
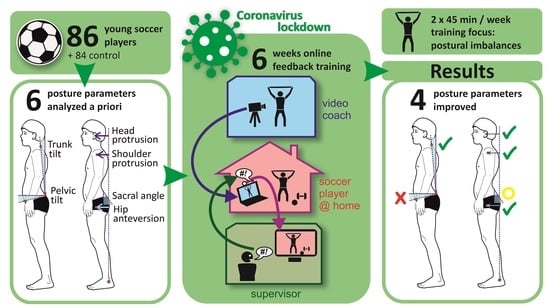
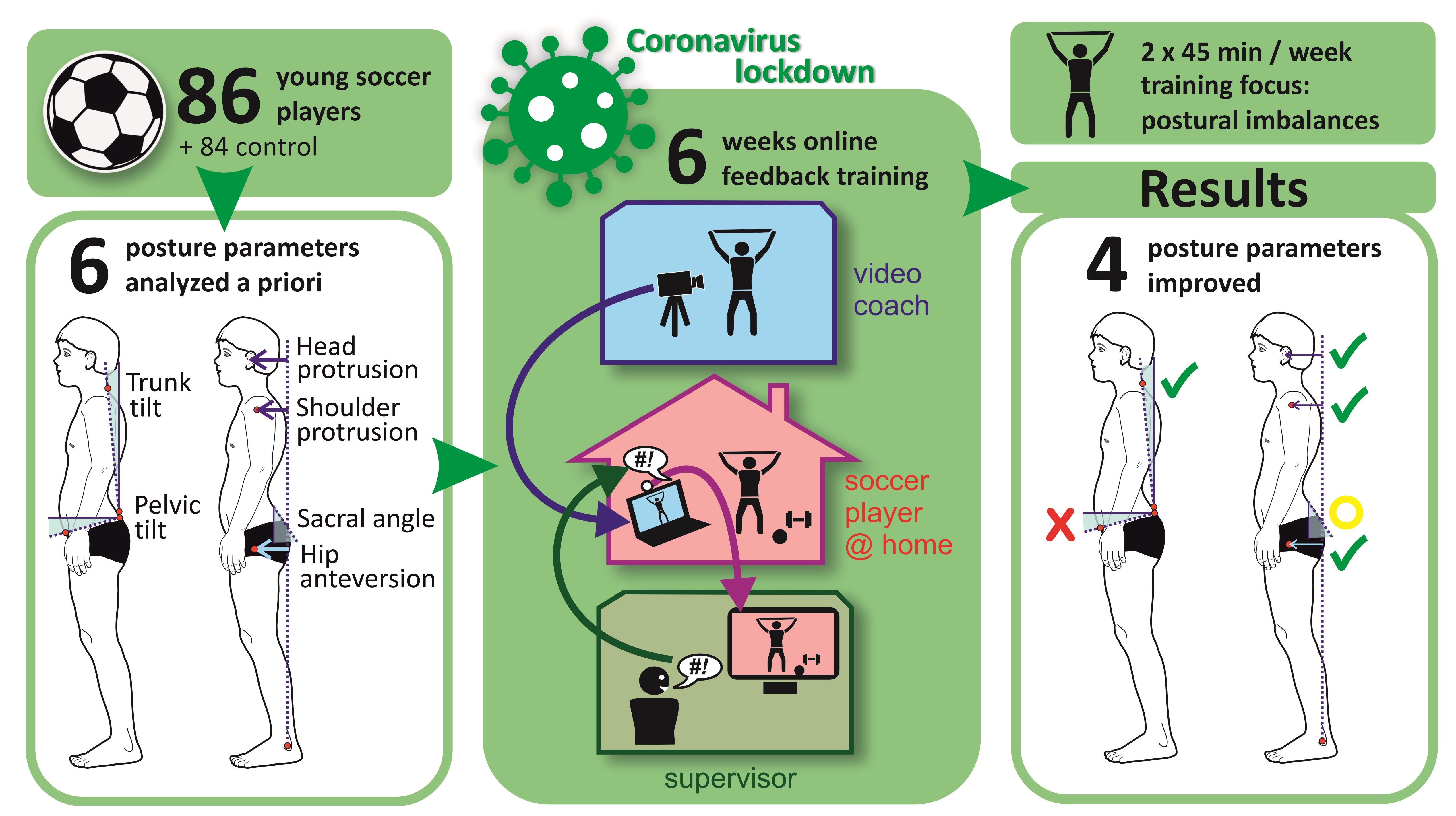
Effects of Feedback-Supported Online Training during the Coronavirus Lockdown on Posture in Children and Adolescents

 ,
,  , ,
, , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Posture Analysis
2.3. Intervention
- 1.
- Strengthening of the target muscles for segmental postural improvement;
- 2.
- Feasibility with aids available in the household;
- 3.
- Easy to correct via video.
2.4. Statistics
3. Results
3.1. Interaction Effects
3.2. Main Effects of “Between-Subject Factors” (Group)
3.3. Main Effects of “Within-Subject Factors” (Time)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kratenova, J.; Zejglicova, K.; Malý, M.; Filipová, V. Prevalence and Risk Factors of Poor Posture in School Children in the Czech Republic. J. Sch. Health 2007, 77, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Wirth, B.; Humphreys, B.K. Pain characteristics of adolescent spinal pain. BMC Pediatr. 2015, 15, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-H. Effects of forward head posture on static and dynamic balance control. J. Phys. Ther. Sci. 2016, 28, 274–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czaprowski, D.; Stoliński, Ł.; Tyrakowski, M.; Kozinoga, M.; Kotwicki, T. Non-structural misalignments of body posture in the sagittal plane. Scoliosis Spinal Disord. 2018, 13, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolphens, M.; Cagnie, B.; Coorevits, P. Sagittal standing posture and its association with spinal pain: A school-based epidemiological study of 1196 Flemish adolescents before age at peak height velocity. Spine 2012, 37, 1657–1666. [Google Scholar] [CrossRef]
- Kim, M.S.; Cha, Y.J.; Choi, J.D. Correlation between forward head posture, respiratory functions, and respiratory accessory muscles in young adults. J. Back Musculoskelet. Rehabil. 2017, 30, 711–715. [Google Scholar] [CrossRef]
- Buchtelová, E.; Tichy, M.; Vaniková, K. Influence of muscular imbalances on pelvic position and lumbar lordosis: A theoretical basis. J. Nurs. Soc. Stud. Public Health Rehabil. 2013, 1, 25–36. [Google Scholar]
- Ludwig, O.; Mazet, C.; Mazet, D.; Hammes, A.; Schmitt, E. Age-dependency of posture parameters in children and adolescents. J. Phys. Ther. Sci. 2016, 28, 1607–1610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foltran-Mescollotto, F.; Gonçalves, B.; de Castro-Carletti, E.M.; Oliveira, A.B.; Pelai, E.B.; Rodrigues-Bigaton, D. Smartphone addiction and the relationship with head and neck pain and electromiographic activity of masticatory muscles. Work 2021, 68, 633–640. [Google Scholar] [CrossRef] [PubMed]
- David, D.; Giannini, C.; Chiarelli, F.; Mohn, A. Text neck syndrome in children and adolescents. Int. J. Environ. Res. Public Health 2021, 18, 1565. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.C.E.; Anedda, B.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Nigg, C.; Niessner, C.; Oriwol, D.; Worth, A.; Woll, A. Physical activity and screen time of children and adolescents before and during the COVID-19 lockdown in Germany: A natural experiment. Sci. Rep. 2020, 10, 21780. [Google Scholar] [CrossRef] [PubMed]
- Chambonniere, C.; Lambert, C.; Fearnbach, N.; Tardieu, M.; Fillon, A.; Genin, P.; Larras, B.; Melsens, P.; Bois, J.; Pereira, B.; et al. Effect of the COVID-19 lockdown on physical activity and sedentary behaviors in French children and adolescents: New results from the ONAPS national survey. Eur. J. Integr. Med. 2021, 43, 101308. [Google Scholar] [CrossRef] [PubMed]
- Guan, H.; Okely, A.D.; Aguilar-Farias, N.; Del Pozo Cruz, B.; Draper, C.E.; El Hamdouchi, A.; Florindo, A.A.; Jáuregui, A.; Katzmarzyk, P.T.; Kontsevaya, A.; et al. Promoting healthy movement behaviours among children during the COVID-19 pandemic. Lancet Child Adolesc. Health 2020, 4, 416–418. [Google Scholar] [CrossRef]
- Caneiro, J.P.; O’Sullivan, P.; Burnett, A.; Barach, A.; O’Neil, D.; Tveit, O.; Olafsdottir, K. The influence of different sitting postures on head/neck posture and muscle activity. Man. Ther. 2010, 15, 54–60. [Google Scholar] [CrossRef]
- Ertekin, E.; Günaydın, Ö.E. Neck pain in rounded shoulder posture: Clinico-radiologic correlation by shear wave elastography. Int. J. Clin. Pract. 2021, 75, e14240. [Google Scholar] [CrossRef]
- Ruivo, R.M.; Pezarat-Correia, P.; Carita, A.I. Cervical and shoulder postural assessment of adolescents between 15 and 17 years old and association with upper quadrant pain. Braz. J. Phys. Ther. 2014, 18, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Häkkinen, A.; Salo, P.; Tarvainen, U.; Wiren, K.; Ylinen, J. Effect of manual therapy and stretching on neck muscle strength and mobility in chronic neck pain. J. Rehabil. Med. 2007, 39, 575–579. [Google Scholar] [CrossRef] [Green Version]
- Tjønndal, A. # Quarantineworkout: The Use of Digital Tools and Online Training Among Boxers and Boxing Coaches During the COVID-19 Pandemic. Front. Sports Act. Living 2020, 2, 589483. [Google Scholar] [CrossRef]
- Parker, K.; Uddin, R.; Ridgers, N.D.; Brown, H.; Veitch, J.; Salmon, J.; Timperio, A.; Sahlqvist, S.; Cassar, S.; Toffoletti, K.; et al. The Use of Digital Platforms for Adults’ and Adolescents’ Physical Activity During the COVID-19 Pandemic (Our Life at Home): Survey Study. J. Med. Internet Res. 2021, 23, e23389. [Google Scholar] [CrossRef]
- Rohleder, B. Kinder- & Jugendstudie 2022 [Children & Youth Study 2022]; Bitcom Research: Berlin, Germany, 2022; p. 4. [Google Scholar]
- Fourchet, F.; Materne, O.; Rajeb, A.; Horobeanu, C.; Farooq, A. Pelvic Tilt: Reliability of Measuring the Standing Position and Range of Motion in Adolescent Athletes. Br. J. Sports Med. 2014, 48, 594. [Google Scholar] [CrossRef]
- Hazar, Z.; Karabicak, G.O.; Tiftikci, U. Reliability of photographic posture analysis of adolescents. J. Phys. Ther. Sci. 2015, 27, 3123–3126. [Google Scholar] [CrossRef]
- Sikka, I.; Chawla, C.; Seth, S.; Alghadir, A.H.; Khan, M. Effects of Deep Cervical Flexor Training on Forward Head Posture, Neck Pain, and Functional Status in Adolescents Using Computer Regularly. BioMed Res. Int. 2020, 2020, 8327565. [Google Scholar] [CrossRef]
- Ludwig, O.; Fröhlich, M.; Schmitt, E. Therapy of poor posture in adolescents: Sensorimotor training increases the effectiveness of strength training to reduce increased anterior pelvic tilt. Cogent Med. 2016, 3, 1262094. [Google Scholar] [CrossRef]
- Mair, P.; Wilcox, R. Robust statistical methods in R using the WRS2 package. Behav. Res. Methods 2020, 52, 464–488. [Google Scholar] [CrossRef]
- Waskom, M.L. Seaborn: Statistical data visualization. J. Open Source Softw. 2021, 6, 3021. [Google Scholar] [CrossRef]
- Dolphens, M.; Vansteelandt, S.; Cagnie, B.; Nijs, J.; Danneels, L. Factors associated with low back and neck pain in young adolescence: A multivariable modeling study. Physiotherapy 2015, 101, e1090–e1091. [Google Scholar] [CrossRef] [Green Version]
- Ruivo, R.M.; Pezarat-Correia, P.; Carita, A.I. Effects of a Resistance and Stretching Training Program on Forward Head and Protracted Shoulder Posture in Adolescents. J. Manip. Physiol. Ther. 2017, 40, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sheikhhoseini, R.; Shahrbanian, S.; Sayyadi, P.; O’Sullivan, K. Effectiveness of therapeutic exercise on forward head posture: A systematic review and meta-analysis. J. Manip. Physiol. Ther. 2018, 41, 530–539. [Google Scholar] [CrossRef]
- Dolphens, M.; Vansteelandt, S.; Cagnie, B.; Vleeming, A.; Nijs, J.; Vanderstraeten, G.; Danneels, L. Multivariable modeling of factors associated with spinal pain in young adolescence. Eur. Spine J. 2016, 25, 2809–2821. [Google Scholar] [CrossRef]
- Bruhn, S.; Kullmann, N.; Gollhofer, A. Combinatory Effects of High-Intensity-Strength Training and Sensorimotor Training on Muscle Strength. Int. J. Sport. Med. 2006, 27, 401–406. [Google Scholar] [CrossRef]
- Bansal, S.; Katzman, W.B.; Giangregorio, L.M. Exercise for Improving Age-Related Hyperkyphotic Posture: A Systematic Review. Arch. Phys. Med. Rehabil. 2014, 95, 129–140. [Google Scholar]
- Kim, D.; Cho, M.; Park, Y.; Yang, Y. Effect of an exercise program for posture correction on musculoskeletal pain. J. Phys. Ther. Sci. 2015, 27, 1791–1794. [Google Scholar] [CrossRef] [PubMed]
- Park, H.C.; Kim, Y.-S.; Seok, S.-H.; Lee, S.-K. The effect of complex training on the children with all of the deformities including forward head, rounded shoulder posture, and lumbar lordosis. J. Exerc. Rehabil. 2014, 10, 172–175. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Zoom (N = 86) | Control (N = 84) | |
|---|---|---|
| Age [years] | 15.6 ± 1.6 | 15.7 ± 1.6 |
| Weight [kg] | 63.0 ± 12.2 | 65.3 ± 10.9 |
| Height [cm] | 173.0 ± 9.8 | 174.1 ± 9.0 |
| Age | N | Forward Head | Protracted Shoulder | Scapulae Alatae | Pelvic Anteversion | Increased Pelvic Tilt | Hunchback |
|---|---|---|---|---|---|---|---|
| 13–14 | 17 | 8/47% | 10/59% | 3/18% | 2/12% | 8/47% | 2/12% |
| 14–15 | 17 | 11/65% | 12/71% | 1/6% | 11/65% | 3/18% | 7/41% |
| 15–16 | 20 | 11/55% | 11/55% | 3/15% | 11/55% | 4/20% | 2/10% |
| 16–17 | 20 | 8/40% | 7/35% | 2/10% | 10/50% | 1/5% | 5/25% |
| 17–19 | 22 | 14/64% | 11/50% | 1/5% | 15/68% | 3/14% | 5/23% |
| Sum | 96 | 52/54% | 51/53% | 10/10% | 49/51% | 19/20% | 21/22% |
| Exercise | Target Muscles | Execution |
|---|---|---|
| #1 Swimmer |
| Starting position: Prone, arms and legs extended, feet slightly off the floor, head slightly raised, looking down towards the floor. Execution: Bring arms back in a motion similar to breaststroke with the thumb pointing upwards. Raise the arms above bottles placed at the sides at shoulder height and then lower them again. Consciously pull the shoulder blades together. Keep the legs in a straight position. |
| #2 Reverse Butterfly in Standing Position |
| Starting position: Stand hip-width apart, knees slightly bent, upper body bent forward. Keep back straight throughout the exercise. Hold dumbbells/bottles in upper grip and bend arms slightly. Execution: Raise arms sideways until elbows are level with shoulders, contracting scapulae. Slowly lower the arms to the sides. |
| #3 Torso Rotation with Lunge Backward |
| Starting position: Lunge backwards, hold exercise ball in front of the body with arms outstretched, tense abdomen. Execution: Slowly rotate the upper body as far as possible, always looking at the ball, hold briefly and then rotate to the other side. |
| #4 Push-Ups on the Ball |
| Starting position: Lean on the exercise ball with bent forearms; upper body, buttocks and legs in a straight line, keep tension. Execution: Lower arms perform a circular movement with the ball, keep body tension. |
| #5 Rowing with Exercise Band in Standing Position |
| Starting position: Stand hip-width apart, knees slightly bent, upper body bent forward. Back is straight. Hold the exercise band around the feet with both hands, arms slightly bent. Execution: Draw shoulder blades together, then tighten the exercise band with bent arms, hold position briefly, then slowly return to starting position. |
| #6 Pelvic lift with Exercise Ball |
| Starting position: Supine, heels on the exercise ball, body forms a straight line and has tension, only shoulders and arms support the body, head lies relaxed on the floor in extension of the spine. Execution: Heels are pulled towards the buttocks, pelvis is lifted up to 90° flexion in the knee joint, then slowly return to starting position. |
| #7 Squat with Bar |
| Starting position: Feet slightly wider than shoulders, knees slightly out, hold broomstick above head with arms extended. Execution: Lower buttocks backwards in a controlled manner, back remains straight, do not push knees over toes, always turn knees slightly outwards, bend until 90° flexion in knee joint, then return to starting position. |
| #8 Neck Press |
| Starting position: Sitting on the floor, training band around the back of the head, holding both ends with the hands, upper body upright, back straight, hands at forehead level in front of the head. Execution: Head is moved backwards slowly and in a controlled manner. |
| Group | Zoom | Control | ||
|---|---|---|---|---|
| Time | Pre | Post | Pre | Post |
| Head protrusion [% BH] | 4.4 ± 1.8 | 1.8 ± 1.3 | 4.0 ± 1.6 | 3.9 ± 1.5 |
| Shoulder protrusion [% BH] | 3.1 ± 1.8 | 1.4 ± 1.0 | 3.2 ± 1.5 | 3.1 ± 1.6 |
| Hip anteversion [% BH] | 3.1 ± 1.4 | 2.2 ± 1.2 | 3.1 ± 1.1 | 3.3 ± 4.7 |
| Trunk tilt [°] | 3.6 ± 1.8 | 2.1 ±1.3 | 2.8 ± 1.3 | 3.6 ± 1.4 |
| Pelvic tilt [°] | 9.5 ± 5.6 | 9.7 ± 3.6 | 9.9 ± 3.7 | 9.7 ± 4.4 |
| Sacrum angle [°] | 21.8 ± 7.9 | 17.9 ± 6.0 | 17.8 ± 5.8 | 12.4 ± 5.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ludwig, O.; Dindorf, C.; Schuh, T.; Haab, T.; Marchetti, J.; Fröhlich, M. Effects of Feedback-Supported Online Training during the Coronavirus Lockdown on Posture in Children and Adolescents. J. Funct. Morphol. Kinesiol. 2022, 7, 88. https://doi.org/10.3390/jfmk7040088
Ludwig O, Dindorf C, Schuh T, Haab T, Marchetti J, Fröhlich M. Effects of Feedback-Supported Online Training during the Coronavirus Lockdown on Posture in Children and Adolescents. Journal of Functional Morphology and Kinesiology. 2022; 7(4):88. https://doi.org/10.3390/jfmk7040088
Chicago/Turabian StyleLudwig, Oliver, Carlo Dindorf, Torsten Schuh, Thomas Haab, Johannes Marchetti, and Michael Fröhlich. 2022. "Effects of Feedback-Supported Online Training during the Coronavirus Lockdown on Posture in Children and Adolescents" Journal of Functional Morphology and Kinesiology 7, no. 4: 88. https://doi.org/10.3390/jfmk7040088