
Characterization of Ag-Ion Releasing Zeolite Filled 3D Printed Resins
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials Used
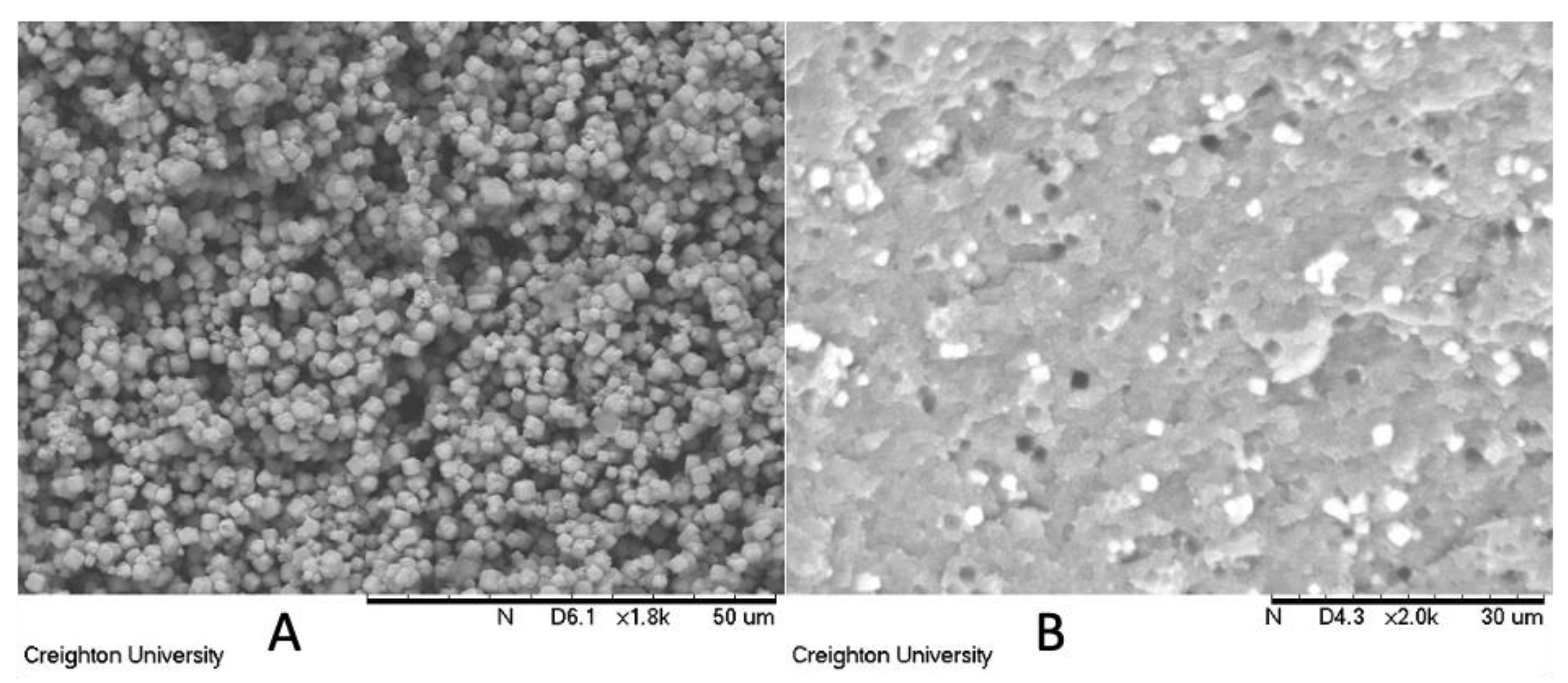
2.2. Formulations and Scanning Electron Microscopy (SEM)
2.3. Polymerization Kinetics
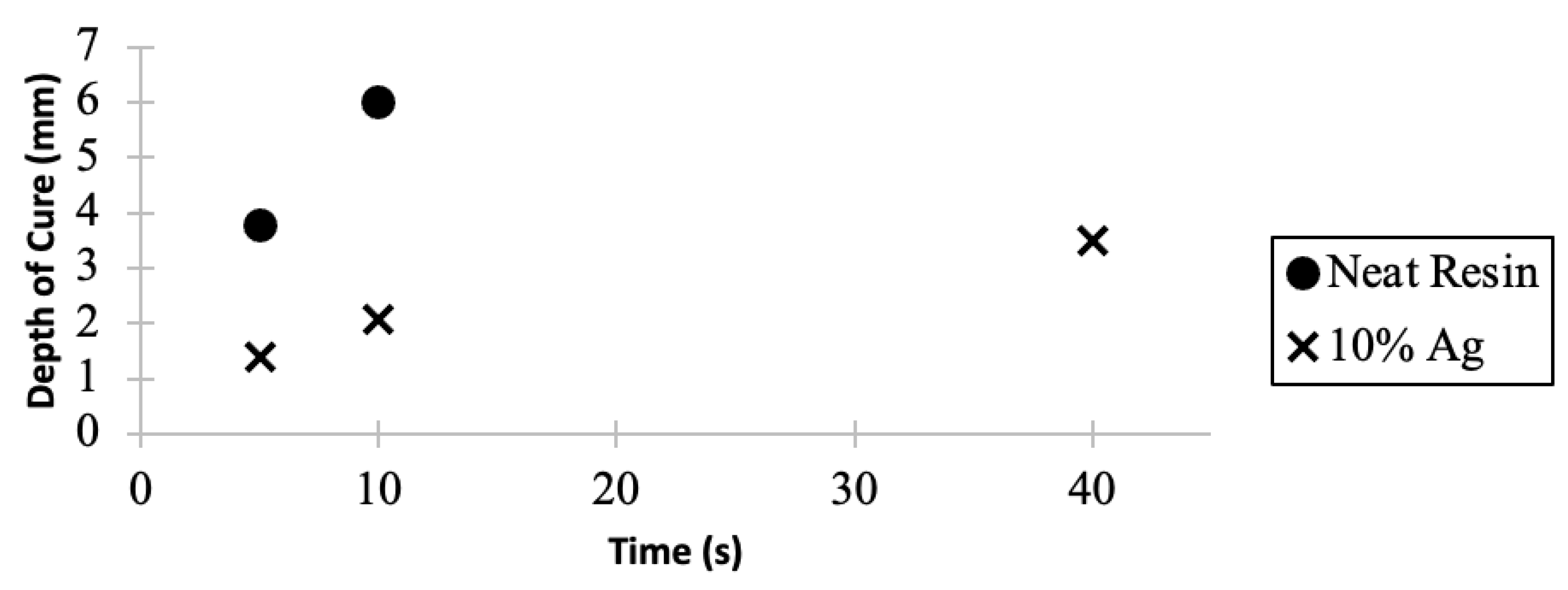
2.4. Depth of Cure
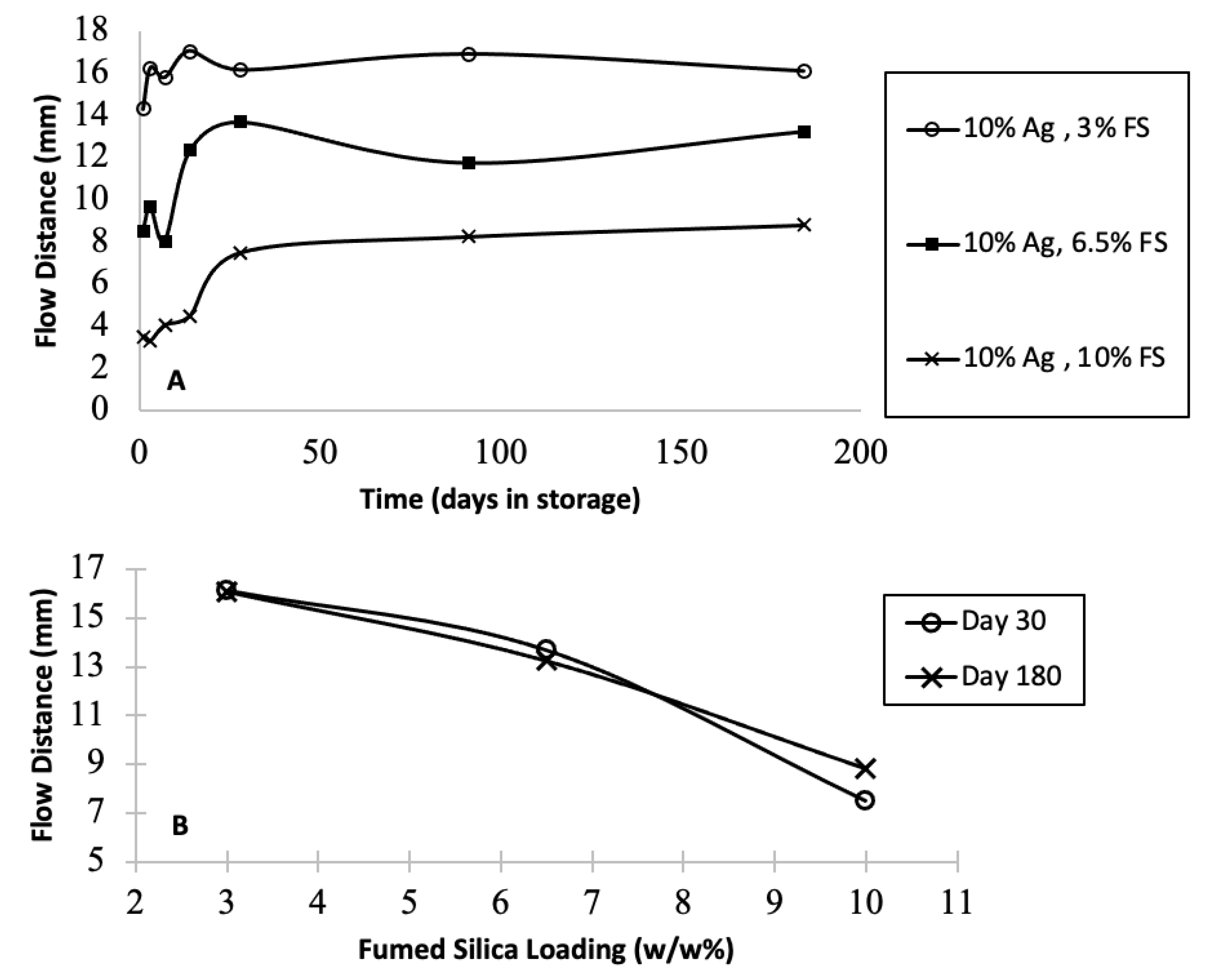
2.5. Flow and Stability
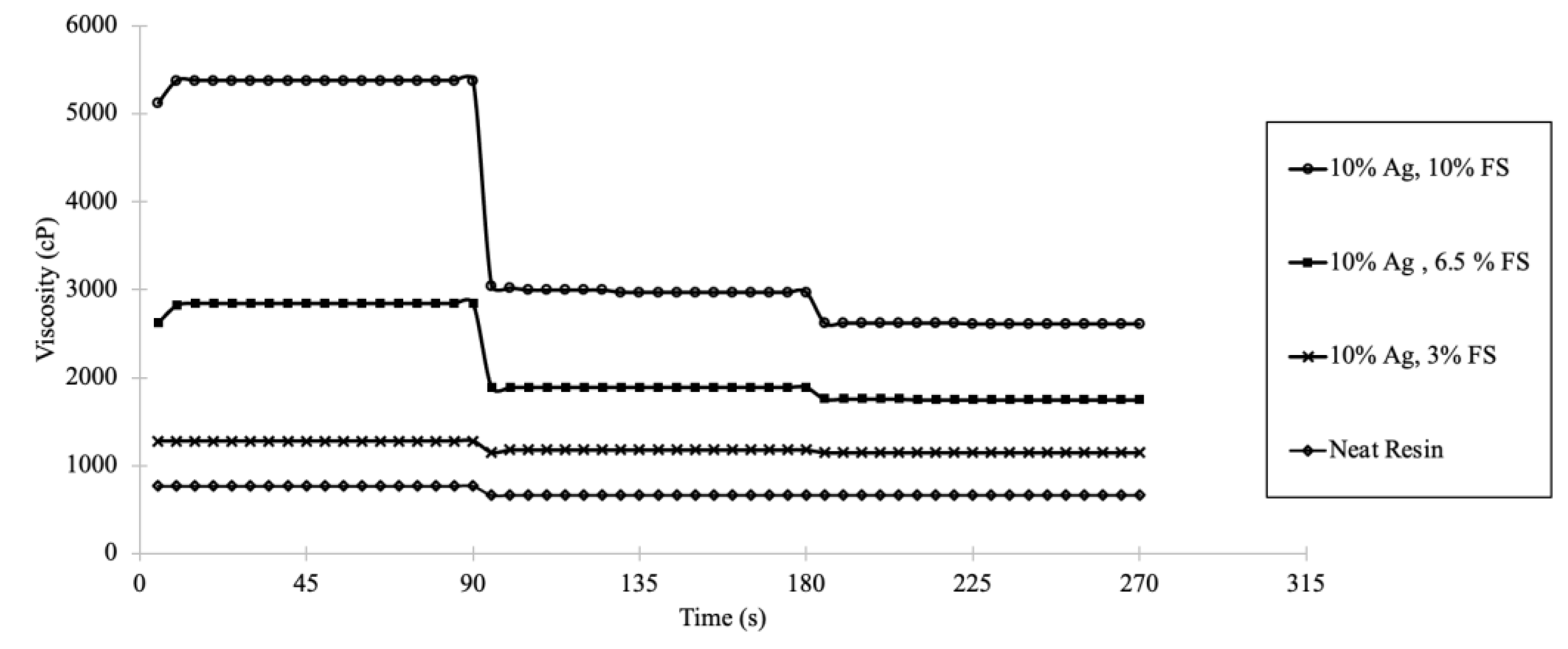
2.6. Viscosity
2.7. Flexural Strength
2.8. Silver Ion Release
2.9. Cell Culture and Virus Assays
3. Results
3.1. Scanning Electron Microscopy
3.2. Polymerization Kinetics
3.3. Depth of Cure
3.4. Colloid Flow Measurement
3.5. Viscosity
3.6. Flexural Strength
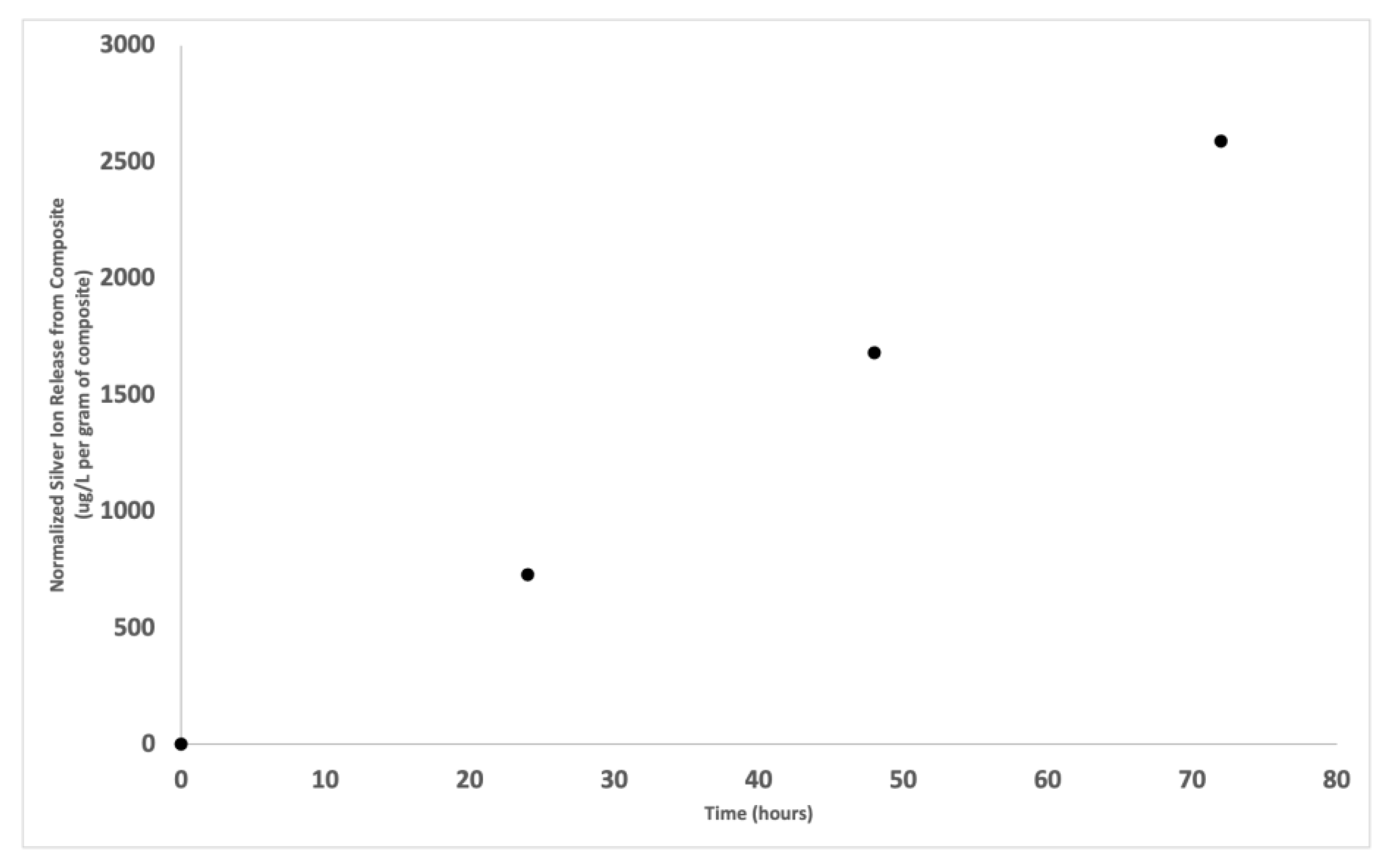
3.7. Silver Ion Release
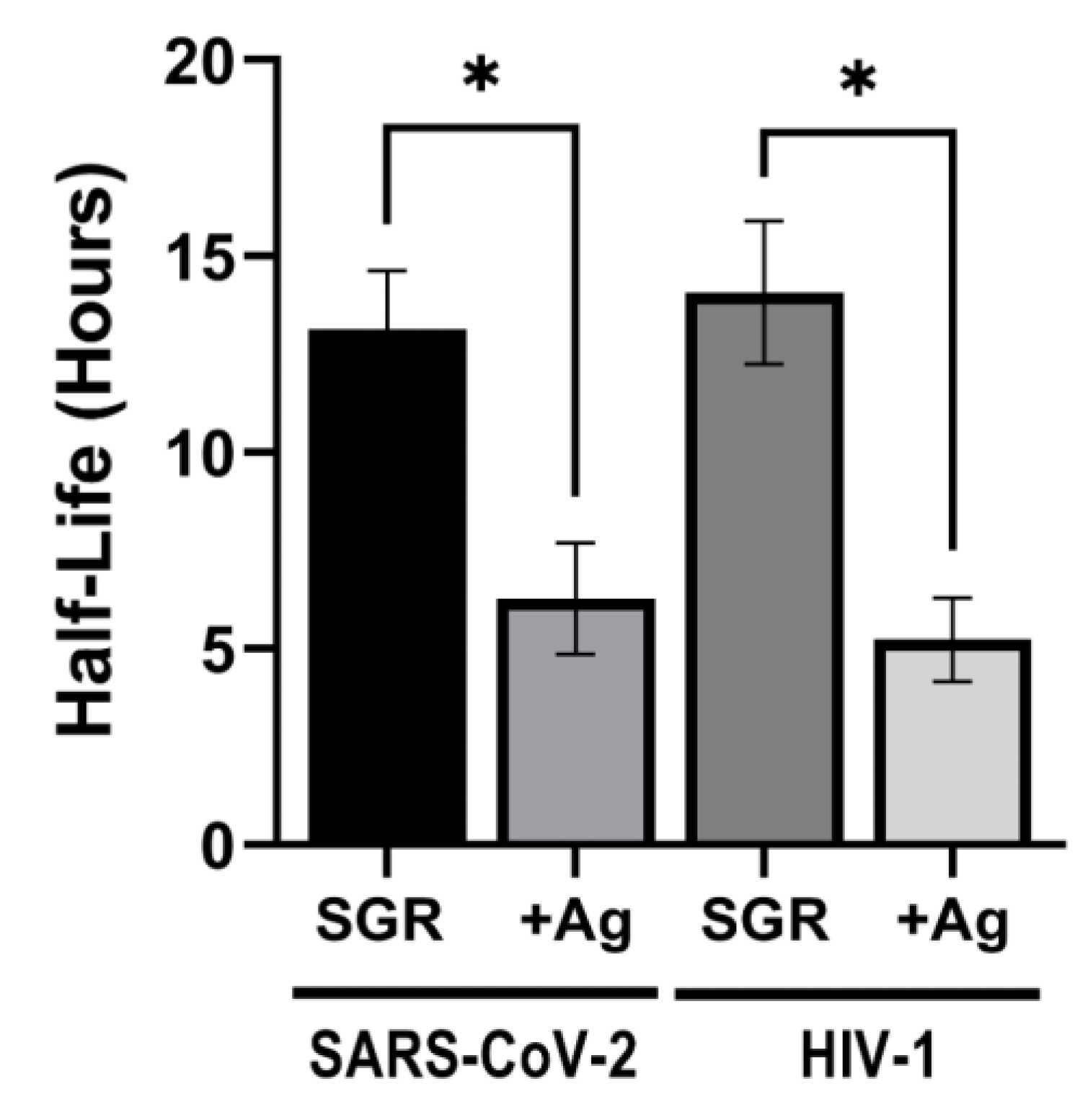
3.8. Antiviral Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stansbury, J.; Idacavage, M. 3D printing with polymers: Challenges among expanding options and opportunities. Dent. Mater. 2015, 32, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Turkyilmaz, I.; Wilkins, G. 3D printing in dentistry—Exploring the new horizons. J. Dent. Sci. 2021, 16, 1037–1038. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.-S.; Jiang, H.B. A Review of 3D Printing in Dentistry: Technologies, Affecting Factors, and Applications. Scanning 2021, 2021, 9950131. [Google Scholar] [CrossRef] [PubMed]
- Della Bona, A.; Cantelli, V.; Britto, V.; Collares, K.; Stansbury, J. 3D printing restorative materials using a stereolithographic technique: A systematic review. Dent. Mater. 2021, 37, 336–350. [Google Scholar] [CrossRef]
- Sehrawat, S.; Kumar, A.; Prabhakar, M.; Nindra, J. The expanding domains of 3D printing pertaining to the specialty of orthodontics. Mater. Today Proc. 2022, 50, 1611–1618. [Google Scholar] [CrossRef]
- Schweiger, J.; Edelhoff, D.; Güth, J. 3D Printing in Digital Prosthetic Dentistry: An Overview of Recent Developments in Additive Manufacturing. J. Clin. Med. 2021, 10, 2010. [Google Scholar] [CrossRef]
- Ma, Y.; Xie, L.; Yang, B.; Tian, W. Three-dimensional printing biotechnology for the regeneration of the tooth and tooth-supporting tissues. Biotechnol. Bioeng. 2019, 116, 452–468. [Google Scholar] [CrossRef]
- Scotti, C.; Velo, M.; Rizzante, F.; Nascimento, T.; Mondelli, R.; Bombonatti, J. Physical and surface properties of a 3D-printed composite resin for a digital workflow. J. Prosthet. Dent. 2020, 124, 614.e1–614.e5. [Google Scholar] [CrossRef]
- Sa, L.; Kaiwu, L.; Shenggui, C.; Junzhong, Y.; Yongguang, J.; Lin, W.; Li, R. 3D printing dental composite resins with sustaining antibacterial ability. J. Mater. Sci. 2019, 54, 3309–3318. [Google Scholar] [CrossRef]
- Yue, J.; Zhao, P.; Gerasimov, J.; Van de Lagemaat, M.; Grotenhuis, A.; Rustema-Abbing, M.; Ren, Y. 3D-Printable Antimicrobial Composite Resins. Adv. Funct. Mater. 2015, 25, 6756–6767. [Google Scholar] [CrossRef]
- Totu, E.E.; Voicila, E.; Pistritu, V.; Nechifor, G.; Cristache, C.M. Evaluation of Electrical Characteristics for PMMA-TiO2 Nanocomposites Used in Dentistry. Rev. Chim. 2018, 69, 155–159. [Google Scholar] [CrossRef]
- Revilla-León, M.; Meyer, M.; Zandinejad, A.; Özcan, M. Additive manufacturing technologies for processing zirconia in dental applications. Int. J. Comput. Dent. 2020, 23, 27–37. [Google Scholar] [PubMed]
- McCullough, M.; Savage, N. Oral viral infections and the therapeutic use of antiviral agents in dentistry. Aust. Dent. J. 2005, 50, S31–S35. [Google Scholar] [CrossRef]
- Alkattan, R.; Rojo, L.; Deb, S. Antimicrobials in Dentistry. Appl. Sci. 2021, 11, 3279. [Google Scholar] [CrossRef]
- Ferracane, J.; Giannobile, W. Novel Biomaterials and Technologies for the Dental, Oral, and Craniofacial Structures. J. Dent. Res. 2014, 93, 1185–1186. [Google Scholar] [CrossRef] [Green Version]
- Makvandi, P.; Wang, C.; Zare, E.; Borzacchiello, A.; Niu, L.; Tay, F. Metal-Based Nanomaterials in Biomedical Applications: Antimicrobial Activity and Cytotoxicity Aspects. Adv. Funct. Mater. 2020, 30, 1910021. [Google Scholar] [CrossRef]
- Song, W.; Ge, S. Application of antimicrobial nanoparticles in dentistry. Molecules 2019, 24, 1033. [Google Scholar] [CrossRef] [Green Version]
- Mok, Z.H.; Proctor, G.; Thanou, M. Emerging nanomaterials for dental treatments. Emerg. Top. Life Sci. 2020, 4, 613–625. [Google Scholar] [CrossRef]
- Agnihotri, R.; Gaur, S.; Albin, S. Nanometals in Dentistry: Applications and Toxicological Implications—a Systematic Review. Biological Trace Element Research 2020, 197, 70–88. [Google Scholar] [CrossRef]
- Raura, N.; Garg, A.; Arora, A.; Roma, M. Nanoparticle technology and its implications in endodontics: A review. Biomater. Res. 2020, 24, 21. [Google Scholar] [CrossRef]
- Jandt, K.; Watts, D. Nanotechnology in dentistry: Present and future perspectives on dental nanomaterials. Dent. Mater. 2020, 36, 1365–1378. [Google Scholar] [CrossRef] [PubMed]
- Makvandi, P.; Gu, J.T.; Zare, E.N.; Ashtari, B.; Moeini, A.; Tay, F.R.; Niu, L.N. Polymeric and inorganic nanoscopical antimicrobial fillers in dentistry. Acta Biomater. 2020, 101, 69–101. [Google Scholar] [CrossRef] [PubMed]
- Chouirfa, H.; Bouloussa, H.; Migonney, V.; Falentin-Daudré, C. Review of titanium surface modification techniques and coatings for antibacterial applications. Acta Biomater. 2019, 83, 37–54. [Google Scholar] [CrossRef]
- Fernandez, C.; Sokolonski, A.; Fonseca, M.; Stanisic, D.; Araújo, D.; Azevedo, V.; Portela, R.; Tasic, L. Applications of Silver Nanoparticles in Dentistry: Advances and Technological Innovation. Int. J. Mol. Sci. 2021, 22, 2485. [Google Scholar] [CrossRef] [PubMed]
- Salas-Orozco, M.; Niño-Martínez, N.; Martínez-Castañón, G.; Méndez, F.; Jasso, M.; Ruiz, F. Mechanisms of Resistance to Silver Nanoparticles in Endodontic Bacteria: A Literature Review. J. Nanomater. 2019, 2019, 7630316. [Google Scholar] [CrossRef] [Green Version]
- Sivolella, S.; Stellini, E.; Brunello, G.; Gardin, C.; Ferroni, L.; Bressan, E.; Zavan, B. Silver Nanoparticles in Alveolar Bone Surgery Devices. J. Nanomater. 2012, 2012, 15. [Google Scholar] [CrossRef]
- Corrêa, J.; Mori, M.; Sanches, H.; Cruz, A.; Poiate, E.; Poiate, I. Silver Nanoparticles in Dental Biomaterials. Int. J. Biomater. 2015, 2015, 485275–485279. [Google Scholar] [CrossRef] [Green Version]
- Noronha, V.; Paula, A.; Durán, G.; Galembeck, A.; Cogo-Müller, K.; Franz-Montan, M.; Durán, N. Silver nanoparticles in dentistry. Dent. Mater. 2017, 33, 1110–1126. [Google Scholar] [CrossRef]
- Almatroudi, A. Silver nanoparticles: Synthesis, characterisation and biomedical applications. Open Life Sci. 2020, 15, 819–839. [Google Scholar] [CrossRef]
- Yin, I.; Zhang, J.; Zhao, I.; Mei, M.; Li, Q.; Chu, C. The antibacterial mechanism of silver nanoparticles and its application in dentistry. Int. J. Nanomed. 2020, 15, 2555–2562. [Google Scholar] [CrossRef]
- Nuñez-Anita, R.; Acosta-Torres, L.; Vilar-Pineda, J.; Martínez-Espinosa, J.; De la Fuente-Hernández, J.; Castaño, V. Toxicology of antimicrobial nanoparticles for prosthetic devices. Int. J. Nanomed. 2014, 9, 3999–4006. [Google Scholar]
- Talapko, J.; Matijević, T.; Juzbašić, M.; Antolović-Požgain, A.; Škrlec, I. Antibacterial activity of silver and its application in dentistry, cardiology and dermatology. Microorganisms 2020, 8, 1400. [Google Scholar] [CrossRef] [PubMed]
- Niska, K.; Knap, N.; Kędzia, A.; Jaskiewicz, M.; Kamysz, W.; Inkielewicz-Stepniak, I. Capping Agent-Dependent Toxicity and Antimicrobial Activity of Silver Nanoparticles: An In Vitro Study. Concerns about Potential Application in Dental Practice. Int. J. Med. Sci. 2016, 13, 772–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zannella, C.; Shinde, S.; Vitiello, M.; Falanga, A.; Galdiero, E.; Fahmi, A.; Santella, B.; Nucci, L.; Gasparro, R.; Galdiero, M.; et al. Antibacterial Activity of Indolicidin-Coated Silver Nanoparticles in Oral Disease. Appl. Sci. 2020, 10, 1837. [Google Scholar] [CrossRef] [Green Version]
- Prabha, R.; Kandasamy, R.; Sivaraman, U.; Nandkumar, M.; Nair, P. Antibacterial nanosilver coated orthodontic bands with potential implications in dentistry. Indian J. Med. Res. 2016, 144, 580–586. [Google Scholar]
- Halkai, K.; Halkai, R.; Mudda, J.; Shivanna, V.; Rathod, V. Antibiofilm efficacy of biosynthesized silver nanoparticles against endodontic-periodontal pathogens: An in vitro study. J. Conserv. Dent. 2018, 21, 662–666. [Google Scholar] [CrossRef]
- Dos Santos Junior, V.; Targino, A.; Flores, M.; Rodríguez-Díaz, J.; Teixeira, J.; Heimer, M.; de Luna Freire Pessoa, H.; Galembeck, A.; Rosenblatt, A. Antimicrobial activity of silver nanoparticle colloids of different sizes and shapes against Streptococcus mutans. Res. Chem. Intermed. 2017, 43, 5889–5899. [Google Scholar] [CrossRef]
- Espinosa-Cristóbal, L.; Holguín-Meráz, C.; Zaragoza-Contreras, E.; Martínez-Martínez, R.; Donohue-Cornejo, A.; Loyola-Rodríguez, J.P.; Cuevas-González, J.C.; Reyes-López, S. Antimicrobial and Substantivity Properties of Silver Nanoparticles against Oral Microbiomes Clinically Isolated from Young and Young-Adult Patients. J. Nanomater. 2019, 2019, 3205971. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, M.; Rolim, W.; Viana, M.; Souza, T.; Gonçalves, F.; Tanaka, C.; Bueno-Silva, B.; Seabra, A. Biogenic synthesis and antimicrobial activity of silica-coated silver nanoparticles for esthetic dental applications. J. Dent. 2020, 96, 103327. [Google Scholar] [CrossRef]
- Juan Carlos, F.-A.; Rene, G.-C.; Germán, V.-S.; Laura Susana, A.-T. Antimicrobial Poly (methyl methacrylate) with Silver Nanoparticles for Dentistry: A Systematic Review. Appl. Sci. 2020, 10, 4007. [Google Scholar] [CrossRef]
- Shani, S.; Friedman, M.; Steinberg, D. In Vitro Assessment of the Antimicrobial Activity of a Local Sustained Release Device Containing Amine Fluoride for the Treatment of Oral Infectious Diseases. Diagn. Microbiol. Infect. Dis. 1998, 30, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, K.; Niazi, S.; Mylonas, P.; Mannocci, F.; Deb, S. The synthesis of nano silver-graphene oxide system and its efficacy against endodontic biofilms using a novel tooth model. Dent. Mater. 2019, 35, 1614–1629. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.; De Castro, D.; Schiavon, M.; Dos Reis, A. Cytotoxicity and release ions of endodontic sealers incorporated with a silver and vanadium base nanomaterial. Odontology 2020, 108, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Del Pilar Rodriguez-Torres, M.; Díaz-Torres, L.; Millán-Chiu, B.; García-Contreras, R.; Hernández-Padrón, G.; Acosta-Torres, L. Antifungal and Cytotoxic Evaluation of Photochemically Synthesized Heparin-Coated Gold and Silver Nanoparticles. Molecules 2020, 25, 2849. [Google Scholar] [CrossRef]
- Nia, A.; Ataei, M.; Zeighami, H. A comparative study on the antimicrobial activity of irreversible hydrocolloid mixed with silver nanoparticles and chlorhexidine. Dent. Res. J. 2020, 17, 120–125. [Google Scholar]
- de Carvalho Bernardo, W.L.; Boriollo, M.F.G.; Tonon, C.C.; da Silva, J.J.; Cruz, F.M.; Martins, A.L.; Höfling, J.F.; Spolidorio, D.M.P. Antimicrobial effects of silver nanoparticles and extracts of Syzygium cumini flowers and seeds: Periodontal, cariogenic and opportunistic pathogens. Arch. Oral Biol. 2021, 125, 105101. [Google Scholar] [CrossRef]
- Hao, J.; Lang, S.; Mante, F.; Pavelić, K.; Ozer, F. Antimicrobial and mechanical effects of zeolite use in dental materials: A systematic review. Acta Stomatol. Croat. 2021, 55, 76–89. [Google Scholar] [CrossRef]
- Li, W.; Qi, M.; Sun, X.; Chi, M.; Wan, Y.; Zheng, X.; Li, C.; Wang, L.; Dong, B. Novel dental adhesive containing silver exchanged EMT zeolites against cariogenic biofilms to combat dental caries. Microporous Mesoporous Mater. 2020, 299, 110113. [Google Scholar] [CrossRef]
- Bright, K.R.; Sicairos-Ruelas, E.E.; Gundy, P.M.; Gerba, C.P. Assessment of the Antiviral Properties of Zeolites Containing Metal Ions. Food Environ. Virol. 2009, 1, 37. [Google Scholar] [CrossRef]
- Fan, W.; Li, Y.; Sun, Q.; Ma, T.; Fan, B. Calcium-silicate mesoporous nanoparticles loaded with chlorhexidine for both anti- Enterococcus faecalis and mineralization properties. J. Nanobiotechnol. 2016, 14, 72. [Google Scholar] [CrossRef] [Green Version]
- Seneviratne, C.J.; Leung, K.C.-F.; Wong, C.-H.; Lee, S.-F.; Li, X.; Leung, P.C.; Lau, C.; Wat, E.; Jin, L. Nanoparticle-encapsulated chlorhexidine against oral bacterial biofilms. PLoS ONE 2014, 9, e103234. [Google Scholar] [CrossRef] [Green Version]
- Garner, S.; Barbour, M. Nanoparticles for controlled delivery and sustained release of chlorhexidine in the oral environment. Oral Dis. 2015, 21, 641–644. [Google Scholar] [CrossRef] [PubMed]
- Tokajuk, G.; Niemirowicz, K.; Deptuła, P.; Piktel, E.; Cieśluk, M.; Wilczewska, A.; Dąbrowski, J.R.; Bucki, R. Use of magnetic nanoparticles as a drug delivery system to improve chlorhexidine antimicrobial activity. Int. J. Nanomed. 2017, 12, 7833–7846. [Google Scholar] [CrossRef] [PubMed]
- Bapat, R.; Chaubal, T.; Dharmadhikari, S.; Abdulla, A.; Bapat, P.; Alexander, A.; Dubey, S.K.; Kesharwani, P. Recent advances of gold nanoparticles as biomaterial in dentistry. Int. J. Pharm. 2020, 586, 119596. [Google Scholar] [CrossRef] [PubMed]
- Radhi, A.; Mohamad, D.; Rahman, F.S.A.; Abdullah, A.M.; Hasan, H. Mechanism and Factors Influence of Graphene-based Nanomaterials Antimicrobial Activities and Application in Dentistry. J. Mater. Res. Technol. 2021, 11, 1290–1307. [Google Scholar] [CrossRef]
- Konar, M.; Nayak, N.; Priyadarsini, S.; Mishra, M.; Sahoo, H. Antimicrobial activity of nanoparticle-based dental fillers on novel chromogenic bacteria Enterobacter ludwigii. Mater. Res. Express 2019, 6, 85407. [Google Scholar] [CrossRef]
- He, J.; Zhu, X.; Qi, Z.; Wang, C.; Mao, X.; Zhu, C.; He, Z.; Li, M.; Tang, Z. Killing Dental Pathogens Using Antibacterial Graphene Oxide. ACS Appl. Mater. Interfaces 2015, 7, 5605–5611. [Google Scholar] [CrossRef]
- Noori, A.; Kareem, F. The effect of magnesium oxide nanoparticles on the antibacterial and antibiofilm properties of glass-ionomer cement. Heliyon 2019, 5, e02568. [Google Scholar] [CrossRef] [Green Version]
- Nikolova, M.; Chavali, M. Metal oxide nanoparticles as biomedical materials. Biomimetics 2020, 5, 27. [Google Scholar] [CrossRef]
- Makvandi, P.; Jamaledin, R.; Jabbari, M.; Nikfarjam, N.; Borzacchiello, A. Antibacterial quaternary ammonium compounds in dental materials: A systematic review. Dent. Mater. 2018, 34, 851–867. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Hu, Y.; Huang, F.; Xiao, Y. Quaternary ammonium compounds in dental restorative materials. Dent. Mater. J. 2018, 37, 183–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrugia, C.; Camilleri, J. Antimicrobial properties of conventional restorative filling materials and advances in antimicrobial properties of composite resins and glass ionomer cements—A literature review. Dent. Mater. 2014, 31, E89–E99. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.; Wang, S.; Zhou, X.; Wang, H.; Xu, H.; Cheng, L. The use of quaternary ammonium to combat dental caries. Materials 2015, 8, 3532–3549. [Google Scholar] [CrossRef] [PubMed]
- Miglani, S.; Tani-Ishii, N. Biosynthesized selenium nanoparticles: Characterization, antimicrobial, and antibiofilm activity against Enterococcus faecalis. PeerJ 2021, 9, E11653. [Google Scholar] [CrossRef]
- Fernandez-Garcia, E.; Chen, X.; Gutierrez-Gonzalez, C.; Fernandez, A.; Lopez-Esteban, S.; Aparicio, C. Peptide-functionalized zirconia and new zirconia/titanium biocermets for dental applications. J. Dent. 2015, 43, 1162–1174. [Google Scholar] [CrossRef]
- Hafshejani, T.M.; Zamanian, A.; Venugopal, J.R.; Rezvani, Z.; Sefat, F.; Saeb, M.R.; Vahabi, H.; Zarrintaj, P.; Mozafari, M. Antibacterial glass-ionomer cement restorative materials: A critical review on the current status of extended release formulations. J. Control. Release Off. J. Control. Release Soc. 2017, 262, 317–328. [Google Scholar] [CrossRef]
- Dimkov, A.; Nicholson, J.; Gjorgievska, E. On the possibility of incorporating antimicrobial components into glass-ionomer cements. Pril. Makedon. Akad. Nauk. Umetnostite. Oddel. Biološki Med. Nauk. 2009, 30, 219–237. [Google Scholar]
- Michaïlesco, P.; Kouassi, M.; El Briak, H.; Armynot, A.; Boudeville, P. Antimicrobial activity and tightness of a DCPD-CaO-based hydraulic calcium phosphate cement for root canal filling. J. Biomed. Mater. Research. Part B Appl. Biomater. 2005, 74, 760–767. [Google Scholar] [CrossRef]
- Esteban-Tejeda, L.; Smirnov, A.; Prado, C.; Moya, J.S.; Torrecillas, R.; Bartolomé, J.F. Multifunctional ceramic-metal biocomposites with zinc containing antimicrobial glass coatings. Ceram. Int. 2016, 42, 7023–7029. [Google Scholar] [CrossRef]
- Gbureck, U.; Barralet, J.; Hofmann, M.; Thulĺ, R. Nanocrystalline Tetracalcium Phosphate Cement. J. Dent. Res. 2004, 83, 425–428. [Google Scholar] [CrossRef]
- Cicciu, M.; Fiorillo, L.; Cervino, G. Chitosan Use in Dentistry: A Systematic Review of Recent Clinical Studies. Mar. Drugs 2019, 17, 417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, J.; Bordini, E.; Ferreira, J.; Mei, L.; Dubey, N.; Fenno, J.; Piva, E.; Lund, R.G.; Schwendeman, A.; Bottino, M. Injectable MMP-Responsive Nanotube-Modified Gelatin Hydrogel for Dental Infection Ablation. ACS Appl. Mater. Interfaces 2020, 12, 16006–16017. [Google Scholar] [CrossRef]
- Pakzad, Y.; Ganji, F. Thermosensitive hydrogel for periodontal application: In vitro drug release, antibacterial activity and toxicity evaluation. J. Biomater. Appl. 2016, 30, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Cosgun, A.; Bolgul, B.; Duran, N. In vitro investigation of antimicrobial effects, nanohardness, and cytotoxicity of different glass ionomer restorative materials in dentistry. Niger. J. Clin. Pract. 2019, 22, 422–431. [Google Scholar] [PubMed]
- Sun, R.W.; Chen, R.; Chung, N.P.; Ho, C.M.; Lin, C.L.; Che, C.M. Silver nanoparticles fabricated in Hepes buffer exhibit cytoprotective activities toward HIV-1 infected cells. Chem. Commun. 2005, 40, 5059–5061. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Sun, R.W.-Y.; Chen, R.; Hui, C.-K.; Ho, C.-M.; Luk, J.M.; Lau, G.K.; Che, C.-M. Silver nanoparticles inhibit hepatitis B virus replication. Antivir. Ther. 2008, 13, 253–262. [Google Scholar] [CrossRef]
- Chen, N.; Zheng, Y.; Yin, J.; Li, X.; Zheng, C. Inhibitory effects of silver nanoparticles against adenovirus type 3 in vitro. J. Virol. Methods 2013, 193, 470–477. [Google Scholar] [CrossRef]
- Xiang, D.X.; Chen, Q.; Pang, L.; Zheng, C.L. Inhibitory effects of silver nanoparticles on H1N1 influenza A virus in vitro. J. Virol. Methods 2011, 178, 137–142. [Google Scholar] [CrossRef]
- Jeremiah, S.S.; Miyakawa, K.; Morita, T.; Yamaoka, Y.; Ryo, A. Potent antiviral effect of silver nanoparticles on SARS-CoV-2. Biochem. Biophys. Res. Commun. 2020, 533, 195–200. [Google Scholar] [CrossRef]
- Warnes, S.L.; Keevil, C.W. Inactivation of norovirus on dry copper alloy surfaces. PLoS ONE 2013, 8, e75017. [Google Scholar] [CrossRef] [Green Version]
- Atukorallaya, D.; Ratnayake, R. Oral Mucosa, Saliva, and COVID-19 Infection in Oral Health Care. Front. Med. 2021, 8, 656926. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ren, B.; Peng, X.; Hu, T.; Li, J.; Gong, T.; Tang, B.; Xu, X.; Zhou, X. Saliva is a non-negligible factor in the spread of COVID-19. Mol. Oral Microbiol. 2020, 35, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Bhumireddy, J.; Mallineni, S.; Nuvvula, S. Challenges and possible solutions in dental practice during and post COVID-19. Environ. Sci. Pollut. Res. Int. 2020, 28, 1275–1277. [Google Scholar] [CrossRef] [PubMed]
- Checchi, V.; Bellini, P.; Bencivenni, D.; Consolo, U. COVID-19 Dentistry-Related Aspects: A Literature Overview. Int. Dent. J. 2021, 71, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Shamsoddin, E.; DeTora, L.; Tovani-Palone, M.; Bierer, B. Dental Care in Times of the COVID-19 Pandemic: A Review. Med. Sci. 2021, 9, 13. [Google Scholar] [CrossRef]
- Amante, L.; Afonso, J.; Skrupskelyte, G. Dentistry and the COVID-19 Outbreak. Int. Dent. J. 2021, 71, 358–368. [Google Scholar] [CrossRef]
- Barabari, P.; Moharamzadeh, K. Novel coronavirus (COVID-19) and dentistry–A comprehensive review of literature. Dent. J. 2020, 8, 53. [Google Scholar] [CrossRef]
- Bordea, I.R.; Xhajanka, E.; Candrea, S.; Bran, S.; Onișor, F.; Inchingolo, A.D.; Malcangi, G.; Pham, V.H.; Inchingolo, A.M.; Scarano, A.; et al. Coronavirus (SARS-CoV-2) Pandemic: Future Challenges for Dental Practitioners. Microorganisms 2020, 8, 1704. [Google Scholar] [CrossRef]
- Ashtiani, R.; Tehrani, S.; Revilla-León, M.; Zandinejad, A. Reducing the Risk of COVID-19 Transmission in Dental Offices: A Review. J. Prosthodont. 2020, 29, 739–745. [Google Scholar] [CrossRef]
- Suprono, M.S.; Won, J.; Savignano, R.; Zhong, Z.; Ahmed, A.; Roque-Torres, G.; Zhang, W.; Oyoyo, U.; Richardson, P.; Caruso, J.; et al. A clinical investigation of dental evacuation systems in reducing aerosols. J. Am. Dent. Assoc. 2021, 152, 455–462. [Google Scholar] [CrossRef]
- Botros, N.; Iyer, P.; Ojcius, D. Is there an association between oral health and severity of COVID-19 complications? Biomed. J. 2020, 43, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Chavis, S.; Hines, S.; Dyalram, D.; Wilken, N.; Dalby, R. Can extraoral suction units minimize droplet spatter during a simulated dental procedure? J. Am. Dent. Assoc. 2021, 152, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Maiorani, C.; Natoli, V.; Bruni, A.; Coscione, C.; Magliano, G.; Giacobbo, G.; Morelli, A.; Moressa, S.; Scribante, A. Bio-Inspired Systems in Nonsurgical Periodontal Therapy to Reduce Contaminated Aerosol during COVID-19: A Comprehensive and Bibliometric Review. J. Clin. Med. 2020, 9, 3914. [Google Scholar] [CrossRef] [PubMed]
- Eden, E.; Frencken, J.; Gao, S.; Horst, J.; Innes, N. Managing dental caries against the backdrop of COVID-19: Approaches to reduce aerosol generation. Br. Dent. J. 2020, 229, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S.; Geisinger, M.L.; Avila-Ortiz, G. Methods to mitigate infection spread from aerosol-generating dental procedures. J. Periodontol. 2021, 92, 784–792. [Google Scholar] [CrossRef]
- Ge, Z.; Yang, L.; Xia, J.; Fu, X.; Zhang, Y. Possible aerosol transmission of COVID-19 and special precautions in dentistry. J. Zhejiang Univ. B Sci. 2020, 21, 361–368. [Google Scholar] [CrossRef] [Green Version]
- Chowdhry, A.; Kapoor, P.; Kharbanda, O.; Popli, D. Saliva and COVID 19: Current dental perspective. J. Oral Maxillofac. Pathol. JOMFP 2021, 25, 18–21. [Google Scholar] [CrossRef]
- Comisi, J.; Ravenel, T.; Kelly, A.; Teich, S.; Renne, W. Aerosol and spatter mitigation in dentistry: Analysis of the effectiveness of 13 setups. J. Esthet. Restor. Dent. 2021, 33, 466–479. [Google Scholar] [CrossRef]
- Ahmed, M.; Jouhar, R. Dissemination of aerosol and splatter in clinical environment during cavity preparation: An in vitro study. Int. J. Environ. Res. Public Health 2021, 18, 3773. [Google Scholar] [CrossRef]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Chan, J.F.; Kok, K.H.; Zhu, Z.; Chu, H.; To, K.K.; Yuan, S.; Yuen, K.Y. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg. Microbes Infect. 2020, 9, 221–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barré-Sinoussi, F.; Chermann, J.C.; Rey, F.; Nugeyre, M.T.; Chamaret, S.; Gruest, J.; Dauguet, C.; Axler-Blin, C.; Vézinet-Brun, F.; Rouzioux, C.; et al. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). Science 1983, 220, 868–871. [Google Scholar] [CrossRef] [PubMed]
- Popovic, M.; Sarngadharan, M.G.; Read, E.; Gallo, R.C. Detection, isolation, and continuous production of cytopathic retroviruses (HTLV-III) from patients with AIDS and pre-AIDS. Science 1984, 224, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Harcourt, J.; Tamin, A.; Lu, X.; Kamili, S.; Sakthivel, S.K.; Murray, J.; Queen, K.; Tao, Y.; Paden, C.R.; Zhang, J.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with 2019 Novel Coronavirus Disease, United States. Emerg. Infect. Dis. J. 2020, 26, 1266–1273. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, E.J.; Manguiat, K.; Wood, H.; Drebot, M. Two Detailed Plaque Assay Protocols for the Quantification of Infectious SARS-CoV-2. Curr. Protoc. Microbiol. 2020, 57, ecpmc105. [Google Scholar] [CrossRef] [PubMed]
- Brown, H.E.; Chen, H.; Engelman, A. Structure-based mutagenesis of the human immunodeficiency virus type 1 DNA attachment site: Effects on integration and cDNA synthesis. J. Virol. 1999, 73, 9011–9020. [Google Scholar] [CrossRef] [Green Version]
- Schweitzer, C.J.; Jagadish, T.; Haverland, N.; Ciborowski, P.; Belshan, M. Proteomic analysis of early HIV-1 nucleoprotein complexes. J. Proteome Res. 2013, 12, 559–572. [Google Scholar] [CrossRef] [Green Version]
- Sanford, B.; Li, Y.; Maly, C.J.; Madson, C.J.; Chen, H.; Zhou, Y.; Belshan, M. Deletions in the fifth alpha helix of HIV-1 matrix block virus release. Virology 2014, 468–470, 293–302. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Jambou, C.; Sun, K.; Lalevée, J.; Simon-Masseron, A.; Xiao, P. Effect of Zeolite Fillers on the Photopolymerization Kinetics for Photocomposites and Lithography. ACS Appl. Polym. Mater. 2019, 1, 2854–2861. [Google Scholar] [CrossRef]
- Rakowska, P.D.; Tiddia, M.; Faruqui, N.; Bankier, C.; Pei, Y.; Pollard, A.J.; Zhang, J.; Gilmore, I.S. Antiviral surfaces and coatings and their mechanisms of action. Commun. Mater. 2021, 2, 53. [Google Scholar] [CrossRef]
- Thurman, R.B.; Gerba, C.P.; Bitton, G. The molecular mechanisms of copper and silver ion disinfection of bacteria and viruses. Crit. Rev. Environ. Control. 1989, 18, 295–315. [Google Scholar] [CrossRef]
- Soliman, M.Y.M.; Medema, G.; Bonilla, B.E.; Brouns, S.J.J.; van Halem, D. Inactivation of RNA and DNA viruses in water by copper and silver ions and their synergistic effect. Water Res. X 2020, 9, 100077. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Chen, L.; Duan, S.M.; Yang, Q.X.; Yang, M.; Gao, C.; Zhang, B.Y.; He, H.; Dong, X.P. Efficient and quick inactivation of SARS coronavirus and other microbes exposed to the surfaces of some metal catalysts. Biomed. Environ. Sci. 2005, 18, 176–180. [Google Scholar]
- Lara, H.H.; Ayala-Nunez, N.V.; Ixtepan-Turrent, L.; Rodriguez-Padilla, C. Mode of antiviral action of silver nanoparticles against HIV-1. J. Nanobiotechnol. 2010, 8, 1. [Google Scholar] [CrossRef]
- Elechiguerra, J.L.; Burt, J.L.; Morones, J.R.; Camacho-Bragado, A.; Gao, X.; Lara, H.H.; Yacaman, M.J. Interaction of silver nanoparticles with HIV-1. J. Nanobiotechnol. 2005, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- Fogari, R.; Zoppi, A. A drug safety evaluation of valsartan. Expert Opin. Drug Saf. 2011, 10, 295–303. [Google Scholar] [CrossRef]
- Pan, X.; Zhang, Y.; Zhao, Y.; Yao, S.; Guan, C.; Wang, L.; Chen, L. Inhibitory activity and mechanism of silver nanoparticles against herpes simplex virus type 1. Arch. Virol. 2022, 167, 1619–1636. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Flexural Strength (MPa) |
|---|---|
| Neat Resin | 102.42 ± 13.67 |
| 10 w/w% Ag Only/0 w/w% FS | 130.83 ± 9.55 |
| 10 w/w% Ag Only/3 w/w% FS | 137.28 ± 8.67 |
| 10 w/w% Ag Only/6.5 w/w% FS | 143.33 ± 5.36 |
| 10 w/w% Ag Only/10 w/w% FS | 146.25 ± 9.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pacho, M.O.; Deeney, D.; Johnson, E.A.; Bravo, B.N.; Patel, K.; Latta, M.A.; Belshan, M.A.; Gross, S.M. Characterization of Ag-Ion Releasing Zeolite Filled 3D Printed Resins. J. Funct. Biomater. 2023, 14, 7. https://doi.org/10.3390/jfb14010007
Pacho MO, Deeney D, Johnson EA, Bravo BN, Patel K, Latta MA, Belshan MA, Gross SM. Characterization of Ag-Ion Releasing Zeolite Filled 3D Printed Resins. Journal of Functional Biomaterials. 2023; 14(1):7. https://doi.org/10.3390/jfb14010007
Chicago/Turabian StylePacho, Marian O., Dylan Deeney, Emily A. Johnson, Bryanna N. Bravo, Kishen Patel, Mark A. Latta, Michael A. Belshan, and Stephen M. Gross. 2023. "Characterization of Ag-Ion Releasing Zeolite Filled 3D Printed Resins" Journal of Functional Biomaterials 14, no. 1: 7. https://doi.org/10.3390/jfb14010007