Role of Thromboelastography as an Early Predictor of Disseminated Intravascular Coagulation in Patients with Septic Shock

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
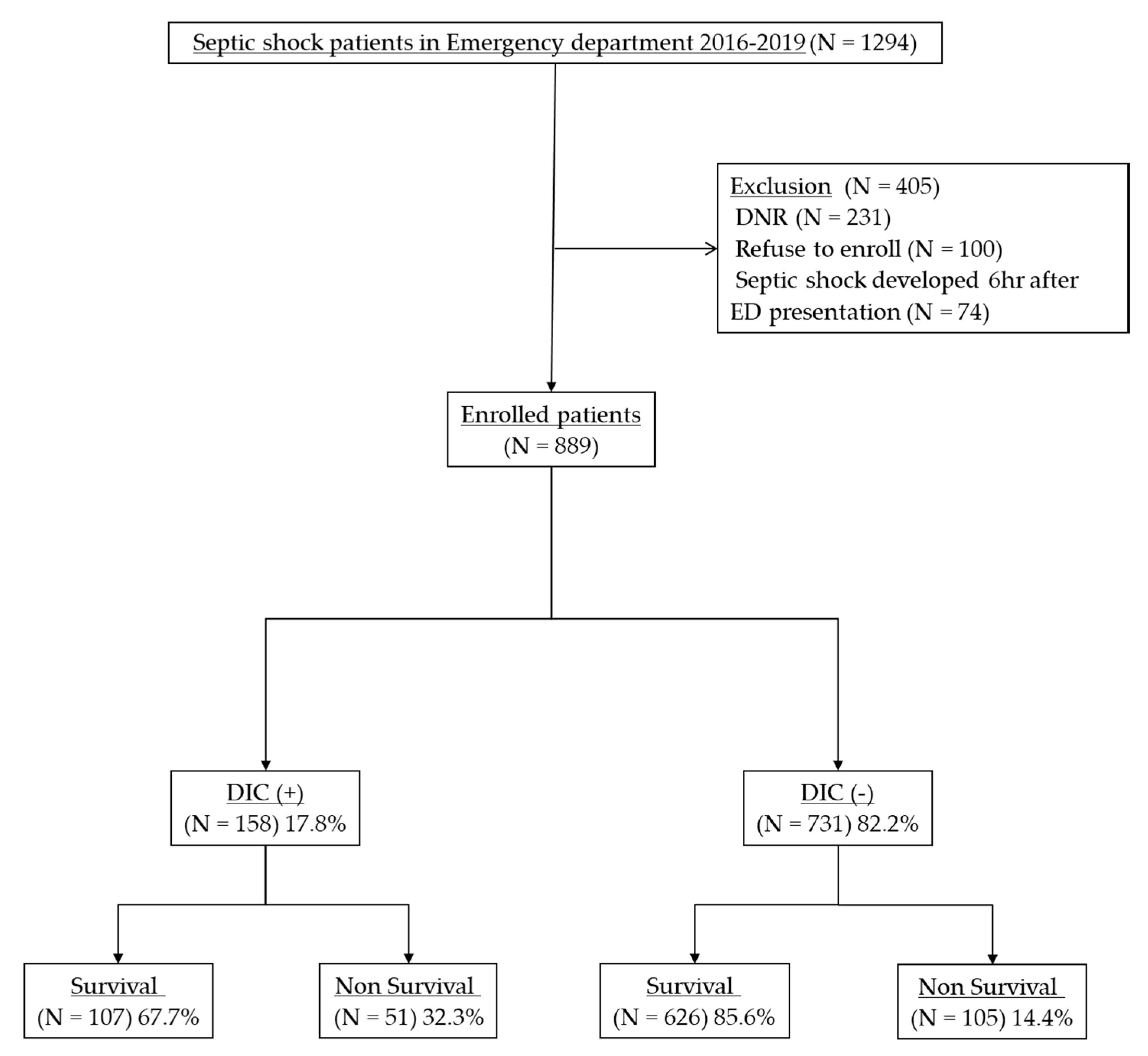
2.1. Study Design and Patients
2.2. Data Collection
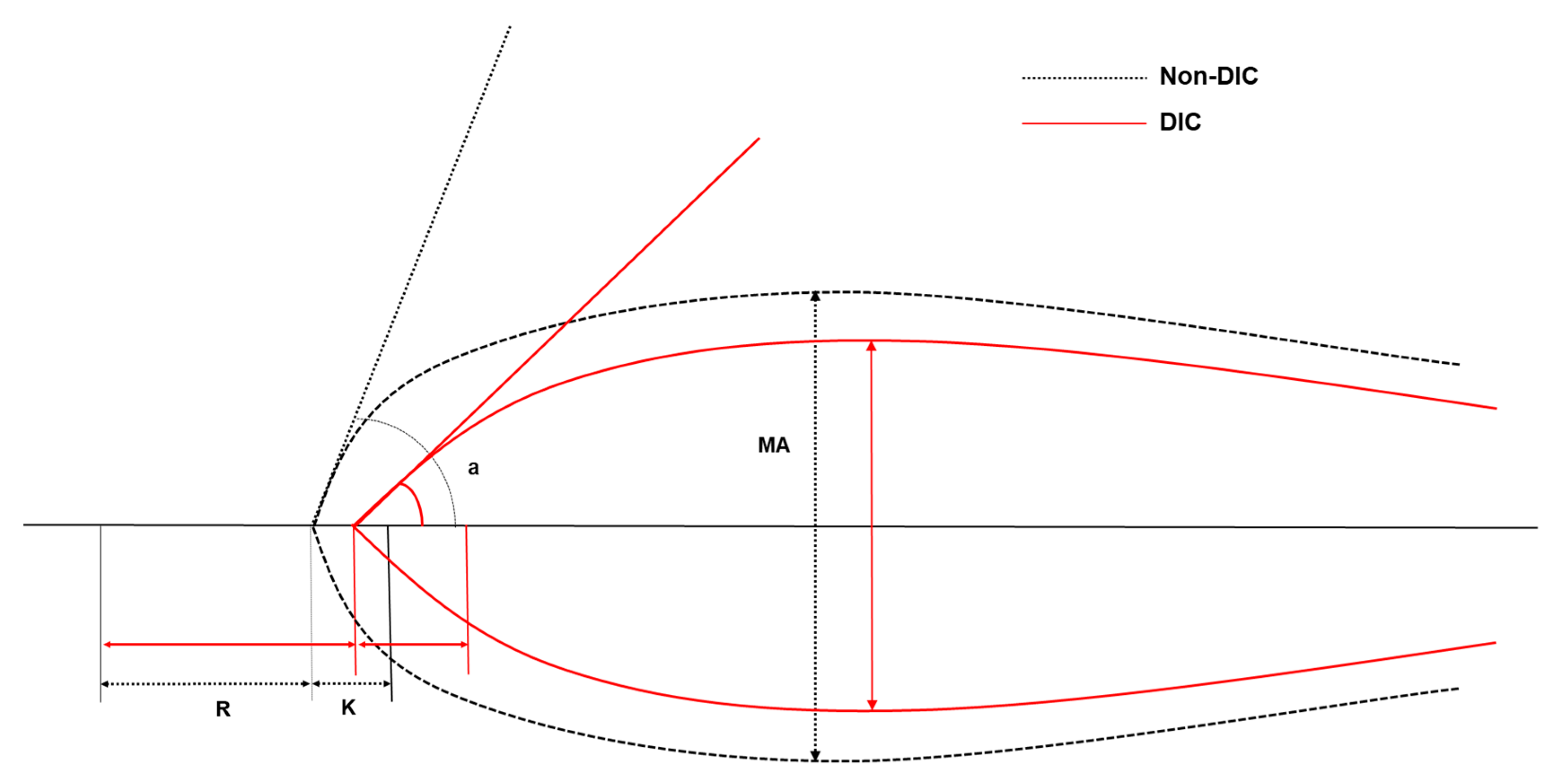
2.3. Thromboelastography
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Thromboelastography Analysis
3.3. Risk Factors Associated with DIC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Iba, T.; Levy, J.H. Sepsis-induced Coagulopathy and Disseminated Intravascular Coagulation. Anesthesiology 2020, 132, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Delabranche, X.; Helms, J.; Meziani, F. Immunohaemostasis: A new view on haemostasis during sepsis. Ann. Intens. Care 2017, 7, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wada, H.; Wakita, Y.; Nakase, T.; Shimura, M.; Hiyoyama, K.; Nagaya, S.; Mori, Y.; Shiku, H. Outcome of disseminated intravascular coagulation in relation to the score when treatment was begun. Mie DIC Study Group. Thromb. Haemost. 1995, 74, 848–852. [Google Scholar] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Taylor, F.B., Jr.; Toh, C.H.; Hoots, W.K.; Wada, H.; Levi, M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef] [Green Version]
- Iba, T.; Umemura, Y.; Watanabe, E.; Wada, T.; Hayashida, K.; Kushimoto, S. Diagnosis of sepsis-induced disseminated intravascular coagulation and coagulopathy. Acute Med Surg 2019, 6, 223–232. [Google Scholar] [CrossRef]
- Reikvam, H.; Steien, E.; Hauge, B.; Liseth, K.; Hagen, K.G.; Størkson, R.; Hervig, T. Thrombelastography. Trans. Apher. Sci. 2009, 40, 119–123. [Google Scholar] [CrossRef]
- Mohamed, M.; Majeske, K.; Sachwani, G.R.; Kennedy, K.; Salib, M.; McCann, M. The impact of early thromboelastography directed therapy in trauma resuscitation. Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 99. [Google Scholar] [CrossRef] [Green Version]
- Trautman, C.L.; Palmer, W.C.; Taner, C.B.; Canabal, J.M.; Getz, T.; Goldman, A.; Heckman, M.G.; Diehl, N.N.; Lee, D.D.; Stancampiano, F.F. Thromboelastography as a Predictor of Outcomes Following Liver Transplantation. Transplant Proc. 2017, 49, 2110–2116. [Google Scholar] [CrossRef]
- Welsby, I.J.; Jiao, K.; Ortel, T.L.; Brudney, C.S.; Roche, A.M.; Bennett-Guerrero, E.; Gan, T.J. The kaolin-activated Thrombelastograph predicts bleeding after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2006, 20, 531–535. [Google Scholar] [CrossRef]
- Yu, G.; Kim, Y.J.; Jeon, S.B.; Kim, W.Y. Thromboelastography for prediction of hemorrhagic transformation in patients with acute ischemic stroke. Am. J. Emerg. Med. 2020, 38, 1772–1777. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.; Kim, Y.J.; Kim, J.S.; Kim, S.I.; Ryoo, S.M.; Ahn, S.; Kim, W.Y. Prognostic value of repeated thromboelastography measurement for favorable neurologic outcome during targeted temperature management in out-of-hospital cardiac arrest survivors. Resuscitation 2020, 155, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Ostrowski, S.R.; Windeløv, N.A.; Ibsen, M.; Haase, N.; Perner, A.; Johansson, P.I. Consecutive thrombelastography clot strength profiles in patients with severe sepsis and their association with 28-day mortality: A prospective study. J. Crit. Care 2013, 28, 317.e311. [Google Scholar] [CrossRef] [PubMed]
- Haase, N.; Ostrowski, S.R.; Wetterslev, J.; Lange, T.; Møller, M.H.; Tousi, H.; Steensen, M.; Pott, F.; Søe-Jensen, P.; Nielsen, J.; et al. Thromboelastography in patients with severe sepsis: A prospective cohort study. Intens. Care Med. 2015, 41, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Koami, H.; Sakamoto, Y.; Ohta, M.; Goto, A.; Narumi, S.; Imahase, H.; Yahata, M.; Miike, T.; Iwamura, T.; Yamada, K.C.; et al. Can rotational thromboelastometry predict septic disseminated intravascular coagulation? Blood Coagul. Fibrinol. 2015, 26, 778–783. [Google Scholar] [CrossRef]
- Ryoo, S.M.; Lee, J.; Lee, Y.S.; Lee, J.H.; Lim, K.S.; Huh, J.W.; Hong, S.B.; Lim, C.M.; Koh, Y.; Kim, W.Y. Lactate Level Versus Lactate Clearance for Predicting Mortality in Patients With Septic Shock Defined by Sepsis-3. Crit. Care Med. 2018, 46, e489–e495. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef]
- Levi, M.; Toh, C.H.; Thachil, J.; Watson, H.G. Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br. J. Haematol. 2009, 145, 24–33. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intens. Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Sharma, S.K.; Philip, J.; Wiley, J. Thromboelastographic changes in healthy parturients and postpartum women. Anesth. Analg. 1997, 85, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, N.A.; Hathaway, W.E.; Jacobson, L.; Manco-Johnson, M.J. A new global assay of coagulation and fibrinolysis. Thromb. Res. 2005, 116, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Iba, T.; Eguchi, Y.; Ohtomo, Y.; Okamoto, K.; Koseki, K.; Mayumi, T.; Murata, A.; Ikeda, T.; Ishikura, H.; et al. A multicenter, prospective validation of disseminated intravascular coagulation diagnostic criteria for critically ill patients: Comparing current criteria. Crit. Care Med. 2006, 34, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Nisio, M.D.; Levy, J.H.; Kitamura, N.; Thachil, J. New criteria for sepsis-induced coagulopathy (SIC) following the revised sepsis definition: A retrospective analysis of a nationwide survey. BMJ Open 2017, 7, e017046. [Google Scholar] [CrossRef] [Green Version]
- Hunt, B.J.; Allard, S.; Keeling, D.; Norfolk, D.; Stanworth, S.J.; Pendry, K. A practical guideline for the haematological management of major haemorrhage. Br. J. Haematol. 2015, 170, 788–803. [Google Scholar] [CrossRef]
- McDonald, M.M.; Wetzel, J.; Fraser, S.; Elliott, A.; Bowry, R.; Kawano-Castillo, J.F.; Cai, C.; Sangha, N.; Messier, J.; Hassler, A.; et al. Thrombelastography does not predict clinical response to rtPA for acute ischemic stroke. J. Thromb. Thrombol. 2016, 41, 505–510. [Google Scholar] [CrossRef]
- Sharma, P.; Saxena, R. A novel thromboelastographic score to identify overt disseminated intravascular coagulation resulting in a hypocoagulable state. Am. J. Clin. Pathol. 2010, 134, 97–102. [Google Scholar] [CrossRef] [Green Version]
- Gonano, C.; Sitzwohl, C.; Meitner, E.; Weinstabl, C.; Kettner, S.C. Four-day antithrombin therapy does not seem to attenuate hypercoagulability in patients suffering from sepsis. Crit. Care 2006, 10, R160. [Google Scholar] [CrossRef] [Green Version]
- Daudel, F.; Kessler, U.; Folly, H.; Lienert, J.S.; Takala, J.; Jakob, S.M. Thromboelastometry for the assessment of coagulation abnormalities in early and established adult sepsis: A prospective cohort study. Crit. Care 2009, 13, R42. [Google Scholar] [CrossRef] [Green Version]
- Sivula, M.; Pettilä, V.; Niemi, T.T.; Varpula, M.; Kuitunen, A.H. Thromboelastometry in patients with severe sepsis and disseminated intravascular coagulation. Blood Coagul. Fibrinol. 2009, 20, 419–426. [Google Scholar] [CrossRef]
- Panigada, M.; Zacchetti, L.; L’Acqua, C.; Cressoni, M.; Anzoletti, M.B.; Bader, R.; Protti, A.; Consonni, D.; D’Angelo, A.; Gattinoni, L. Assessment of Fibrinolysis in Sepsis Patients with Urokinase Modified Thromboelastography. PLoS ONE 2015, 10, e0136463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semeraro, N.; Ammollo, C.T.; Semeraro, F.; Colucci, M. Coagulopathy of Acute Sepsis. Semin. Thromb. Hemost. 2015, 41, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Arakawa, M.; Di Nisio, M.; Gando, S.; Anan, H.; Sato, K.; Ueki, Y.; Levy, J.H.; Thachil, J. Newly Proposed Sepsis-Induced Coagulopathy Precedes International Society on Thrombosis and Haemostasis Overt-Disseminated Intravascular Coagulation and Predicts High Mortality. J Intens. Care Med. 2020, 35, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Warren, B.L.; Eid, A.; Singer, P.; Pillay, S.S.; Carl, P.; Novak, I.; Chalupa, P.; Atherstone, A.; Pénzes, I.; Kübler, A.; et al. Caring for the critically ill patient. High-dose antithrombin III in severe sepsis: A randomized controlled trial. JAMA 2001, 286, 1869–1878. [Google Scholar] [CrossRef] [PubMed]
- Allingstrup, M.; Wetterslev, J.; Ravn, F.B.; Møller, A.M.; Afshari, A. Antithrombin III for critically ill patients: A systematic review with meta-analysis and trial sequential analysis. Intens. Care Med. 2016, 42, 505–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranieri, V.M.; Thompson, B.T.; Barie, P.S.; Dhainaut, J.F.; Douglas, I.S.; Finfer, S.; Gårdlund, B.; Marshall, J.C.; Rhodes, A.; Artigas, A.; et al. Drotrecogin alfa (activated) in adults with septic shock. N. Engl. J. Med. 2012, 366, 2055–2064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.L.; Francois, B.; Zabolotskikh, I.; Daga, M.K.; Lascarrou, J.B.; Kirov, M.Y.; Pettilä, V.; Wittebole, X.; Meziani, F.; Mercier, E.; et al. Effect of a Recombinant Human Soluble Thrombomodulin on Mortality in Patients With Sepsis-Associated Coagulopathy: The SCARLET Randomized Clinical Trial. JAMA 2019, 321, 1993–2002. [Google Scholar] [CrossRef] [Green Version]
- Kienast, J.; Juers, M.; Wiedermann, C.J.; Hoffmann, J.N.; Ostermann, H.; Strauss, R.; Keinecke, H.O.; Warren, B.L.; Opal, S.M. Treatment effects of high-dose antithrombin without concomitant heparin in patients with severe sepsis with or without disseminated intravascular coagulation. J. Thromb. Haemost. 2006, 4, 90–97. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Raj, A.; Warkentin, T.E. Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation. J. Clin. Med. 2019, 8, 728. [Google Scholar] [CrossRef] [Green Version]
- Umemura, Y.; Yamakawa, K. Optimal patient selection for anticoagulant therapy in sepsis: An evidence-based proposal from Japan. J. Thromb. Haemost 2018, 16, 462–464. [Google Scholar] [CrossRef] [Green Version]
- Othman, M.; Kaur, H. Thromboelastography (TEG). Methods Mol. Biol. 2017, 1646, 533–543. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, S.G.; Luddington, R.J. Critical factors contributing to the thromboelastography trace. Semin. Thromb. Hemost. 2010, 36, 712–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Total (N = 889) | Non-DIC (N = 731) | DIC (N = 158) | p-Value |
|---|---|---|---|---|
| Age, years | 65.6 ± 12.7 | 66.2 ± 12.5 | 62.8 ± 13.2 | 0.002 |
| Male | 521 (58.6) | 437 (59.8) | 84 (53.2) | 0.131 |
| Medical history | ||||
| Hypertension | 314 (35.3) | 56 (35.4) | 258 (35.3) | 1.000 |
| Diabetes mellitus | 227 (25.5) | 196 (26.8) | 31 (19.6) | 0.070 |
| Chronic pulmonary disease | 89 (10.0) | 76 (10.4) | 13 (8.2) | 0.467 |
| Hematologic disease | 55 (6.2) | 44 (6.0) | 11 (7.0) | 0.715 |
| Malignancy | 425 (47.8) | 343 (46.9) | 82 (51.9) | 0.292 |
| Chronic renal disease | 59 (6.6) | 48 (6.6) | 11 (7.0) | 0.860 |
| Chronic liver disease | 141 (15.9) | 86 (11.8) | 55 (34.8) | 0.000 |
| Source of infection | ||||
| Pulmonary | 216 (24.3) | 187 (25.6) | 29 (18.4) | 0.065 |
| Genitourinary | 125 (14.1) | 105 (14.4) | 20 (12.7) | 0.616 |
| Gastrointestinal | 124 (13.9) | 99 (13.5) | 25 (15.8) | 0.449 |
| Hepatobiliary | 302 (34.0) | 242 (33.1) | 60 (38.0) | 0.266 |
| Blood stream | 58 (6.5) | 41 (5.6) | 17 (10.8) | 0.031 |
| Others | 36 (4.0) | 28 (3.8) | 8 (5.1) | 0.503 |
| Unknown | 90 (10.1) | 69 (9.4) | 21 (13.3) | 0.147 |
| Laboratory findings | ||||
| White blood cell, ×103/uL | 11.8 ± 10.7 | 12.1 ± 10.8 | 10.7 ± 10.3 | 0.138 |
| Hemoglobin, g/dL | 10.7 ± 2.4 | 10.8 ± 2.4 | 10.1 ± 2.3 | 0.001 |
| Blood urea nitrogen, mg/dL | 31.1 ± 20.3 | 30.8 ± 20.8 | 32.7 ± 17.7 | 0.299 |
| Creatinine, mg/dL | 2.0 ± 2.3 | 1.9 ± 2.0 | 2.4 ± 3.1 | 0.053 |
| Albumin, g/dL | 2.7 ± 1.6 | 2.8 ± 1.6 | 2.4 ± 1.6 | 0.025 |
| Initial Lactate, mmol/L | 4.1 ± 3.1 | 3.7 ± 2.8 | 5.8 ± 3.8 | 0.000 |
| Initial SOFA score | 5.9 ± 3.1 | 5.4 ± 2.9 | 8.1 ± 3.0 | 0.000 |
| APACHE II score | 17.5 ± 8.1 | 16.8 ± 7.7 | 20.4 ± 9.1 | 0.000 |
| Length of ICU stay | 8.1 ± 11.1 | 8.1 ± 11.7 | 8.0 ± 9.0 | 0.924 |
| Clinical Outcome | ||||
| 28-day mortality | 156 (17.5%) | 105 (14.4%) | 51 (32.3%) | 0.000 |
| 90-day mortality | 273 (30.7%) | 195 (26.7%) | 78 (49.4%) | 0.000 |
| Total (N = 889) | Non-DIC (N = 731) | DIC (N = 158) | p-Value | |
|---|---|---|---|---|
| Platelet, ×103/uL | 161.9 ± 114.1 | 180.9 ± 112.3 | 74.2 ± 75.0 | 0.000 |
| PT (INR) | 1.47 ± 0.91 | 1.34 ± 0.53 | 2.05 ± 1.74 | 0.000 |
| aPTT, s | 34.5 ± 15.9 | 32.1 ± 11.7 | 45.7 ± 25.3 | 0.000 |
| D-dimer, ug/mL | 4.6 (2.2–10.6) | 3.8 (1.8–7.3) | 12.3 (7.7–21.8) | 0.000 |
| FDP, ug/mL | 13.9 (7.2–26.6) | 12.1 (6.8–21.2) | 29.6 (17.7–54.4) | 0.000 |
| Fibrinogen, mg/dL | 424.5 ± 186.5 | 446.3 ± 180.5 | 323.3 ± 180.7 | 0.000 |
| ISTH score | 3 (2–4) | 2 (1–3) | 5 (5–6) | 0.000 |
| Variables | Total (N = 889) | Non-DIC (N = 731) | DIC (N = 158) | AUC | p-Value |
|---|---|---|---|---|---|
| R, min | 6.9 ± 6.7 | 6.5 ± 5.9 | 9.0 ± 9.5 | 0.679 | 0.001 |
| K, min | 2.6 ± 3.9 | 2.2 ± 3.4 | 4.3 ± 5.3 | 0.793 | 0.000 |
| Alpha angle, degree | 61.6 ± 15.8 | 64.0 ± 14.5 | 50.6 ± 16.9 | 0.766 | 0.000 |
| MA, mm | 61.3 ± 14.5 | 64.1 ± 12.9 | 48.5 ± 14.6 | 0.814 | 0.000 |
| LY30, % | 1.2 ± 6.2 | 1.3 ± 6.0 | 0.9 ± 7.1 | 0.631 | 0.549 |
| Coagulation index | 2.2 ± 2.5 | 2.7 ± 2.2 | −0.1 ± 2.9 | 0.819 | 0.000 |
| Variables | Non-DIC | DIC | Se/Sp (%) | PPV/NPV (%) | PLR/NLR |
|---|---|---|---|---|---|
| K > 2.0, min | 235 (32.1%) | 122 (77.2%) | 77.22/67.85% | 34.17/93.23% | 2.40/0.34 |
| MA < 60, mm | 77 (10.5%) | 80 (50.6%) | 79.11/73.05% | 38.82/94.18% | 2.94/0.29 |
| CI < 1.8 | 187 (25.6%) | 120 (75.9%) | 75.95/74.42% | 39.09/93.47% | 2.97/0.32 |
| Characteristics | Univariate OR (95% CI) | Multivariate OR (95% CI) | p-Value |
|---|---|---|---|
| Age, years | OR, 0.979 (95% CI, 0.967–0.992) | OR, 0.981 (95% CI, 0.965–0.997) | 0.019 |
| Initial lactate, mmol/L | OR, 1.210 (95% CI, 1.150–1.273) | OR, 1.179 (95% CI, 1.109–1.253) | 0.000 |
| SOFA score | OR, 1.316 (95% CI, 1.241–1.397) | OR, 1.167 (95% CI, 1.091–1.248) | 0.000 |
| APACHE II score | OR, 1.052 (95% CI, 1.031–1.074) | ||
| K > 2.0, min | OR, 7.153 (95% CI, 4.781–10.701) | OR, 1.696 (95% CI, 0.972–2.959) | 0.063 |
| MA < 60, mm | OR, 10.268 (95% CI, 6.767–15.579) | OR, 5.616 (95% CI, 3.213–9.818) | 0.000 |
| CI < 1.8 | OR, 9.187 (95% CI, 6.153–13.717) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.M.; Kim, S.-I.; Yu, G.; Kim, J.-S.; Hong, S.I.; Chae, B.; Shin, Y.S.; Kim, Y.J.; Jang, S.; Kim, W.Y. Role of Thromboelastography as an Early Predictor of Disseminated Intravascular Coagulation in Patients with Septic Shock. J. Clin. Med. 2020, 9, 3883. https://doi.org/10.3390/jcm9123883
Kim SM, Kim S-I, Yu G, Kim J-S, Hong SI, Chae B, Shin YS, Kim YJ, Jang S, Kim WY. Role of Thromboelastography as an Early Predictor of Disseminated Intravascular Coagulation in Patients with Septic Shock. Journal of Clinical Medicine. 2020; 9(12):3883. https://doi.org/10.3390/jcm9123883
Chicago/Turabian StyleKim, Sang Min, Sang-Il Kim, Gina Yu, June-Sung Kim, Seok In Hong, Bora Chae, Yo Sep Shin, Youn Jung Kim, Seongsoo Jang, and Won Young Kim. 2020. "Role of Thromboelastography as an Early Predictor of Disseminated Intravascular Coagulation in Patients with Septic Shock" Journal of Clinical Medicine 9, no. 12: 3883. https://doi.org/10.3390/jcm9123883