
Reliability of OMERACT Scoring System in Ultra-High Frequency Ultrasonography of Minor Salivary Glands: Inter-Rater Agreement Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Registration
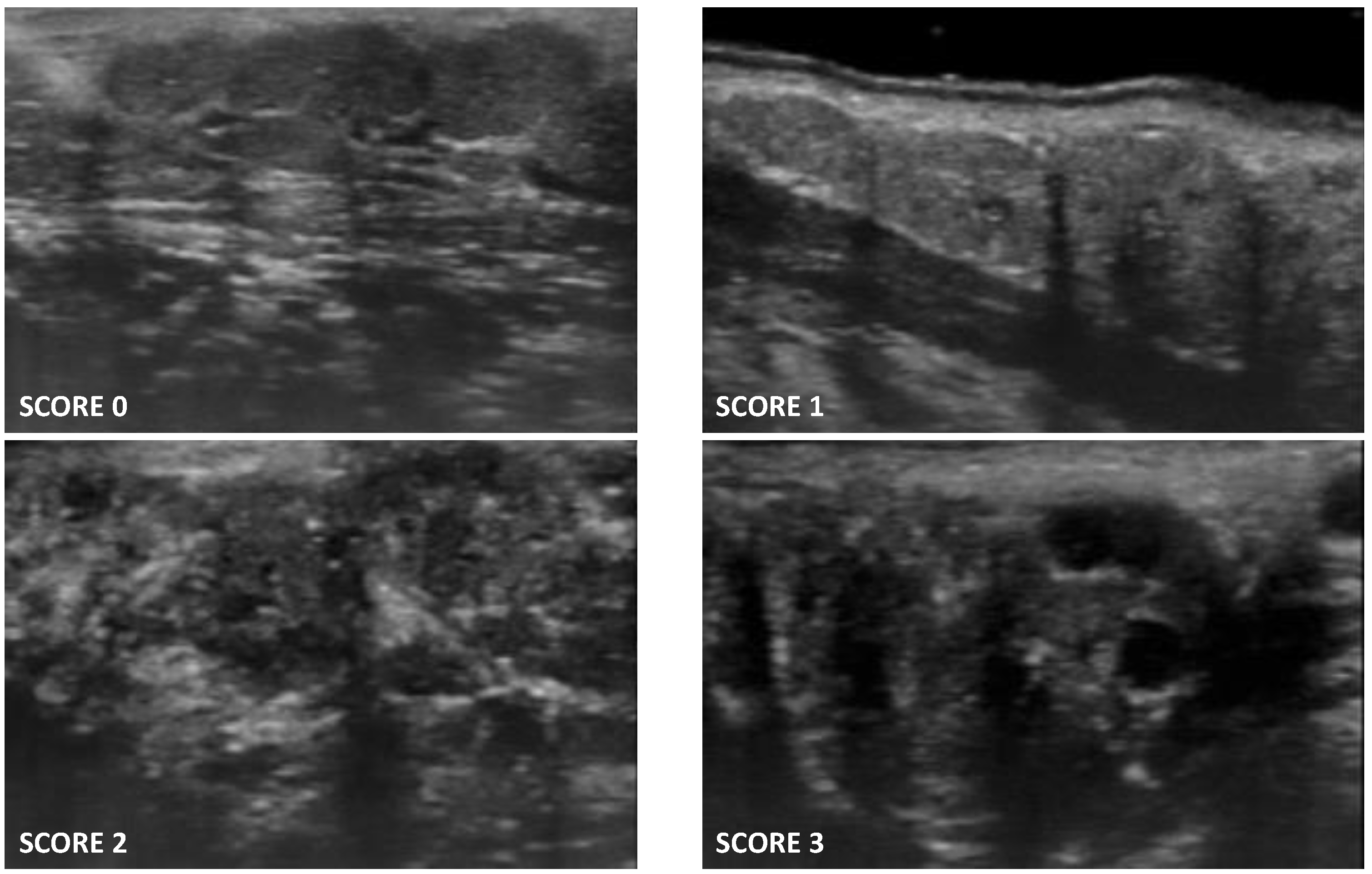
2.2. UHFUS Scoring System of Minor Salivary Glands
- Score 0: normal glandular parenchyma in the absence of alterations;
- Score 1: presence of fine echogenicity in the absence of clear alterations, or slight, diffuse glandular hypoechogenicity, mild glandular alteration;
- Score 2: presence of focal hypoechoic areas, but partial conservation of normal glandular parenchyma, moderate glandular alteration;
- Score 3: diffuse presence of hypoechoic areas in the absence of normal glandular parenchyma, or the presence of glandular fibrosis, severe glandular alteration.
2.3. UHFUS Scans Acquisition Protocol
2.4. Evaluation of Inter-Rater Reliability of UHFUS Scoring System of Minor Salivary Glands
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Image Analysis
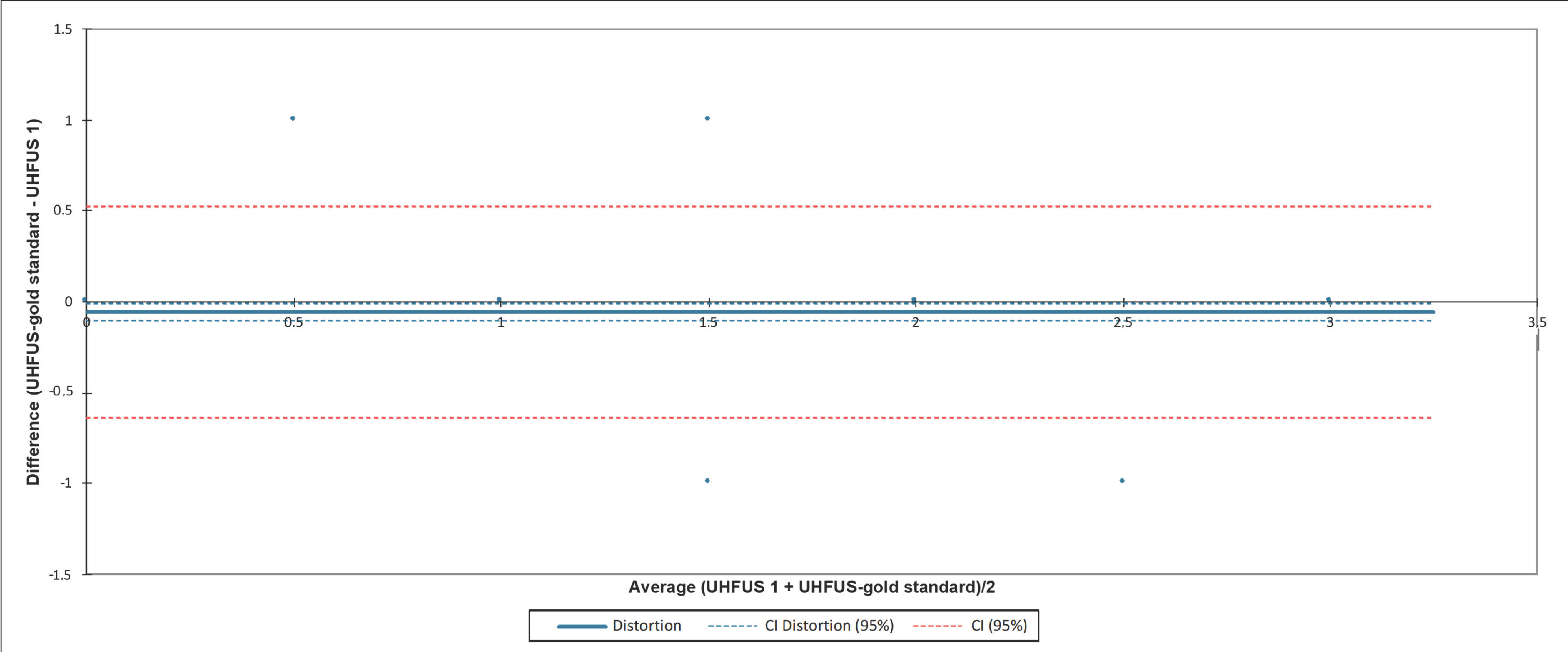
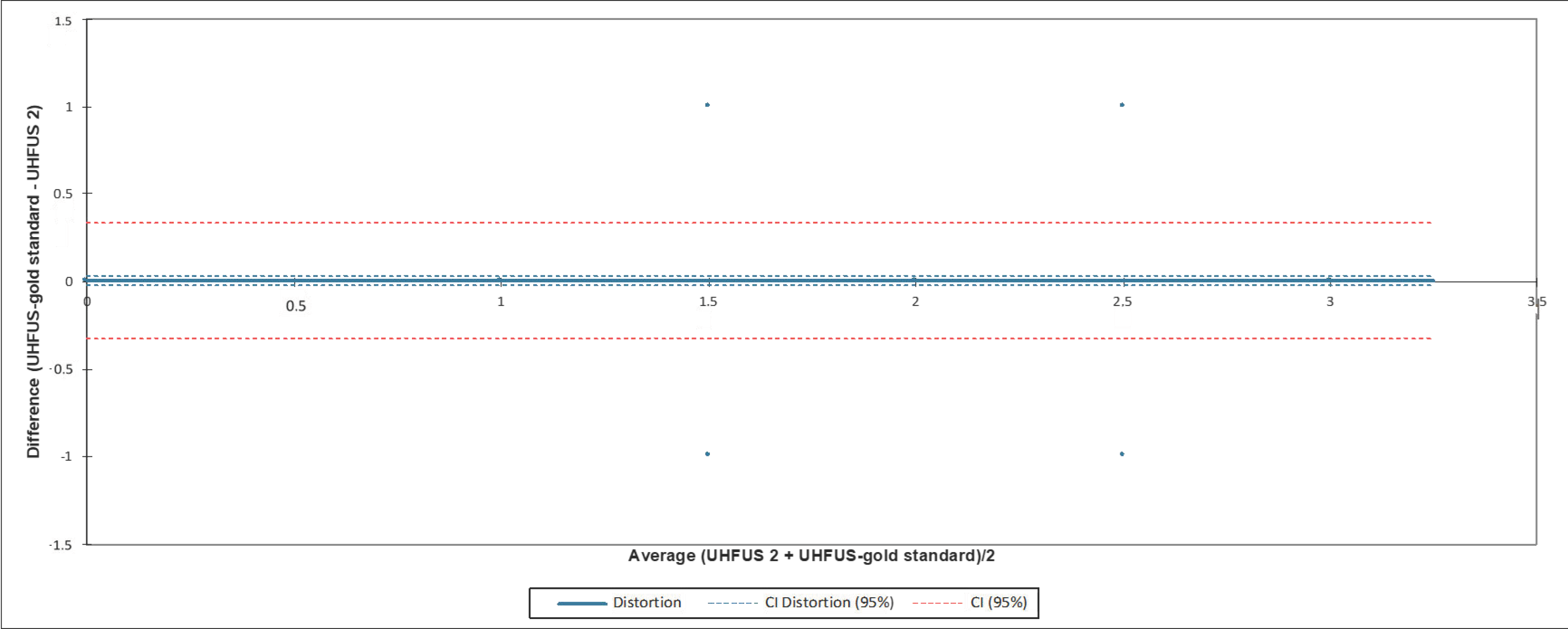
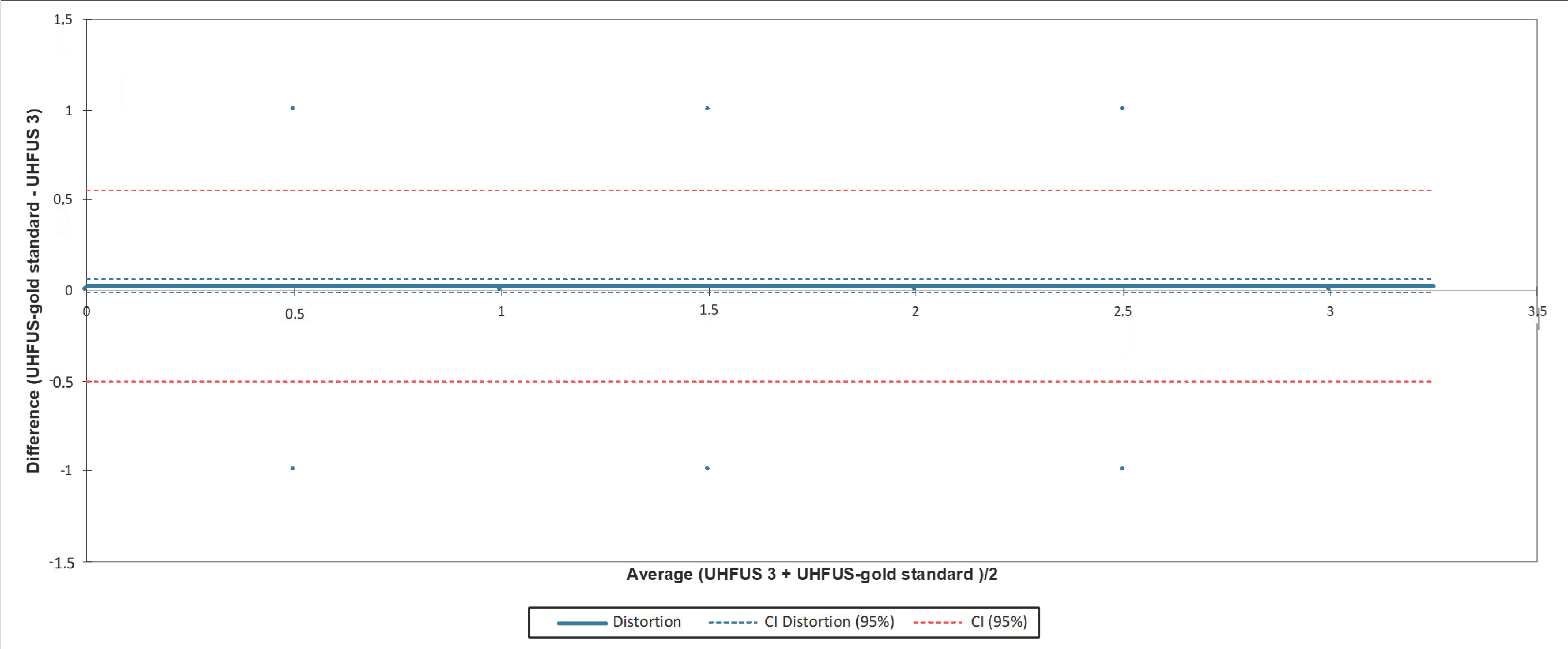
3.3. Analysis of Agreement with the Gold Standard Examiner
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cafaro, G.; Bursi, R.; Chatzis, L.G.; Fulvio, G.; Ferro, F.; Bartoloni, E.; Baldini, C. One year in review 2021: Sjögren’s syndrome. Clin. Exp. Rheumatol. 2021, 39 (Suppl. S133), 3–13. [Google Scholar] [CrossRef] [PubMed]
- Brito-Zerón, P.; Baldini, C.; Bootsma, H.; Bowman, S.J.; Jonsson, R.; Mariette, X.; Sivils, K.; Theander, E.; Tzioufas, A.; Ramos-Casals, M. Sjögren syndrome. Nat. Rev. Dis. Primers 2016, 2, 16047. [Google Scholar] [CrossRef] [PubMed]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017, 69, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Seror, R.; Ravaud, P.; Bowman, S.J.; Baron, G.; Tzioufas, A.; Theander, E.; Gottenberg, J.E.; Bootsma, H.; Mariette, X.; Vitali, C.; et al. EULAR Sjogren’s syndrome disease activity index: Development of a consensus systemic disease activity index for primary Sjogren’s syndrome. Ann. Rheum. Dis. 2010, 69, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Cornec, D.; Jousse-Joulin, S.; Pers, J.O.; Marhadour, T.; Cochener, B.; Boisramé-Gastrin, S.; Nowak, E.; Youinou, P.; Saraux, A.; Devauchelle-Pensec, V. Contribution of salivary gland ultrasonography to the diagnosis of Sjögren’s syndrome: Toward new diagnostic criteria? Arthritis Rheum. 2013, 65, 216–225. [Google Scholar] [CrossRef]
- Jousse-Joulin, S.; Gatineau, F.; Baldini, C.; Baer, A.; Barone, F.; Bootsma, H.; Bowman, S.; Brito-Zerón, P.; Cornec, D.; Dorner, T.; et al. Weight of salivary gland ultrasonography compared to other items of the 2016 ACR/EULAR classification criteria for primary Sjögren’s syndrome. J. Intern. Med. 2020, 287, 180–188. [Google Scholar] [CrossRef]
- Geng, Y.; Li, B.; Deng, X.; Ji, L.; Zhang, X.; Zhang, Z. Salivary gland ultrasound integrated with 2016 ACR/EULAR classification criteria improves the diagnosis of primary Sjögren’s syndrome. Clin. Exp. Rheumatol. 2020, 38, 322–328. [Google Scholar]
- Luciano, N.; Ferro, F.; Bombardieri, S.; Baldini, C. Advances in salivary gland ultrasonography in primary Sjögren’s syndrome. Clin. Exp. Rheumatol. 2018, 36 (Suppl. S114), 159–164. [Google Scholar]
- Terslev, L.; Naredo, E.; Keen, H.I.; Bruyn, G.; Iagnocco, A.; Wakefield, R.J.; Conaghan, P.G.; Maxwell, L.J.; Beaton, D.E.; Boers, M.; et al. The OMERACT Stepwise Approach to Select and Develop Imaging Outcome Measurement Instruments: The Musculoskeletal Ultrasound Example. J. Rheumatol. 2019, 46, 1394–1400. [Google Scholar] [CrossRef]
- Reda, R.; Zanza, A.; Cicconetti, A.; Bhandi, S.; Miccoli, G.; Gambarini, G.; Di Nardo, D. Ultrasound imaging in dentistry: A literature overview. J. Imaging 2021, 7, 238. [Google Scholar] [CrossRef]
- Izzetti, R.; Vitali, S.; Aringhieri, G.; Nisi, M.; Oranges, T.; Dini, V.; Ferro, F.; Baldini, C.; Romanelli, M.; Caramella, D.; et al. Ultra-High Frequency Ultrasound, A Promising Diagnostic Technique: Review of the Literature and Single-Center Experience. Can. Assoc. Radiol. J. 2021, 72, 418–431. [Google Scholar] [CrossRef] [PubMed]
- Izzetti, R.; Ferro, F.; Vitali, S.; Nisi, M.; Fonzetti, S.; Oranges, T.; Donati, V.; Caramella, D.; Baldini, C.; Gabriele, M. Ultra-high frequency ultrasonography (UHFUS)-guided minor salivary gland biopsy: A promising procedure to optimize labial salivary gland biopsy in Sjögren’s syndrome. J. Oral Pathol. Med. 2021, 50, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Ferro, F.; Izzetti, R.; Vitali, S.; Aringhieri, G.; Fonzetti, S.; Donati, V.; Dini, V.; Mosca, M.; Gabriele, M.; Caramella, D.; et al. Ultra-high frequency ultrasonography of labial glands is a highly sensitive tool for the diagnosis of Sjögren’s syndrome: A preliminary study. Clin. Exp. Rheumatol. 2020, 38 (Suppl. S126), 210–215. [Google Scholar] [PubMed]
- Aringhieri, G.; Izzetti, R.; Vitali, S.; Ferro, F.; Gabriele, M.; Baldini, C.; Caramella, D. Ultra-high frequency ultrasound (UHFUS) applications in Sjögren syndrome: Narrative review and current concepts. Gland Surg. 2020, 9, 2248–2259. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Robin, F.; Albert, J.D.; Lescoat, A.; Martel, A.; Perdriger, A.; DeBandt, M.; Maillot, F.; Coiffier, G. Diagnostic performances of ultrasound evaluation of major salivary glands according to the 2019 OMERACT US scoring system. Arthritis Care Res. 2021. preprint. [Google Scholar] [CrossRef]
- Jousse-Joulin, S.; Nowak, E.; Cornec, D.; Brown, J.; Carr, A.; Carotti, M.; Fisher, B.; Fradin, J.; Hocevar, A.; Jonsson, M.V.; et al. Salivary gland ultrasound abnormalities in primary Sjögren’s syndrome: Consensual US-SG core items definition and reliability. RMD Open 2017, 3, e000364. [Google Scholar] [CrossRef] [Green Version]
- De Vita, S.; Lorenzon, G.; Rossi, G.; Sabella, M.; Fossaluzza, V. Salivary gland echography in primary and secondary Sjögren’s syndrome. Clin. Exp. Rheumatol. 1992, 10, 351–356. [Google Scholar]
- Hocevar, A.; Ambrozic, A.; Rozman, B.; Kveder, T.; Tomsic, M. Ultrasonographic changes of major salivary glands in primary Sjogren’s syndrome. Diagnostic value of a novel scoring system. Rheumatology 2005, 44, 768–772. [Google Scholar] [CrossRef] [Green Version]
- Delli, K.; Arends, S.; van Nimwegen, J.F.; Dijkstra, P.U.; Stel, A.J.; Spijkervet, F.; Bootsma, H.; Vissink, A. Ultrasound of the Major Salivary Glands is a Reliable Imaging Technique in Patients with Clinically Suspected Primary Sjögren’s Syndrome. Ultraschall Med. 2018, 39, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Jousse-Joulin, S.; Milic, V.; Jonsson, M.V.; Plagou, A.; Theander, E.; Luciano, N.; Rachele, P.; Baldini, C.; Bootsma, H.; Vissink, A.; et al. Is salivary gland ultrasonography a useful tool in Sjögren’s syndrome? A systematic review. Rheumatology 2016, 55, 789–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jousse-Joulin, S.; D’Agostino, M.A.; Nicolas, C.; Naredo, E.; Ohrndorf, S.; Backhaus, M.; Tamborrini, G.; Chary-Valckenaere, I.; Terslev, L.; Iagnocco, A.; et al. Video clip assessment of a salivary gland ultrasound scoring system in Sjögren’s syndrome using consensual definitions: An OMERACT ultrasound working group reliability exercise. Ann. Rheum. Dis. 2019, 78, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Zabotti, A.; Zandonella Callegher, S.; Tullio, A.; Vukicevic, A.; Hočevar, A.; Milic, V.; Cafaro, G.; Carotti, M.; Delli, K.; De Lucia, O.; et al. Salivary Gland Ultrasonography in Sjögren’s Syndrome: A European Multicenter Reliability Exercise for the HarmonicSS Project. Front. Med. 2020, 7, 581248. [Google Scholar] [CrossRef]
- Izzetti, R.; Oranges, T.; Janowska, A.; Gabriele, M.; Graziani, F.; Romanelli, M. The Application of Ultra-High-Frequency Ultrasound in Dermatology and Wound Management. Int. J. Low Extrem. Wounds 2020, 19, 334–340. [Google Scholar] [CrossRef]
- Oranges, T.; Janowska, A.; Vitali, S.; Loggini, B.; Izzetti, R.; Romanelli, M.; Dini, V. Dermatoscopic and ultra-high frequency ultrasound evaluation in cutaneous postradiation angiosarcoma. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e741. [Google Scholar] [CrossRef]
- Wang, B.; Chen, S.; Zheng, Q.; Li, Y.; Zhang, X.; Xuan, J.; Liu, Y.; Shi, G. Early diagnosis and treatment for Sjögren’s syndrome: Current challenges, redefined disease stages and future prospects. J. Autoimmun. 2021, 117, 102590. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OMERACT Scoring System | ICC | 95% Cis (Lower, Upper Bound) |
|---|---|---|
| Score 0 | 0.938 | (0.912, 0.964) |
| Score 1 | 0.953 | (0.928, 0.979) |
| Score 2 | 0.873 | (0.853, 0.902) |
| Score 3 | 0.785 | (0.756, 0.847) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izzetti, R.; Fulvio, G.; Nisi, M.; Gennai, S.; Graziani, F. Reliability of OMERACT Scoring System in Ultra-High Frequency Ultrasonography of Minor Salivary Glands: Inter-Rater Agreement Study. J. Imaging 2022, 8, 111. https://doi.org/10.3390/jimaging8040111
Izzetti R, Fulvio G, Nisi M, Gennai S, Graziani F. Reliability of OMERACT Scoring System in Ultra-High Frequency Ultrasonography of Minor Salivary Glands: Inter-Rater Agreement Study. Journal of Imaging. 2022; 8(4):111. https://doi.org/10.3390/jimaging8040111
Chicago/Turabian StyleIzzetti, Rossana, Giovanni Fulvio, Marco Nisi, Stefano Gennai, and Filippo Graziani. 2022. "Reliability of OMERACT Scoring System in Ultra-High Frequency Ultrasonography of Minor Salivary Glands: Inter-Rater Agreement Study" Journal of Imaging 8, no. 4: 111. https://doi.org/10.3390/jimaging8040111