Early Evaluation of Patients on Axial Flow Pump Support for Refractory Cardiogenic Shock Is Associated with Left Ventricular Recovery

 , , ,
, , ,
Abstract
:1. Introduction
2. Experimental Section
3. Results
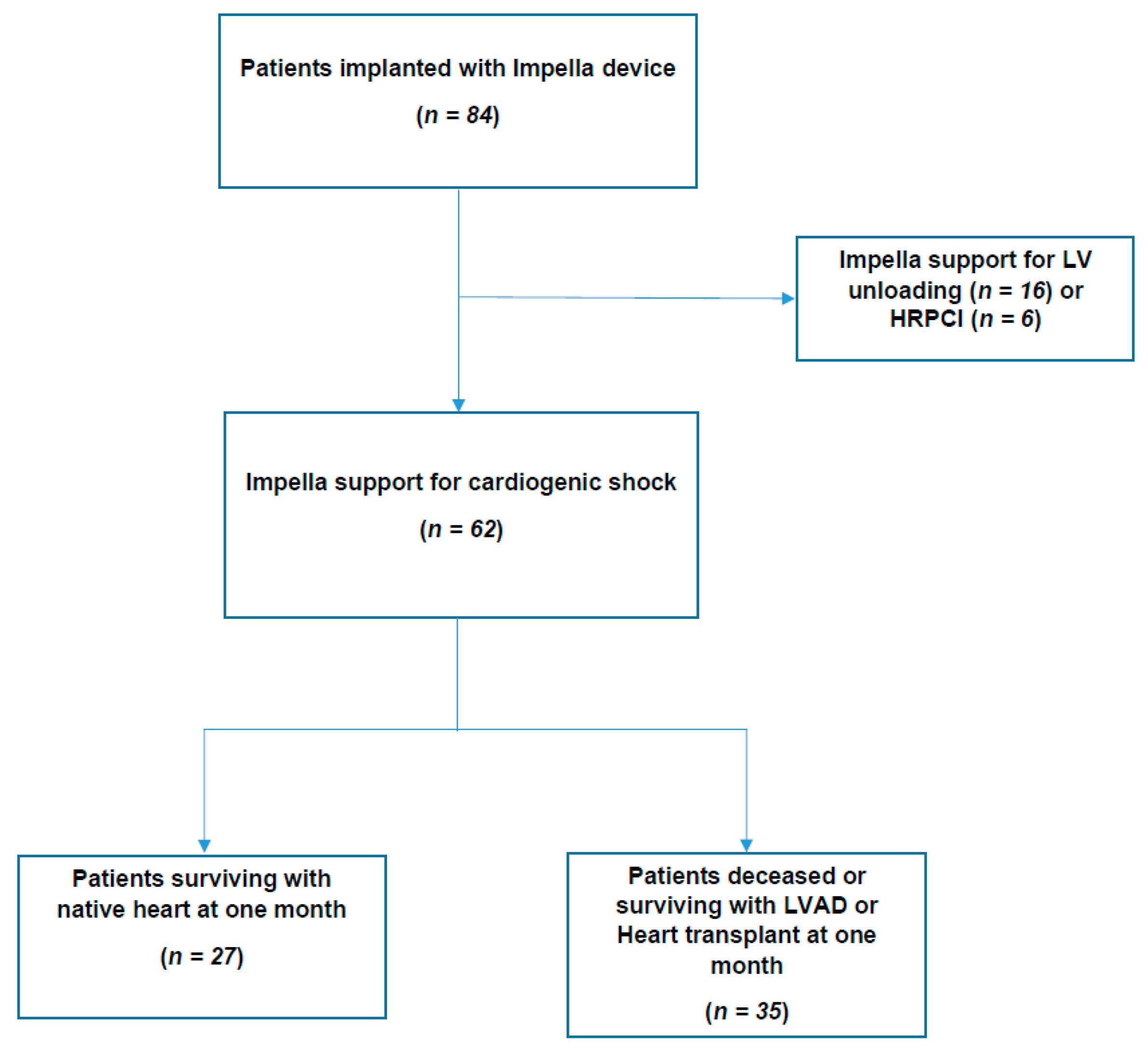
3.1. Population Characteristics
3.2. 30 Day Outcome
3.3. Comparative Analysis between Recovery and Non-Recovery Groups at 30 Days
3.4. Factors Associated with 30 Day Outcomes
3.5. Factors Associated with 30 Day Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hochman, J.S.; Buller, C.E.; Sleeper, L.A.; Boland, J.; Dzavik, V.; Sanborn, T.A.; Godfrey, E.; White, H.D.; Lim, J.; LeJemtel, T. Cardiogenic shock complicating acute myocardial infarction—Etiologies, management and outcome: A report from the SHOCK Trial Registry. J. Am. Coll. Cardiol. 2000, 36, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- Harjola, V.-P.; Lassus, J.; Sionis, A.; Køber, L.; Tarvasmäki, T.; Spinar, J.; Parissis, J.; Banaszewski, M.; Cardoso, J.S.; Carubelli, V.; et al. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur. J. Heart Fail. 2015, 17, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Delmas, C.; Puymirat, E.; Leurent, G.; Elbaz, M.; Manzo-Silberman, S.; Bonello, L.; Gerbaud, E.; Bataille, V.; Levy, B.; Lamblin, N.; et al. Design and preliminary results of FRENSHOCK 2016: A prospective nationwide multicentre registry on cardiogenic shock. Arch. Cardiovasc. Dis. 2019, 112, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Jeger, R.V.; Radovanovic, D.; Hunziker, P.R.; Pfisterer, M.E.; Stauffer, J.C.; Erne, P.; Urban, P. AMIS Plus Registry Investigators. Ten-year trends in the incidence and treatment of cardiogenic shock. Ann. Intern. Med. 2008, 149, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Aissaoui, N.; Puymirat, E.; Delmas, C.; Ortuno, S.; Durand, E.; Bataille, V.; Drouet, E.; Bonello, L.; Bonnefoy-Cudraz, E.; Lesmeles, G.; et al. Trends in cardiogenic shock complicating acute myocardial infarction. Eur. J. Heart Fail. 2020, 22, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Sanborn, T.A.; White, H.D.; Talley, J.D.; Buller, C.E.; Jacobs, A.K.; Slater, J.N.; Col, J.; et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N. Engl. J. Med. 1999, 341, 625–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, R.J.; Spencer, F.A.; Gore, J.M.; Lessard, D.; Yarzebski, J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: A population-based perspective. Circulation 2009, 119, 1211–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolte, D.; Khera, S.; Aronow, W.S.; Mujib, M.; Palaniswamy, C.; Sule, S.; Jain, D.; Gotsis, W.; Ahmed, A.; Frishman, H.W.; et al. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States. J. Am. Heart Assoc. 2014, 3, e000590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. American Heart Association Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; and Mission: Lifeline. Contemporary Management of Cardiogenic Shock: A Scientific Statement from the American Heart Association. Circulation 2017, 136, e232–e268. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Ohman, E.M.; Desch, S.; Eitel, I.; de Waha, S. Management of cardiogenic shock. Eur. Heart J. 2015, 36, 1223–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhruva, S.S.; Ross, J.S.; Mortazavi, B.J.; Hurley, N.C.; Krumholz, H.M.; Curtis, J.P.; Berkowitz, A.; Masoudi, F.A.; Messenger, J.C.; Parzynski, C.S.; et al. Association of Use of an Intravascular Microaxial Left Ventricular Assist Device vs Intra-aortic Balloon Pump with In-Hospital Mortality and Major Bleeding Among Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock. JAMA 2020, 323, 734–745. [Google Scholar] [PubMed]
- Amin, A.P.; Spertus, J.A.; Curtis, J.P.; Desai, N.; Masoudi, F.A.; Bach, R.G.; McNeely, C.; Badarin, F.; House, J.A.; Kulkaeni, H.; et al. The Evolving Landscape of Impella Use in the United States Among Patients Undergoing Percutaneous Coronary Intervention with Mechanical Circulatory Support. Circulation 2020, 141, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chieffo, A.; Ancona, M.B.; Burzotta, F.; Pazzanese, V.; Briguori, C.; Trani, C.; Piva, T.; De Marco, F.; Di Biasi, M.; Pagnotta, P.; et al. Observational multicentre registry of patients treated with IMPella mechanical circulatory support device in ITaly: The IMP-IT registry. EuroIntervention 2020, 15, e1343–e1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neill, W.W.; Grines, C.; Schreiber, T.; Moses, J.F.; Maini, B.S.; Dixon, S.R.; Ohman, E.M. Analysis of outcomes for 15,259 US patients with acute myocardial infarction cardiogenic shock (AMICS) supported with the Impella device. Am. Heart J. 2018, 202, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Baran, D.A.; Grines, C.L.; Bailey, S.; Burkhoff, D.; Hall, S.A.; Henry, T.D.; Hollenberg, S.M.; Kapur, N.K.; O’Neill, W.; Ornato, J.P.; et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock: This document was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society of Critical Care Medicine (SCCM), and the Society of ThoracicSurgeons (STS) in April 2019. Catheter Cardiovasc. Interv. 2019, 94, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basir, M.B.; Schreiber, T.L.; Grines, C.L.; Dixon, S.R.; Moses, J.F.; Maini, B.S.; Khandelwal, A.K.; Ohman, E.M.; O’Neill, W.W. Effect of Early Initiation of Mechanical Circulatory Support on Survival in Cardiogenic Shock. Am. J. Cardiol. 2017, 119, 845–851. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, W.W.; Schreiber, T.; Wohns, D.H.; Rihal, C.; Naidu, S.S.; Civitello, A.B.; Dixon, S.R.; Massaro, J.M.; Maini, B.; Ohman, E.M. The current use of Impella 2.5 in acute myocardial infarction complicated by cardiogenic shock: Results from the USpella Registry. J. Interv. Cardiol. 2014, 27, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, A.; Werner, N.; Burkhoff, D.; Sieweke, J.-T.; Zietzer, A.; Masyuk, M.; Udesen, N.L.J.; Westenfeld, R.; Møller, J.E. Influence of Timing and Predicted Risk on Mortality in Impella-Treated Infarct-Related Cardiogenic Shock Patients. Front. Cardiovasc. Med. 2020, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Bellumkonda, L.; Gul, B.; Masri, S.C. Evolving Concepts in Diagnosis and Management of Cardiogenic Shock. Am. J. Cardiol. 2018, 122, 1104–1110. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cardiogenic Shock (n = 62) | Recovery (n = 27, 44%) | Non-Recovery (n = 35, 56%) | p-Value | |
|---|---|---|---|---|
| Baseline Characteristics | ||||
| Age-yrs. | 58 ± 11 | 58 ± 12 | 59 ± 10 | 0.80 |
| Male Gender-no. (%) | 55 (88) | 24 (89) | 31 (89) | 0.96 |
| Body Mass Index-kg/m2 | 25.9 ± 4.0 | 27.1 ± 4.6 | 25.0 ± 3.3 | 0.03 |
| Current smoker-no. (%) | 36 (59) | 14 (52) | 22 (65) | 0.31 |
| Hypertension-no. (%) | 22 (36) | 10 (37) | 12 (35) | 0.88 |
| Diabetes mellitus-no. (%) | 15 (24) | 6 (22) | 9 (26) | 0.75 |
| Dyslipidemia-no. (%) | 17 (27) | 8 (30) | 9 (26) | 0.73 |
| History of heart failure-no. (%) | 4 (7) | 1 (4) | 3 (9) | 0.44 |
| History of coronary artery disease-no. (%) | 11 (18) | 4 (15) | 7 (21) | 0.56 |
| Peripheral vascular disease-no. (%) | 8 (13) | 3 (11) | 5 (15) | 0.71 |
| No history of cardiopathy-no. (%) | 42 (70) | 20 (77) | 22 (65) | 0.31 |
| SAPS2 | 40 ± 19 | 37 ± 18 | 43 ± 20 | 0.23 |
| Cardiac arrest prior to Impella® placement-no. (%) | 6 (10) | 3 (11) | 3 (9) | 0.73 |
| Cardiogenic shock etiology | ||||
| Acute coronary syndrome-no. (%) | 57 (91) | 26 (96) | 31 (88) | 0.27 |
| Acute decompensated heart failure-no. (%) | 3 (5) | 0 (0) | 3 (9) | 0.12 |
| Acute Myocarditis-no. (%) | 1 (2) | 1 (4) | 0 (0) | 0.25 |
| Post-cardiotomy cardiogenic shock-no. (%) | 1 (2) | 0 (0) | 1 (3) | 0.38 |
| Clinical features | ||||
| SBP, mmHg | 101 ± 21 | 108 ± 20 | 97 ± 21 | 0.04 |
| DBP, mmHg | 67 ± 13 | 70 ± 12 | 64 ± 13 | 0.03 |
| MBP, mmHg | 78 ± 15 | 83 ± 14 | 75 ± 15 | 0.04 |
| Heart rate, bpm | 107 ± 20 | 104 ± 16 | 109 ± 22 | 0.26 |
| Invasive mechanical ventilation-no. (%) | 18 (30) | 8 (31) | 10 (29) | 0.85 |
| Diuresis per hour, liters | 0.091 [0.057–0.171] | 0.161 [0.078–0.217] | 0.079 [0.055–0.107] | 0.01 |
| Biology | ||||
| pH | 7.37 ± 0.14 | 7.35 ± 0.14 | 7.39 ± 0.14 | 0.36 |
| Lactic acid-mmol/L | 3.1 ± 2.1 | 3.2 ± 2.4 | 3.0 ± 1.9 | 0.68 |
| Troponin-ng/L | 5030 [471–10776] | 6018 [1461–12126] | 2547 [269–8671] | 0.73 |
| Sodium-mmol/L | 136 ± 5 | 138 ± 3 | 134 ± 5 | 0.004 |
| Serum creatinine-µmol/L | 117 ± 53 | 107 ± 38 | 125 ± 61 | 0.16 |
| GFR-mL/min | 68 ± 26 | 72 ± 26 | 65 ± 26 | 0.31 |
| Glycemia-mmol/L | 11.8 ± 5.6 | 11.5 ± 5.6 | 12.1 ± 5.5 | 0.66 |
| Total bilirubin-µmol/L | 11.2 [7.2–17.7] | 12.9 [5.9–15.4] | 16.0 [8.0–22.0] | 0.31 |
| ASAT-IU/L | 180 [72–764] | 507 [147–854] | 378 [49–662] | 0.19 |
| ALAT-IU/L | 94 [49–158] | 113 [56–160] | 121 [46–151] | 0.76 |
| GammaGT-IU/L | 53 [36–103] | 66 [34–84] | 85 [40–113] | 0.21 |
| Alkaline phosphatase-IU/L | 85 [62–103] | 90 [59–94] | 126 [68–117] | 0.15 |
| Hemoglobin-g/dL | 13.9 ± 2.3 | 14.5 ± 2.1 | 13.4 ± 2.4 | 0.07 |
| Leukocytes-g/L | 17.8 ± 7.1 | 17.8 ± 7.6 | 18.0 ± 6.8 | 0.92 |
| C-reactive proteing/L | 67 ± 100 | 53 ± 96 | 78 ± 102 | 0.34 |
| Echocardiography | ||||
| LVEF-% | 22 ± 9 | 24 ± 10 | 21 ± 9 | 0.20 |
| Aortic velocity–time integral-cm | 10 ± 4 | 10 ± 4 | 9 ± 4 | 0.43 |
| Cardiac Index-L/min/m2 | 1.93 ± 0.55 | 1.98 ± 0.61 | 1.87 ± 0.49 | 0.69 |
| Elevated LVEDP-no. (%) | 16 (42) | 3 (18) | 13 (57) | 0.01 |
| Moderate to Severe MR-no. (%) | 17 (27) | 4 (15) | 13 (38) | 0.04 |
| TAPSE-mm | 18 ± 4 | 19 ± 3 | 17 ± 5 | 0.08 |
| Management | ||||
| Dobutamine-no. (%) | 37 (60) | 12 (44) | 25 (71) | 0.03 |
| Dobutamine-µg/kg/min | 7.61 ± 4.22 | 5.63 ± 3.05 | 8.20 ± 4.67 | 0.06 |
| NAD-no. (%) | 41 (66) | 15 (56) | 26 (74) | 0.12 |
| NAD dose-µg/kg/min | 0.406 ± 0.479 | 0.227 ± 0.186 | 0.527 ± 0.572 | 0.03 |
| Adrenalin-no. (%) | 7 (11) | 3 (11) | 4 (11) | 0.97 |
| Adrenalin dose-µg/kg/min | 0.423 ± 0.481 | 0.348 ± 0.501 | 0.638 ± 0.524 | 0.53 |
| Cardiogenic Shock (n = 62) | Recovery (n = 27,44%) | Non-Recovery (n = 35, 56%) | p-Value | |
|---|---|---|---|---|
| Clinical features | ||||
| SBP, mmHg | 99 ± 14 | 103 ± 14 | 96 ± 14 | 0.07 |
| DBP, mmHg | 68 ± 9 | 68 ± 9 | 67 ± 10 | 0.54 |
| MBP, mmHg | 78 ± 9 | 80 ± 8 | 77 ± 9 | 0.38 |
| Heart rate, bpm | 97 ± 18 | 94 ± 16 | 100 ± 19 | 0.26 |
| Invasive mechanical ventilation-no. (%) | 35 (58) | 13 (50) | 22 (65) | 0.25 |
| Diuresis per hour, liters | 0.073 [0.046–0.102] | 0.062 [0.041–0.099] | 0.081 [0.065–0.102] | 0.24 |
| Biology | ||||
| pH | 7.42 ± 0.08 | 7.42 ± 0.07 | 7.42 ± 0.09 | 0.85 |
| Lactic acid-mmol/L | 1.8 [1.2–2.1] | 1.6 [1.2–1.8] | 2.0 [1.2–2.2] | 0.09 |
| Troponin peak-ng/L | 20789 [5016–28059] | 18444 [5917–24013] | 22731 [5016–36142] | 0.40 |
| Na-mmol/L | 138.3 [135.0–142.0] | 139.4 [137.0–142.0] | 137.4 [132.0–142.8] | 0.13 |
| Creatinine-µmol/L | 147 [83–171] | 138 [77–142] | 153 [89–182] | 0.53 |
| GFR-mL/min | 62 [35–91] | 68 [44–99] | 58 [30–82] | 0.21 |
| Glycemia-mmol/L | 8.7 ± 3.0 | 8.0 ± 2.1 | 9.1 ± 3.5 | 0.14 |
| Total bilirubin-µmol/L | 24.9 [14.2–29.0] | 19.8 [11.3–25.5] | 28.9 [14.9–33.0] | 0.01 |
| ASAT-IU/L | 722 [137–651] | 491 [162–590] | 910 [112–767] | 0.18 |
| ALAT-IU/L | 385 [62–176] | 185 [57–121] | 545 [71–215] | 0.13 |
| GammaGT-IU/L | 63 [28–80] | 44 [24–55] | 77 [36–93] | 0.005 |
| Alkaline phosphatase-IU/L | 89 [57–87] | 66 [49–73] | 109 [62–96] | 0.03 |
| Hemoglobin-g/dL | 11.4 ± 1.8 | 11.7 ± 1.9 | 11.1 ± 1.7 | 0.16 |
| Leukocytes-g/L | 16.1 ± 5.8 | 14.2 ± 5.1 | 17.5 ± 5.9 | 0.02 |
| C-reactive protein-g/L | 141 ± 85 | 121 ± 94 | 154 ± 88 | 0.28 |
| Echocardiography | ||||
| LVEF-% | 22 ± 10.9 | 27 ± 11.7 | 18 ± 8.2 | 0.001 |
| Aortic velocity-time integral-cm | 10,2 ± 3.7 | 11.9 ± 3.4 | 8.9 ± 3.4 | 0.004 |
| TAPSE-mm | 18 ± 5.2 | 19.6 ± 4.8 | 16.0 ± 5.0 | 0.01 |
| LVEF change * | −0.1 ± 12.2 | 3.2 ± 14.4 | −3.1 ± 9.1 | 0.03 |
| Aortic TVI change * | 0.4 ± 4.0 | 1.4 ± 4.4 | −0.9 ± 5.5 | 0.04 |
| TAPSE change * | 0.4 ± 5.3 | 2.1 ± 4.0 | −1.2 ± 6.0 | 0.06 |
| Management | ||||
| Dobutamine-no. (%) | 17 (28) | 2 (7) | 15 (44) | 0.001 |
| Dobutamine dose-µg/kg/min | 7.38 ± 4.11 | 10.00 ± 5.00 | 7.35 ± 3.54 | 0.29 |
| NAD-no. (%) | 38 (62) | 13 (48) | 25 (74) | 0.04 |
| NAD dose-µg/kg/min | 0.44 ± 0.46 | 0.26 ± 0.25 | 0.52 ± 0.52 | 0.04 |
| Adrenalin-no. (%) | 4 (7) | 0 (0) | 4 (11) | 0.07 |
| Adrenalin dose-µg/kg/min | 1.099 ± 0.864 | - | 1.099 ± 0.864 | - |
| Cardiogenic Shock (n = 62) | Recovery (n = 27, 44%) | Non-Recovery (n = 35, 56%) | p-Value | |
|---|---|---|---|---|
| Impella® < 24 h after admission- no. (%) | 50 (81) | 25 (93) | 25 (71) | 0.036 |
| 3.5-no. (%) | 49 (79) | 23 (85) | 26 (74) | 0.30 |
| 5.0-no. (%) | 13 (21) | 4 (15) | 9 (26) | 0.30 |
| Femoral access-no. (%) | 48 (77) | 23 (85) | 25 (71) | 0.20 |
| Subclavian access-no. (%) | 7 (11) | 1 (4) | 6 (17) | 0.10 |
| Axillar access-no. (%) | 7 (11) | 3 (11) | 4 (11) | 0.97 |
| Impella® maximal output-L/min | 3.2 ± 0.7 | 2.9 ± 0.6 | 3.3 ± 0.8 | 0.02 |
| Impella® duration-days | 6.8 [3.0–8.8] | 5.5 [2.0–6.0] | 7.9 [4.0–9.5] | 0.19 |
| VA-ECMO-no. (%) | 16 (26) | 5 (19) | 11 (31) | 0.25 |
| IABP-no. (%) | 9 (15) | 3 (11) | 6 (17) | 0.50 |
| Renal replacement therapy-no. (%) | 15 (24) | 3 (11) | 12 (34) | 0.03 |
| Invasive ventilation-no. (%) | 43 (69) | 15 (56) | 28 (80) | 0.04 |
| Invasive ventilation median duration-days | 8.0 [4.0–11.5] | 6.0 [3.0–11.0] | 9.0 [4.8–11.3] | 0.89 |
| Non-invasive ventilation | 24 (39) | 9 (33) | 15 (43) | 0.11 |
| Electric shock-no. (%) | 18 (29) | 7 (26) | 11 (31) | 0.64 |
| Dobutamine-no. (%) | 49 (79) | 20 (74) | 29 (83) | 0.40 |
| Mean dobutamine support duration-days | 3.9 [0.6–4.0] | 2.2 [0.1–2] | 5.2 [1.0–6.5] | 0.02 |
| NAD-no. (%) | 53 (86) | 21 (78) | 32 (91) | 0.13 |
| Mean NAD support duration-days | 5.4 [1.6–7.8] | 3.7 [0.75–3.5] | 6.6 [2.8–10.5] | 0.08 |
| Adrenalin-no. (%) | 16 (26) | 6 (22) | 10 (29) | 0.57 |
| Mean adrenalin support duration-days | 0.6 ± 2.0 | 0.2 ± 0.46 | 0.9 ± 2.7 | 0.12 |
| 2 or more amines at day one-no. (%) | 16 (26) | 0 (0) | 16 (46) | <0.001 |
| Furosemide-no. (%) | 56 (90) | 24 (89) | 32 (91) | 0.35 |
| Maximal furosemide dose while on Impella® support-mg per day | 273 [0–500] | 214 [0–250] | 318 [0–500] | 0.29 |
| Furosemide duration on Impella® support-days | 2.6 [0.0–4.0] | 2.1 [0.0–2.5] | 2.9 [0.0–4.5] | 0.32 |
| Fluid challenge while on Impella® support-Liters | 4.9 [2.1–6.4] | 4.8 [2.2–5.4] | 4.89 [2.1–7.6] | 0.94 |
| Levosimendan-no. (%) | 10 (16) | 3 (11) | 7 (20) | 0.35 |
| Amiodarone-no. (%) | 38 (61) | 14 (52) | 24 (69) | 0.73 |
| Primary percutaneous coronary intervention (n = 57) | ||||
| Ischemic time > 4 hours-no. (%) | 38 (68) | 17 (68) | 21 (68) | 0.98 |
| Multivessel disease-no. (%) | 44 (76) | 20 (77) | 24 (75) | 0.86 |
| Pre-PCI Impella® placement-no. (%) | 12 (22) | 4 (17) | 8 (26) | 0.46 |
| Culprit PCI-no. (%) | 53 (95) | 23 (92) | 30 (97) | 0.43 |
| Immediate complete PCI-no. (%) | 23 (41) | 11 (44) | 12 (39) | 0.69 |
| Delayed complete PCI-no. (%) | 9 (16) | 6 (24) | 3 (10) | 0.15 |
| Pre-PCI TIMI-no. (%) | 37 (65) | 13 (50) | 24 (75) | 0.046 |
| post-PCI TIMI 3-no. (%) | 50 (88) | 21 (84) | 28 (90) | 0.48 |
| Cardiogenic Shock (n = 62) | Recovery (n = 27, 44%) | Non-Recovery (n = 35, 56%) | p-Value | |
|---|---|---|---|---|
| Complications | ||||
| Atrial tachycardia-no. (%) | 20 (32) | 9 (33) | 11 (31) | 0.87 |
| Sustained ventricular Tachycardia-no. (%) | 21 (34) | 7 (26) | 14 (40) | 0.25 |
| High grade atrioventricular block-no. (%) | 5 (8) | 0 (0) | 5 (14) | 0.04 |
| Biological hemolysis-no. (%) | 54 (89) | 19 (73) | 35 (100) | 0.001 |
| Clinical hemolysis-no. (%) | 23 (38) | 8 (31) | 15 (44) | 0.29 |
| Sepsis-no. (%) | 30 (48) | 7 (26) | 23 (66) | 0.002 |
| Severe bleeding-no. (%) | 10 (16) | 3 (11) | 7 (20) | 0.35 |
| Impella® access-site bleeding-no. (%) | 31 (50) | 15 (58) | 16 (46) | 0.35 |
| Gastrointestinal bleeding-no. (%) | 7 (11) | 4 (15) | 3 (9) | 0.67 |
| Hemorrhagic shock-no. (%) | 9 (11) | 3 (11) | 6 (17) | 0.72 |
| Bleeding requiring surgical hemostasis-no. (%) | 5 (8) | 2 (7) | 3 (9) | 0.87 |
| Bleeding requiring Impella® removal-no. (%) | 6 (10) | 3 (11) | 3 (9) | 0.73 |
| Packed red blood cell transfusion | 5.2 ± 5.8 | 4.3 ± 5.7 | 5.8 ± 5.8 | 0.32 |
| Fresh frozen plasma transfusion | 1.1 ± 2.5 | 1.0 ± 3.0 | 1.2 ± 2.1 | 0.74 |
| Platelet concentrate transfusion | 2.5 ± 6.1 | 2.5 ± 5.4 | 2.5 ± 6.6 | 0.99 |
| Limb ischemia-no. (%) | 8 (13) | 4 (15) | 4 (11) | 0.72 |
| Limb ischemia requiring vascular surgery-no. (%) | 1 (2) | 0 (0) | 1 (3) | 0.36 |
| Ischemic stroke-no. (%) | 4 (7) | 2 (7) | 2 (6) | 0.79 |
| Hemorrhagic stroke-no. (%) | 0 (0) | 0 (0) | 0 (0) | - |
| Outcome at one month | ||||
| Still hospitalized-no. (%) | 23 (37) | 9 (33) | 14 (40) | 0.59 |
| Still hospitalized in ICU-no. (%) | 12 (19) | 3 (11) | 9 (26) | 0.15 |
| Hospital readmission-no. (%) | 3 (5) | 3 (11) | 0 (0) | 0.08 |
| ICU readmission-no. (%) | 2 (3) | 2 (7) | 0 (0) | 0.19 |
| Death-no. (%) | 22 (36) | 0 (0) | 22 (63) | - |
| LVAD-no. (%) | 12 (19) | 0 (0) | 12 (34) | - |
| Heart transplant-no. (%) | 3 (5) | 0 (0) | 3 (9) | - |
| Univariate Analysis | Multivariate Analysis (n = 55) | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| LVEF (for each more %) | 0.91 [0.85–0.97] | 0.004 | 0.89 [0.81–0.96] | 0.006 |
| Number of amines (for each additional amine) | 4.09 [1.74–9.62] | 0.001 | 4.31 [1.30–14.30] | 0.016 |
| Total bilirubin | 1.05 [1.00–1.09] | 0.03 | 1.07 [1.00–1.14] | 0.039 |
| Obesity (BMI > 30 kg/m2) | 0.22 [0.05–0.94] | 0.04 | 0.16 [0.23–1.08] | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fagot, J.; Bouisset, F.; Bonello, L.; Biendel, C.; Lhermusier, T.; Porterie, J.; Roncalli, J.; Galinier, M.; Elbaz, M.; Lairez, O.; et al. Early Evaluation of Patients on Axial Flow Pump Support for Refractory Cardiogenic Shock Is Associated with Left Ventricular Recovery. J. Clin. Med. 2020, 9, 4130. https://doi.org/10.3390/jcm9124130
Fagot J, Bouisset F, Bonello L, Biendel C, Lhermusier T, Porterie J, Roncalli J, Galinier M, Elbaz M, Lairez O, et al. Early Evaluation of Patients on Axial Flow Pump Support for Refractory Cardiogenic Shock Is Associated with Left Ventricular Recovery. Journal of Clinical Medicine. 2020; 9(12):4130. https://doi.org/10.3390/jcm9124130
Chicago/Turabian StyleFagot, Jérôme, Frédéric Bouisset, Laurent Bonello, Caroline Biendel, Thibaut Lhermusier, Jean Porterie, Jerome Roncalli, Michel Galinier, Meyer Elbaz, Olivier Lairez, and et al. 2020. "Early Evaluation of Patients on Axial Flow Pump Support for Refractory Cardiogenic Shock Is Associated with Left Ventricular Recovery" Journal of Clinical Medicine 9, no. 12: 4130. https://doi.org/10.3390/jcm9124130