Association of the Hemoglobin to Serum Creatinine Ratio with In-Hospital Adverse Outcomes after Percutaneous Coronary Intervention among Non-Dialysis Patients: Insights from a Japanese Nationwide Registry (J-PCI Registry)

 , , , , ,
, , , , ,
Abstract
:1. Introduction
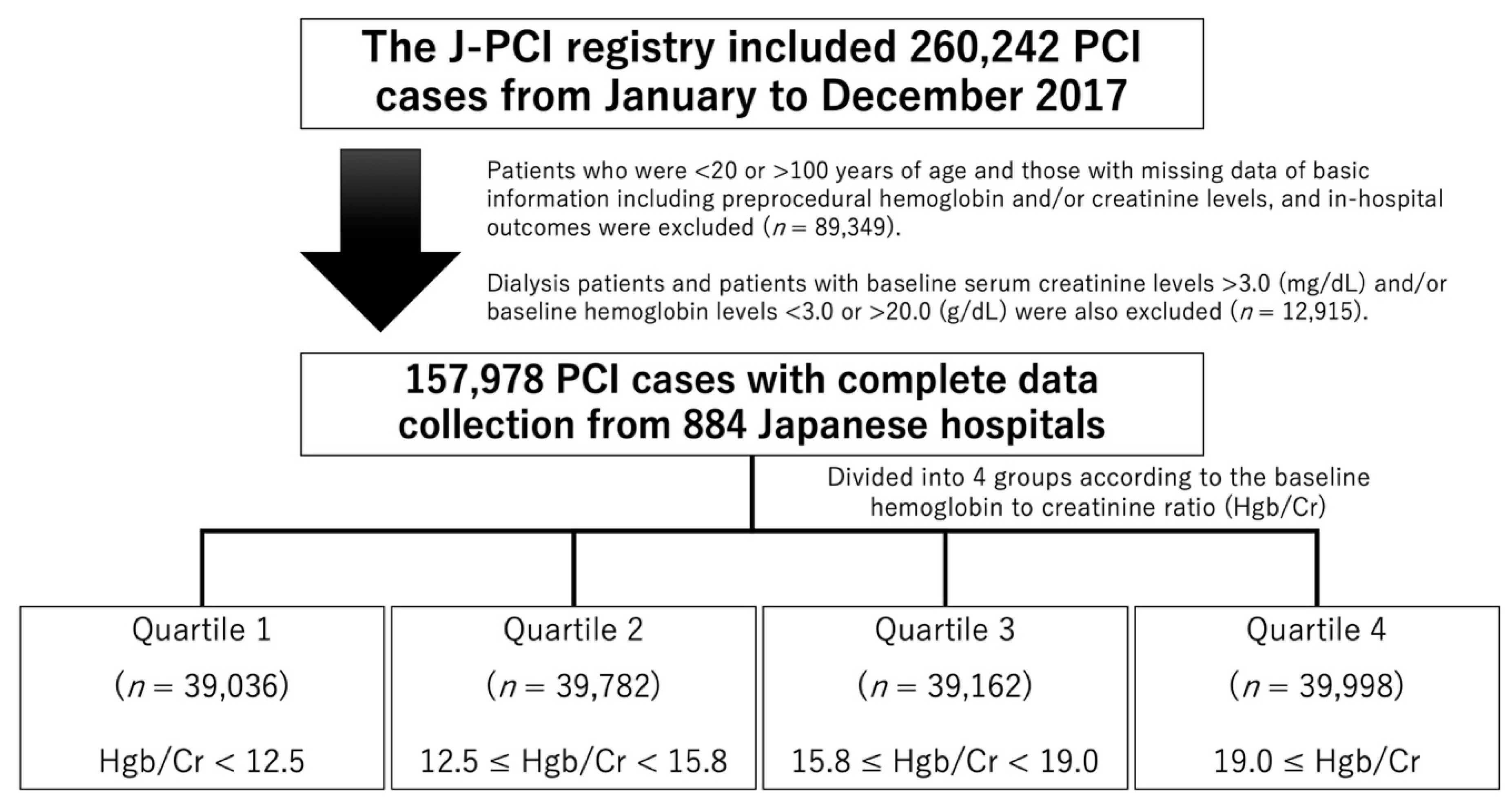
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Faggioni, M.; Baber, U.; Sartori, S.; Chandrasekhar, J.; Cohen, D.J.; Henry, T.D.; Claessen, B.E.; Dangas, G.D.; Gibson, C.M.; Krucoff, M.W.; et al. Influence of Baseline Anemia on Dual Antiplatelet Therapy Cessation and Risk of Adverse Events After Percutaneous Coronary Intervention. Circ. Cardiovasc. Interv. 2019, 12, e007133. [Google Scholar] [CrossRef] [PubMed]
- Nagao, K.; Watanabe, H.; Morimoto, T.; Inada, T.; Hayashi, F.; Nakagawa, Y.; Furukawa, Y.; Kadota, K.; Akasaka, T.; Natsuaki, M.; et al. CREDO-Kyoto PCI/CABG Registry Cohort-2, RESET and NEXT Investigators. Prognostic Impact of Baseline Hemoglobin Levels on Long-Term Thrombotic and Bleeding Events after Percutaneous Coronary Interventions. J. Am. Heart Assoc. 2019, 8, e013703. [Google Scholar] [CrossRef] [PubMed]
- Numasawa, Y.; Ueda, I.; Sawano, M.; Kuno, T.; Kodaira, M.; Noma, S.; Suzuki, M.; Miyata, H.; Fukuda, K.; Kohsaka, S. Relation of Baseline Hemoglobin Level to In-Hospital Outcomes in Patients Who Undergo Percutaneous Coronary Intervention (from a Japanese Multicenter Registry). Am. J. Cardiol. 2018, 121, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Pilgrim, T.; Vetterli, F.; Kalesan, B.; Stefanini, G.G.; Raber, L.; Stortecky, S.; Gloekler, S.; Binder, R.K.; Wenaweser, P.; Moschovitis, A.; et al. The impact of anemia on long-term clinical outcome in patients undergoing revascularization with the unrestricted use of drug-eluting stents. Circ. Cardiovasc. Interv. 2012, 5, 202–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwok, C.S.; Tiong, D.; Pradhan, A.; Andreou, A.Y.; Nolan, J.; Bertrand, O.F.; Curzen, N.; Urban, P.; Myint, P.K.; Zaman, A.G.; et al. Meta-Analysis of the Prognostic Impact of Anemia in Patients Undergoing Percutaneous Coronary Intervention. Am. J. Cardiol. 2016, 118, 610–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brener, S.J.; Mehran, R.; Dangas, G.D.; Ohman, E.M.; Witzenbichler, B.; Zhang, Y.; Parvataneni, R.; Stone, G.W. Relation of Baseline Hemoglobin Levels and Adverse Events in Patients With Acute Coronary Syndromes (from the Acute Catheterization and Urgent Intervention Triage strategY and Harmonizing Outcomes with RevasculariZatiON and Stents in Acute Myocardial Infarction Trials). Am. J. Cardiol. 2017, 119, 1710–1716. [Google Scholar]
- Bassand, J.P.; Afzal, R.; Eikelboom, J.; Wallentin, L.; Peters, R.; Budaj, A.; Fox, K.A.; Joyner, C.D.; Chrolavicius, S.; Granger, C.B.; et al. Relationship between baseline haemoglobin and major bleeding complications in acute coronary syndromes. Eur. Heart J. 2010, 31, 50–58. [Google Scholar] [CrossRef]
- Gibson, C.M.; Pinto, D.S.; Murphy, S.A.; Morrow, D.A.; Hobbach, H.P.; Wiviott, S.D.; Giugliano, R.P.; Cannon, C.P.; Antman, E.M.; Braunwald, E.; et al. Association of creatinine and creatinine clearance on presentation in acute myocardial infarction with subsequent mortality. J. Am. Coll. Cardiol. 2003, 42, 1535–1543. [Google Scholar] [CrossRef] [Green Version]
- Santopinto, J.J.; Fox, K.A.; Goldberg, R.J.; Budaj, A.; Pinero, G.; Avezum, A.; Gulba, D.; Esteban, J.; Gore, J.M.; Johnson, J.; et al. Creatinine clearance and adverse hospital outcomes in patients with acute coronary syndromes: Findings from the global registry of acute coronary events (GRACE). Heart 2003, 89, 1003–1008. [Google Scholar] [CrossRef]
- Lee, J.M.; Kang, J.; Lee, E.; Hwang, D.; Rhee, T.M.; Park, J.; Kim, H.L.; Lee, S.E.; Han, J.K.; Yang, H.M.; et al. Chronic Kidney Disease in the Second-Generation Drug-Eluting Stent Era: Pooled Analysis of the Korean Multicenter Drug-Eluting Stent Registry. JACC Cardiovasc. Interv. 2016, 9, 2097–2109. [Google Scholar] [CrossRef]
- Tsai, T.T.; Messenger, J.C.; Brennan, J.M.; Patel, U.D.; Dai, D.; Piana, R.N.; Anstrom, K.J.; Eisenstein, E.L.; Dokholyan, R.S.; Peterson, E.D.; et al. Safety and efficacy of drug-eluting stents in older patients with chronic kidney disease: A report from the linked CathPCI Registry-CMS claims database. J. Am. Coll. Cardiol. 2011, 58, 1859–1869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, C.S.; Muntner, P.; Chen, A.Y.; Alexander, K.P.; Roe, M.T.; Cannon, C.P.; Saucedo, J.F.; Kontos, M.C.; Wiviott, S.D. Use of evidence-based therapies in short-term outcomes of ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction in patients with chronic kidney disease: A report from the National Cardiovascular Data Acute Coronary Treatment and Intervention Outcomes Network registry. Circulation 2010, 121, 357–365. [Google Scholar] [PubMed] [Green Version]
- Parikh, P.B.; Jeremias, A.; Naidu, S.S.; Brener, S.J.; Lima, F.; Shlofmitz, R.A.; Pappas, T.; Marzo, K.P.; Gruberg, L. Impact of severity of renal dysfunction on determinants of in-hospital mortality among patients undergoing percutaneous coronary intervention. Catheter. Cardiovasc. Interv. 2012, 80, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Numasawa, Y.; Inohara, T.; Ishii, H.; Yamaji, K.; Hirano, K.; Kohsaka, S.; Sawano, M.; Kuno, T.; Kodaira, M.; Uemura, S.; et al. An overview of percutaneous coronary intervention in dialysis patients: Insights from a Japanese nationwide registry. Catheter. Cardiovasc. Interv. 2019, 94, E1–E8. [Google Scholar] [CrossRef]
- Brennan, J.M.; Curtis, J.P.; Dai, D.; Fitzgerald, S.; Khandelwal, A.K.; Spertus, J.A.; Rao, S.V.; Singh, M.; Shaw, R.E.; Ho, K.K.; et al. Enhanced mortality risk prediction with a focus on high-risk percutaneous coronary intervention: Results from 1,208,137 procedures in the NCDR (National Cardiovascular Data Registry). JACC Cardiovasc. Interv. 2013, 6, 790–799. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.V.; McCoy, L.A.; Spertus, J.A.; Krone, R.J.; Singh, M.; Fitzgerald, S.; Peterson, E.D. An updated bleeding model to predict the risk of post-procedure bleeding among patients undergoing percutaneous coronary intervention: A report using an expanded bleeding definition from the National Cardiovascular Data Registry CathPCI Registry. JACC Cardiovasc. Interv. 2013, 6, 897–904. [Google Scholar] [CrossRef] [Green Version]
- Matsue, Y.; Matsumura, A.; Abe, M.; Ono, M.; Seya, M.; Nakamura, T.; Iwatsuka, R.; Mizukami, A.; Setoguchi, M.; Nagahori, W.; et al. Prognostic implications of chronic kidney disease and anemia after percutaneous coronary intervention in acute myocardial infarction patients. Heart Vessels 2013, 28, 19–26. [Google Scholar] [CrossRef]
- Shiraishi, J.; Kohno, Y.; Nakamura, T.; Yanagiuchi, T.; Hashimoto, S.; Ito, D.; Kimura, M.; Matsui, A.; Yokoi, H.; Arihara, M.; et al. Prognostic impact of chronic kidney disease and anemia at admission on in-hospital outcomes after primary percutaneous coronary intervention for acute myocardial infarction. Int. Heart J. 2014, 55, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Pilgrim, T.; Rothenbuhler, M.; Kalesan, B.; Pulver, C.; Stefanini, G.G.; Zanchin, T.; Raber, L.; Stortecky, S.; Jung, S.; Mattle, H.; et al. Additive effect of anemia and renal impairment on long-term outcome after percutaneous coronary intervention. PLoS ONE 2014, 9, e114846. [Google Scholar] [CrossRef] [Green Version]
- Kitai, Y.; Ozasa, N.; Morimoto, T.; Bao, B.; Furukawa, Y.; Nakagawa, Y.; Kadota, K.; Yanagita, M.; Shizuta, S.; Kimura, T.; et al. Prognostic implications of anemia with or without chronic kidney disease in patients undergoing elective percutaneous coronary intervention. Int. J. Cardiol. 2013, 168, 5221–5228. [Google Scholar] [CrossRef]
- Giraldez, R.R.; Sabatine, M.S.; Morrow, D.A.; Mohanavelu, S.; McCabe, C.H.; Antman, E.M.; Braunwald, E. Baseline hemoglobin concentration and creatinine clearance composite laboratory index improves risk stratification in ST-elevation myocardial infarction. Am. Heart J. 2009, 157, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Numasawa, Y.; Inohara, T.; Ishii, H.; Yamaji, K.; Kohsaka, S.; Sawano, M.; Kodaira, M.; Uemura, S.; Kadota, K.; Amano, T.; et al. Comparison of Outcomes After Percutaneous Coronary Intervention in Elderly Patients, Including 10 628 Nonagenarians: Insights From a Japanese Nationwide Registry (J-PCI Registry). J. Am. Heart Assoc. 2019, 8, e011183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozaki, Y.; Katagiri, Y.; Onuma, Y.; Amano, T.; Muramatsu, T.; Kozuma, K.; Otsuji, S.; Ueno, T.; Shiode, N.; Kawai, K.; et al. CVIT expert consensus document on primary percutaneous coronary intervention (PCI) for acute myocardial infarction (AMI) in 2018. Cardiovasc. Interv. Ther. 2018, 33, 178–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujii, T.; Ikari, Y.; Hashimoto, H.; Kadota, K.; Amano, T.; Uemura, S.; Takashima, H.; Nakamura, M. Post-interventional adverse event risk by vascular access site among patients with acute coronary syndrome in Japan: Observational analysis with a national registry J-PCI database. Cardiovasc. Interv. Ther. 2019, 34, 297–304. [Google Scholar] [CrossRef]
- Sawano, M.; Yamaji, K.; Kohsaka, S.; Inohara, T.; Numasawa, Y.; Ando, H.; Iida, O.; Shinke, T.; Ishii, H.; Amano, T. Contemporary use and trends in percutaneous coronary intervention in Japan: An outline of the J-PCI registry. Cardiovasc. Interv. Ther 2020, 35, 218–226. [Google Scholar] [CrossRef]
- Numasawa, Y.; Inohara, T.; Ishii, H.; Kuno, T.; Kodaira, M.; Kohsaka, S.; Fujii, K.; Uemura, S.; Amano, T.; Kadota, K.; et al. Comparison of Outcomes of Women Versus Men With Non-ST-elevation Acute Coronary Syndromes Undergoing Percutaneous Coronary Intervention (from the Japanese Nationwide Registry). Am. J. Cardiol. 2017, 119, 826–831. [Google Scholar] [CrossRef]
- Kohsaka, S.; Kumamaru, H.; Inohara, T.; Amano, T.; Akasaka, T.; Miyata, H.; Motomura, N.; Nakamura, M. Outcome of Percutaneous Coronary Intervention in Relation to the Institutional Volume of Coronary Artery Bypass Surgery. J. Clin. Med. 2020, 9, 1267. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Kuno, T.; Numasawa, Y.; Mikami, T.; Niimi, N.; Sawano, M.; Kodaira, M.; Suzuki, M.; Ueno, K.; Ueda, I.; Fukuda, K.; et al. Association of decreasing hemoglobin levels with the incidence of acute kidney injury after percutaneous coronary intervention: A prospective multi-center study. Heart Vessels 2020. [Google Scholar] [CrossRef]
- Ohno, Y.; Maekawa, Y.; Miyata, H.; Inoue, S.; Ishikawa, S.; Sueyoshi, K.; Noma, S.; Kawamura, A.; Kohsaka, S.; Fukuda, K. Impact of periprocedural bleeding on incidence of contrast-induced acute kidney injury in patients treated with percutaneous coronary intervention. J. Am. Coll. Cardiol. 2013, 62, 1260–1266. [Google Scholar] [CrossRef] [Green Version]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized Bleeding Definitions for Cardiovascular Clinical Trials: A Consensus Report From the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Hemoglobin to Creatinine Ratio (Hemoglobin [g/dL]/Creatinine [mg/dL]) | |||||
|---|---|---|---|---|---|---|
| Total Cohort | Quartile 1 <12.5 | Quartile 2 12.5 ≤ … < 15.8 | Quartile 3 15.8 ≤ … <19.0 | Quartile 4 19.0≤ | p-Value | |
| n = 157,978 | n = 39,036 | n = 39,782 | n = 39,162 | n = 39,998 | ||
| Age, (years) | 70.6 ± 11.2 | 75.7 ± 9.7 | 71.5 ± 10.4 | 68.6 ± 11.1 | 66.7 ± 11.6 | <0.001 |
| Sex, female | 36,768 (23.3) | 8098 (20.7) | 7014 (17.6) | 7888 (20.1) | 13,768 (34.4) | <0.001 |
| Hypertension | 117,034 (77.2) | 31,296 (82.7) | 29,830 (78.3) | 28,062 (75.0) | 27,846 (73.0) | <0.001 |
| Hyperlipidemia | 103,908 (68.6) | 23,906 (63.1) | 26,188 (68.7) | 26,655 (71.2) | 27,159 (71.2) | <0.001 |
| Diabetes mellitus | 67,231 (44.4) | 18,942 (50.0) | 16,488 (43.3) | 15,416 (41.2) | 16,385 (43.0) | <0.001 |
| Current smoker | 50,159 (33.1) | 10,525 (27.8) | 12,375 (32.5) | 13,165 (35.2) | 14,094 (37.0) | <0.001 |
| History of percutaneous coronary intervention | 72,780 (46.2) | 19,888 (51.1) | 19,971 (50.3) | 17,932 (45.9) | 14,989 (37.5) | <0.001 |
| History of coronary artery bypass grafting | 5056 (3.2) | 2015 (5.2) | 1358 (3.4) | 999 (2.6) | 684 (1.7) | <0.001 |
| History of heart failure | 20,476 (13.1) | 9563 (24.8) | 4937 (12.5) | 3359 (8.7) | 2617 (6.6) | <0.001 |
| History of myocardial infarction | 37,144 (23.7) | 10,947 (28.3) | 10,333 (26.2) | 8803 (22.6) | 7061 (17.8) | <0.001 |
| Peripheral artery disease | 10,375 (6.8) | 4030 (10.6) | 2652 (7.0) | 2024 (5.4) | 1669 (4.4) | <0.001 |
| Chronic obstructive pulmonary disease | 4052 (2.7) | 1389 (3.7) | 1068 (2.8) | 924 (2.5) | 671 (1.8) | <0.001 |
| Cardiogenic shock | 5183 (3.3) | 2551 (6.5) | 1219 (3.1) | 767 (2.0) | 646 (1.6) | <0.001 |
| Acute heart failure | 6289 (4.0) | 2982 (7.7) | 1401 (3.5) | 948 (2.4) | 958 (2.4) | <0.001 |
| Chronic kidney disease | 22,402 (14.8) | 16,183 (42.7) | 4767 (12.5) | 1096 (2.9) | 356 (0.9) | <0.001 |
| Cardiopulmonary arrest | 2948 (1.9) | 1379 (3.5) | 729 (1.8) | 463 (1.2) | 377 (0.9) | <0.001 |
| Presentation or diagnosis | ||||||
| Acute coronary syndrome | 60,594 (38.4) | 14,799 (38.0) | 13,423 (33.8) | 14,474 (37.0) | 17,898 (44.8) | <0.001 |
| ST-elevation myocardial infarction | 28,294 (17.9) | 6636 (17.0) | 6069 (15.3) | 6666 (17.0) | 8923 (22.3) | <0.001 |
| Non-ST-elevation myocardial infarction | 8350 (5.3) | 2310 (5.9) | 1797 (4.5) | 1864 (4.8) | 2379 (6.0) | <0.001 |
| Laboratory values | ||||||
| Baseline hemoglobin (g/dL) | 13.3 ± 1.9 | 11.8 ± 1.9 | 13.2 ± 1.6 | 13.9 ± 1.6 | 14.3 ± 1.6 | <0.001 |
| Baseline creatinine (mg/dL) | 0.9 ± 0.3 | 1.3 ± 0.4 | 0.9 ± 0.1 | 0.8 ± 0.1 | 0.7 ± 0.1 | <0.001 |
| Hemoglobin to creatinine ratio | 15.9 ± 5.0 | 9.6 ± 2.2 | 14.2 ± 0.9 | 17.3 ± 0.9 | 22.2 ± 2.6 | <0.001 |
| Access site | ||||||
| Transfemoral intervention | 35,019 (22.2) | 10,400 (26.6) | 8690 (21.8) | 7960 (20.3) | 7969 (19.9) | <0.001 |
| Transradial intervention | 115,670 (73.2) | 26,296 (67.4) | 29,362 (73.8) | 29,600 (75.6) | 30,412 (76.0) | |
| Others | 7289 (4.6) | 2340 (6.0) | 1730 (4.3) | 1602 (4.1) | 1617 (4.0) | |
| Number of diseased vessels | ||||||
| 1-vessel disease | 97,835 (61.9) | 22,018 (56.4) | 24,463 (61.5) | 25,080 (64.0) | 26,274 (65.7) | <0.001 |
| 2-vessel disease | 40,569 (25.7) | 10,803 (27.7) | 10,375 (26.1) | 9731 (24.8) | 9660 (24.2) | <0.001 |
| 3-vessel disease | 19,100 (12.1) | 5994 (15.4) | 4806 (12.1) | 4280 (10.9) | 4020 (10.1) | <0.001 |
| Left main trunk lesion | 6504 (4.1) | 2262 (5.8) | 1700 (4.3) | 1408 (3.6) | 1134 (2.8) | <0.001 |
| Target coronary artery | ||||||
| Right coronary artery | 52,709 (33.4) | 14,126 (36.2) | 13,441 (33.8) | 12,856 (32.8) | 12,286 (30.7) | <0.001 |
| Left main trunk-Left anterior descending artery | 83,220 (52.7) | 20,009 (51.3) | 20,602 (51.8) | 20,647 (52.7) | 21,962 (54.9) | <0.001 |
| Left circumflex artery | 39,471 (25.0) | 10,095 (25.9) | 10,199 (25.6) | 9636 (24.6) | 9541 (23.9) | <0.001 |
| Bypass graft | 672 (0.4) | 263 (0.7) | 190 (0.5) | 126 (0.3) | 93 (0.2) | <0.001 |
| Devices | ||||||
| Drug-eluting stent | 135,601 (85.8) | 32,948 (84.4) | 34,070 (85.6) | 33,787 (86.3) | 34,796 (87.0) | <0.001 |
| Bare-metal stent | 1709 (1.1) | 518 (1.3) | 419 (1.1) | 387 (1.0) | 385 (1.0) | <0.001 |
| Drug-coated balloon | 20,195 (12.8) | 5282 (13.5) | 5366 (13.5) | 4960 (12.7) | 4587 (11.5) | <0.001 |
| Rotational atherectomy | 4887 (3.1) | 1588 (4.1) | 1273 (3.2) | 1093 (2.8) | 933 (2.3) | <0.001 |
| Preprocedural medications | ||||||
| Aspirin | 140,382 (88.9) | 34,560 (88.5) | 35,686 (89.7) | 34,926 (89.2) | 35,210 (88.0) | <0.001 |
| Clopidogrel | 53,941 (34.1) | 14,584 (37.4) | 14,073 (35.4) | 13,065 (33.4) | 12,219 (30.5) | <0.001 |
| Prasugrel | 79,549 (50.4) | 18,136 (46.5) | 20,021 (50.3) | 20,171 (51.5) | 21,221 (53.1) | <0.001 |
| Ticagrelor | 123 (0.1) | 33 (0.1) | 37 (0.1) | 29 (0.1) | 24 (0.1) | 0.375 |
| Oral anticoagulants | 11,263 (7.1) | 4292 (11.0) | 3104 (7.8) | 2258 (5.8) | 1609 (4.0) | <0.001 |
| Outcomes | Hemoglobin to Creatinine Ratio (Hemoglobin (g/dL)/Creatinine (mg/dL)) | |||||
|---|---|---|---|---|---|---|
| Total Cohort | Quartile 1 <12.5 | Quartile 2 12.5 ≤ … < 15.8 | Quartile 3 15.8 ≤ … < 19.0 | Quartile 4 19.0≤ | p-Value | |
| n = 157,978 | n = 39,036 | n = 39,782 | n = 39,162 | n = 39,998 | ||
| Procedural success (final TIMI III flow) | 155,017 (98.1) | 38,171 (97.8) | 39,051 (98.2) | 38,485 (98.3) | 39,310 (98.3) | <0.001 |
| In-hospital mortality | 1296 (0.82) | 786 (2.01) | 243 (0.61) | 141 (0.36) | 126 (0.32) | <0.001 |
| Cardiac tamponade | 230 (0.15) | 76 (0.19) | 53 (0.13) | 48 (0.12) | 53 (0.13) | 0.032 |
| Cardiogenic shock | 1636 (1.04) | 729 (1.87) | 385 (0.97) | 277 (0.71) | 245 (0.61) | <0.001 |
| Emergency operation | 141 (0.09) | 50 (0.13) | 33 (0.08) | 32 (0.08) | 26 (0.07) | 0.022 |
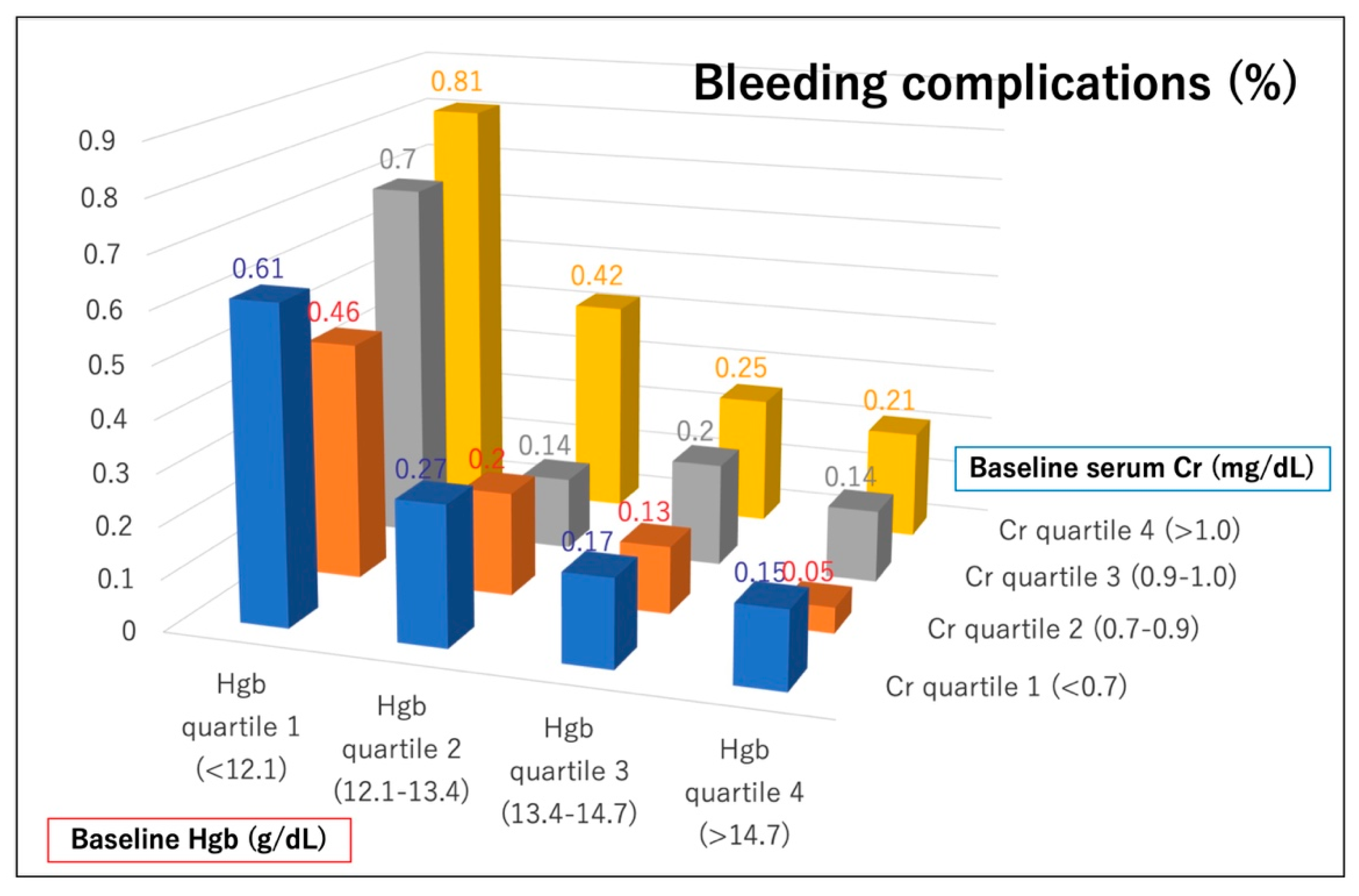
| Bleeding complications | 491 (0.31) | 258 (0.66) | 90 (0.23) | 79 (0.20) | 64 (0.16) | <0.001 |
| Access-site bleeding | 246 (0.16) | 115 (0.29) | 48 (0.12) | 44 (0.11) | 39 (0.10) | <0.001 |
| Non-access-site bleeding | 256 (0.16) | 147 (0.38) | 44 (0.11) | 37 (0.09) | 28 (0.07) | <0.001 |
| Variables | In-Hospital Mortality | Bleeding Complications | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | |
| Age | 1.02 | 1.02–1.03 | <0.001 | 1.01 | 1.00–1.02 | 0.040 |
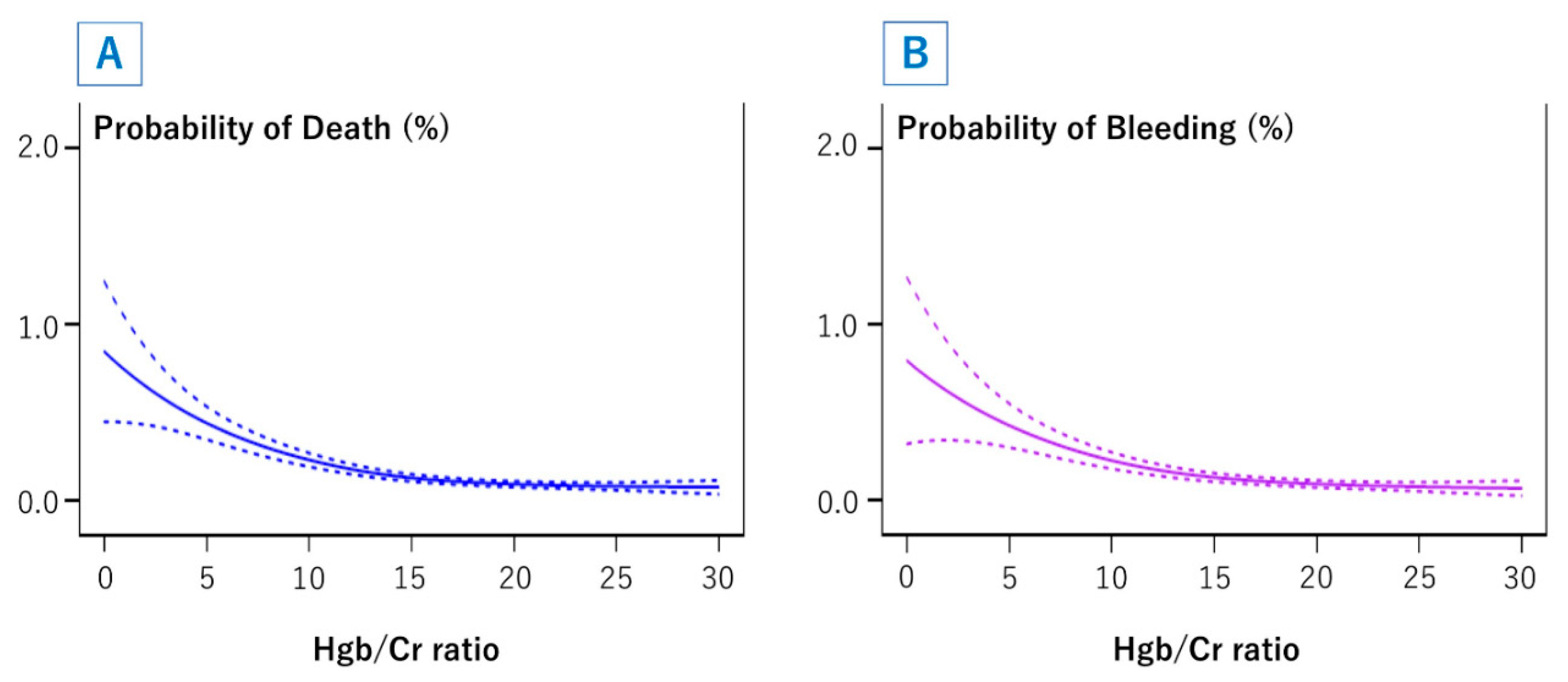
| Hgb/Cr ratio | 0.91 | 0.89–0.92 | <0.001 | 0.92 | 0.90–0.94 | <0.001 |
| Oral anticoagulants | 1.09 | 0.83–1.42 | 0.539 | 1.66 | 1.24–2.22 | 0.006 |
| Female sex | 1.69 | 1.45–1.97 | <0.001 | 2.64 | 2.15–3.23 | <0.001 |
| History of heart failure | 1.34 | 1.12–1.61 | 0.002 | 1.19 | 0.94–1.52 | 0.148 |
| Acute heart failure | 2.80 | 2.33–3.37 | <0.001 | 1.09 | 0.78–1.51 | 0.620 |
| Presentation | ||||||
| ST-elevation myocardial infarction | 4.26 | 3.57–5.08 | <0.001 | 1.49 | 1.16–1.90 | 0.001 |
| Non-ST-elevation myocardial infarction | 2.94 | 2.31–3.74 | <0.001 | 1.62 | 1.15–2.27 | 0.005 |
| Cardiogenic shock | 7.03 | 5.82–8.48 | <0.001 | 2.98 | 2.15–4.14 | <0.001 |
| Hypertension | 0.68 | 0.59–0.79 | <0.001 | 0.94 | 0.75–1.18 | 0.596 |
| Hyperlipidemia | 0.55 | 0.47–0.63 | <0.001 | 0.74 | 0.61–0.90 | 0.003 |
| Diabetes mellitus | 1.06 | 0.92–1.22 | 0.389 | 0.79 | 0.65–0.96 | 0.017 |
| 3-vessel disease | 1.59 | 1.35–1.87 | <0.001 | 1.13 | 0.88–1.45 | 0.339 |
| Left main trunk lesion | 1.73 | 1.40–2.12 | <0.001 | 1.45 | 1.05–1.99 | 0.024 |
| Access site | ||||||
| Transfemoral intervention (reference) | - | - | - | - | - | - |
| Transradial intervention | 0.41 | 0.35–0.49 | <0.001 | 0.30 | 0.24–0.37 | <0.001 |
| Other | 0.97 | 0.72–1.30 | 0.825 | 0.75 | 0.50–1.12 | 0.155 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Numasawa, Y.; Inohara, T.; Ishii, H.; Yamaji, K.; Kohsaka, S.; Sawano, M.; Kodaira, M.; Uemura, S.; Kadota, K.; Amano, T.; et al. Association of the Hemoglobin to Serum Creatinine Ratio with In-Hospital Adverse Outcomes after Percutaneous Coronary Intervention among Non-Dialysis Patients: Insights from a Japanese Nationwide Registry (J-PCI Registry). J. Clin. Med. 2020, 9, 3612. https://doi.org/10.3390/jcm9113612
Numasawa Y, Inohara T, Ishii H, Yamaji K, Kohsaka S, Sawano M, Kodaira M, Uemura S, Kadota K, Amano T, et al. Association of the Hemoglobin to Serum Creatinine Ratio with In-Hospital Adverse Outcomes after Percutaneous Coronary Intervention among Non-Dialysis Patients: Insights from a Japanese Nationwide Registry (J-PCI Registry). Journal of Clinical Medicine. 2020; 9(11):3612. https://doi.org/10.3390/jcm9113612
Chicago/Turabian StyleNumasawa, Yohei, Taku Inohara, Hideki Ishii, Kyohei Yamaji, Shun Kohsaka, Mitsuaki Sawano, Masaki Kodaira, Shiro Uemura, Kazushige Kadota, Tetsuya Amano, and et al. 2020. "Association of the Hemoglobin to Serum Creatinine Ratio with In-Hospital Adverse Outcomes after Percutaneous Coronary Intervention among Non-Dialysis Patients: Insights from a Japanese Nationwide Registry (J-PCI Registry)" Journal of Clinical Medicine 9, no. 11: 3612. https://doi.org/10.3390/jcm9113612