Pilot Study on the Role of Circulating miRNAs for the Improvement of the Predictive Ability of the 2MACE Score in Patients with Atrial Fibrillation

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Assessment of the 2MACE Score
2.2. Blood Samples Collection and miRNome Analysis
2.3. Follow-Up and Endpoints
2.4. Statistical Analysis
3. Results
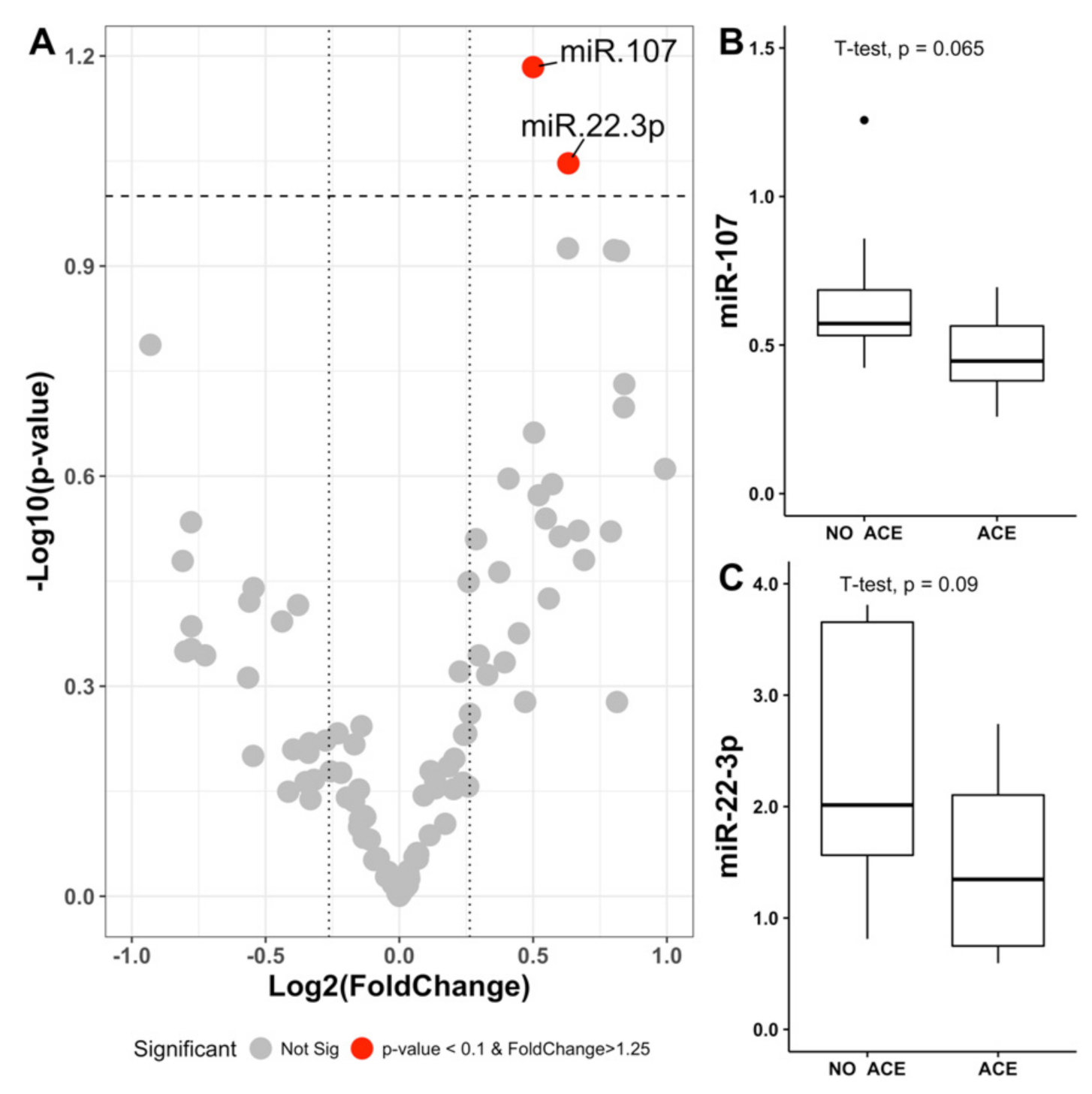
3.1. Pilot Study
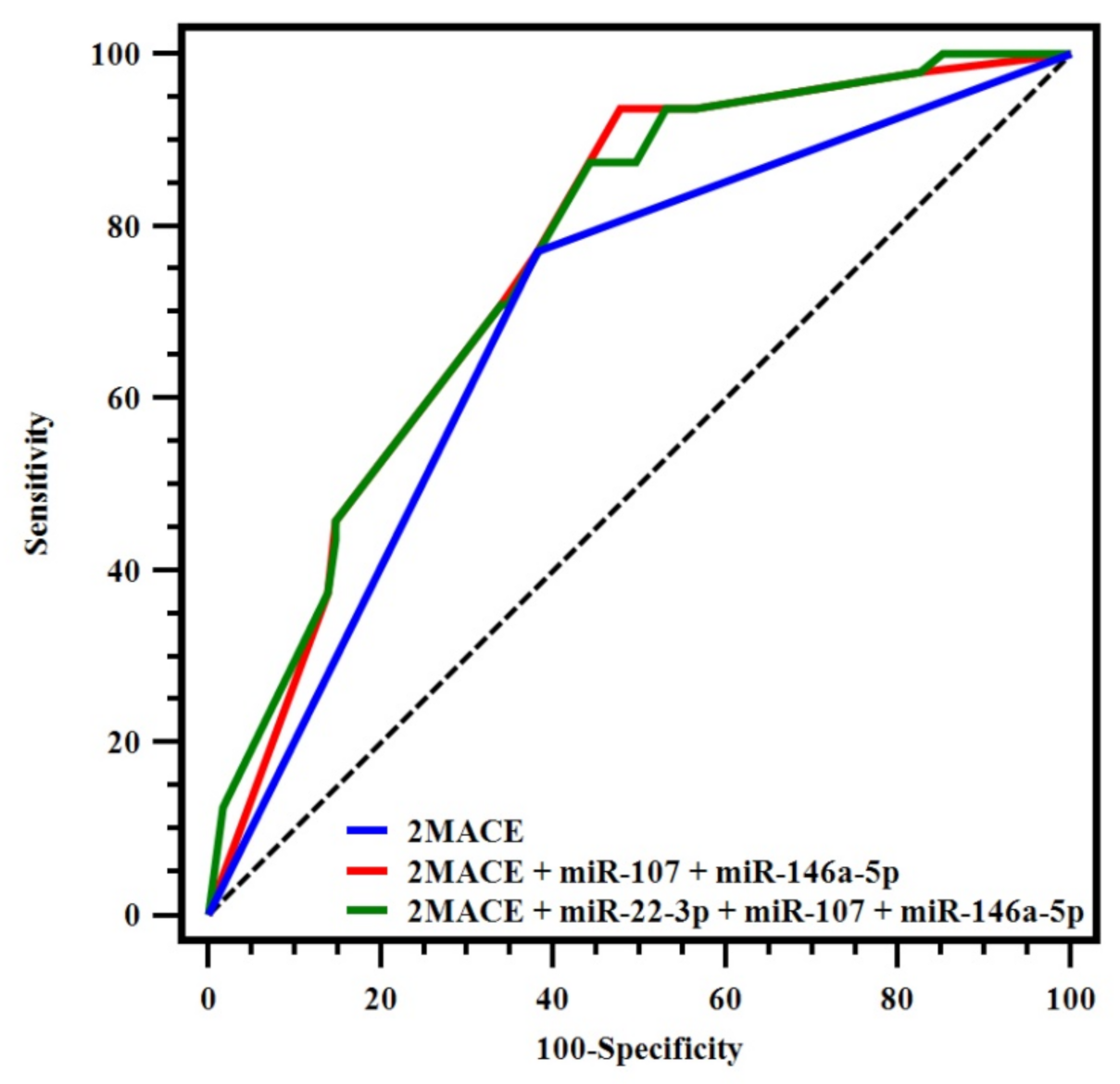
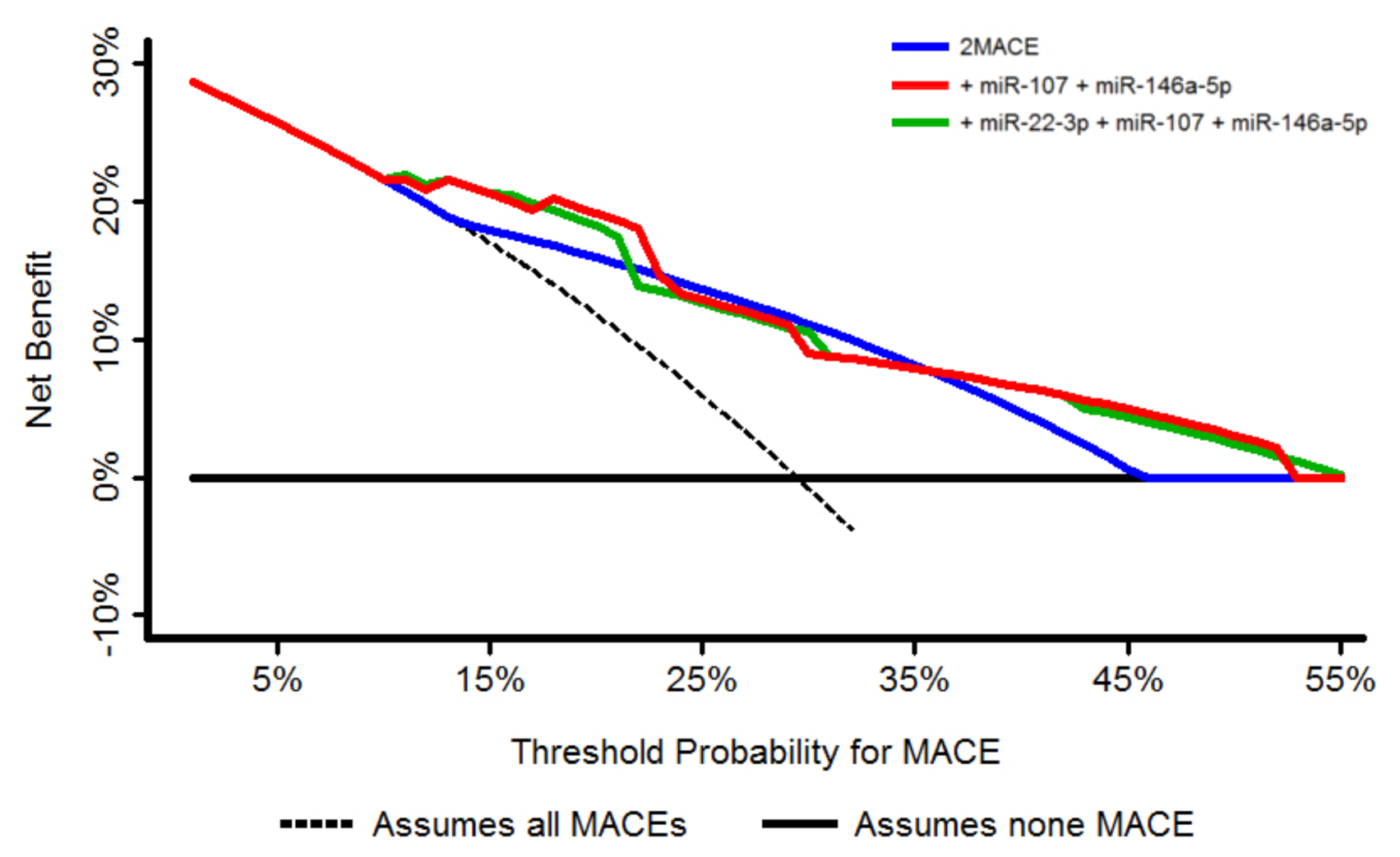
3.2. Validation Study
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lip, G.; Freedman, B.; de Caterina, R.; Potpara, T.S. Stroke prevention in atrial fibrillation: Past, present and future. Comparing the guidelines and practical decision-making. Thromb. Haemost. 2017, 117, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Lip, G.Y.H. The prothrombotic state in atrial fibrillation: Pathophysiological and management implications. Cardiovasc. Res. 2019, 115, 31–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Violi, F.; Soliman, E.Z.; Pignatelli, P.; Pastori, D. Atrial fibrillation and myocardial infarction: A systematic review and appraisal of pathophysiologic mechanisms. J. Am. Heart Assoc. 2016, 5, e003347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastori, D.; Farcomeni, A.; Poli, D.; Antonucci, E.; Angelico, F.; Del Ben, M.; Cangemi, R.; Tanzilli, G.; Lip, G.Y.; Pignatelli, P.; et al. Cardiovascular risk stratification in patients with non-valvular atrial fibrillation: The 2MACE score. Intern. Emerg. Med. 2016, 11, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Polovina, M.; Đikić, D.; Vlajković, A.; Vilotijević, M.; Milinković, I.; Ašanin, M.; Ostojić, M.; Coats, A.J.S.; Seferović, P.M. Adverse cardiovascular outcomes in atrial fibrillation: Validation of the new 2MACE risk score. Int. J. Cardiol. 2017, 249, 191–197. [Google Scholar] [CrossRef]
- Rivera-Caravaca, J.M.; Marín, F.; Esteve-Pastor, M.A.; Raña-Míguez, P.; Anguita, M.; Muñiz, J.; Cequier, Á.; Bertomeu-Martínez, V.; Valdés, M.; Vicente, V.; et al. Usefulness of the 2MACE score to predicts adverse cardiovascular events in patients with atrial fibrillation. Am. J. Cardiol. 2017, 120, 2176–2181. [Google Scholar] [CrossRef]
- Halushka, P.V.; Goodwin, A.J.; Halushka, M.K. Opportunities for microRNAs in the crowded field of cardiovascular biomarkers. Annu. Rev. Pathol. 2019, 14, 211–238. [Google Scholar] [CrossRef]
- Viereck, J.; Thum, T. Circulating Noncoding RNAs as Biomarkers of Cardiovascular Disease and Injury. Circ. Res. 2017, 120, 381–399. [Google Scholar] [CrossRef]
- Vrijens, K.; Bollati, V.; Nawrot, T.S. MicroRNAs as potential signatures of environmental exposure or effect: A systematic review. Environ. Health Perspect. 2015, 123, 399–411. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakob, P.; Kacprowski, T.; Briand-Schumacher, S.; Heg, D.; Klingenberg, R.; Stähli, B.E.; Jaguszewski, M.; Rodondi, N.; Nanchen, D.; Räber, L.; et al. Profiling and validation of circulating microRNAs for cardiovascular events in patients presenting with ST-segment elevation myocardial infarction. Eur. Heart J. 2017, 38, 511–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzacasa, B.; Morini, E.; Mango, R.; Vancheri, C.; Budassi, S.; Massaro, G.; Maletta, S.; Macrini, M.; D’Annibale, S.; Romeo, F.; et al. MiR-423 is differentially expressed in patients with stable and unstable coronary artery disease: A pilot study. PLoS ONE 2019, 14, e0216363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barraclough, J.Y.; Joan, M.; Joglekar, M.V.; Hardikar, A.A.; Patel, S. MicroRNAs as prognostic markers in acute coronary syndrome patients—A systematic review. Cells 2019, 8, 1572. [Google Scholar] [CrossRef] [Green Version]
- Manna, I.; Iaccino, E.; Dattilo, V.; Barone, S.; Vecchio, E.; Mimmi, S.; Filippelli, E.; Demonte, G.; Polidoro, S.; Granata, A.; et al. Exosome-associated miRNA profile as a prognostic tool for therapy response monitoring in multiple sclerosis patients. FASEB J. 2018, 32, 4241–4246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Pencina, M.J.; D’Agostino, R.B., Sr.; D’Agostino, R.B., Jr.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2008, 27, 157–172. [Google Scholar] [CrossRef]
- Vickers, A.J.; Elkin, E.B. Decision curve analysis: A novel method for evaluating prediction models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Arroyo, A.B.; de Los Reyes-García, A.M.; Rivera-Caravaca, J.M.; Valledor, P.; García-Barberá, N.; Roldán, V.; Vicente, V.; Martínez, C.; González-Conejero, R. MiR-146a regulates neutrophil extracellular trap formation that predicts adverse cardiovascular events in patients with atrial fibrillation. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 892–902. [Google Scholar] [CrossRef] [Green Version]
- Roldán, V.; Arroyo, A.B.; Salloum-Asfar, S.; Manzano-Fernández, S.; García-Barberá, N.; Marín, F.; Vicente, V.; González-Conejero, R.; Martínez, C. Prognostic role of MIR146A polymorphisms for cardiovascular events in atrial fibrillation. Thromb. Haemost. 2014, 112, 781–788. [Google Scholar] [CrossRef]
- Komal, S.; Yin, J.J.; Wang, S.H.; Huang, C.Z.; Tao, H.L.; Dong, J.Z.; Han, S.N.; Zhang, L.R. MicroRNAs: Emerging biomarkers for atrial fibrillation. J. Cardiol. 2019, 74, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Franco, D.; Aranega, A.; Dominguez, J.N. Non-coding RNAs and atrial fibrillation. Adv. Exp. Med. Biol. 2020, 1229, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Guo, C.; Zhang, W.; Che, W.; Zhang, J.; Zhuang, S.; Wang, Y.; Zhang, Y.; Liu, B. The integrative regulatory network of circRNA, microRNA, and mRNA in Atrial Fibrillation. Front. Genet. 2019, 10, 526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briasoulis, A.; Sharma, S.; Telila, T.; Mallikethi-Reddy, S.; Papageorgiou, N.; Oikonomou, E.; Tousoulis, D. MicroRNAs in Atrial Fibrillation. Curr. Med. Chem. 2019, 26, 855–863. [Google Scholar] [CrossRef]
- da Silva, A.M.; de Araújo, J.N.; de Freitas, R.C.; Silbiger, V.N. Circulating MicroRNAs as potential biomarkers of atrial fibrillation. BioMed. Res. Int. 2017, 2017, 7804763. [Google Scholar] [CrossRef]
- Kapodistrias, N.; Theocharopoulou, G.; Vlamos, P. A hypothesis of circulating MicroRNAs’ implication in high incidence of atrial fibrillation and other electrocardiographic abnormalities in cancer patients. Adv. Exp. Med. Biol. 2020, 1196, 1–9. [Google Scholar] [CrossRef]
- Zhang, P.P.; Sun, J.; Li, W. Genome-wide profiling reveals atrial fibrillation-related circular RNAs in atrial appendages. Gene 2020, 728, 144286. [Google Scholar] [CrossRef]
- Xu, X.; Zhao, Z.; Li, G. The therapeutic potential of MicroRNAs in Atrial Fibrillation. Mediat. Inflamm. 2020, 2020, 3053520. [Google Scholar] [CrossRef]
- Lozano-Velasco, E.; Garcia-Padilla, C.; Aránega, A.E.; Franco, D. Genetics of Atrial Fibrilation: In search of novel therapeutic targets. Cardiovasc. Hematol. Disord. Drug Targets 2019, 19, 183–194. [Google Scholar] [CrossRef]
- Huang, Z.P.; Wang, D.Z. miR-22 in cardiac remodeling and disease. Trends Cardiovasc. Med. 2014, 24, 267–272. [Google Scholar] [CrossRef] [Green Version]
- Kiyosawa, N.; Watanabe, K.; Morishima, Y.; Yamashita, T.; Yagi, N.; Arita, T.; Otsuka, T.; Suzuki, S. Exploratory analysis of circulating miRNA signatures in Atrial Fibrillation patients determining potential biomarkers to support decision-making in anticoagulation and catheter ablation. Int. J. Mol. Sci. 2020, 21, 2444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goren, Y.; Kushnir, M.; Zafrir, B.; Tabak, S.; Lewis, B.S.; Amir, O. Serum levels of microRNAs in patients with heart failure. Eur. J. Heart Fail. 2012, 14, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.P.; Chen, J.; Seok, H.Y.; Zhang, Z.; Kataoka, M.; Hu, X.; Wang, D.Z. MicroRNA-22 regulates cardiac hypertrophy and remodeling in response to stress. Circ. Res. 2013, 112, 1234–1243. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.D.; Song, X.W.; Li, Q.; Wang, G.K.; Jing, Q.; Qin, Y.W. Attenuation of microRNA-22 derepressed PTEN to effectively protect rat cardiomyocytes from hypertrophy. J. Cell. Physiol. 2012, 227, 1391–1398. [Google Scholar] [CrossRef] [PubMed]
- Kiliszek, M.; Maciak, K.; Maciejak, A.; Krzyżanowski, K.; Wierzbowski, R.; Gora, M.; Burzynska, B.; Segiet, A.; Skrobowski, A. Serum microRNA in patients undergoing atrial fibrillation ablation. Sci. Rep. 2020, 10, 4424. [Google Scholar] [CrossRef]
- Li, Y.; Tan, W.; Ye, F.; Wen, S.; Hu, R.; Cai, X.; Wang, K.; Wang, Z. Inflammation as a risk factor for stroke in atrial fibrillation: Data from a microarray data analysis. J. Int. Med Res. 2020, 48. [Google Scholar] [CrossRef]
- Zhang, Y.; Shen, H.; Wang, P.; Min, J.; Yu, Y.; Wang, Q.; Wang, S.; Xi, W.; Nguyen, Q.M.; Xiao, J.; et al. Identification and characterization of circular RNAs in atrial appendage of patients with atrial fibrillation. Exp. Cell Res. 2020, 389, 111821. [Google Scholar] [CrossRef]
- Camelo-Castillo, A.; Rivera-Caravaca, J.M.; Marín, F.; Vicente, V.; Lip, G.Y.H.; Roldán, V. Predicting adverse events beyond stroke and bleeding with the ABC-stroke and ABC-bleeding scores in patients with atrial fibrillation: The murcia AF project. Thromb. Haemost. 2020, 120, 1200–1207. [Google Scholar] [CrossRef]
- Rivera-Caravaca, J.M.; Esteve-Pastor, M.A. Heart failure and cardiac events: Is a consecutive measurement of biomarkers a simple and practical approach? Thromb. Haemost. 2019, 119, 1891–1893. [Google Scholar] [CrossRef] [Green Version]
- Esteve-Pastor, M.A.; Roldán, V.; Rivera-Caravaca, J.M.; Ramírez-Macías, I.; Lip, G.Y.H.; Marín, F. The use of biomarkers in clinical management guidelines: A critical appraisal. Thromb. Haemost. 2019, 119, 1901–1919. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, B. Circular RNA in diseased heart. Cells 2020, 9, 1240. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, A.; Papageorgiou, N.; Falconer, D.; Rehal, O.; Sewart, E.; Zacharia, E.; Toutouzas, K.; Vlachopoulos, C.; Siasos, G.; Tsioufis, C.; et al. Biomarkers associated with stroke risk in Atrial Fibrillation. Curr. Med. Chem. 2019, 26, 803–823. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall N = 166 | Patients Without MACE N = 117 | Patients with MACE N = 49 | p | |
|---|---|---|---|---|
| Demographic | ||||
| Male sex, n (%) | 78 (47.0) | 54 (46.2) | 24 (49.0) | 0.739 |
| Age (years), median (IQR) | 77 (70–81) | 74 (68–79) | 80 (77–84) | <0.001 |
| Comorbidities, n (%) | ||||
| Hypertension | 140 (84.3) | 96 (82.1) | 44 (89.8) | 0.210 |
| Diabetes mellitus | 41 (24.7) | 25 (21.4) | 16 (32.7) | 0.124 |
| Heart failure | 68 (41.0) | 37 (31.6) | 31 (63.3) | 0.001 |
| History of stroke/TIA/thromboembolism | 32 (19.3) | 17 (14.5) | 15 (30.6) | 0.016 |
| Renal impairment | 13 (7.8) | 6 (5.1) | 7 (14.3) | 0.045 |
| Coronary artery disease | 36 (21.7) | 22 (18.8) | 14 (28.6) | 0.163 |
| Hypercholesterolemia | 54 (32.5) | 41 (35.0) | 13 (26.5) | 0.286 |
| Current smoking habit | 26 (15.7) | 12 (10.3) | 14 (28.6) | <0.01 |
| Current alcohol consumption | 3 (1.8) | 3 (2.6) | 0 (0.0) | 0.622 |
| History of previous bleeding | 12 (7.2) | 5 (4.3) | 7 (14.3) | 0.052 |
| Concomitant treatment, n (%) | ||||
| Amiodarone | 13 (7.8) | 10 (8.5) | 3 (6.1) | 0.596 |
| Digoxin | 28 (16.9) | 17 (14.5) | 11 (22.4) | 0.214 |
| Calcium antagonist | 41 (24.7) | 24 (20.5) | 17 (34.7) | 0.053 |
| Beta-blockers | 53 (31.9) | 39 (33.3) | 14 (28.6) | 0.548 |
| Statins | 35 (21.1) | 27 (23.1) | 8 (16.3) | 0.331 |
| Diuretics | 81 (48.8) | 52 (44.4) | 29 (59.2) | 0.083 |
| Antiplatelet therapy | 25 (15.1) | 16 (13.7) | 9 (18.4) | 0.441 |
| ACE inhibitors/ARBs | 80 (48.2) | 51 (43.6) | 29 (59.2) | 0.067 |
| TTR at 6 months of entry, n (%) | 80 (60–100) | 80 (60–100) | 80 (60–83) | 0.250 |
| CHA2DS2-VASc score, median (IQR) | 4 (3–5) | 4 (3–5) | 5 (4–6) | <0.001 |
| HAS-BLED score, median (IQR) | 2 (2–3) | 2 (2–3) | 3 (2–3) | <0.001 |
| HR | 95% CI | p-Value | |
|---|---|---|---|
| miR-22-3p | 1.07 | 1.02–1.14 | 0.013 |
| miR-107 | 3.66 | 1.19–11.24 | 0.023 |
| miR-146a-5p | 0.86 | 0.74–0.99 | 0.042 |
| C-index | 95% CI | Z Score * | p * | IDI | 95% CI | p | NRI | 95% CI | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| 2MACE | 0.694 | 0.617–0.764 | ||||||||
| + miR-107 + miR-146a-5p | 0.759 | 0.686–0.822 | 2.876 | 0.004 | 0.053 | 0.011/0.096 | 0.014 | 0.345 | −0.327/0.518 | 0.736 |
| + miR-107 + miR-146a-5p+ miR-22-3p | 0.762 | 0.689–0.825 | 2.518 | 0.012 | 0.056 | 0.012/0.101 | 0.015 | 0.047 | −0.274/0.519 | 0.627 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera-Caravaca, J.M.; Teruel-Montoya, R.; Roldán, V.; Cifuentes-Riquelme, R.; Crespo-Matas, J.A.; de los Reyes-García, A.M.; Águila, S.; Fernández-Pérez, M.P.; Reguilón-Gallego, L.; Zapata-Martínez, L.; et al. Pilot Study on the Role of Circulating miRNAs for the Improvement of the Predictive Ability of the 2MACE Score in Patients with Atrial Fibrillation. J. Clin. Med. 2020, 9, 3645. https://doi.org/10.3390/jcm9113645
Rivera-Caravaca JM, Teruel-Montoya R, Roldán V, Cifuentes-Riquelme R, Crespo-Matas JA, de los Reyes-García AM, Águila S, Fernández-Pérez MP, Reguilón-Gallego L, Zapata-Martínez L, et al. Pilot Study on the Role of Circulating miRNAs for the Improvement of the Predictive Ability of the 2MACE Score in Patients with Atrial Fibrillation. Journal of Clinical Medicine. 2020; 9(11):3645. https://doi.org/10.3390/jcm9113645
Chicago/Turabian StyleRivera-Caravaca, José Miguel, Raúl Teruel-Montoya, Vanessa Roldán, Rosa Cifuentes-Riquelme, José Antonio Crespo-Matas, Ascensión María de los Reyes-García, Sonia Águila, María Piedad Fernández-Pérez, Laura Reguilón-Gallego, Laura Zapata-Martínez, and et al. 2020. "Pilot Study on the Role of Circulating miRNAs for the Improvement of the Predictive Ability of the 2MACE Score in Patients with Atrial Fibrillation" Journal of Clinical Medicine 9, no. 11: 3645. https://doi.org/10.3390/jcm9113645