1. Introduction
Anorexia nervosa (AN) is an eating disorder defined by undernutrition, i.e., body mass index (BMI) <18.5kg/m² and intense fear of gaining weight [
1], and is associated with a decrease of fat mass (FM) and fat-free mass (FFM) [
2]. The assessment of body composition plays a key role in evaluating nutritional status in AN because body weight and BMI could be unreliable in cases of edema for example. Several accurate techniques for the assessment of body composition in humans have been developed [
3].
The reference method is dual-energy X-ray absorptiometry (DXA), which provides a rapid assessment of FM, FFM and bone mineral density [
4], but DXA is expensive and requires specialized radiology equipment and environment, thus it is hardly feasible in routine clinical practice. Inversely, bioelectrical impedance analysis (BIA) is easily used for the assessment of body composition in clinical practice and research studies. Indeed, BIA is a non-invasive, simple, low-cost device that estimates total body water through the body’s resistance to a small alternating current [
5]. Several BIA devices are available and use manufacturers’ predictive equations involving the body’s resistance to current flow, and other variables such as body weight, height and age. BIA equations developed in a specific population are only generalizable to similar populations, so caution is needed when applying them to a different population, in order to avoid imprecise results and wrong interpretation.
Comparison of body composition assessment by DXA and BIA in AN patients has been reported in some studies [
6,
7,
8,
9] showing inconsistent results. We previously reported in malnourished patients that BIA underestimated FFM and overestimated FM when using the manufacturer’s BIA equation [
10]. Interestingly, higher differences were observed for lower BMIs. The lack of a disease-specific equation developed for the estimation of body composition in severely malnourished patients may explain this result.
Furthermore, strong evidence shows that undernutrition associated with loss of muscle mass negatively impacts clinical outcomes [
11] and the preservation or improvement of muscle mass represents a challenge not only in AN but also in chronic diseases. Reduced muscle mass is a phenotypic criterion for malnutrition in GLIM (Global Leadership Initiative on Malnutrition) criteria [
12] and in the recommendations from the European Working Group on Sarcopenia in Older People [
13]. However, to our knowledge, no study has evaluated the validity of equations developed to estimate muscle mass or appendicular lean mass (ALM) in anorectic patients.
In this context, we aimed to evaluate the validity of BIA equations developed either for FFM or for muscle mass in a large sample of severe patients with AN (BMI <16 kg/m2) by using DXA as reference.
4. Discussion
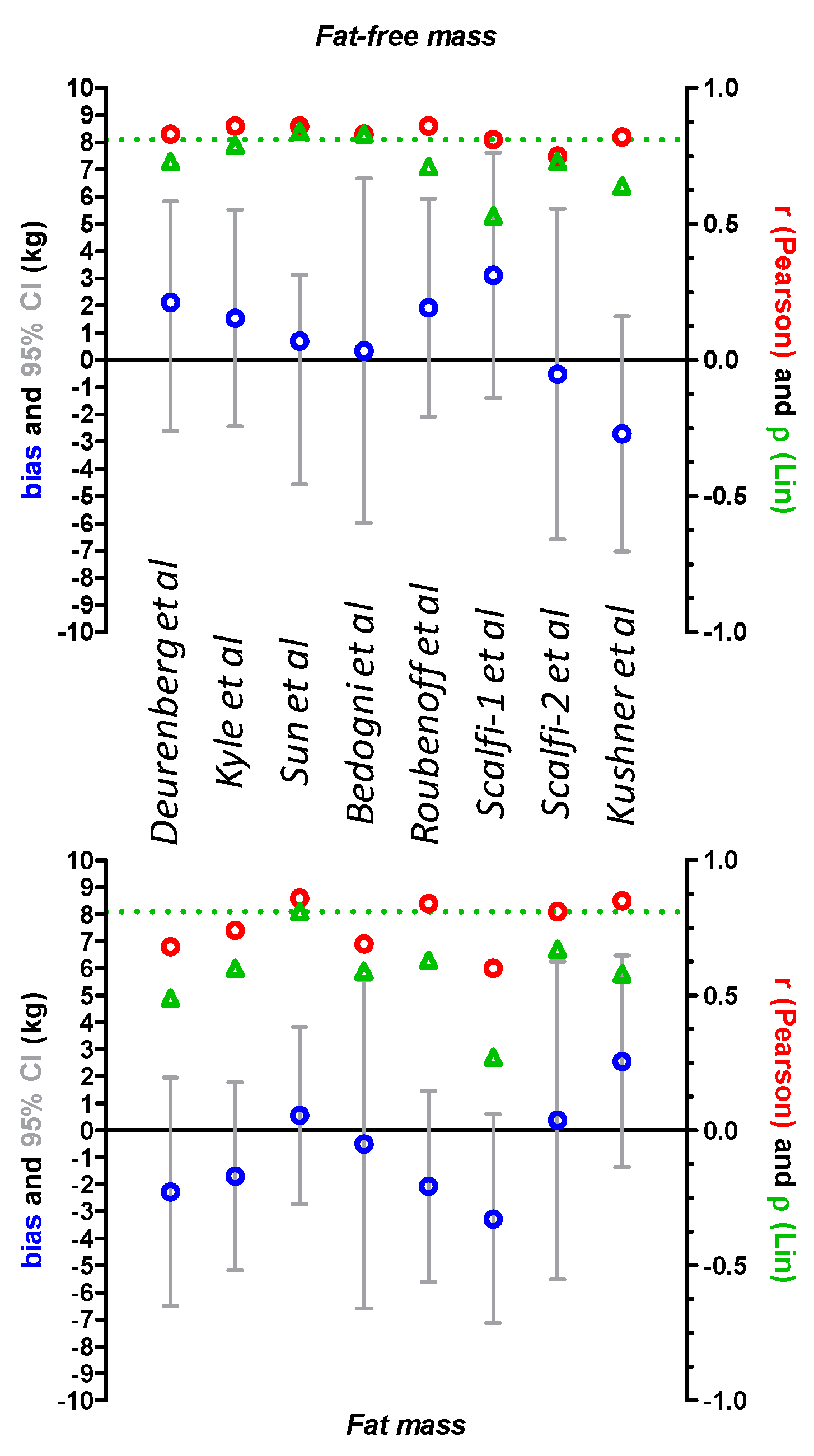
In this study, we evaluated the validity of several BIA equations developed for FFM and muscle mass, in 115 severely malnourished patients with AN, by using DXA as reference. Regarding FM and FFM, the best results were obtained with the Sun equation reporting low bias (0.548 and 0.706 kg respectively), acceptable accuracy for FFM (66.9%), but poor accuracy for FM (13.9%). However, 95% CIs were high for all equations, highlighting the lack of a disease-specific equation developed for the estimation of body composition in AN patients. Previously, Birmingham et al. reported the inability of BIA to detect changes in body composition due to altered hydration, compared to skinfold measurements, in AN patients [
9]. Skinfold measurements and DXA were similar in performance for the estimation of percentage of body fat in 80 AN patients [
8]. Bonaccorsi et al. compared BIA (BIA software and Deurenberg equations) to DXA in 30 young girls (11 to 19 years old) with AN [
6]. They found a high correlation between FFM values estimated with the two methods (BIA software vs. DXA r = 0.917,
p < 0.001; Deurenberg equation vs. DXA r = 0.931,
p < 0.001). However, the limits of agreement were high for FFM (±3.34 kg for the BIA software and ±2.96 kg for the Deurenberg equation) and FM (±4.60 kg for the BIA software and ±3.82 kg for the Deurenberg equation). In our study, the Deurenberg equation also provided high 95% CI. Mattar et al. reported that the Deurenberg equation gave the best estimates of FFM and FM, compared to DXA, in 50 AN patients (BMI = 14.3 ± 1.49 kg/m², age = 19.98 ± 5.68 years), while the Sun equation gave the broadest differences for FM and FFM [
7]. Recently, Marra et al. observed in 82 AN patients that the five tested predictive BIA equations exhibited very low accuracy at population and individual levels, compared to DXA, with a percentage of accurate predictions varying from 12.2% to 35.4% with the Kyle and Sun equations respectively [
34]. Differences in the BIA device used could explain the inconsistencies observed, as well as the characteristics of studied populations. In our study, AN patients had substantially lower BMI (BMI = 14.6 ± 1.2 kg/m² vs. 15.7 ± 1.7 kg/m²), higher FM (11.0 ± 5.6% vs. 9.8 ± 5.0%), and were older (32.3 ± 14.5 years vs. 20.5 ± 3.7 years). Other physiological (e.g., hydration) and anthropometric (e.g., segment lengths, circumferences and volumes) variables may also explain individual discrepancies.
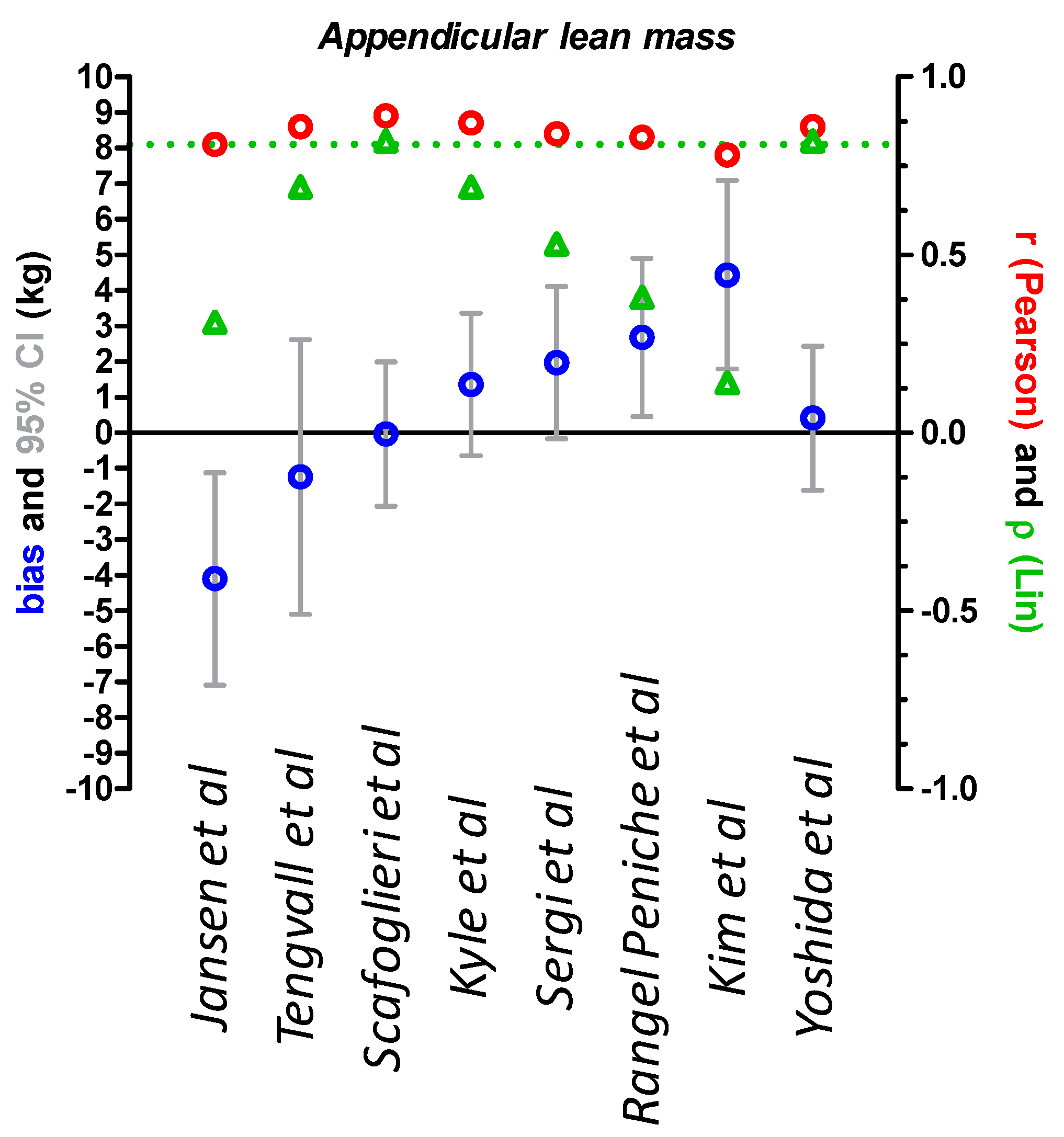
To our knowledge, this is the first study to evaluate BIA equations developed for ALM in AN patients, by using DXA as reference. Scafoglieri and Yoshida equations showed acceptable results at the population level with low bias (−0.03 and 0.41 kg, respectively), and good accuracy (83.5 and 82.6%, respectively) but exhibited high 95% limits of agreement. Recently, Moore et al. reported that ALM estimates were equivalent between DXA and BIA, in 179 normal-weight adults [
35], even if the 95% limits of agreement were high. In addition, the authors used the unknown manufacturer’s equation. The BIA equation tested does not seem to be adapted to severely malnourished patients with AN to evaluate muscle mass at the individual level.
Both FFM and FM compartments are markedly altered during AN. The use of BIA allows the monitoring of compartmental weight gain during refeeding. A recent meta-analysis by Hübel et al. reported 50% less FM and 5 kg less FFM in AN patients compared to the control group [
36]. Recovery was associated with restored FM primarily stored in the trunk as previously described [
37], while long-term lower levels of FFM were observed compared to the control group. These results contradict those of El Ghoch et al. showing normalization of FFM after weight gain in 90 AN patients [
38]. This discrepancy could be explained by the different methods used to measure body composition. El Ghoch et al. used DXA while Hübel included studies with BIA, DXA, dual photon absorptiometry, or magnetic resonance imaging. The restoration of lean body mass is also a key determinant of outcome and quality of life in chronic diseases. Routine investigation of muscle mass is needed in AN patients, particularly to evaluate the impact of new therapeutic tools such as adapted physical activity that has been reported to be associated with increased muscle mass, and to avoid excessive gain of abdominal FM during refeeding [
39]. Moreover, AN is an eating disorder associated with body image disturbance and body shape concerns, therefore an inadequate gain of FM can be a major risk factor for relapse, while a gain of muscle mass may enhance a patient’s compliance, therapeutic outcome and long-term recovery. Accurate body composition monitoring should be routinely implemented in the standard care of AN patients during refeeding.
Our study has some limitations. For muscle mass analyses, we evaluated all the equations together although ALM and skeletal muscle mass are not the same. ALM is the sum of the lean soft tissue of the four limbs, while skeletal muscle mass includes ALM, trunk and head skeletal mass. Thus, as discussed before, our results are not comparable with those of other studies using different devices (BIA, DXA) and population characteristics (age, BMI, etc.).

 ,
, 


{kind=link}
{kind=link}