1004. [Google Scholar]
- Struijk, G.H.; Gijsen, A.F.; Yong, S.L.; Zwinderman, A.H.; Geerlings, S.E.; Lettinga, K.D.; van Donselaar-van der Pant, K.A.; ten Berge, I.J.; Bemelman, F.J. Risk of Pneumocystis jiroveci pneumonia in patients long after renal transplantation. Nephrol. Dial. Transplant. 2011, 26, 3391–3398. [Google Scholar] [CrossRef] [PubMed]
- Munoz, P.; Munoz, R.M.; Palomo, J.; Rodriguez-Creixems, M.; Munoz, R.; Bouza, E. Pneumocystis carinii infection in heart transplant recipients: Efficacy of a weekend prophylaxis schedule. Medicine 1997, 76, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, M.; Fishman, J.A. Prevention of infection due to Pneumocystis spp. in human immunodeficiency virus-negative immunocompromised patients. Clin. Microbiol. Rev. 2004, 17, 770–782. [Google Scholar] [CrossRef] [PubMed]
- Fishman, J.A. Prevention of infection caused by Pneumocystis carinii in transplant recipients. Clin. Infect. Dis. 2001, 33, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Lufft, V.; Kliem, V.; Behrend, M.; Pichlmayr, R.; Koch, K.M.; Brunkhorst, R. Incidence of Pneumocystis carinii pneumonia after renal transplantation: Impact of immunosuppression. Transplantation 1996, 62, 421–423. [Google Scholar] [CrossRef] [PubMed]
- Sepkowitz, K.A.; Brown, A.E.; Armstrong, D. Pneumocystis carinii pneumonia without acquired immunodeficiency syndrome: More patients; same risk. Arch. Intern. Med. 1995, 155, 1125–1128. [Google Scholar] [CrossRef] [PubMed]
- Colombo, J.L.; Sammut, P.H.; Langnas, A.N.; Shaw, B.W., Jr. The spectrum of Pneumocystis carinii infection after liver transplantation in children. Transplantation 1992, 54, 621–624. [Google Scholar] [CrossRef] [PubMed]
- Hayes, M.J.; Torzillo, P.J.; Sheil, A.G.; McCaughan, G.W. Pneumocystis carinii pneumonia after liver transplantation in adults. Clin. Transplant. 1994, 8, 499–503. [Google Scholar] [PubMed]
- Paya, C.V.; Hermans, P.E.; Washington, J.A., 2nd; Smith, T.F.; Anhalt, J.P.; Wiesner, R.H.; Krom, R.A. Incidence, distribution, and outcome of episodes of infection in 100 orthotopic liver transplantations. Mayo Clin. Proc. 1989, 64, 555–564. [Google Scholar] [CrossRef]
- Choi, Y.I.; Hwang, S.; Park, G.C.; Namgoong, J.M.; Jung, D.H.; Song, G.W.; Ha, T.Y.; Moon, D.B.; Kim, K.H.; Ahn, C.S.; et al. Clinical outcomes of Pneumocystis carinii pneumonia in adult liver transplant recipients. Transplant. Proc. 2013, 45, 3057–3060. [Google Scholar] [CrossRef] [PubMed]
- Gryzan, S.; Paradis, I.L.; Zeevi, A.; Duquesnoy, R.J.; Dummer, J.S.; Griffith, B.P.; Hardesty, R.L.; Trento, A.; Nalesnik, M.A.; Dauber, J.H. Unexpectedly high incidence of Pneumocystis carinii infection after lung-heart transplantation: Implications for lung defense and allograft survival. Am. Rev. Respir Dis. 1988, 137, 1268–1274. [Google Scholar] [CrossRef] [PubMed]
- Janner, D.; Bork, J.; Baum, M.; Chinnock, R. Pneumocystis carinii pneumonia in infants after heart transplantation. J. Heart Lung Transplant. 1996, 15, 758–763. [Google Scholar] [PubMed]
- Olsen, S.L.; Renlund, D.G.; OʼConnell, J.B.; Taylor, D.O.; Lassetter, J.E.; Eastburn, T.E.; Hammond, E.H.; Bristow, M.R. Prevention of Pneumocystis carinii pneumonia in cardiac transplant recipients by trimethoprim sulfamethoxazole. Transplantation 1993, 56, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Dummer, J.S.; Montero, C.G.; Griffith, B.P.; Hardesty, R.L.; Paradis, I.L.; Ho, M. Infections in heart-lung transplant recipients. Transplantation 1986, 41, 725–729. [Google Scholar] [CrossRef]
- Radisic, M.; Lattes, R.; Chapman, J.F.; del Carmen Rial, M.; Guardia, O.; Seu, F.; Gutierrez, P.; Goldberg, J.; Casadei, D.H. Risk factors for Pneumocystis carinii pneumonia in kidney transplant recipients: A case-control study. Transpl. Infect. Dis. 2003, 5, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Fillatre, P.; Decaux, O.; Jouneau, S.; Revest, M.; Gacouin, A.; Robert-Gangneux, F.; Fresnel, A.; Guiguen, C.; le Tulzo, Y.; Jego, P.; et al. Incidence of Pneumocystis jiroveci pneumonia among groups at risk in HIV-negative patients. Am. J. Med. 2014, 127, 1242.e11–1242.e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, A.M.; Wajszczuk, C.P.; Suffredini, A.F.; Hakala, T.R.; Ho, M. Pneumocystis carinii pneumonia in renal-transplant recipients treated with cyclosporine and steroids. J. Infect. Dis. 1984, 149, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Dummer, J.S. Pneumocystis carinii infections in transplant recipients. Semin. Respir. Infect. 1990, 5, 50–57. [Google Scholar] [PubMed]
- Elinder, C.G.; Andersson, J.; Bolinder, G.; Tyden, G. Effectiveness of low-dose cotrimoxazole prophylaxis against Pneumocystis carinii pneumonia after renal and/or pancreas transplantation. Transpl. Int. 1992, 5, 81–84. [Google Scholar] [PubMed]
- Hennequin, C.; Page, B.; Roux, P.; Legendre, C.; Kreis, H. Outbreak of Pneumocystis carinii pneumonia in a renal transplant unit. Eur. J. Clin. Microbiol. Infect. Dis. 1995, 14, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Branten, A.J.; Beckers, P.J.; Tiggeler, R.G.; Hoitsma, A.J. Pneumocystis carinii pneumonia in renal transplant recipients. Nephrol Dial. Transplant. 1995, 10, 1194–1197. [Google Scholar] [PubMed]
- Arend, S.M.; Westendorp, R.G.; Kroon, F.P.; vanʼt Wout, J.W.; Vandenbroucke, J.P.; van Es, L.A.; van der Woude, F.J. Rejection treatment and cytomegalovirus infection as risk factors for Pneumocystis carinii pneumonia in renal transplant recipients. Clin. Infect. Dis. 1996, 22, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Green, H.; Paul, M.; Vidal, L.; Leibovici, L. Prophylaxis for Pneumocystis pneumonia (PCP) in non-HIV immunocompromised patients. Cochrane Database Syst. Rev. 2007. [Google Scholar] [CrossRef]
- Catherinot, E.; Lanternier, F.; Bougnoux, M.E.; Lecuit, M.; Couderc, L.J.; Lortholary, O. Pneumocystis jirovecii Pneumonia. Infect. Dis. Clin. North. Am. 2010, 24, 107–138. [Google Scholar] [CrossRef] [PubMed]
- Cushion, M.T. Are members of the fungal genus Pneumocystis (a) commensals; (b) opportunists, (c) pathogens; or (d) all of the above? PLoS Pathog. 2010, 6, e1001009. [Google Scholar] [CrossRef] [PubMed]
- Lubis, N.; Baylis, D.; Short, A.; Stebbing, J.; Teague, A.; Portsmouth, S.; Bower, M.; Nelson, M.; Gazzard, B. Prospective cohort study showing changes in the monthly incidence of Pneumocystis carinii pneumonia. Postgrad. Med. J. 2003, 79, 164–166. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.F.; Grant, A.D.; Foley, N.M. Seasonal variation in presentation of Pneumocystis carinii pneumonia. Lancet 1992, 339, 747–748. [Google Scholar] [CrossRef]
- Varela, J.M.; Regordan, C.; Medrano, F.J.; Respaldiza, N.; de La Horra, C.; Montes-Cano, M.A.; Calderon, E.J. Climatic factors and Pneumocystis jiroveci infection in southern Spain. Clin. Microbiol. Infect. 2004, 10, 770–772. [Google Scholar] [CrossRef] [PubMed]
- Sing, A.; Schmoldt, S.; Laubender, R.P.; Heesemann, J.; Sing, D.; Wildner, M. Seasonal variation of Pneumocystis jirovecii infection: Analysis of underlying climatic factors. Clin. Microbiol. Infect. 2009, 15, 957–960. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.F.; Evans, H.E.; Copas, A.J.; Huggett, J.F.; Edwards, S.G.; Walzer, P.D. Seasonal variation in mortality of Pneumocystis jirovecii pneumonia in HIV-infected patients. Int. J. STD AIDS 2010, 21, 497–503. [Google Scholar] [CrossRef] [PubMed]
- De Boer, M.G.; de Fijter, J.W.; Kroon, F.P. Outbreaks and clustering of Pneumocystis pneumonia in kidney transplant recipients: A systematic review. Med. Mycol. 2011, 49, 673–680. [Google Scholar] [PubMed]
- Arichi, N.; Kishikawa, H.; Mitsui, Y.; Kato, T.; Nishimura, K.; Tachikawa, R.; Tomii, K.; Shiina, H.; Igawa, M.; Ichikawa, Y. Cluster outbreak of Pneumocystis pneumonia among kidney transplant patients within a single center. Transplant. Proc. 2009, 41, 170–172. [Google Scholar] [CrossRef] [PubMed]
- De Boer, M.G.; Bruijnesteijn van Coppenraet, L.E.; Gaasbeek, A.; Berger, S.P.; Gelinck, L.B.; van Houwelingen, H.C.; van den Broek, P.; Kuijper, E.J.; Kroon, F.P.; Vandenbroucke, J.P. An outbreak of Pneumocystis jiroveci pneumonia with 1 predominant genotype among renal transplant recipients: Interhuman transmission or a common environmental source? Clin. Infect. Dis. 2007, 44, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Hocker, B.; Wendt, C.; Nahimana, A.; Tonshoff, B.; Hauser, P.M. Molecular evidence of Pneumocystis transmission in pediatric transplant unit. Emerg. Infect. Dis. 2005, 11, 330–332. [Google Scholar] [CrossRef] [PubMed]
- Schmoldt, S.; Schuhegger, R.; Wendler, T.; Huber, I.; Sollner, H.; Hogardt, M.; Arbogast, H.; Heesemann, J.; Bader, L.; Sing, A. Molecular evidence of nosocomial Pneumocystis jirovecii transmission among 16 patients after kidney transplantation. J. Clin. Microbiol. 2008, 46, 966–971. [Google Scholar] [CrossRef] [PubMed]
- Rabodonirina, M.; Vanhems, P.; Couray-Targe, S.; Gillibert, R.P.; Ganne, C.; Nizard, N.; Colin, C.; Fabry, J.; Touraine, J.L.; van Melle, G.; et al. Molecular evidence of interhuman transmission of Pneumocystis pneumonia among renal transplant recipients hospitalized with HIV-infected patients. Emerg. Infect. Dis. 2004, 10, 1766–1773. [Google Scholar] [CrossRef] [PubMed]
- Phipps, L.M.; Chen, S.C.; Kable, K.; Halliday, C.L.; Firacative, C.; Meyer, W.; Wong, G.; Nankivell, B.J. Nosocomial Pneumocystis jirovecii pneumonia: Lessons from a cluster in kidney transplant recipients. Transplantation 2011, 92, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Le Gal, S.; Damiani, C.; Rouille, A.; Grall, A.; Treguer, L.; Virmaux, M.; Moalic, E.; Quinio, D.; Moal, M.C.; Berthou, C.; et al. A cluster of Pneumocystis infections among renal transplant recipients: Molecular evidence of colonized patients as potential infectious sources of Pneumocystis jirovecii. Clin. Infect. Dis. 2012, 54, e62–e71. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, M.S.; Vermund, S.H.; Jacobs, R.; Durant, P.J.; Shaw, M.M.; Smith, J.W.; Tang, X.; Lu, J.J.; Li, B.; Jin, S.; et al. Detection of Pneumocystis carinii DNA in air samples: Likely environmental risk to susceptible persons. J. Clin. Microbiol. 1997, 35, 2511–2513. [Google Scholar] [PubMed]
- Olsson, M.; Lidman, C.; Latouche, S.; Bjorkman, A.; Roux, P.; Linder, E.; Wahlgren, M. Identification of Pneumocystis carinii f. sp. hominis gene sequences in filtered air in hospital environments. J. Clin. Microbiol. 1998, 36, 1737–1740. [Google Scholar] [PubMed]
- Martin, S.I.; Fishman, J.A. Pneumocystis pneumonia in solid organ transplant recipients. Am. J. Transplant. 2009, 9, S227–S233. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, J.; Mahalati, K.; Kiberd, B.; McAlister, V.C.; MacDonald, A.S. Conversion to rapamycin immunosuppression in renal transplant recipients: Report of an initial experience. Transplantation 2000, 70, 1244–1247. [Google Scholar] [CrossRef] [PubMed]
- Neff, R.T.; Jindal, R.M.; Yoo, D.Y.; Hurst, F.P.; Agodoa, L.Y.; Abbott, K.C. Analysis of USRDS: Incidence and risk factors for Pneumocystis jiroveci pneumonia. Transplantation 2009, 88, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Franson, T.R.; Kauffman, H.M., Jr.; Adams, M.B.; Lemann, J., Jr.; Cabrera, E.; Hanacik, L. Cyclosporine therapy and refractory Pneumocystis carinii pneumonia: A potential association. Arch. Surg. 1987, 122, 1034–1035. [Google Scholar] [CrossRef] [PubMed]
- Strom, T.B. Immunosuppressive agents in renal transplantation. Kidney Int. 1984, 26, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Kreis, H. Antilymphocyte globulins in kidney transplantation. Kidney Int. Suppl. 1992, 38, S188–S192. [Google Scholar]
- Dantal, J.; Soulillou, J.P. Use of monoclonal antibodies in human transplantation. Curr. Opin. Immunol. 1991, 3, 740–747. [Google Scholar] [CrossRef]
- Fishman, J.A. Infection in renal transplant recipients. Semin. Nephrol. 2007, 27, 445–461. [Google Scholar] [CrossRef]
- Reid, A.B.; Chen, S.C.; Worth, L.J. Pneumocystis jirovecii pneumonia in non-HIV-infected patients: New risks and diagnostic tools. Curr. Opin. Infect. Dis. 2011, 24, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.I.; Marty, F.M.; Fiumara, K.; Treon, S.P.; Gribben, J.G.; Baden, L.R. Infectious complications associated with alemtuzumab use for lymphoproliferative disorders. Clin. Infect. Dis. 2006, 43, 16–24. [Google Scholar] [CrossRef]
- Eitner, F.; Hauser, I.A.; Rettkowski, O.; Rath, T.; Lopau, K.; Pliquett, R.U.; Fiedler, R.; Guba, M.; Hilgers, R.D.; Floege, J.; Fischereder, M. Risk factors for Pneumocystis jiroveci pneumonia (PcP) in renal transplant recipients. Nephrol Dial. Transplant. 2011, 26, 2013–2017. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.C. Adrenocorticotropic Hormone: Adrenocortical Steroids and Their Synthetic Analogs, Inhibitors of the Synthesis and Actions of Adrenocortical Hormones; Pergamon Press: New York, NY, USA, 1990. [Google Scholar]
- Schaffner, A.; Schaffner, T. Glucocorticoid-induced impairment of macrophage antimicrobial activity: Mechanisms and dependence on the state of activation. Rev. Infect. Dis. 1987, 9, S620–S629. [Google Scholar] [CrossRef] [PubMed]
- Russo-Marie, F. Macrophages and the glucocorticoids. J. Neuroimmunol. 1992, 40, 281–286. [Google Scholar] [CrossRef]
- Ten Berge, R.J.; Sauerwein, H.P.; Yong, S.L.; Schellekens, P.T. Administration of prednisolone in vivo affects the ratio of OKT4/OKT8 and the LDH-isoenzyme pattern of human T lymphocytes. Clin. Immunol. Immunopathol. 1984, 30, 91–103. [Google Scholar] [CrossRef]
- Sepkowitz, K.A.; Brown, A.E.; Telzak, E.E.; Gottlieb, S.; Armstrong, D. Pneumocystis carinii pneumonia among patients without AIDS at a cancer hospital. JAMA 1992, 267, 832–837. [Google Scholar] [CrossRef] [PubMed]
- Yale, S.H.; Limper, A.H. Pneumocystis carinii pneumonia in patients without acquired immunodeficiency syndrome: Associated illness and prior corticosteroid therapy. Mayo Clin. Proc. 1996, 71, 5–13. [Google Scholar] [CrossRef] [PubMed]
- De Castro, N.; Xu, F.; Porcher, R.; Pavie, J.; Molina, J.M.; Peraldi, M.N. Pneumocystis jirovecii pneumonia in renal transplant recipients occurring after discontinuation of prophylaxis: A case-control study. Clin. Microbiol. Infect. 2010, 16, 1375–1377. [Google Scholar] [CrossRef] [PubMed]
- Ransom, J.T. Mechanism of action of mycophenolate mofetil. Ther. Drug Monit. 1995, 17, 681–684. [Google Scholar] [CrossRef] [PubMed]
- Oz, H.S.; Hughes, W.T. Novel anti-Pneumocystis carinii effects of the immunosuppressant mycophenolate mofetil in contrast to provocative effects of tacrolimus, sirolimus, and dexamethasone. J. Infect. Dis. 1997, 175, 901–904. [Google Scholar] [CrossRef] [PubMed]
- Placebo-controlled study of mycophenolate mofetil combined with cyclosporin and corticosteroids for prevention of acute rejection. European Mycophenolate Mofetil Cooperative Study Group. Lancet 1995, 345, 1321–1325.
- The Tricontinental Mycophenolate Mofetil Renal Transplantation Study Group. A blinded, randomized clinical trial of mycophenolate mofetil for the prevention of acute rejection in cadaveric renal transplantation. Transplantation 1996, 61, 1029–1037. [Google Scholar]
- Sollinger, H.W. Mycophenolate mofetil for the prevention of acute rejection in primary cadaveric renal allograft recipients. U.S. Renal Transplant Mycophenolate Mofetil Study Group. Transplantation 1995, 60, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Ritter, M.L.; Pirofski, L. Mycophenolate mofetil: Effects on cellular immune subsets, infectious complications, and antimicrobial activity. Transpl. Infect. Dis. 2009, 11, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Gianella, S.; Haeberli, L.; Joos, B.; Ledergerber, B.; Wuthrich, R.P.; Weber, R.; Kuster, H.; Hauser, P.M.; Fehr, T.; Mueller, N.J. Molecular evidence of interhuman transmission in an outbreak of Pneumocystis jirovecii pneumonia among renal transplant recipients. Transpl. Infect. Dis. 2010, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rostved, A.A.; Sassi, M.; Kurtzhals, J.A.; Sorensen, S.S.; Rasmussen, A.; Ross, C.; Gogineni, E.; Huber, C.; Kutty, G.; Kovacs, J.A.; et al. Outbreak of Pneumocystis Pneumonia in Renal and Liver Transplant Patients Caused by Genotypically Distinct Strains of Pneumocystis jirovecii. Transplantation 2013, 96, 834–842. [Google Scholar]
- Azevedo, L.S.; Castro, M.C.; Paula, F.J.; Ianhez, L.E.; David-Neto, E. Mycophenolate mofetil may protect against Pneumocystis carinii pneumonia in renal transplanted patients. Rev. Inst. Med. Trop. Sao Paulo 2005, 47, 143–145. [Google Scholar] [CrossRef] [PubMed]
- Kahan, B.D.; Julian, B.A.; Pescovitz, M.D.; Vanrenterghem, Y.; Neylan, J. Sirolimus reduces the incidence of acute rejection episodes despite lower cyclosporine doses in caucasian recipients of mismatched primary renal allografts: A phase II trial. Rapamune Study Group. Transplantation 1999, 68, 1526–1532. [Google Scholar] [CrossRef] [PubMed]
- Andres, A.M.; Lopez Santamaria, M.; Ramos, E.; Hernandez, F.; Prieto, G.; Encinas, J.; Leal, N.; Molina, M.; Sarria, J.; Tovar, J. The use of sirolimus as a rescue therapy in pediatric intestinal transplant recipients. Pediatr. Transplant. 2010, 14, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Pliquett, R.U.; Asbe-Vollkopf, A.; Hauser, P.M.; Presti, L.L.; Hunfeld, K.P.; Berger, A.; Scheuermann, E.H.; Jung, O.; Geiger, H.; Hauser, I.A. A Pneumocystis jirovecii pneumonia outbreak in a single kidney-transplant center: Role of cytomegalovirus co-infection. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 2429–2437. [Google Scholar] [CrossRef] [PubMed]
- Linnemann, C.C., Jr.; Kauffman, C.A.; First, M.R.; Schiff, G.M.; Phair, J.P. Cellular immune response to cytomegalovirus infection after renal transplantation. Infect. Immun. 1978, 22, 176–180. [Google Scholar] [PubMed]
- Beck, J.M.; Harmsen, A.G. Lymphocytes in host defense against Pneumocystis carinii. Semin. Respir. Infect. 1998, 13, 330–338. [Google Scholar] [PubMed]
- Masur, H.; Ognibene, F.P.; Yarchoan, R.; Shelhamer, J.H.; Baird, B.F.; Travis, W.; Suffredini, A.F.; Deyton, L.; Kovacs, J.A.; Falloon, J.; et al. CD4 counts as predictors of opportunistic pneumonias in human immunodeficiency virus (HIV) infection. Ann. Intern. Med. 1989, 111, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Nevez, G.; Raccurt, C.; Vincent, P.; Jounieaux, V.; Dei-Cas, E. Pulmonary colonization with Pneumocystis carinii in human immunodeficiency virus-negative patients: Assessing risk with blood CD4+ T cell counts. Clin. Infect. Dis. 1999, 29, 1331–1332. [Google Scholar] [CrossRef] [PubMed]
- Castagnola, E.; Dini, G.; Lanino, E.; Tasso, L.; Dallorso, S.; Garaventa, A.; Rossi, G.A.; Giacchino, R. Low CD4 lymphocyte count in a patient with P. carinii pneumonia after autologous bone marrow transplantation. Bone Marrow Transplant. 1995, 15, 977–978. [Google Scholar] [PubMed]
- Mansharamani, N.G.; Balachandran, D.; Vernovsky, I.; Garland, R.; Koziel, H. Peripheral blood CD4+ T-lymphocyte counts during Pneumocystis carinii pneumonia in immunocompromised patients without HIV infection. Chest 2000, 118, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.N.; Shellito, J.E. Current understanding of Pneumocystis immunology. Future Microbiol. 2010, 5, 43–65. [Google Scholar] [CrossRef] [PubMed]
- Sassi, M.; Ripamonti, C.; Mueller, N.J.; Yazaki, H.; Kutty, G.; Ma, L.; Huber, C.; Gogineni, E.; Oka, S.; Goto, N.; et al. Outbreaks of Pneumocystis pneumonia in 2 renal transplant centers linked to a single strain of Pneumocystis: Implications for transmission and virulence. Clin. Infect. Dis. 2012, 54, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Yazaki, H.; Goto, N.; Uchida, K.; Kobayashi, T.; Gatanaga, H.; Oka, S. Outbreak of Pneumocystis jiroveci pneumonia in renal transplant recipients: P. jiroveci is contagious to the susceptible host. Transplantation 2009, 88, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Mitsides, N.; Greenan, K.; Green, D.; Middleton, R.; Lamerton, E.; Allen, J.; Redshaw, J.; Chadwick, P.R.; Subudhi, C.P.; Wood, G. Complications and outcomes of trimethoprim-sulphamethoxazole as chemoprophylaxis for Pneumocystis pneumonia in renal transplant recipients. Nephrology 2014, 19, 157–163. [Google Scholar] [CrossRef]
- Russian, D.A.; Levine, S.J. Pneumocystis carinii pneumonia in patients without HIV infection. Am. J. Med. Sci. 2001, 321, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, J.A.; Hiemenz, J.W.; Macher, A.M.; Stover, D.; Murray, H.W.; Shelhamer, J.; Lane, H.C.; Urmacher, C.; Honig, C.; Longo, D.L.; et al. Pneumocystis carinii pneumonia: A comparison between patients with the acquired immunodeficiency syndrome and patients with other immunodeficiencies. Ann. Intern. Med. 1984, 100, 663–671. [Google Scholar] [CrossRef]
- Martin, S.I.; Fishman, J.A. Pneumocystis pneumonia in solid organ transplantation. Am. J. Transplant. 2013, 13, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Ewig, S.; Bauer, T.; Schneider, C.; Pickenhain, A.; Pizzulli, L.; Loos, U.; Luderitz, B. Clinical characteristics and outcome of Pneumocystis carinii pneumonia in HIV-infected and otherwise immunosuppressed patients. Eur. Respir. J. 1995, 8, 1548–1553. [Google Scholar] [PubMed]
- Bollee, G.; Sarfati, C.; Thiery, G.; Bergeron, A.; de Miranda, S.; Menotti, J.; de Castro, N.; Tazi, A.; Schlemmer, B.; Azoulay, E. Clinical picture of Pneumocystis jiroveci pneumonia in cancer patients. Chest 2007, 132, 1305–1310. [Google Scholar] [CrossRef] [PubMed]
- Walzer, P.D.; Perl, D.P.; Krogstad, D.J.; Rawson, P.G.; Schultz, M.G. Pneumocystis carinii pneumonia in the United States: Epidemiologic, diagnostic, and clinical features. Ann. Intern. Med. 1974, 80, 83–93. [Google Scholar] [CrossRef] [PubMed]
- McKinnell, J.A.; Cannella, A.P.; Kunz, D.F.; Hook, E.W., 3rd; Moser, S.A.; Miller, L.G.; Baddley, J.W.; Pappas, P.G. Pneumocystis pneumonia in hospitalized patients: A detailed examination of symptoms, management, and outcomes in human immunodeficiency virus (HIV)-infected and HIV-uninfected persons. Transpl. Infect. Dis. 2012, 14, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Santiago-Delpin, E.A.; Mora, E.; Gonzalez, Z.A.; Morales-Otero, L.A.; Bermudez, R. Factors in an outbreak of Pneumocystis carinii in a transplant unit. Transplant. Proc. 1988, 20, 462–465. [Google Scholar] [PubMed]
- Talseth, T.; Holdaas, H.; Albrechtsen, D.; Berg, K.J.; Fauchald, P.; Naalsund, A.; Nordal, K.P.; Skar, A.G.; Sodal, G.; Flatmark, A. Increasing incidence of Pneumocystis carinii pneumonia in renal transplant patients. Transplant. Proc. 1988, 20, 400–401. [Google Scholar] [PubMed]
- Sugimoto, H.; Uchida, H.; Akiyama, N.; Nagao, T.; Tomikawa, S.; Mita, K.; Beck, Y.; Inoue, S.; Watanabe, K.; Nakayama, Y.; et al. Improved survival of renal allograft recipients with Pneumocystis carinii pneumonia by early diagnosis and treatment. Transplant. Proc. 1992, 24, 1556–1558. [Google Scholar] [PubMed]
- Zaoutis, T.E.; Webber, S.; Naftel, D.C.; Chrisant, M.A.; Kaufman, B.; Pearce, F.B.; Spicer, R.; Dipchand, A.I. Invasive fungal infections in pediatric heart transplant recipients: Incidence, risk factors, and outcomes. Pediatr. Transplant. 2011, 15, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Ng, B.; Dipchand, A.; Naftel, D.; Rusconi, P.; Boyle, G.; Zaoutis, T.; Edens, R.E. Outcomes of Pneumocystis jiroveci pneumonia infections in pediatric heart transplant recipients. Pediatr. Transplant. 2011, 15, 844–848. [Google Scholar] [CrossRef] [PubMed]
- Roux, A.; Gonzalez, F.; Roux, M.; Mehrad, M.; Menotti, J.; Zahar, J.R.; Tadros, V.X.; Azoulay, E.; Brillet, P.Y.; Vincent, F. Update on pulmonary Pneumocystis jirovecii infection in non-HIV patients. Med. Mal. Infect. 2014, 44, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Toper, C.; Rivaud, E.; Daniel, C.; Cerf, C.; Parquin, F.; Catherinot, E.; Honderlick, P.; Escande, M.C.; Dreyfus, J.F.; Stern, M.; et al. Pneumocystis jirovecii pneumonia in non-HIV infected patients: A study of 41 cases. Rev. Pneumol. Clin. 2011, 67, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Zahar, J.R.; Robin, M.; Azoulay, E.; Fieux, F.; Nitenberg, G.; Schlemmer, B. Pneumocystis carinii pneumonia in critically ill patients with malignancy: A descriptive study. Clin. Infect. Dis. 2002, 35, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Limper, A.H.; Offord, K.P.; Smith, T.F.; Martin, W.J., 2nd. Pneumocystis carinii pneumonia: Differences in lung parasite number and inflammation in patients with and without AIDS. Am. Rev. Respir. Dis. 1989, 140, 1204–1209. [Google Scholar] [CrossRef] [PubMed]
- DeLorenzo, L.J.; Huang, C.T.; Maguire, G.P.; Stone, D.J. Roentgenographic patterns of Pneumocystis carinii pneumonia in 104 patients with AIDS. Chest 1987, 91, 323–327. [Google Scholar] [CrossRef]
- Boiselle, P.M.; Crans, C.A., Jr.; Kaplan, M.A. The changing face of Pneumocystis carinii pneumonia in AIDS patients. Am. J. Roentgenol. 1999, 172, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Kanne, J.P.; Yandow, D.R.; Meyer, C.A. Pneumocystis jiroveci pneumonia: High-resolution CT findings in patients with and without HIV infection. AJR Am. J. Roentgenol. 2012, 198, W555–W561. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Nakamura, T.; Iwamoto, A. Pneumocystis pneumonia in patients with HIV infection: Clinical manifestations, laboratory findings, and radiological features. J. Infect. Chemother. 2007, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Vogel, M.N.; Brodoefel, H.; Hierl, T.; Beck, R.; Bethge, W.A.; Claussen, C.D.; Horger, M.S. Differences and similarities of cytomegalovirus and Pneumocystis pneumonia in HIV-negative immunocompromised patients thin section CT morphology in the early phase of the disease. Br. J. Radiol. 2007, 80, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Vogel, M.N.; Vatlach, M.; Weissgerber, P.; Goeppert, B.; Claussen, C.D.; Hetzel, J.; Horger, M. HRCT-features of Pneumocystis jiroveci pneumonia and their evolution before and after treatment in non-HIV immunocompromised patients. Eur. J. Radiol. 2012, 81, 1315–1320. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.F., Jr.; Limper, A.H. Pneumocystis pneumonia: Clinical presentation and diagnosis in patients with and without acquired immune deficiency syndrome. Semin. Respir. Infect. 1998, 13, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Helweg-Larsen, J.; Jensen, J.S.; Lundgren, B. Non-invasive diagnosis of Pneumocystis carinii pneumonia by PCR on oral washes. Lancet 1997, 350, 1363. [Google Scholar] [CrossRef]
- Larsen, H.H.; Huang, L.; Kovacs, J.A.; Crothers, K.; Silcott, V.A.; Morris, A.; Turner, J.R.; Beard, C.B.; Masur, H.; Fischer, S.H. A prospective, blinded study of quantitative touch-down polymerase chain reaction using oral-wash samples for diagnosis of Pneumocystis pneumonia in HIV-infected patients. J. Infect. Dis. 2004, 189, 1679–1683. [Google Scholar] [CrossRef] [PubMed]
- De Boer, M.G.; Gelinck, L.B.; van Zelst, B.D.; van de Sande, W.W.; Willems, L.N.; van Dissel, J.T.; de Jonge, R.; Kroon, F.P. β-d-glucan and S-adenosylmethionine serum levels for the diagnosis of Pneumocystis pneumonia in HIV-negative patients: A prospective study. J. Infect. 2011, 62, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.K.; Young, L.S.; Remington, J.S. Pneumocystis carinii pneumonia: Diagnosis by examination of pulmonary secretions. JAMA 1976, 236, 2399–2402. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, J.A.; Ng, V.L.; Masur, H.; Leoung, G.; Hadley, W.K.; Evans, G.; Lane, H.C.; Ognibene, F.P.; Shelhamer, J.; Parrillo, J.E.; et al. Diagnosis of Pneumocystis carinii pneumonia: Improved detection in sputum with use of monoclonal antibodies. N. Engl. J. Med. 1988, 318, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Fishman, J.A. Pneumocystis carinii and Parasitic Infections in the Immunocompromised Host; Kluwer Academic/Plenum Publishers: New York, NY, USA, 2002. [Google Scholar]
- Stover, D.E.; Zaman, M.B.; Hajdu, S.I.; Lange, M.; Gold, J.; Armstrong, D. Bronchoalveolar lavage in the diagnosis of diffuse pulmonary infiltrates in the immunosuppressed host. Ann. Intern. Med. 1984, 101, 1–7. [Google Scholar]
- Broaddus, C.; Dake, M.D.; Stulbarg, M.S.; Blumenfeld, W.; Hadley, W.K.; Golden, J.A.; Hopewell, P.C. Bronchoalveolar lavage and transbronchial biopsy for the diagnosis of pulmonary infections in the acquired immunodeficiency syndrome. Ann. Intern. Med. 1985, 102, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Rossiter, S.J.; Miller, C.; Churg, A.M.; Carrington, C.B.; Mark, J.B. Open lung biopsy in the immunosuppressed patient: Is it really beneficial? J. Thorac. Cardiovasc. Surg. 1979, 77, 338–345. [Google Scholar] [PubMed]
- Thomas, C.F., Jr.; Limper, A.H. Current insights into the biology and pathogenesis of Pneumocystis pneumonia. Nat. Rev. Microbiol. 2007, 5, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.F., Jr.; Limper, A.H. Pneumocystis pneumonia. N. Engl. J. Med. 2004, 350, 2487–2498. [Google Scholar] [CrossRef] [PubMed]
- Weig, M.; Klinker, H.; Bogner, B.H.; Meier, A.; Gross, U. Usefulness of PCR for diagnosis of Pneumocystis carinii pneumonia in different patient groups. J. Clin. Microbiol. 1997, 35, 1445–1449. [Google Scholar] [PubMed]
- Ribes, J.A.; Limper, A.H.; Espy, M.J.; Smith, T.F. PCR detection of Pneumocystis carinii in bronchoalveolar lavage specimens: Analysis of sensitivity and specificity. J. Clin. Microbiol. 1997, 35, 830–835. [Google Scholar] [PubMed]
- Gupta, R.; Mirdha, B.R.; Guleria, R.; Kumar, L.; Samantaray, J.C.; Agarwal, S.K.; Kabra, S.K.; Luthra, K. Diagnostic significance of nested polymerase chain reaction for sensitive detection of Pneumocystis jirovecii in respiratory clinical specimens. Diagn. Microbiol. Infect. Dis. 2009, 64, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Flori, P.; Bellete, B.; Durand, F.; Raberin, H.; Cazorla, C.; Hafid, J.; Lucht, F.; Sung, R.T. Comparison between real-time PCR, conventional PCR and different staining techniques for diagnosing Pneumocystis jiroveci pneumonia from bronchoalveolar lavage specimens. J. Med. Microbiol. 2004, 53, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Robberts, F.J.; Liebowitz, L.D.; Chalkley, L.J. Polymerase chain reaction detection of Pneumocystis jiroveci: Evaluation of 9 assays. Diagn. Microbiol. Infect. Dis. 2007, 58, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; Bergeron, A.; Chevret, S.; Bele, N.; Schlemmer, B.; Menotti, J. Polymerase chain reaction for diagnosing Pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary infiltrates. Chest 2009, 135, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, T.; Suda, T.; Matsuda, H.; Inui, N.; Nakamura, Y.; Sato, J.; Toyoshima, M.; Nakano, Y.; Yasuda, K.; Gemma, H.; et al. Real-time PCR is more specific than conventional PCR for induced sputum diagnosis of Pneumocystis pneumonia in immunocompromised patients without HIV infection. Respirology 2009, 14, 203–209. [Google Scholar] [CrossRef]
- Larsen, H.H.; Masur, H.; Kovacs, J.A.; Gill, V.J.; Silcott, V.A.; Kogulan, P.; Maenza, J.; Smith, M.; Lucey, D.R.; Fischer, S.H. Development and evaluation of a quantitative, touch-down, real-time PCR assay for diagnosing Pneumocystis carinii pneumonia. J. Clin. Microbiol. 2002, 40, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Chumpitazi, B.F.; Flori, P.; Kern, J.B.; Brenier-Pinchart, M.P.; Hincky-Vitrat, V.; Brion, J.P.; Thiebaut-Bertrand, A.; Minet, C.; Maubon, D.; Pelloux, H. Characteristics and clinical relevance of the quantitative touch-down major surface glycoprotein polymerase chain reaction in the diagnosis of Pneumocystis pneumonia. Med. Mycol. 2011, 49, 704–713. [Google Scholar] [PubMed]
- Alanio, A.; Desoubeaux, G.; Sarfati, C.; Hamane, S.; Bergeron, A.; Azoulay, E.; Molina, J.M.; Derouin, F.; Menotti, J. Real-time PCR assay-based strategy for differentiation between active Pneumocystis jirovecii pneumonia and colonization in immunocompromised patients. Clin. Microbiol. Infect. 2011, 17, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Fillaux, J.; Malvy, S.; Alvarez, M.; Fabre, R.; Cassaing, S.; Marchou, B.; Linas, M.D.; Berry, A. Accuracy of a routine real-time PCR assay for the diagnosis of Pneumocystis jirovecii pneumonia. J. Microbiol. Methods 2008, 75, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Rohner, P.; Jacomo, V.; Studer, R.; Schrenzel, J.; Graf, J.D. Detection of Pneumocystis jirovecii by two staining methods and two quantitative PCR assays. Infection 2009, 37, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Dini, L.; du Plessis, M.; Frean, J.; Fernandez, V. High prevalence of dihydropteroate synthase mutations in Pneumocystis jirovecii isolated from patients with Pneumocystis pneumonia in South Africa. J. Clin. Microbiol. 2010, 48, 2016–2021. [Google Scholar] [CrossRef] [PubMed]
- Hauser, P.M.; Bille, J.; Lass-Florl, C.; Geltner, C.; Feldmesser, M.; Levi, M.; Patel, H.; Muggia, V.; Alexander, B.; Hughes, M.; et al. Multicenter, prospective clinical evaluation of respiratory samples from subjects at risk for Pneumocystis jirovecii infection by use of a commercial real-time PCR assay. J. Clin. Microbiol. 2011, 49, 1872–1878. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Martinez, M.J.; Miro, J.M.; Valls, M.E.; Moreno, A.; Rivas, P.V.; Sole, M.; Benito, N.; Domingo, P.; Munoz, C.; Rivera, E.; et al. Sensitivity and specificity of nested and real-time PCR for the detection of Pneumocystis jiroveci in clinical specimens. Diagn. Microbiol. Infect. Dis. 2006, 56, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, S.; Morilla, R.; Leon, J.A.; Martin-Garrido, I.; Rivero, L.; Friaza, V.; Respaldiza, N.; Montes-Cano, M.A.; Teran, R.; de la Horra, C. High prevalence of Pneumocystis jiroveci colonization among young HIV-infected patients. J. Adolesc. Health 2011, 48, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Iriart, X.; Witkowski, B.; Courtais, C.; Abbes, S.; Tkaczuk, J.; Courtade, M.; Cassaing, S.; Fillaux, J.; Blancher, A.; Magnaval, J.F.; et al. Cellular and cytokine changes in the alveolar environment among immunocompromised patients during Pneumocystis jirovecii infection. Med. Mycol. 2010, 48, 1075–1087. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, M.E.; Tedrow, J.R.; Hillenbrand, M.E.; Lucht, L.; Richards, T.; Norris, K.A.; Zhang, Y.; Sciurba, F.C.; Kaminski, N.; Morris, A. Pneumocystis jirovecii colonization is associated with enhanced Th1 inflammatory gene expression in lungs of humans with chronic obstructive pulmonary disease. Microbiol. Immunol. 2014, 58, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.; Wei, K.; Afshar, K.; Huang, L. Epidemiology and clinical significance of Pneumocystis colonization. J. Infect. Dis. 2008, 197, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.; Norris, K.A. Colonization by Pneumocystis jirovecii and its role in disease. Clin. Microbiol. Rev. 2012, 25, 297–317. [Google Scholar] [CrossRef] [PubMed]
- Desmet, S.; van Wijngaerden, E.; Maertens, J.; Verhaegen, J.; Verbeken, E.; de Munter, P.; Meersseman, W.; van Meensel, B.; van Eldere, J.; Lagrou, K. Serum (1–3)-β-d-glucan as a tool for diagnosis of Pneumocystis jirovecii pneumonia in patients with human immunodeficiency virus infection or hematological malignancy. J. Clin. Microbiol. 2009, 47, 3871–3874. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Yasuoka, A.; Tanuma, J.; Yazaki, H.; Honda, H.; Tsukada, K.; Honda, M.; Gatanaga, H.; Teruya, K.; Kikuchi, Y.; et al. Serum (1→3) β-d-glucan as a noninvasive adjunct marker for the diagnosis of Pneumocystis pneumonia in patients with AIDS. Clin. Infect. Dis. 2009, 49, 1128–1131. [Google Scholar] [CrossRef] [PubMed]
- Damiani, C.; Le Gal, S.; Lejeune, D.; Brahimi, N.; Virmaux, M.; Nevez, G.; Totet, A. Serum (1→3)-β-d-glucan levels in primary infection and pulmonary colonization with Pneumocystis jirovecii. J. Clin. Microbiol. 2011, 49, 2000–2002. [Google Scholar] [CrossRef] [PubMed]
- Damiani, C.; le Gal, S.; Da Costa, C.; Virmaux, M.; Nevez, G.; Totet, A. Combined quantification of pulmonary Pneumocystis jirovecii DNA and serum (1→3) β-d-glucan for differential diagnosis of Pneumocystis pneumonia and Pneumocystis colonization. J. Clin. Microbiol. 2013, 51, 3380–3388. [Google Scholar] [CrossRef] [PubMed]
- Held, J.; Koch, M.S.; Reischl, U.; Danner, T.; Serr, A. Serum (1→3)-β-d-glucan measurement as an early indicator of Pneumocystis jirovecii pneumonia and evaluation of its prognostic value. Clin. Microbiol. Infect. 2011, 17, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Matsuda, S.; Tegoshi, T. Yeast glucan in the cyst wall of Pneumocystis carinii. J. Protozool. 1989, 36, 21S–22S. [Google Scholar] [CrossRef] [PubMed]
- Finkelman, M.A. Pneumocystis jirovecii infection: Cell wall (1–3)-β-d-glucan biology and diagnostic utility. Crit. Rev. Microbiol. 2010, 36, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Mennink-Kersten, M.A.; Ruegebrink, D.; Verweij, P.E. Pseudomonas aeruginosa as a cause of 1,3-β-d-glucan assay reactivity. Clin. Infect. Dis. 2008, 46, 1930–1931. [Google Scholar] [CrossRef] [PubMed]
- Sulahian, A.; Touratier, S.; Ribaud, P. False positive test for aspergillus antigenemia related to concomitant administration of piperacillin and tazobactam. N. Engl. J. Med. 2003, 349, 2366–2367. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for the Prevention and Treatment of Opportunistic Infections in HIV-infected adults and adolescents. Recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. Available online: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5804a1.htm (accessed on 7 September 2015).
- EBPG Expert Group on Renal Transplantation. European Best Practice Guidelines for Renal Transplantation. Section IV: Long-term management of the transplant recipient. IV.7.1 Late infectionsPneumocystis carinii pneumonia. Nephrol. Dial. Transplant. 2002, 17, 36–39. [Google Scholar]
- Kasiske, B.L.; Zeier, M.G.; Chapman, J.R.; Craig, J.C.; Ekberg, H.; Garvey, C.A.; Green, M.D.; Jha, V.; Josephson, M.A.; Kiberd, B.A.; et al. KDIGO clinical practice guideline for the care of kidney transplant recipients: A summary. Kidney Int. 2010, 77, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Higgins, R.M.; Bloom, S.L.; Hopkin, J.M.; Morris, P.J. The risks and benefits of low-dose cotrimoxazole prophylaxis for Pneumocystis pneumonia in renal transplantation. Transplantation 1989, 47, 558–560. [Google Scholar] [PubMed]
- Chapman, J.R.; Marriott, D.J.; Chen, S.C.; Macdonald, P.S. Post-transplant Pneumocystis jirovecii pneumonia: A re-emerged public health problem? Kidney Int. 2013, 84, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Masur, H.; Kaplan, J.E.; Holmes, K.K. Guidelines for preventing opportunistic infections among HIV-infected persons 2002. Recommendations of the U.S. Public Health Service and the Infectious Diseases Society of America. Ann. Intern. Med. 2002, 137, 435–478. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, U.M.; Helweg-Larsen, J. Pneumocystis jiroveci pneumonia (PCP) in HIV-1-negative patients: A retrospective study 2002–2004. Scand. J. Infect. Dis. 2007, 39, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.; Cappelleri, J.C.; Skolnik, P.R.; Lau, J.; Sacks, H.S. A meta-analysis of the relative efficacy and toxicity of Pneumocystis carinii prophylactic regimens. Arch. Intern. Med. 1996, 156, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Torre-Cisneros, J.; de la Mata, M.; Pozo, J.C.; Serrano, P.; Briceno, J.; Solorzano, G.; Mino, G.; Pera, C.; Sanchez-Guijo, P. Randomized trial of weekly sulfadoxine/pyrimethamine vs. daily low-dose trimethoprim-sulfamethoxazole for the prophylaxis of Pneumocystis carinii pneumonia after liver transplantation. Clin. Infect. Dis. 1999, 29, 771–774. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.; Green, H.; Paul, M.; Vidal, L.; Leibovici, L. Prophylaxis for Pneumocystis pneumonia (PCP) in non-HIV immunocompromised patients. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Hughes, W.T. Use of dapsone in the prevention and treatment of Pneumocystis carinii pneumonia: A review. Clin. Infect. Dis. 1998, 27, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Mohle-Boetani, J.; Akula, S.K.; Holodniy, M.; Katzenstein, D.; Garcia, G. The sulfone syndrome in a patient receiving dapsone prophylaxis for Pneumocystis carinii pneumonia. West. J. Med. 1992, 156, 303–306. [Google Scholar] [PubMed]
- Lee, I.; Barton, T.D.; Goral, S.; Doyle, A.M.; Bloom, R.D.; Chojnowski, D.; Korenda, K.; Blumberg, E.A. Complications related to dapsone use for Pneumocystis jirovecii pneumonia prophylaxis in solid organ transplant recipients. Am. J. Transplant. 2005, 5, 2791–2795. [Google Scholar] [CrossRef] [PubMed]
- El-Sadr, W.M.; Murphy, R.L.; Yurik, T.M.; Luskin-Hawk, R.; Cheung, T.W.; Balfour, H.H., Jr.; Eng, R.; Hooton, T.M.; Kerkering, T.M.; Schutz, M.; et al. Atovaquone compared with dapsone for the prevention of Pneumocystis carinii pneumonia in patients with HIV infection who cannot tolerate trimethoprim, sulfonamides, or both. Community Program for Clinical Research on AIDS and the AIDS Clinical Trials Group. N. Engl. J. Med. 1998, 339, 1889–1895. [Google Scholar] [CrossRef] [PubMed]
- Gabardi, S.; Millen, P.; Hurwitz, S.; Martin, S.; Roberts, K.; Chandraker, A. Atovaquone versus trimethoprim-sulfamethoxazole as Pneumocystis jirovecii pneumonia prophylaxis following renal transplantation. Clin. Transplant. 2012, 26, E184–E190. [Google Scholar] [CrossRef] [PubMed]
- Baggish, A.L.; Hill, D.R. Antiparasitic agent atovaquone. Antimicrob. Agents Chemother. 2002, 46, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Saukkonen, K.; Garland, R.; Koziel, H. Aerosolized pentamidine as alternative primary prophylaxis against Pneumocystis carinii pneumonia in adult hepatic and renal transplant recipients. Chest 1996, 109, 1250–1255. [Google Scholar] [CrossRef]
- Vasconcelles, M.J.; Bernardo, M.V.; King, C.; Weller, E.A.; Antin, J.H. Aerosolized pentamidine as Pneumocystis prophylaxis after bone marrow transplantation is inferior to other regimens and is associated with decreased survival and an increased risk of other infections. Biol. Blood Marrow Transplant. 2000, 6, 35–43. [Google Scholar] [CrossRef]
- Hardy, W.D.; Northfelt, D.W.; Drake, T.A. Fatal, disseminated pneumocystosis in a patient with acquired immunodeficiency syndrome receiving prophylactic aerosolized pentamidine. Am. J. Med. 1989, 87, 329–331. [Google Scholar] [CrossRef]
- Zavascki, A.P.; Maia, A.L.; Goldani, L.Z. Pneumocystis jiroveci thyroiditis: Report of 15 cases in the literature. Mycoses 2007, 50, 443–446. [Google Scholar] [CrossRef] [PubMed]
- Sepkowitz, K.A.; Telzak, E.E.; Gold, J.W.; Bernard, E.M.; Blum, S.; Carrow, M.; Dickmeyer, M.; Armstrong, D. Pneumothorax in AIDS. Ann. Intern. Med. 1991, 114, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Jules-Elysee, K.M.; Stover, D.E.; Zaman, M.B.; Bernard, E.M.; White, D.A. Aerosolized pentamidine: Effect on diagnosis and presentation of Pneumocystis carinii pneumonia. Ann. Intern. Med. 1990, 112, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L. 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings. Am. J. Infect. Control 2007, 35, S65–S164. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, J.E.; Benson, C.; Holmes, K.K.; Brooks, J.T.; Pau, A.; Masur, H. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: Recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. MMWR Recomm. Rep. 2009, 58, 1–207. [Google Scholar] [PubMed]
- Carmona, E.M.; Limper, A.H. Update on the diagnosis and treatment of Pneumocystis pneumonia. Ther. Adv. Respir. Dis. 2011, 5, 41–59. [Google Scholar] [CrossRef] [PubMed]
- Briel, M.; Bucher, H.C.; Boscacci, R.; Furrer, H. Adjunctive corticosteroids for Pneumocystis jiroveci pneumonia in patients with HIV-infection. Cochrane Database Syst Rev. 2006. [Google Scholar] [CrossRef]
- Navin, T.R.; Beard, C.B.; Huang, L.; del Rio, C.; Lee, S.; Pieniazek, N.J.; Carter, J.L.; Le, T.; Hightower, A.; Rimland, D. Effect of mutations in Pneumocystis carinii dihydropteroate synthase gene on outcome of P. carinii pneumonia in patients with HIV-1: A prospective study. Lancet 2001, 358, 545–549. [Google Scholar] [PubMed]
- Crothers, K.; Beard, C.B.; Turner, J.; Groner, G.; Fox, M.; Morris, A.; Eiser, S.; Huang, L. Severity and outcome of HIV-associated Pneumocystis pneumonia containing Pneumocystis jirovecii dihydropteroate synthase gene mutations. AIDS 2005, 19, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Wharton, J.M.; Coleman, D.L.; Wofsy, C.B.; Luce, J.M.; Blumenfeld, W.; Hadley, W.K.; Ingram-Drake, L.; Volberding, P.A.; Hopewell, P.C. Trimethoprim-sulfamethoxazole or pentamidine for Pneumocystis carinii pneumonia in the acquired immunodeficiency syndrome: A prospective randomized trial. Ann. Intern. Med. 1986, 105, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Sattler, F.R.; Cowan, R.; Nielsen, D.M.; Ruskin, J. Trimethoprim-sulfamethoxazole compared with pentamidine for treatment of Pneumocystis carinii pneumonia in the acquired immunodeficiency syndrome: A prospective, noncrossover study. Ann. Intern. Med. 1988, 109, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Klein, N.C.; Duncanson, F.P.; Lenox, T.H.; Forszpaniak, C.; Sherer, C.B.; Quentzel, H.; Nunez, M.; Suarez, M.; Kawwaff, O.; Pitta-Alvarez, A.; et al. Trimethoprim-sulfamethoxazole versus pentamidine for Pneumocystis carinii pneumonia in AIDS patients: Results of a large prospective randomized treatment trial. AIDS 1992, 6, 301–305. [Google Scholar] [CrossRef] [PubMed]
- OʼBrien, J.G.; Dong, B.J.; Coleman, R.L.; Gee, L.; Balano, K.B. A 5-year retrospective review of adverse drug reactions and their risk factors in human immunodeficiency virus-infected patients who were receiving intravenous pentamidine therapy for Pneumocystis carinii pneumonia. Clin. Infect. Dis. 1997, 24, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Benfield, T.; Atzori, C.; Miller, R.F.; Helweg-Larsen, J. Second-line salvage treatment of AIDS-associated Pneumocystis jirovecii pneumonia: A case series and systematic review. J. Acquir. Immun. Defic. Syndr. 2008, 48, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Hong, H.L.; Lee, Y.M.; Sung, H.; Kim, S.H.; Choi, S.H.; Kim, Y.S.; Woo, J.H.; Lee, S.O. Is caspofungin really an effective treatment for Pneumocystis jirovecii pneumonia in immunocompromised patients without human immunodeficiency virus infection? Experiences at a single center and a literature review. Scand. J. Infect. Dis. 2013, 45, 484–488. [Google Scholar] [CrossRef] [PubMed]
- Fishman, J.A. Treatment of infection due to Pneumocystis carinii. Antimicrob. Agents Chemother. 1998, 42, 1309–1314. [Google Scholar] [PubMed]
- McKinnell, J.A.; Cannella, A.P.; Injean, P.; Gregson, A. Adjunctive glucocorticoid therapy for non-HIV-related Pneumocystis carinii pneumonia (NH-PCP). Am. J. Transplant. 2014, 14, 982–983. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.I. Muted, but not mute. Am. J. Transplant. 2014, 14, 984. [Google Scholar] [CrossRef] [PubMed]
- Delclaux, C.; Zahar, J.R.; Amraoui, G.; Leleu, G.; Lebargy, F.; Brochard, L.; Schlemmer, B.; Brun-Buisson, C. Corticosteroids as adjunctive therapy for severe Pneumocystis carinii pneumonia in non-human immunodeficiency virus-infected patients: Retrospective study of 31 patients. Clin. Infect. Dis. 1999, 29, 670–672. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.M.; Kim, T.; Sung, H.; Kim, M.N.; Kim, S.H.; Choi, S.H.; Jeong, J.Y.; Woo, J.H.; Kim, Y.S.; Lee, S.O. Outcomes of moderate-to-severe Pneumocystis pneumonia treated with adjunctive steroid in non-HIV-infected patients. Antimicrob. Agents Chemother. 2011, 55, 4613–4618. [Google Scholar] [CrossRef] [PubMed]
- Lemiale, V.; Debrumetz, A.; Delannoy, A.; Alberti, C.; Azoulay, E. Adjunctive steroid in HIV-negative patients with severe Pneumocystis pneumonia. Respir Res. 2013, 14, 87. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iriart, X.; Bouar, M.L.; Kamar, N.; Berry, A. Pneumocystis Pneumonia in Solid-Organ Transplant Recipients. J. Fungi 2015, 1, 293-331. https://doi.org/10.3390/jof1030293
Iriart X, Bouar ML, Kamar N, Berry A. Pneumocystis Pneumonia in Solid-Organ Transplant Recipients. Journal of Fungi. 2015; 1(3):293-331. https://doi.org/10.3390/jof1030293
Chicago/Turabian StyleIriart, Xavier, Marine Le Bouar, Nassim Kamar, and Antoine Berry. 2015. "Pneumocystis Pneumonia in Solid-Organ Transplant Recipients" Journal of Fungi 1, no. 3: 293-331. https://doi.org/10.3390/jof1030293