Recent Updates and Advances in the Use of Glycated Albumin for the Diagnosis and Monitoring of Diabetes and Renal, Cerebro- and Cardio-Metabolic Diseases

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Search Strategy
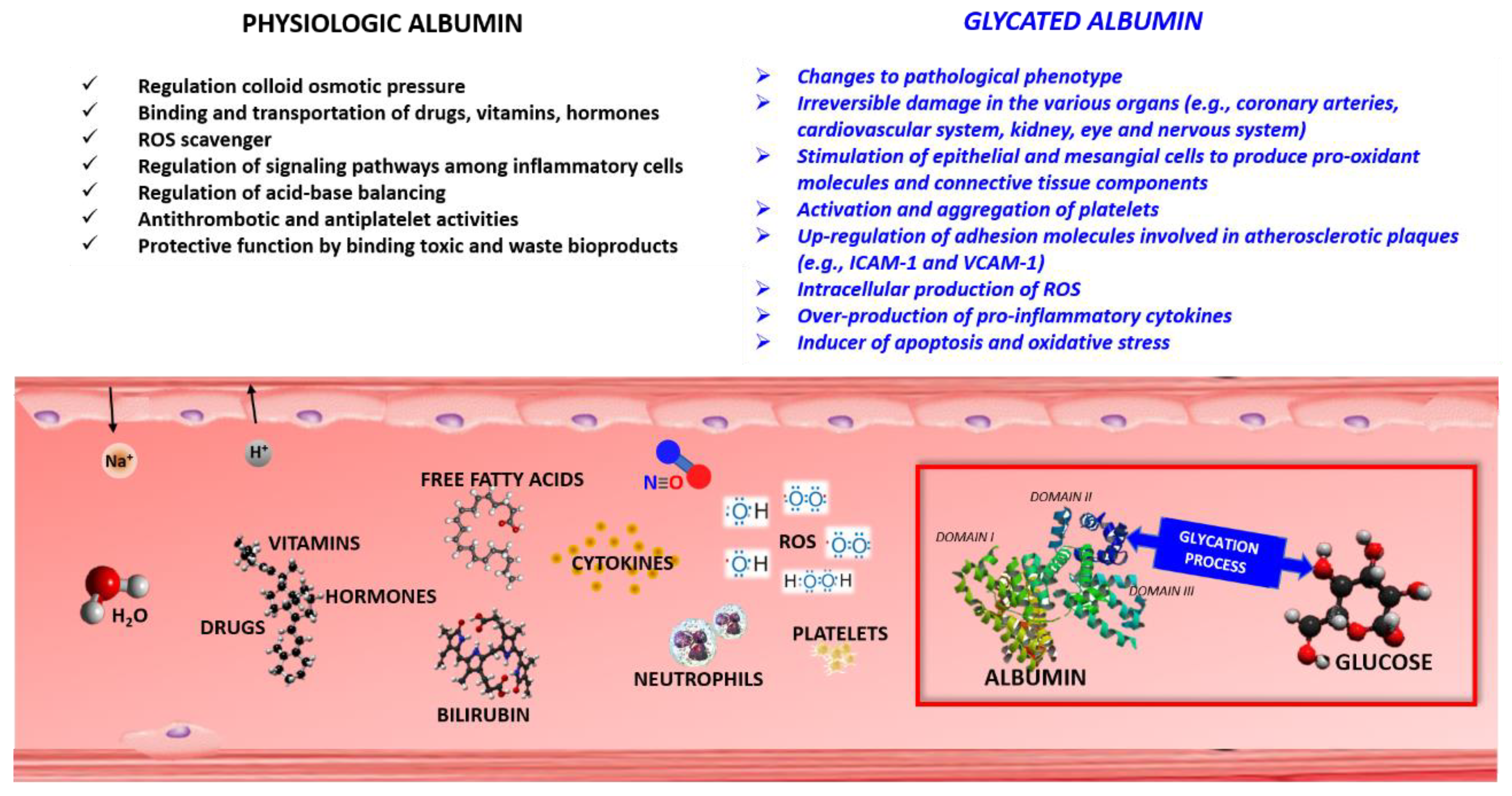
3. Glycated Albumin (GA)
GA Test
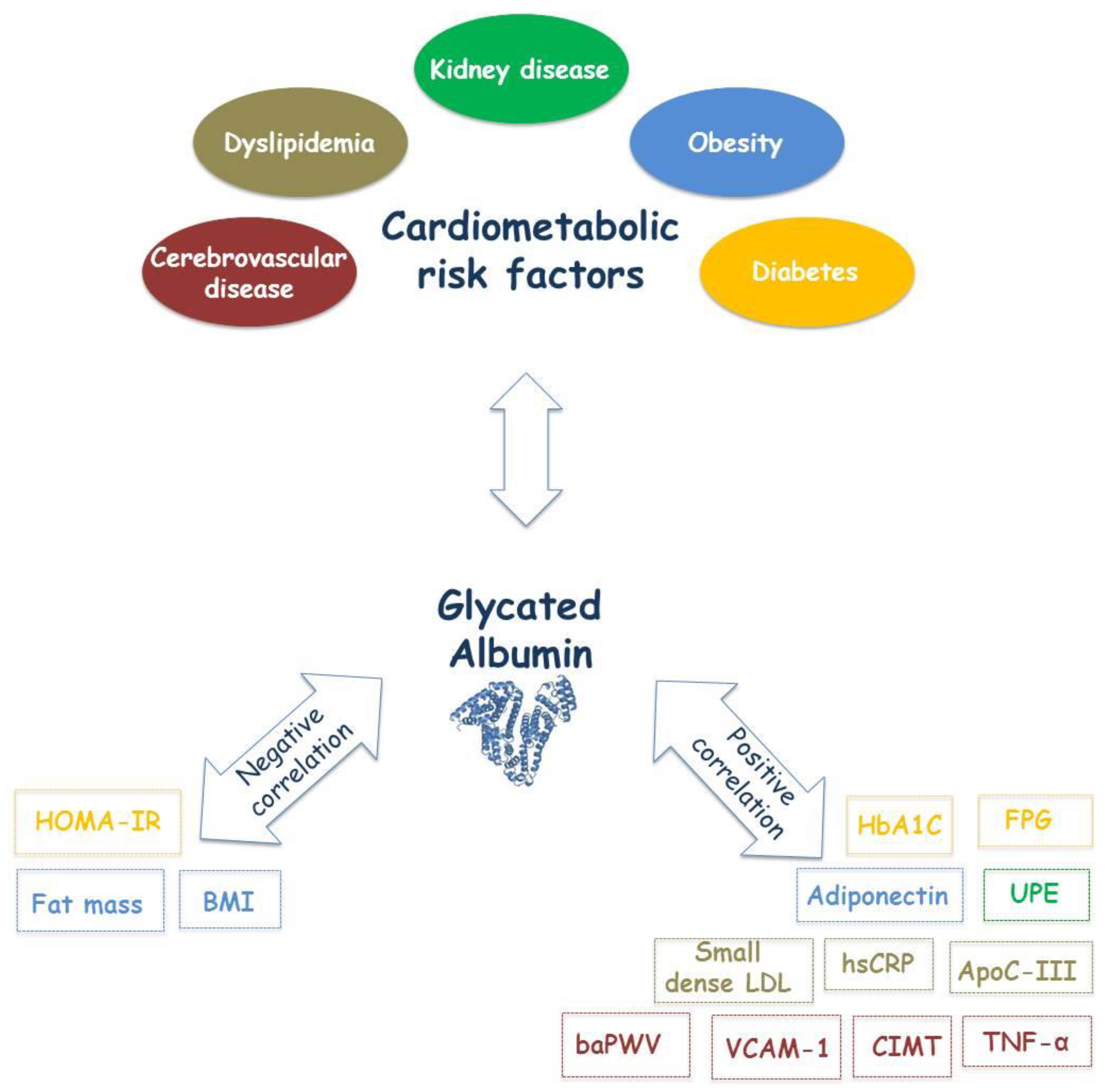
4. GA and Cardio-Metabolic Risk Factors
4.1. GA and Diabetes
4.1.1. GA and Diabetes Diagnosis
4.1.2. GA and Monitoring of Diabetes Treatment
4.2. GA and Dyslipidemia
4.2.1. GA and Dyslipidemia Diagnosis
4.2.2. GA and Monitoring of Dyslipidemia Treatment
4.3. GA and Obesity
4.4. GA and Kidney Diseases
4.4.1. Glycated Albumin and Kidney Disease Diagnosis
4.4.2. Glycated Albumin and Kidney Disease Treatment Monitoring
4.5. GA and Cerebro-Cardiovascular Diseases
4.5.1. GA and Cerebro-Cardiovascular Diagnosis
4.5.2. GA and Cerebro-Cardiovascular Treatment Monitoring
5. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Westerman, K.; Fernandez-Sanles, A.; Patil, P.; Sebastiani, P.; Jacques, P.; Starr, J.M.; Deary, I.J.; Liu, Q.; Liu, S.; Elosua, R.; et al. Epigenomic Assessment of Cardiovascular Disease Risk and Interactions with Traditional Risk Metrics. J. Am. Heart Assoc. 2020, 9, e015299. [Google Scholar] [CrossRef]
- Gulizia, M.M.; Colivicchi, F.; Ricciardi, G.; Giampaoli, S.; Maggioni, A.P.; Averna, M.; Graziani, M.S.; Ceriotti, F.; Mugelli, A.; Rossi, F.; et al. ANMCO/ISS/AMD/ANCE/ARCA/FADOI/GICR-IACPR/SICI-GISE/SIBioC/SIC/SICOA/SID/SIF/SIMEU/SIMG/SIMI/SISA Joint Consensus Document on cholesterol and cardiovascular risk: Diagnostic-therapeutic pathway in Italy. Eur. Heart J. Suppl. J. Eur. Soc. Cardiol. 2017, 19, D3–D54. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Watson, K.E. New insights into understanding cardiometabolic risk. Introduction. Rev. Cardiovasc. Med. 2007, 8 (Suppl. 4), S1–S2. [Google Scholar]
- Bellia, C.; Zaninotto, M.; Cosma, C.; Agnello, L.; Bivona, G.; Marinova, M.; Lo Sasso, B.; Plebani, M.; Ciaccio, M. Clinical usefulness of Glycated Albumin in the diagnosis of diabetes: Results from an Italian study. Clin. Biochem. 2018, 54, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Bellia, C.; Zaninotto, M.; Cosma, C.; Agnello, L.; Lo Sasso, B.; Bivona, G.; Plebani, M.; Ciaccio, M. Definition of the upper reference limit of glycated albumin in blood donors from Italy. Clin. Chem. Lab. Med. 2017, 56, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Zendjabil, M. Glycated albumin. Clin. Chim. Acta Int. J. Clin. Chem. 2020, 502, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.C.; Ma, W.Y.; Wei, J.N.; Yu, T.Y.; Lin, M.S.; Shih, S.R.; Hua, C.H.; Liao, Y.J.; Chuang, L.M.; Li, H.Y. Serum Glycated Albumin to Guide the Diagnosis of Diabetes Mellitus. PLoS ONE 2016, 11, e0146780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay-Lombardie, A.; Kamel, S.; Bigot-Corbel, E. Insights on glycated albumin. Ann. Biol. Clin. 2019, 77, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Bellia, C.; Cosma, C.; Lo Sasso, B.; Bivona, G.; Agnello, L.; Zaninotto, M.; Ciaccio, M. Glycated albumin as a glycaemic marker in patients with advanced chronic kidney disease and anaemia: A preliminary report. Scand. J. Clin. Lab. Investig. 2019, 79, 293–297. [Google Scholar] [CrossRef]
- Miyabe, M.; Kurajoh, M.; Mori, K.; Okuno, S.; Okada, S.; Emoto, M.; Tsujimoto, Y.; Inaba, M. Superiority of glycated albumin over glycated haemoglobin as indicator of glycaemic control and predictor of all-cause mortality in patients with type 2 diabetes mellitus receiving peritoneal dialysis. Ann. Clin. Biochem. 2019, 56, 684–691. [Google Scholar] [CrossRef]
- Chume, F.C.; Kieling, M.H.; Correa Freitas, P.A.; Cavagnolli, G.; Camargo, J.L. Glycated albumin as a diagnostic tool in diabetes: An alternative or an additional test? PLoS ONE 2019, 14, e0227065. [Google Scholar] [CrossRef] [PubMed]
- Renz, P.B.; Chume, F.C.; Timm, J.R.T.; Pimentel, A.L.; Camargo, J.L. Diagnostic accuracy of glycated hemoglobin for gestational diabetes mellitus: A systematic review and meta-analysis. Clin. Chem. Lab. Med. 2019, 57, 1435–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suo, M.; Wen, D.; Wang, W.; Zhang, T. Comparative study on hemoglobin A1c, glycated albumin and glycosylated serum protein in aplastic anemia patients with Type 2 diabetes mellitus. Biosci. Rep. 2020, 40. [Google Scholar] [CrossRef]
- Shima, K.; Abe, F.; Chikakiyo, H.; Ito, N. The relative value of glycated albumin, hemoglobin A1c and fructosamine when screening for diabetes mellitus. Diabetes Res. Clin. Pract. 1989, 7, 243–250. [Google Scholar] [CrossRef]
- Mo, Y.; Ma, X.; Li, H.; Ran, X.; Yang, W.; Li, Q.; Peng, Y.; Li, Y.; Gao, X.; Luan, X.; et al. Relationship between glycated albumin and glycated hemoglobin according to glucose tolerance status: A multicenter study. Diabetes Res. Clin. Pract. 2016, 115, 17–23. [Google Scholar] [CrossRef]
- Wright, A.; Burden, A.C.; Paisey, R.B.; Cull, C.A.; Holman, R.R.; U.K. Prospective Diabetes Study Group. Sulfonylurea inadequacy: Efficacy of addition of insulin over 6 years in patients with type 2 diabetes in the U.K. Prospective Diabetes Study (UKPDS 57). Diabetes Care 2002, 25, 330–336. [Google Scholar] [CrossRef] [Green Version]
- Groop, L.; Schalin, C.; Franssila-Kallunki, A.; Widen, E.; Ekstrand, A.; Eriksson, J. Characteristics of non-insulin-dependent diabetic patients with secondary failure to oral antidiabetic therapy. Am. J. Med. 1989, 87, 183–190. [Google Scholar] [CrossRef]
- Patti, A.M.; Giglio, R.V.; Pafili, K.; Rizzo, M.; Papanas, N. Pharmacotherapy for gestational diabetes. Expert Opin. Pharmacother. 2018, 19, 1407–1414. [Google Scholar] [CrossRef]
- Patti, A.M.; Rizvi, A.A.; Giglio, R.V.; Stoian, A.P.; Ligi, D.; Mannello, F. Impact of Glucose-Lowering Medications on Cardiovascular and Metabolic Risk in Type 2 Diabetes. J. Clin. Med. 2020, 9, 912. [Google Scholar] [CrossRef] [Green Version]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Diabetes Prevention Program Research, G. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Schellenberg, E.S.; Dryden, D.M.; Vandermeer, B.; Ha, C.; Korownyk, C. Lifestyle interventions for patients with and at risk for type 2 diabetes: A systematic review and meta-analysis. Ann. Intern. Med. 2013, 159, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Sacks, D.B. A1C versus glucose testing: A comparison. Diabetes Care 2011, 34, 518–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, C.L.; Pyle, L.; Kelsey, M.; Newnes, L.; Zeitler, P.S.; Nadeau, K.J. Screening for type 2 diabetes and prediabetes in obese youth: Evaluating alternate markers of glycemia—1,5-anhydroglucitol, fructosamine, and glycated albumin. Pediatric Diabetes 2016, 17, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Feskens, E.; Brennan, L.; Dussort, P.; Flourakis, M.; Lindner, L.M.E.; Mela, D.; Rabbani, N.; Rathmann, W.; Respondek, F.; Stehouwer, C.; et al. Potential Markers of Dietary Glycemic Exposures for Sustained Dietary Interventions in Populations without Diabetes. Adv. Nutr. 2020. [Google Scholar] [CrossRef]
- Rathore, R.; Sonwane, B.P.; Jagadeeshaprasad, M.G.; Kahar, S.; Santhakumari, B.; Unnikrishnan, A.G.; Kulkarni, M.J. Glycation of glucose sensitive lysine residues K36, K438 and K549 of albumin is associated with prediabetes. J. Proteom. 2019, 208, 103481. [Google Scholar] [CrossRef]
- Welsh, K.J.; Kirkman, M.S.; Sacks, D.B. Role of Glycated Proteins in the Diagnosis and Management of Diabetes: Research Gaps and Future Directions. Diabetes Care 2016, 39, 1299–1306. [Google Scholar] [CrossRef] [Green Version]
- Tramarin, A.; Naldi, M.; Degani, G.; Lupu, L.; Wiegand, P.; Mazzolari, A.; Altomare, A.; Aldini, G.; Popolo, L.; Vistoli, G.; et al. Unveiling the molecular mechanisms underpinning biorecognition of early-glycated human serum albumin and receptor for advanced glycation end products. Anal. Bioanal. Chem. 2020. [Google Scholar] [CrossRef]
- Baraka-Vidot, J.; Guerin-Dubourg, A.; Bourdon, E.; Rondeau, P. Impaired drug-binding capacities of in vitro and in vivo glycated albumin. Biochimie 2012, 94, 1960–1967. [Google Scholar] [CrossRef]
- Baraka-Vidot, J.; Planesse, C.; Meilhac, O.; Militello, V.; van den Elsen, J.; Bourdon, E.; Rondeau, P. Glycation alters ligand binding, enzymatic, and pharmacological properties of human albumin. Biochemistry 2015, 54, 3051–3062. [Google Scholar] [CrossRef]
- Singh, V.P.; Bali, A.; Singh, N.; Jaggi, A.S. Advanced glycation end products and diabetic complications. Korean J. Physiol. Pharmacol. 2014, 18, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Szkudlarek, A.; Wilk, M.; Maciazek-Jurczyk, M. In Vitro Investigations of Acetohexamide Binding to Glycated Serum Albumin in the Presence of Fatty Acid. Molecules 2020, 25, 2340. [Google Scholar] [CrossRef] [PubMed]
- Doweiko, J.P.; Bistrian, B.R. The effect of glycosylated albumin on platelet aggregation. Jpn. J. Parenter. Enter. Nutr. 1994, 18, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Juhan-Vague, I.; Alessi, M.C.; Vague, P. Thrombogenic and fibrinolytic factors and cardiovascular risk in non-insulin-dependent diabetes mellitus. Ann. Med. 1996, 28, 371–380. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of Medical Care in Diabetes-2019 Abridged for Primary Care Providers. Clin. Diabetes Publ. Am. Diabetes Assoc. 2019, 37, 11–34. [Google Scholar] [CrossRef] [Green Version]
- Bergman, M.; Abdul-Ghani, M.; DeFronzo, R.A.; Manco, M.; Sesti, G.; Fiorentino, T.V.; Ceriello, A.; Rhee, M.; Phillips, L.S.; Chung, S.; et al. Review of methods for detecting glycemic disorders. Diabetes Res. Clin. Pract. 2020, 165, 108233. [Google Scholar] [CrossRef]
- Desouza, C.V.; Holcomb, R.G.; Rosenstock, J.; Frias, J.P.; Hsia, S.H.; Klein, E.J.; Zhou, R.; Kohzuma, T.; Fonseca, V.A. Results of a Study Comparing Glycated Albumin to Other Glycemic Indices. J. Clin. Endocrinol. Metab. 2020, 105. [Google Scholar] [CrossRef]
- Choi, H.; Son, S.E.; Hur, W.; Tran, V.K.; Lee, H.B.; Park, Y.; Han, D.K.; Seong, G.H. Electrochemical Immunoassay for Determination of Glycated Albumin using Nanozymes. Sci. Rep. 2020, 10, 9513. [Google Scholar] [CrossRef]
- Kohzuma, T.; Koga, M. Lucica GA-L glycated albumin assay kit: A new diagnostic test for diabetes mellitus. Mol. Diagn. Ther. 2010, 14, 49–51. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, B.; Yang, L.; Lou, J.; Jiang, Y.; Zhang, S. Individualized Correction of the Interference of Hemolysis on Glycated Albumin Determined by the Ketamine Oxidase Method. Lab. Med. 2020, 51, 151–156. [Google Scholar] [CrossRef]
- Ziyadeh, F.N.; Cohen, M.P. Effects of glycated albumin on mesangial cells: Evidence for a role in diabetic nephropathy. Mol. Cell. Biochem. 1993, 125, 19–25. [Google Scholar] [CrossRef]
- Chen, S.; Cohen, M.P.; Lautenslager, G.T.; Shearman, C.W.; Ziyadeh, F.N. Glycated albumin stimulates TGF-beta 1 production and protein kinase C activity in glomerular endothelial cells. Kidney Int. 2001, 59, 673–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Cohen, M.P.; Ziyadeh, F.N. Amadori-glycated albumin in diabetic nephropathy: Pathophysiologic connections. Kidney Int. Suppl. 2000, 77, S40–S44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, M.P.; Chen, S.; Ziyadeh, F.N.; Shea, E.; Hud, E.A.; Lautenslager, G.T.; Shearman, C.W. Evidence linking glycated albumin to altered glomerular nephrin and VEGF expression, proteinuria, and diabetic nephropathy. Kidney Int. 2005, 68, 1554–1561. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, A.M.; Regazzoni, L.; Brioschi, M.; Gianazza, E.; Agostoni, P.; Aldini, G.; Banfi, C. Pro-oxidant and pro-inflammatory effects of glycated albumin on cardiomyocytes. Free Radic. Biol. Med. 2019, 144, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Lu, L.; Zhang, R.Y.; Zhang, Q.; Ding, F.H.; Chen, Q.J.; Shen, W.F. Association of serum glycated albumin, C-reactive protein and ICAM-1 levels with diffuse coronary artery disease in patients with type 2 diabetes mellitus. Clin. Chim. Acta Int. J. Clin. Chem. 2009, 408, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Blache, D.; Bourdon, E.; Salloignon, P.; Lucchi, G.; Ducoroy, P.; Petit, J.M.; Verges, B.; Lagrost, L. Glycated albumin with loss of fatty acid binding capacity contributes to enhanced arachidonate oxygenation and platelet hyperactivity: Relevance in patients with type 2 diabetes. Diabetes 2015, 64, 960–972. [Google Scholar] [CrossRef] [Green Version]
- Kravchenko, I.V.; Furalyov, V.A.; Popov, V.O. Glycated albumin stimulates expression of inflammatory cytokines in muscle cells. Cytokine 2020, 128, 154991. [Google Scholar] [CrossRef]
- Nie, X.; Shen, Y.; Ma, X.; Xu, Y.; Wang, Y.; Zhou, J.; Bao, Y. Associations Between Thyroid Hormones and Glycated Albumin in Euthyroid and Subclinical Hypothyroid Individuals: Results of an Observational Study. Diabetesmetabolic Syndr. Obes. Targets Ther. 2020, 13, 915–923. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Kim, K.J.; Huh, J.H.; Lee, B.W.; Kang, E.S.; Cha, B.S.; Lee, H.C. The ratio of glycated albumin to glycated haemoglobin correlates with insulin secretory function. Clin. Endocrinol. 2012, 77, 679–683. [Google Scholar] [CrossRef]
- Vetter, S.W. Glycated Serum Albumin and AGE Receptors. Adv. Clin. Chem. 2015, 72, 205–275. [Google Scholar] [CrossRef]
- DeFronzo, R.A. Pathogenesis of type 2 diabetes mellitus. Med. Clin. N. Am. 2004, 88, 787–835. [Google Scholar] [CrossRef] [PubMed]
- Florkowski, C. HbA1c as a Diagnostic Test for Diabetes Mellitus—Reviewing the Evidence. Clin. Biochem. Rev. 2013, 34, 75–83. [Google Scholar] [PubMed]
- Danese, E.; Montagnana, M.; Nouvenne, A.; Lippi, G. Advantages and pitfalls of fructosamine and glycated albumin in the diagnosis and treatment of diabetes. J. Diabetes Sci. Technol. 2015, 9, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitas, P.A.C.; Ehlert, L.R.; Camargo, J.L. Glycated albumin: A potential biomarker in diabetes. Arch. Endocrinol. Metab. 2017, 61, 296–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koga, M.; Kasayama, S. Clinical impact of glycated albumin as another glycemic control marker. Endocr. J. 2010, 57, 751–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koga, M.; Murai, J.; Saito, H.; Kasayama, S. Glycated albumin and glycated hemoglobin are influenced differently by endogenous insulin secretion in patients with type 2 diabetes. Diabetes Care 2010, 33, 270–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zemlin, A.E.; Barkhuizen, M.; Kengne, A.P.; Erasmus, R.T.; Matsha, T.E. Performance of glycated albumin for type 2 diabetes and prediabetes diagnosis in a South African population. Clin. Chim. Acta Int. J. Clin. Chem. 2019, 488, 122–128. [Google Scholar] [CrossRef]
- Lee, Y.H.; Lee, B.W.; Chun, S.W.; Cha, B.S.; Lee, H.C. Predictive characteristics of patients achieving glycaemic control with insulin after sulfonylurea failure. Int. J. Clin. Pract. 2011, 65, 1076–1084. [Google Scholar] [CrossRef]
- Takahashi, S.; Uchino, H.; Shimizu, T.; Kanazawa, A.; Tamura, Y.; Sakai, K.; Watada, H.; Hirose, T.; Kawamori, R.; Tanaka, Y. Comparison of glycated albumin (GA) and glycated hemoglobin (HbA1c) in type 2 diabetic patients: Usefulness of GA for evaluation of short-term changes in glycemic control. Endocr. J. 2007, 54, 139–144. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Guerin-Deremaux, L.; Pochat, M.; Wils, D.; Reifer, C.; Miller, L.E. NUTRIOSE dietary fiber supplementation improves insulin resistance and determinants of metabolic syndrome in overweight men: A double-blind, randomized, placebo-controlled study. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2010, 35, 773–782. [Google Scholar] [CrossRef]
- Florez, H.; Mendez, A.; Casanova-Romero, P.; Larreal-Urdaneta, C.; Castillo-Florez, S.; Lee, D.; Goldberg, R. Increased apolipoprotein C-III levels associated with insulin resistance contribute to dyslipidemia in normoglycemic and diabetic subjects from a triethnic population. Atherosclerosis 2006, 188, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.C.; Chen, M.M.; Ooi, E.M.; Watts, G.F. An ABC of apolipoprotein C-III: A clinically useful new cardiovascular risk factor? Int. J. Clin. Pract. 2008, 62, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, W.; Chung, H.S.; Hong, K.S. Diagnostic Utility of Serum Glycated Albumin for Diabetes Mellitus and Its Correlation with Hyperlipidemia. Ann. Lab. Med. 2016, 36, 306–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, P.H.; Davidson, M.H.; Stein, E.A.; Bays, H.E.; McKenney, J.M.; Miller, E.; Cain, V.A.; Blasetto, J.W.; Group, S.S. Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR* Trial). Am. J. Cardiol. 2003, 92, 152–160. [Google Scholar] [CrossRef]
- McKenney, J.M.; Jones, P.H.; Adamczyk, M.A.; Cain, V.A.; Bryzinski, B.S.; Blasetto, J.W.; Group, S.S. Comparison of the efficacy of rosuvastatin versus atorvastatin, simvastatin, and pravastatin in achieving lipid goals: Results from the STELLAR trial. Curr. Med Res. Opin. 2003, 19, 689–698. [Google Scholar] [CrossRef]
- van Himbergen, T.M.; Matthan, N.R.; Resteghini, N.A.; Otokozawa, S.; Ai, M.; Stein, E.A.; Jones, P.H.; Schaefer, E.J. Comparison of the effects of maximal dose atorvastatin and rosuvastatin therapy on cholesterol synthesis and absorption markers. J. Lipid Res. 2009, 50, 730–739. [Google Scholar] [CrossRef] [Green Version]
- Otokozawa, S.; Ai, M.; Van Himbergen, T.; Asztalos, B.F.; Tanaka, A.; Stein, E.A.; Jones, P.H.; Schaefer, E.J. Effects of intensive atorvastatin and rosuvastatin treatment on apolipoprotein B-48 and remnant lipoprotein cholesterol levels. Atherosclerosis 2009, 205, 197–201. [Google Scholar] [CrossRef] [Green Version]
- Banach, M.; Patti, A.M.; Giglio, R.V.; Cicero, A.F.G.; Atanasov, A.G.; Bajraktari, G.; Bruckert, E.; Descamps, O.; Djuric, D.M.; Ezhov, M.; et al. The Role of Nutraceuticals in Statin Intolerant Patients. J. Am. Coll. Cardiol. 2018, 72, 96–118. [Google Scholar] [CrossRef]
- Penson, P.E.; Mancini, G.B.J.; Toth, P.P.; Martin, S.S.; Watts, G.F.; Sahebkar, A.; Mikhailidis, D.P.; Banach, M.; Lipid and Blood Pressure Meta-Analysis Collaboration Group & International Lipid Expert Panel. Introducing the ‘Drucebo’ effect in statin therapy: A systematic review of studies comparing reported rates of statin-associated muscle symptoms, under blinded and open-label conditions. J. Cachexia Sarcopenia Muscle 2018, 9, 1023–1033. [Google Scholar] [CrossRef] [Green Version]
- Sattar, N.; Preiss, D.; Murray, H.M.; Welsh, P.; Buckley, B.M.; de Craen, A.J.; Seshasai, S.R.; McMurray, J.J.; Freeman, D.J.; Jukema, J.W.; et al. Statins and risk of incident diabetes: A collaborative meta-analysis of randomised statin trials. Lancet 2010, 375, 735–742. [Google Scholar] [CrossRef]
- O’Donoghue, M.; Morrow, D.A.; Sabatine, M.S.; Murphy, S.A.; McCabe, C.H.; Cannon, C.P.; Braunwald, E. Lipoprotein-associated phospholipase A2 and its association with cardiovascular outcomes in patients with acute coronary syndromes in the PROVE IT-TIMI 22 (PRavastatin or atorVastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction) trial. Circulation 2006, 113, 1745–1752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khera, A.V.; Demler, O.V.; Adelman, S.J.; Collins, H.L.; Glynn, R.J.; Ridker, P.M.; Rader, D.J.; Mora, S. Cholesterol Efflux Capacity, High-Density Lipoprotein Particle Number, and Incident Cardiovascular Events: An Analysis from the JUPITER Trial (Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin). Circulation 2017, 135, 2494–2504. [Google Scholar] [CrossRef] [PubMed]
- Thongtang, N.; Ai, M.; Otokozawa, S.; Himbergen, T.V.; Asztalos, B.F.; Nakajima, K.; Stein, E.; Jones, P.H.; Schaefer, E.J. Effects of maximal atorvastatin and rosuvastatin treatment on markers of glucose homeostasis and inflammation. Am. J. Cardiol. 2011, 107, 387–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Digenio, A.; Dunbar, R.L.; Alexander, V.J.; Hompesch, M.; Morrow, L.; Lee, R.G.; Graham, M.J.; Hughes, S.G.; Yu, R.; Singleton, W.; et al. Antisense-Mediated Lowering of Plasma Apolipoprotein C-III by Volanesorsen Improves Dyslipidemia and Insulin Sensitivity in Type 2 Diabetes. Diabetes Care 2016, 39, 1408–1415. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Ma, X.; Hao, Y.; Yang, R.; Ni, J.; Xiao, Y.; Tang, J.; Bao, Y.; Jia, W. Serum glycated albumin is inversely influenced by fat mass and visceral adipose tissue in Chinese with normal glucose tolerance. PLoS ONE 2012, 7, e51098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Ma, X.; Shen, Y.; Wang, Y.; Zhou, J.; Bao, Y. Increasing waist circumference is associated with decreased levels of glycated albumin. Clin. Chim. Acta Int. J. Clin. Chem. 2019, 495, 118–122. [Google Scholar] [CrossRef]
- Sumner, A.E.; Duong, M.T.; Bingham, B.A.; Aldana, P.C.; Ricks, M.; Mabundo, L.S.; Tulloch-Reid, M.K.; Chung, S.T.; Sacks, D.B. Glycated Albumin Identifies Prediabetes Not Detected by Hemoglobin A1c: The Africans in America Study. Clin. Chem. 2016, 62, 1524–1532. [Google Scholar] [CrossRef]
- Sumner, A.E.; Duong, M.T.; Aldana, P.C.; Ricks, M.; Tulloch-Reid, M.K.; Lozier, J.N.; Chung, S.T.; Sacks, D.B. A1C Combined with Glycated Albumin Improves Detection of Prediabetes in Africans: The Africans in America Study. Diabetes Care 2016, 39, 271–277. [Google Scholar] [CrossRef] [Green Version]
- Koga, M.; Ishizaka, Y.; Yamakado, M. Does Glycated Albumin Increase with Body Weight Reduction in Obese Non-Diabetic Subjects? Ann. Clin. Lab. Sci. 2019, 49, 529–533. [Google Scholar]
- Koga, M.; Matsumoto, S.; Saito, H.; Kasayama, S. Body mass index negatively influences glycated albumin, but not glycated hemoglobin, in diabetic patients. Endocr. J. 2006, 53, 387–391. [Google Scholar] [CrossRef] [Green Version]
- Koga, M.; Hirata, T.; Kasayama, S.; Ishizaka, Y.; Yamakado, M. Body mass index negatively regulates glycated albumin through insulin secretion in patients with type 2 diabetes mellitus. Clin. Chim. Acta Int. J. Clin. Chem. 2015, 438, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, Y.; Nishimura, R.; Morimoto, A.; Matsudaira, T.; Sano, H.; Tajima, N. Glycated albumin is low in obese, type 2 diabetic patients. Diabetes Res. Clin. Pract. 2007, 78, 51–55. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Mo, Y.; Ma, X.; Ying, L.; Zhu, W.; Wang, Y.; Bao, Y.; Zhou, J. Associations of body mass index with glycated albumin and glycated albumin/glycated hemoglobin A1c ratio in Chinese diabetic and non-diabetic populations. Clin. Chim. Acta Int. J. Clin. Chem. 2018, 484, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.H.; Kim, K.J.; Lee, B.W.; Kim, D.W.; Kang, E.S.; Cha, B.S.; Lee, H.C. The relationship between BMI and glycated albumin to glycated hemoglobin (GA/A1c) ratio according to glucose tolerance status. PLoS ONE 2014, 9, e89478. [Google Scholar] [CrossRef] [PubMed]
- Bullo, M.; Garcia-Lorda, P.; Megias, I.; Salas-Salvado, J. Systemic inflammation, adipose tissue tumor necrosis factor, and leptin expression. Obes. Res. 2003, 11, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef]
- Salas-Salvado, J.; Bullo, M.; Garcia-Lorda, P.; Figueredo, R.; Del Castillo, D.; Bonada, A.; Balanza, R. Subcutaneous adipose tissue cytokine production is not responsible for the restoration of systemic inflammation markers during weight loss. Int. J. Obes. 2006, 30, 1714–1720. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, M.; Abate, N.; Chandalia, M.; Rizvi, A.A.; Giglio, R.V.; Nikolic, D.; Marino Gammazza, A.; Barbagallo, I.; Isenovic, E.R.; Banach, M.; et al. Liraglutide reduces oxidative stress and restores heme oxygenase-1 and ghrelin levels in patients with type 2 diabetes: A prospective pilot study. J. Clin. Endocrinol. Metab. 2015, 100, 603–606. [Google Scholar] [CrossRef] [Green Version]
- Sumida, K.; Kovesdy, C.P. Disease Trajectories Before ESRD: Implications for Clinical Management. Semin. Nephrol. 2017, 37, 132–143. [Google Scholar] [CrossRef]
- Williams, M.E.; Garg, R. Glycemic management in ESRD and earlier stages of CKD. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2014, 63, S22–S38. [Google Scholar] [CrossRef] [Green Version]
- Chujo, K.; Shima, K.; Tada, H.; Oohashi, T.; Minakuchi, J.; Kawashima, S. Indicators for blood glucose control in diabetics with end-stage chronic renal disease: GHb vs. glycated albumin (GA). J. Med. Investig. JMI 2006, 53, 223–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaysen, G.A. Albumin turnover in renal disease. Mineral. Electrolyte Metab. 1998, 24, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.A. Albumin in nephrotic syndrome and oedematous malnutrition. Paediatr. Int. Child Health 2015, 35, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Isshiki, K.; Nishio, T.; Isono, M.; Makiishi, T.; Shikano, T.; Tomita, K.; Nishio, T.; Kanasaki, M.; Maegawa, H.; Uzu, T.; et al. Glycated albumin predicts the risk of mortality in type 2 diabetic patients on hemodialysis: Evaluation of a target level for improving survival. Ther. Apher. Dial. 2014, 18, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Schleicher, E.D.; Olgemoller, B.; Wiedenmann, E.; Gerbitz, K.D. Specific glycation of albumin depends on its half-life. Clin. Chem. 1993, 39, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B.I.; Shenoy, R.N.; Planer, J.A.; Clay, K.D.; Shihabi, Z.K.; Burkart, J.M.; Cardona, C.Y.; Andries, L.; Peacock, T.P.; Sabio, H.; et al. Comparison of glycated albumin and hemoglobin A1c concentrations in diabetic subjects on peritoneal and hemodialysis. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2010, 30, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Biesenbach, G.; Pohanka, E. Dialysis: Glycated albumin or HbA(1c) in dialysis patients with diabetes? Nat. Rev. Nephrol. 2011, 7, 490–492. [Google Scholar] [CrossRef]
- Okada, T.; Nakao, T.; Matsumoto, H.; Nagaoka, Y.; Tomaru, R.; Iwasawa, H.; Wada, T. Influence of proteinuria on glycated albumin values in diabetic patients with chronic kidney disease. Intern. Med. 2011, 50, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Jung, M.; Warren, B.; Grams, M.; Kwong, Y.D.; Shafi, T.; Coresh, J.; Rebholz, C.M.; Selvin, E. Performance of non-traditional hyperglycemia biomarkers by chronic kidney disease status in older adults with diabetes: Results from the Atherosclerosis Risk in Communities Study. J. Diabetes 2018, 10, 276–285. [Google Scholar] [CrossRef]
- Selvin, E.; Rawlings, A.M.; Grams, M.; Klein, R.; Sharrett, A.R.; Steffes, M.; Coresh, J. Fructosamine and glycated albumin for risk stratification and prediction of incident diabetes and microvascular complications: A prospective cohort analysis of the Atherosclerosis Risk in Communities (ARIC) study. Lancet Diabetes Endocrinol. 2014, 2, 279–288. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.Y.; Park, S.K.; Yun, G.Y.; Choi, A.R.; Lee, J.E.; Ha, S.K.; Park, H.C. Glycated Albumin is Independently Associated with Arterial Stiffness in Non-Diabetic Chronic Kidney Disease Patients. Medicine 2016, 95, e3362. [Google Scholar] [CrossRef] [PubMed]
- Raghav, A.; Ahmad, J.; Noor, S.; Alam, K.; Mishra, B.K. Glycated albumin and the risk of chronic kidney disease in subjects with Type 2 Diabetes: A study in North Indian Population. Diabetes Metab. Syndr. 2018, 12, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Raghav, A.; Ahmad, J. Glycated albumin in chronic kidney disease: Pathophysiologic connections. Diabetes Metab. Syndr. 2018, 12, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Hattori, S. Sitagliptin reduces albuminuria in patients with type 2 diabetes. Endocr. J. 2011, 58, 69–73. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, Y.; Yamagata, K.; Nishi, S.; Hirakata, H.; Hanafusa, N.; Saito, C.; Hattori, M.; Itami, N.; Komatsu, Y.; Kawaguchi, Y.; et al. Japanese society for dialysis therapy clinical guideline for “hemodialysis initiation for maintenance hemodialysis”. Ther. Apher. Dial. 2015, 19 (Suppl. 1), 93–107. [Google Scholar] [CrossRef]
- Shah, A.M.; Banerjee, T.; Mukherjee, D. Coronary, peripheral and cerebrovascular disease: A complex relationship. J. Indian Med. Assoc. 2010, 108, 292–294, 296. [Google Scholar] [CrossRef]
- Lu, L.; Pu, L.J.; Xu, X.W.; Zhang, Q.; Zhang, R.Y.; Zhang, J.S.; Hu, J.; Yang, Z.K.; Lu, A.K.; Ding, F.H.; et al. Association of serum levels of glycated albumin, C-reactive protein and tumor necrosis factor-alpha with the severity of coronary artery disease and renal impairment in patients with type 2 diabetes mellitus. Clin. Biochem. 2007, 40, 810–816. [Google Scholar] [CrossRef]
- Pu, L.J.; Lu, L.; Shen, W.F.; Zhang, Q.; Zhang, R.Y.; Zhang, J.S.; Hu, J.; Yang, Z.K.; Ding, F.H.; Chen, Q.J.; et al. Increased serum glycated albumin level is associated with the presence and severity of coronary artery disease in type 2 diabetic patients. Circ. J. Off. J. Jpn. Circ. Soc. 2007, 71, 1067–1073. [Google Scholar] [CrossRef] [Green Version]
- Sany, D.; Elshahawy, Y.; Anwar, W. Glycated albumin versus glycated hemoglobin as glycemic indicator in hemodialysis patients with diabetes mellitus: Variables that influence. Saudi J. Kidney Dis. Transpl. 2013, 24, 260–273. [Google Scholar] [CrossRef]
- Selvin, E.; Francis, L.M.; Ballantyne, C.M.; Hoogeveen, R.C.; Coresh, J.; Brancati, F.L.; Steffes, M.W. Nontraditional markers of glycemia: Associations with microvascular conditions. Diabetes Care 2011, 34, 960–967. [Google Scholar] [CrossRef] [Green Version]
- Moon, J.H.; Chae, M.K.; Kim, K.J.; Kim, H.M.; Cha, B.S.; Lee, H.C.; Kim, Y.J.; Lee, B.W. Decreased endothelial progenitor cells and increased serum glycated albumin are independently correlated with plaque-forming carotid artery atherosclerosis in type 2 diabetes patients without documented ischemic disease. Circ. J. Off. J. Jpn. Circ. Soc. 2012, 76, 2273–2279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.O.; Kim, K.J.; Lee, B.W.; Kang, E.S.; Cha, B.S.; Lee, H.C. Serum glycated albumin predicts the progression of carotid arterial atherosclerosis. Atherosclerosis 2012, 225, 450–455. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glucose tolerance and mortality: Comparison of WHO and American Diabetes Association diagnostic criteria. The DECODE study group. European Diabetes Epidemiology Group. Diabetes Epidemiology: Collaborative analysis Of Diagnostic criteria in Europe. Lancet 1999, 354, 617–621. [CrossRef]
- Furusyo, N.; Koga, T.; Ai, M.; Otokozawa, S.; Kohzuma, T.; Ikezaki, H.; Schaefer, E.J.; Hayashi, J. Plasma glycated albumin level and atherosclerosis: Results from the Kyushu and Okinawa Population Study (KOPS). Int. J. Cardiol. 2013, 167, 2066–2072. [Google Scholar] [CrossRef]
- Norimatsu, K.; Miura, S.; Suematsu, Y.; Shiga, Y.; Miyase, Y.; Nakamura, A.; Yamada, M.; Matsunaga, A.; Saku, K. Associations between glycated albumin or hemoglobin A1c and the presence of coronary artery disease. J. Cardiol. 2015, 65, 487–493. [Google Scholar] [CrossRef] [Green Version]
- Pan, Y.; Cai, X.; Jing, J.; Meng, X.; Li, H.; Wang, Y.; Zhao, X.; Liu, L.; Wang, D.; Johnston, S.C.; et al. Stress Hyperglycemia and Prognosis of Minor Ischemic Stroke and Transient Ischemic Attack: The CHANCE Study (Clopidogrel in High-Risk Patients With Acute Nondisabling Cerebrovascular Events). Stroke 2017, 48, 3006–3011. [Google Scholar] [CrossRef]
- Suwa, T.; Ohta, A.; Matsui, T.; Koganei, R.; Kato, H.; Kawata, T.; Sada, Y.; Ishii, S.; Kondo, A.; Murakami, K.; et al. Relationship between clinical markers of glycemia and glucose excursion evaluated by continuous glucose monitoring (CGM). Endocr. J. 2010, 57, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Decode Study Group, the European Diabetes Epidemiology Group. Glucose tolerance and cardiovascular mortality: Comparison of fasting and 2-h diagnostic criteria. Arch. Intern. Med. 2001, 161, 397–405. [Google Scholar] [CrossRef]
- Bando, Y.; Ushiogi, Y.; Okafuji, K.; Toya, D.; Tanaka, N.; Fujisawa, M. The relationship of fasting plasma glucose values and other variables to 2-h postload plasma glucose in Japanese subjects. Diabetes Care 2001, 24, 1156–1160. [Google Scholar] [CrossRef] [Green Version]
- Huebschmann, A.G.; Regensteiner, J.G.; Vlassara, H.; Reusch, J.E. Diabetes and advanced glycoxidation end products. Diabetes Care 2006, 29, 1420–1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodino-Janeiro, B.K.; Gonzalez-Peteiro, M.; Ucieda-Somoza, R.; Gonzalez-Juanatey, J.R.; Alvarez, E. Glycated albumin, a precursor of advanced glycation end-products, up-regulates NADPH oxidase and enhances oxidative stress in human endothelial cells: Molecular correlate of diabetic vasculopathy. Diabetes Metab. Res. Rev. 2010, 26, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.P.; Shea, E.; Chen, S.; Shearman, C.W. Glycated albumin increases oxidative stress, activates NF-kappa B and extracellular signal-regulated kinase (ERK), and stimulates ERK-dependent transforming growth factor-beta 1 production in macrophage RAW cells. J. Lab. Clin. Med. 2003, 141, 242–249. [Google Scholar] [CrossRef]
- Lee, S.H.; Jang, M.U.; Kim, Y.; Park, S.Y.; Kim, C.; Kim, Y.J.; Sohn, J.H. Effect of Prestroke Glycemic Variability Estimated Glycated Albumin on Stroke Severity and Infarct Volume in Diabetic Patients Presenting With Acute Ischemic Stroke. Front. Endocrinol. 2020, 11, 230. [Google Scholar] [CrossRef] [Green Version]
- Koga, M.; Murai, J.; Saito, H.; Matsumoto, S.; Kasayama, S. Effects of thyroid hormone on serum glycated albumin levels: Study on non-diabetic subjects. Diabetes Res. Clin. Pract. 2009, 84, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Koga, M.; Saito, H.; Mukai, M.; Otsuki, M.; Kasayama, S. Serum glycated albumin levels are influenced by smoking status, independent of plasma glucose levels. Acta Diabetol. 2009, 46, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Koga, M.; Murai, J.; Saito, H.; Mukai, M.; Kasayama, S. Serum glycated albumin, but not glycated hemoglobin, is low in relation to glycemia in men with hypertriglyceridemia. J. Diabetes Investig. 2010, 1, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Trenti, T.; Cristani, A.; Cioni, G.; Pentore, R.; Mussini, C.; Ventura, E. Fructosamine and glycated hemoglobin as indices of glycemic control in patients with liver cirrhosis. Ric. Clin. E Lab. 1990, 20, 261–267. [Google Scholar] [CrossRef]
- Koga, M.; Murai, J.; Saito, H.; Mukai, M.; Kasayama, S. Serum glycated albumin levels, but not glycated hemoglobin, is low in relation to glycemia in non-diabetic men with nonalcoholic fatty liver disease with high alanine aminotransferase levels. Clin. Biochem. 2010, 43, 1023–1025. [Google Scholar] [CrossRef]
- Bando, Y.; Kanehara, H.; Toya, D.; Tanaka, N.; Kasayama, S.; Koga, M. Association of serum glycated albumin to haemoglobin A1C ratio with hepatic function tests in patients with chronic liver disease. Ann. Clin. Biochem. 2009, 46, 368–372. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Metabolic Risk Factors | Patients Number and Characteristics | Diagnosis Cut-Off Value of GA | Monitoring Therapy Cut-Off Value of GA | GA Parameters Associated (r = Correlation Coeff.) | Ref. |
|---|---|---|---|---|---|
| Diabetes Mellitus | 1294 prediabetic patients | >14.9% for diagnosing Diabetes | [57] | ||
| Diabetes Mellitus | 120 diabetic treated with SU | GA > 20% to switch to insulin | [58] | ||
| Dyslipidemia | 102 newly diagnosed T2DM 263 diabetic and dyslipidemic patients | >15.6% for diabetic screening | HbA1C LDL-C FPG, TG and LDL-C ↓ TC (r = 0.012) LDL-C (r = 0.073) | [63] | |
| Obesity | 236 healthy non obese and obese individuals | >13.77% for detecting prediabetes | BMI (r = 0.24) | [77] | |
| Kidney Disease | 90 diabetic hemodialysis patients | >25% for predicting mortality | [94] | ||
| Kidney Disease | Without a history of cardiovascular events | <20% for glycemic control | [105] | ||
| With a history of CV events or tendency to hypo-glycemic episodes | <24% for glycemic control | ||||
| Cerebro-cardiovascular disease | 30,000 diabetic and obese subjects | >17.9% for the prediction of CAD | [114] | ||
| Cerebro-cardiovascular disease | 1575 individuals from general population | >15.5% for predicting diabetes | HbA1c, hsCRP and CIMT | [115] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giglio, R.V.; Lo Sasso, B.; Agnello, L.; Bivona, G.; Maniscalco, R.; Ligi, D.; Mannello, F.; Ciaccio, M. Recent Updates and Advances in the Use of Glycated Albumin for the Diagnosis and Monitoring of Diabetes and Renal, Cerebro- and Cardio-Metabolic Diseases. J. Clin. Med. 2020, 9, 3634. https://doi.org/10.3390/jcm9113634
Giglio RV, Lo Sasso B, Agnello L, Bivona G, Maniscalco R, Ligi D, Mannello F, Ciaccio M. Recent Updates and Advances in the Use of Glycated Albumin for the Diagnosis and Monitoring of Diabetes and Renal, Cerebro- and Cardio-Metabolic Diseases. Journal of Clinical Medicine. 2020; 9(11):3634. https://doi.org/10.3390/jcm9113634
Chicago/Turabian StyleGiglio, Rosaria Vincenza, Bruna Lo Sasso, Luisa Agnello, Giulia Bivona, Rosanna Maniscalco, Daniela Ligi, Ferdinando Mannello, and Marcello Ciaccio. 2020. "Recent Updates and Advances in the Use of Glycated Albumin for the Diagnosis and Monitoring of Diabetes and Renal, Cerebro- and Cardio-Metabolic Diseases" Journal of Clinical Medicine 9, no. 11: 3634. https://doi.org/10.3390/jcm9113634