Outcomes of Liver Resections after Liver Transplantation at a High-Volume Hepatobiliary Center

 , , , , , , , , , and
, , , , , , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Data Acquisition
2.2. Liver Resection and ReLT
- with ReLT earlier than twelve months after primary LT,
- high urgency transplantation.
2.3. Immunosuppression
2.4. Statistics
3. Results
3.1. Liver Resections
3.2. ReLTs
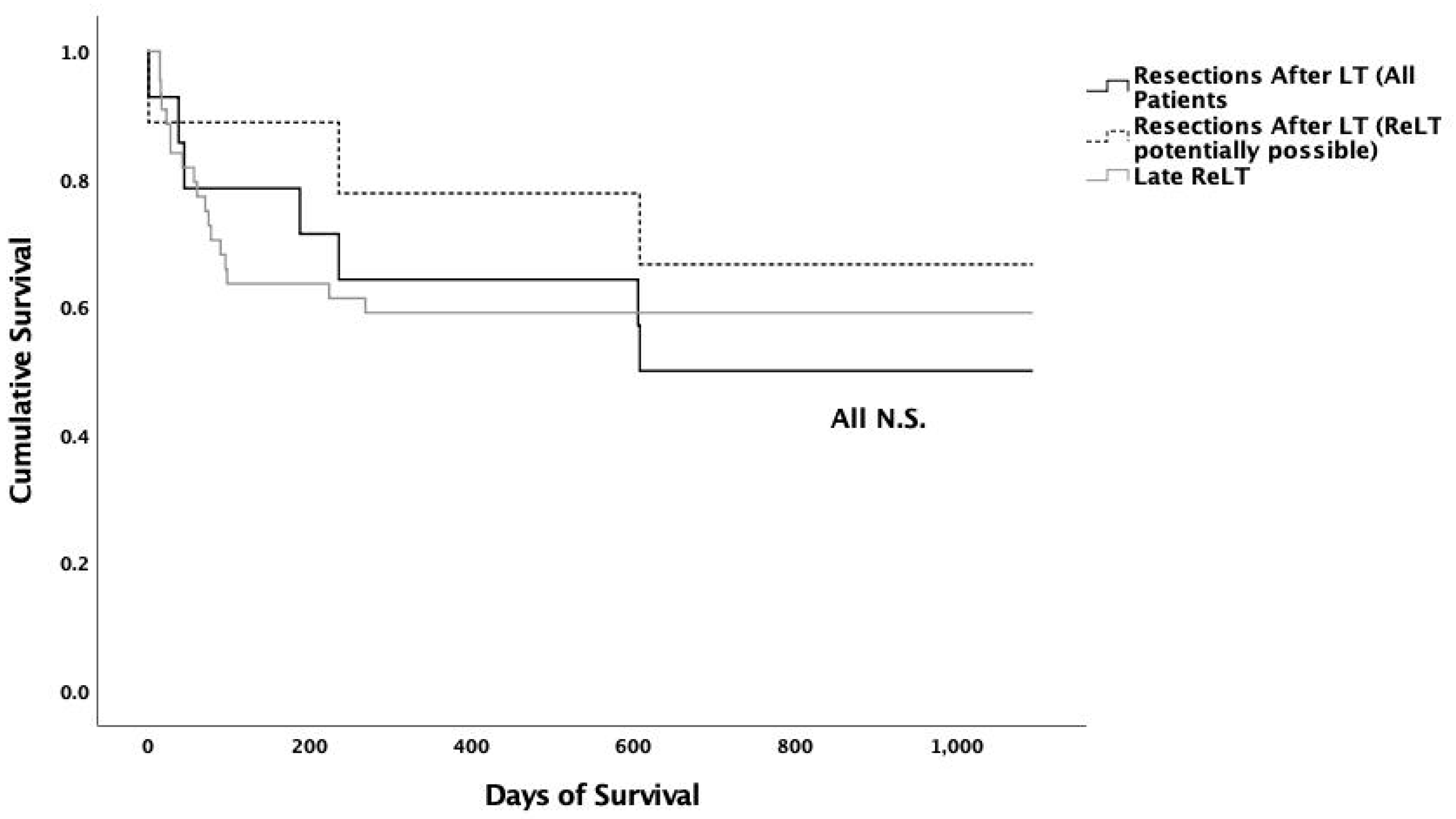
3.3. Complications and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| HCC | Hepatocellular carcinoma |
| HCV | Hepatitis C virus |
| IBL | Ischemic Biliary Lesions |
| ITBL | Ischemic Type Biliary Lesions |
| IQR | Interquartile Range |
| LT | Liver Transplantation |
| MELD | Model for End-Stage Liver Disease |
| POD | Postoperative Day |
| ReLT | Liver Retransplantation |
| SD | Standard Deviation |
References
- Catalano, G.; Urbani, L.; Biancofiore, G.; Bindi, L.; Boldrini, A.; Consani, G.; Bisà, M.; Campatelli, A.; Petruzzi, P.; Cioni, R.; et al. Hepatic resection after liver transplantation as a graft-saving procedure: Indication criteria, timing and outcome. Transplant. Proc. 2004, 36, 545–546. [Google Scholar] [CrossRef]
- Chari, R.S.; Baker, M.E.; Sue, S.R.; Meyers, W.C. Regeneration of a transplanted liver after right hepatic lobectomy. Liver Transplant. Surg. 1996, 2, 233–234. [Google Scholar] [CrossRef]
- Dousset, B.; Filipponi, F.; Soubrane, O.; Boillot, O.; Houssin, D.; Chapuis, Y. Partial hepatic resection for ischemic graft damage after liver transplantation: A graft-saving option? Surgery 1994, 115, 540–545. [Google Scholar]
- Filipponi, F.; Vistoli, F.; Urbani, L.; Mosca, F. Extended right hepatectomy as graft-saving option in non-anastomotic biliary strictures after liver transplantation. Hepatogastroenterology 2002, 49, 1679–1681. [Google Scholar]
- Guckelberger, O.; Stange, B.; Glanemann, M.; Lopez-Hänninen, E.; Heidenhain, C.; Jonas, S.; Klupp, J.; Neuhaus, P.; Langrehr, J.M. Hepatic Resection in Liver Transplant Recipients: Single Center Experience and Review of the Literature. Am. J. Transplant. 2005, 5, 2403–2409. [Google Scholar] [CrossRef]
- Honoré, P.; Detry, O.; Hamoir, E.; Deféchereux, T.; Detroz, B.; Meurisse, M.; Jacquet, N. Right hepatic lobectomy as a liver graft–saving procedure. Liver Transplant. 2001, 7, 269–273. [Google Scholar] [CrossRef]
- Marangoni, G.; Faraj, W.; Sethi, H.; Rela, M.; Muiesan, P.; Heaton, N. Liver resection in liver transplant recipients. Hepatobiliary Pancreat. Dis. Int. 2008, 7, 590–594. [Google Scholar]
- Sommacale, D.; Dondero, F.; Sauvanet, A.; Francoz, C.; Durand, F.; Farges, O.; Kianmanesh, R.; Belghiti, J. Liver resection in transplanted patients: A single-center western experience. Transplant. Proc. 2013, 45, 2726–2728. [Google Scholar] [CrossRef]
- Guerra, J.F.; Jarufe, N.; Martinez, J. Hepatic resection after liver transplantation as a graft-saving procedure. Transplant. Proc. 2009, 41, 1994–1996. [Google Scholar] [CrossRef]
- Huang, J.; Yan, L.; Wu, H.; Yang, J.; Liao, M.H.; Zeng, Y. Is radiofrequency ablation applicable for recurrent hepatocellular carcinoma after liver transplantation? J. Surg. Res. 2016, 200, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Kornberg, A.; Küpper, B.; Tannapfel, A.; Katenkamp, K.; Thrum, K.; Habrecht, O.; Wilberg, J. Long-term survival after recurrent hepatocellular carcinoma in liver transplant patients: Clinical patterns and outcome variables. Eur. J. Surg. Oncol. 2010, 36, 275–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regalia, E.; Fassati, L.R.; Valente, U.; Pulvirenti, A.; Damilano, I.; Dardano, G.; Montalto, F.; Coppa, J.; Mazzaferro, V. Pattern and management of recurrent hepatocellular carcinoma after liver transplantation. J. Hepatobiliary Pancreat. Surg. 1998, 5, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Roayaie, S.; Schwartz, J.D.; Sung, M.W.; Emre, S.; Miller, C.M.; Gondolesi, G.; Krieger, N.; Schwartz, M. Recurrence of hepatocellular carcinoma after liver transplant: Patterns and prognosis. Liver Transplant. 2004, 10, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Schlitt, H.J.; Neipp, M.; Weimann, A.; Oldhafer, K.J.; Schmoll, E.; Boeker, K.; Nashan, B.; Kubicka, S.; Maschek, H.; Tusch, G.; et al. Recurrence patterns of hepatocellular and fibrolamellar carcinoma after liver transplantation. J. Clin. Oncol. 1999, 17, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Taketomi, A.; Fukuhara, T.; Morita, K.; Kayashima, H.; Ninomiya, M.; Yamashita, Y.; Ikegami, T.; Uchiyama, H.; Yoshizumi, T.; Soejima, Y.; et al. Improved results of a surgical resection for the recurrence of hepatocellular carcinoma after living donor liver transplantation. Ann. Surg. Oncol. 2010, 17, 2283–2289. [Google Scholar] [CrossRef] [PubMed]
- Valdivieso, A.; Bustamante, J.; Gastaca, M.; Uriarte, J.; Ventoso, A.; Ruiz, P.; Fernandez, J.; Pijoan, I.; Testillano, M.; Suarez, M.; et al. Management of hepatocellular carcinoma recurrence after liver transplantation. Transplant. Proc. 2010, 42, 660–662. [Google Scholar] [CrossRef]
- Jarnagin, W.R.; Gonen, M.; Fong, Y.; DeMatteo, R.P.; Ben-Porat, L.; Little, S.; Corvera, C.; Weber, S.; Blumgart, L.H. Improvement in perioperative outcome after hepatic resection: Analysis of 1,803 consecutive cases over the past decade. Ann. Surg. 2002, 236, 397–406, discussion -7. [Google Scholar] [CrossRef]
- Azoulay, D.; Linhares, M.M.; Huguet, E.; Delvart, V.; Castaing, D.; Adam, R.; Ichai, P.; Saliba, F.; Lemoine, A.; Samuel, D.; et al. Decision for retransplantation of the liver: An experience- and cost-based analysis. Ann. Surg. 2002, 236, 713–721, discussion 21. [Google Scholar] [CrossRef]
- Dʼalessandro, A.M.; Ploeg, R.J.; Knechtle, S.; Pirsch, J.D.; Stegall, M.D.; Hoffmann, R.; Sollinger, H.W.; Belzer, F.O.; Kalayoglu, M. Retransplantation of the liver—A seven-year experience. Transplantation 1993, 55, 1083–1087. [Google Scholar] [CrossRef]
- Mora, N.P.; Klintmalm, G.B.; Cofer, J.B.; Poplawski, S.S.; Goldstein, R.M.; Gonwa, T.A.; Husberg, B.S. Results after liver retransplantation (RETx): A comparative study between “elective” vs “nonelective” RETx. Transplant. Proc. 1990, 22, 1509–1511. [Google Scholar]
- Powelson, J.A.; Cosimi, A.B.; Lewis, W.D.; Rohrer, R.J.; Freeman, R.B.; Vacanti, J.P.; Jonas, M.; Lorber, M.I.; Marks, W.H.; Bradley, J.; et al. Hepatic retransplantation in New England—A regional experience and survival model. Transplantation 1993, 55, 802–806. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.F.; Liu, C. Liver retransplantation: Indications and outcomes. Hepatobiliary Pancreat. Dis. Int. 2004, 3, 175–178. [Google Scholar] [PubMed]
- Tacke, F.; Kroy, D.C.; Barreiros, A.P.; Neumann, U.P. Liver transplantation in Germany. Liver Transplant. 2016, 22, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Matzinger, P. The danger model: A renewed sense of self. Science 2002, 296, 301–305. [Google Scholar] [CrossRef] [Green Version]
- Semela, D.; Piguet, A.C.; Kolev, M.; Schmitter, K.; Hlushchuk, R.; Djonov, V.; Stoupis, C.; Dufour, J.F. Vascular remodeling and antitumoral effects of mTOR inhibition in a rat model of hepatocellular carcinoma. J. Hepatol. 2007, 46, 840–848. [Google Scholar] [CrossRef]
- Fan, S.T.; Lo, C.M.; Liu, C.L.; Lam, C.M.; Yuen, W.K.; Yeung, C.; Wong, J. Hepatectomy for hepatocellular carcinoma: Toward zero hospital deaths. Ann. Surg. 1999, 229, 322–330. [Google Scholar] [CrossRef]
- Hong, J.C.; Kaldas, F.M.; Kositamongkol, P.; Petrowsky, H.; Farmer, D.G.; Markovic, D.; Hiatt, J.R.; Busuttil, R.W. Predictive index for long-term survival after retransplantation of the liver in adult recipients: Analysis of a 26-year experience in a single center. Ann. Surg. 2011, 254, 444–449, discussion 8–9. [Google Scholar] [CrossRef]
- Wiering, L.; Öllinger, R.; Kruppa, J.; Schoeneberg, U.; Dziodzio, T.; Jara, M.; Biebl, M.; Dargie, R.; Raschzok, N.; Schöning, W.; et al. Hospitalization before liver transplantation predicts post-transplant patient survival—A propensity-score matched analysis. Liver Transplant. 2020, 26, 628–639. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Authors | Year | Patients | Indications for LR | Resection Type | Time after LT (Range) | Survival | Outcome | Key Findings |
|---|---|---|---|---|---|---|---|---|
| Dousett et al. [3] | 1994 | 7 | 4 Septic parenchymal infarcts, 3 Nonanastomotic biliary strictures | 4 Left Hepatectomies, 2 Left Lobectomies, 1 Right Hepatectomy | 3–218 w | 1 dead (tumor recurrence); 6 alive (last follow-up 12–45 mo) | 2 recurrent ischemic cholangitis, 1 ReLT (recurrent Budd-Chiari Syndrome) | In selected patients with localized ischemic damage to the graft LR is a safe procedure. |
| Chari et al. [2] | 1996 | 1 | 1 Ischemic right hepatic lobe | 1 Right Hepatic Lobectomy | 14 mo | Not mentioned | 1 uncomplicated | Due to the preserved regenerative capacity in liver grafts hepatectomies are feasible. |
| Guerra et al. [9] | 1996 | 2 | 1 Arterial thrombosis, 1 Biloma and bile duct necrosis | 2 Left Lateral Segmentectomy | 6 w, 42 mo | ---- | 2 uncomplicated | LR after LT in selected cases is a graft-saving procedure with low morbidity. |
| Regalia et al. [12] | 1998 | 2 | 2 HCC recurrence | ---- | ---- | 2 alive, no recurrence (last follow-up 15 and 67 mo) | ---- | Surgical resection of HCC recurrence is effective in controlling tumor progression, especially if recurrence appears only in the graft. |
| Schlitt et al. [14] | 1999 | 3 | 3 HCC recurrence | ---- | ---- | ---- | ---- | Surgical resection was the only treatment option compared to chemotherapy and radiotherapy with prolonged survival, especially after late recurrence after LT and should therefore be considered whenever possible. |
| Honore et al. [6] | 2001 | 4 | 3 Biliary strictures, 1 Ischemic necrosis | 4 Right Hepatic Lobectomies (Seg V, VI, VII, VIII) | 2 d–78 mo | 4 alive (last follow-up 18–53 mo) | 3 uncomplicated, 1 ReLT | Outcome after right hepatic lobectomies in liver grafts is comparable with non-transplanted patients in selected cases. |
| Catalano et al. [1] | 2004 | 12 | 5 ITBL, 2 HCC recurrence, 2 Accessory left HAT, 1 Segmental left HAT, 1 Trauma, 1 Liver abscesses | 4 Left Lobectomies (Seg II, III); 3 Right Hepatectomies (V, VI, VII, VIII); 2 Extended Right Hemihepatectomies (IV, V, VI, VII, VIII), 1 Right Lateral Sectoriectomy (VI, VII), 1 Anterior Trisegmentomy (IV, V, VI), 1 Segmentectomy (IV) | 5 d–1421 d | 7 dead (3d–29 mo); 5 alive (last follow-up 3-32 mo) | Early resections (<3 mo after LT): 66.6% (n = 2) perioperative mortality; 1 alive Late resections (>3 months after LT): perioperative mortality 22.2% (n = 2); 2 died of recurrent HCC, 1 died of recurrent HCV, 4 alive | Early diagnosis and timing for LR are crucial, in early LR with sepsis ReLT is preferred. In late LR, timing is important to avoid e.g., the development of sepsis. |
| Roayaie et al. [13] | 2004 | 5 | 5 HCC recurrence | ---- | ---- | ---- | ---- | Patients with tumor recurrence should be resected or ablated. However, it is not clear whether surgical resection or the fact that patients with a tumor which is amendable for resection in a potentially more favorable group, causes higher survival rates. |
| Guckelberger et al. [5] | 2005 | 3 | 3 ITBL | 3 Left Hepatectomy | 13–149 mo | 3 alive (last follow-up 12–17 mo) | 1 ReLT (13 mo after resection; IBL) | In selected cases LR may prolong the survival of patients without the need of ReLT; however, early LR should be considered with caution. |
| Marangoni et al. [7] | 2008 | 11 | 4 HCC recurrence, 2 left HAT, 2 ITBL, 1 Liver Abscesses, 1 Sepsis and infected hematoma, 1 Ischemic segment IV | 2 Right Hepatectomies, 1 Extended Right Hepatectomy, 1 Left Hepatectomy, 3 Non-Anatomical Resections, 3 Left Lobectomies, 1 Segmentectomy | 0.1–194 mo | 3 dead (2 HCC recurrence, 1 PTLD); 8 alive (last follow-up 3–144 mo) | 1 ReLT (chronic rejection) | LR are safe and salvage grafts, particularly when performed for ischemic causes. Late resections show shorter ICU and hospital stays. Cure after recurrent HCC is uncommon; however, LR may be beneficial for those perspective patients. In selected patients LR after LT is a safe procedure. |
| Kornberg et al. [11] | 2010 | 2 | 2 HCC recurrence | ---- | ---- | ---- | ---- | If possible, surgical resection should be performed, as it has been shown to be the strongest independent predictor for long-term survival. |
| Taketomi et al. [15] | 2010 | 4 | 4 HCC recurrence | ---- | ---- | ---- | ---- | If available LR may be beneficial for the outcome of recurrence of HCC after LT. |
| Valdivieso et al. [16] | 2010 | 2 | 2 HCC recurrence | ---- | ---- | ---- | ----- | In patients with resectable HCC recurrence LR should be performed. Although in the whole study cohort (hepatic and/or extrahepatic HCC recurrence) 64% of the patients showed HCC re-recurrence). |
| Sommacale et al. [8] | 2013 | 8 | 3 HCC recurrence, 1 Left HAT, 1 Biliary leak, 1 Biliary stricture, 1 Biliary cyst, 1 Hydatid cyst | 4 Left lobectomies, 1 Right Hepatectomy, 1 Bisegmentectomy (VI, VII), 1 Biliary Fenestration, 1 Biliary Pericystectomy | 5–47 mo | 8 alive (last follow-up 11–156 mo) | ---- | LR is a safe procedure with high morbidity. LR can prevent patients from ReLT, particularly those with resectable HCC. |
| Huang et al. [10] | 2015 | 11 | 11 HCC recurrence | ---- | ---- | ---- | ---- | RFA is a treatment option in recurrent HCC, if surgical options are not applicable with comparable survival. |
| Pohl et al. | 2020 | 14 | 5 HCC, 5 Biliary tree pathologies, 2 Bilioma/abscesses, 1 PTLD, 1 Benign tumor | 6 Left Hemihepatectomies, 4 Multisegmentectomies, 2 right Hemihepatectomies, 2 Segmentectomies | 13–348 mo | 8 dead, 6 alive (last follow-up | 1 ReLT (abscesses; unsuccessful), | LR after LT is a safe and graft-saving procedure, especially in patients who are potentially eligible for ReLT. |
| Patient | Sex | Age at Resection [Years] | Indication for LT | Indication for Liver Resection | Type of Resection | Months after LT | MELD at Resection | Retransplantation Possible | Clavien/ Dindo | Immunosuppressive Regimen | Comorbidities | Follow Up (after Resection) | Status | Cause of Death |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. 1 | m | 64 | Alcoholic cirrhosis | HCC | Segmentectomy (IV, V, VIII) | 194 | 21 | yes | II | Tacrolimus, MMF | Coronary heart disease; ESRD; HT; COPD; DM II | 7 mo | Death | HCC |
| No. 2 | m | 58 | HCC | HCC | Left hemihepatectomy | 14 | - | no | IV | Tacrolimus | HT; DM II | 6 mo | Death | HCC Recurrence |
| No. 3 | m | 29 | AIH | Localized biliary stricture | Left hemihepatectomy & extrahepatic bile duct resection | 159 | 14 | yes | III | Tacrolimus, Prednisolone | - | 52 mo | Alive | |
| No. 4 | m | 52 | HCC | Localized biliary stricture | Atypical segmentectomy (V, VIII) | 13 | 7 | yes | III | Tacrolimus | DM II; COPD | 41 mo | Death | Sepsis |
| No. 5 | f | 58 | HCV Cirrhosis | HCC | Segmentectomy (IV) ;(Segmentectomy (II), 09/2018; left hemihepatectomy, 02/2019) | 79 | 6 | yes | - | Tacrolimus, Everolimus | Chronic Hepatitis C | 30 mo | Alive | |
| No. 6 | f | 66 | PBC | Localized biliary stricture | Left hemihepa tectomy & segmentectomy (I), extrahepatic bile duct resection | 130 | 6 | yes | II | Tacrolimus | - | 49 mo | Alive | |
| No. 7 | m | 64 | Alcoholic cirrhosis | Liver abscess | Right hemihepatectomy and segmentectomy (I) | 271 | 15 | yes | V | Tacrolimus, MMF | Coronary heart disease; Depression; DM II; HT; COPD | 2 d | Death | Graft Dysfunction |
| No. 8 | m | 52 | PSC | PSC | Left hemihepatectomy | 60 | 21 | yes | III | Tacrolimus | Coronary heart disease; Dilatative cardiomyopathy; Tricuspid and mitral insufficiency; Sjögren syndrome | 20 mo | Death | Cerebrovascular accident |
| No. 9 | m | 65 | HCC | Localized biliary stricture | Left hemihepatectomy | 82 | 32 | yes | IV | Tacrolimus, MMF | - | 67 mo | Alive | |
| No. 10 | f | 43 | Cryptogenic cirrhosis | PTLD | Right hemihepatectomy | 166 | 8 | no | - | Tacrolimus | - | 84 mo | Alive | |
| No. 11 | f | 64 | HCC | Liver abscesses | Left hemihepatectomy | 348 | 8 | no | V | Azathioprine, Prednisolone | Paralytic ileus; Sepsis; Scoliosis; Osteogenesis imperfecta; Aneurysms A. phrenica dextra and A. hepatis communis | 39 d | Death | Sepsis |
| No. 12 | m | 60 | HCC | Suspected HCC; (HCC 03/2001) | Atypical segmentectomy (V, VI); (Segmentectomy (II, III), 03/2001) | 111 | - | yes | - | Sirolimus, | Chronic Hepatitis B | 158 mo | Alive | |
| No. 13 | m | 69 | HCC | HCC | Segmentectomy (II, III) | 46 | - | no | V | Tacrolimus | Paroxysmal atrial fibrillation | 46 d | Death | Hemorrhagic shock after hepatic tumor rupture |
| No. 14 | m | 65 | HBV cirrhosis | HCC | Segmentectomy (VI) | 215 | - | no | - | MMF | Hepatitis B reinfection after LT; ESRD; HT; COPD; Coronray heart disease | 19 months | Death | HCC |
| LR after LT | LR after LT (ReLT Possible) | ReLT after LT (All Patients) | vs. LR | ReLT after LT (Late ReLT) | vs. LR | |
|---|---|---|---|---|---|---|
| Patients, total * | 14 | 9 | 175 | 44 | ||
| Gender [male/female] * | 10/4 | 7/2 | 96/79 | 25/19 | ||
| Age [years] ** | 57.8 (±10.9) | 56.67 (±11.65) | 49.0 (±10.7) | p = 0.003 | 47.55 (±11.76) | p = 0.003 |
| Hospital Stay [days] *** | 25 (8.75–49) | 17 (7.5–52) | 44 (25–75) | p = 0.017 | 40 (24–68.25) | p = 0.034 |
| ICU Stay [days] *** | 2 (1–8) | 2 (1–5) | 19 (8–49) | p < 0.001 | 16 (8–29.75) | p < 0.001 |
| Indication for LT * | Indication for ReLT * | |||||
| HCC | 6 (42.9%) | 3 (33.3%) | Primary non-function | 41 (25.4%) | 0 (0.0%) | |
| Cirrhosis (alcohol/nutritive/viral) | 4 (28.6%) | 3 (33.3%) | Hepatic artery thrombosis | 37 (21.1%) | 5 (11.4%) | |
| Cryptogenic Cirrhosis/AIH | 2 (14.3%) | 1 (11.1%) | ITBL | 28 (16.0%) | 15 (34.1%) | |
| PBC/PSC | 2 (14.3%) | 2 (22.2%) | Recurrent disease after LT | 20 (11.4%) | 14 (31.8%) | |
| Rejection | 14 (8.0%) | 0 (0.0%) | ||||
| Others, not specified | 35 (20.0%) | 10 (22.7%) | ||||
| Indication for Resection * | ||||||
| HCC | 5 (35.7%) | 2 (22.2%) | ||||
| Biliary tree pathologies | 5 (35.7%) | 5 (55.6) | ||||
| Abscesses and bilioma | 2 (14.3%) | 1 (11.1%) | ||||
| PTLD | 1 (7.1%) | - | ||||
| Benign tumor | 1 (7.1%) | 1 (11.1%) | ||||
| Days after Liver Transplantation *** | 3682.5 (1725–6073.5) | 3401.0 (2116.5–5383.5) | 19.5 (6–2215.75) | p < 0.001 | 3523.5 (1737–5015.5) | p = 0.778 |
| MELD at time of resection/retransplantation *** | 11 (6.75–21) | 14.5 (6.25–21) | 31 (21–36) | p < 0.001 | 32 (17.5–37) | p = 0.001 |
| Survival | ||||||
| three-year Survival | 50.0% | 66.7% | 55.4% | p = 0.913 (vs. LR ReLT possible: p = 0.448) | 59.1% | p = 0.733 (vs. LR ReLT possible: p = 0.598) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pohl, J.M.O.; Raschzok, N.; Eurich, D.; Pflüger, M.; Wiering, L.; Daneshgar, A.; Dziodzio, T.; Jara, M.; Globke, B.; Sauer, I.M.; et al. Outcomes of Liver Resections after Liver Transplantation at a High-Volume Hepatobiliary Center. J. Clin. Med. 2020, 9, 3685. https://doi.org/10.3390/jcm9113685
Pohl JMO, Raschzok N, Eurich D, Pflüger M, Wiering L, Daneshgar A, Dziodzio T, Jara M, Globke B, Sauer IM, et al. Outcomes of Liver Resections after Liver Transplantation at a High-Volume Hepatobiliary Center. Journal of Clinical Medicine. 2020; 9(11):3685. https://doi.org/10.3390/jcm9113685
Chicago/Turabian StylePohl, Julian M. O., Nathanael Raschzok, Dennis Eurich, Michael Pflüger, Leke Wiering, Assal Daneshgar, Tomasz Dziodzio, Maximilian Jara, Brigitta Globke, Igor M. Sauer, and et al. 2020. "Outcomes of Liver Resections after Liver Transplantation at a High-Volume Hepatobiliary Center" Journal of Clinical Medicine 9, no. 11: 3685. https://doi.org/10.3390/jcm9113685