The Effect of the Dose of Isotonic Saline on the Correction of Serum Sodium in the Treatment of Hypovolemic Hyponatremia

 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Spasovski, G.; Vanholder, R.; Allolio, B.; Annane, D.; Ball, S.; Bichet, D.; Decaux, G.; Fenske, W.; Hoorn, E.J.; Ichai, C.; et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Nephrol. Dial. Transplant. 2014, 29, i1–i39. [Google Scholar] [CrossRef] [Green Version]
- Verbalis, J.G.; Goldsmith, S.R.; Greenberg, A.; Korzelius, C.; Schrier, R.W.; Sterns, R.H.; Thompson, C.J. Diagnosis, evaluation, and treatment of hyponatremia: Expert panel recommendations. Am. J. Med. 2013, 126, S1–S42. [Google Scholar] [CrossRef] [PubMed]
- Sahay, M.; Sahay, R. Hyponatremia: A practical approach. Indian J. Endocrinol. Metab. 2014, 18, 760. [Google Scholar] [CrossRef]
- Baylis, P.H. Posterior pituitary function in health and disease. Clin. Endocrinol. Metab. 1983, 12, 747–770. [Google Scholar] [CrossRef]
- Norsk, P. Influence of low- and high-pressure baroreflexes on vasopressin release in humans. Acta Endocrinol. (Copenh) 1989, 121, 3–27. [Google Scholar] [CrossRef] [PubMed]
- Yao, S.T.; Antunes, V.R.; Bradley, P.M.J.; Kasparov, S.; Ueta, Y.; Paton, J.F.R.; Murphy, D. Temporal profile of arginine vasopressin release from the neurohypophysis in response to hypertonic saline and hypotension measured using a fluorescent fusion protein. J. Neurosci. Methods 2011, 201, 191–195. [Google Scholar] [CrossRef] [PubMed]
- NICE Guidelines. Intravenous Fluid Therapy in Children and Young People in Hospital; National Institute for Health and Care Excellence: London, UK, 2015. [Google Scholar]
- Green, J.; Lillie, J. Intravenous fluid therapy in children and young people in hospital N29. Arch. Dis. Child. Educ. Pract. Ed. 2017, 102, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Gharaibeh, K.A.; Brewer, J.M.; Agarwal, M.; Fülöp, T. Risk factors, complication and measures to prevent or reverse catastrophic sodium overcorrection in chronic hyponatremia. Am. J. Med. Sci. 2015, 349, 170–175. [Google Scholar] [CrossRef] [PubMed]
- George, J.C.; Zafar, W.; Dan Bucaloiu, I.; Chang, A.R. Risk factors and outcomes of rapid correction of severe hyponatremia. Clin. J. Am. Soc. Nephrol. 2018, 13, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Tanneau, R.S.; Henry, A.; Rouhart, F.; Bourbigot, B.; Garo, B.; Mocquard, Y.; Goas, J.Y. High incidence of neurologic complications following rapid correction of severe hyponatremia in polydipsic patients. J. Clin. Psychiatry 1994, 55, 349–354. [Google Scholar]
- Sterns, R.H.; Riggs, J.E.; Schochet, S.S. Osmotic Demyelination Syndrome Following Correction of Hyponatremia. N. Engl. J. Med. 1986, 314, 1535–1542. [Google Scholar] [CrossRef] [PubMed]
- Sterns, R.H.; Cappuccio, J.D.; Silver, S.M.; Cohen, E.P. Neurologic sequelae after treatment of severe hyponatremia: A multicenter perspective. J. Am. Soc. Nephrol. 1994, 4, 1522–1530. [Google Scholar] [PubMed]
- Aratani, S.; Hara, M.; Nagahama, M.; Taki, F.; Futatsuyama, M.; Tsuruoka, S.; Komatsu, Y. A low initial serum sodium level is associated with an increased risk of overcorrection in patients with chronic profound hyponatremia: A retrospective cohort analysis. BMC Nephrol. 2017, 18, 316. [Google Scholar] [CrossRef] [Green Version]
- Hillier, T.A.; Abbott, R.D.; Barrett, E.J. Hyponatremia: Evaluating the correction factor for hyperglycemia. Am. J. Med. 1999, 106, 399–403. [Google Scholar] [CrossRef]
- Tzoulis, P.; Runkle-De la Vega, I. The Diagnostic Approach to the Patient with Hyponatremia: Are the Correct Investigations Being Done? In Frontiers of Hormone Research. Disorders of Fluid and Electrolyte Metabolism. Focus on Hyponatremia; Peri, A., Thompson, C.J., Verbalis, J.G., Eds.; KARGER: Berlin, Germany, 2019; pp. 190–199. [Google Scholar]
- Hoorn, E.J.; Zietse, R. Diagnosis and treatment of hyponatremia: Compilation of the guidelines. J. Am. Soc. Nephrol. 2017, 28, 1340–1349. [Google Scholar] [CrossRef]
- Chung, H.-M.; Kluge, R.; Schrier, R.W.; Anderson, R.J. Clinical assessment of extracellular fluid volume in hyponatremia. Am. J. Med. 1987, 83, 905–908. [Google Scholar] [CrossRef]
- Runkle, I.; Gomez-Hoyos, E.; Cuesta-Hernández, M.; Chafer-Vilaplana, J.; de Miguel, P. Hyponatraemia in older patients: A clinical and practical approach. Rev. Clin. Gerontol. 2015, 25, 31–52. [Google Scholar] [CrossRef]
- Ruiz Sanchez, J.G.; Cárdenas Salas, J.; López Nevado, C.; Durán Rodriguez-Hervada, A.; Cuesta Hernández, M.; Calle Pascual, A.; Runkle de La vega, I. Nuevo Método Bioquímico Para la Clasificación Volémica de la Hiponatremia; Madrid, Spain. Endocrinol. Diabetes Nutr. 2019, 66, 7. [Google Scholar] [CrossRef]
- Vu, T.; Wong, R.; Hamblin, P.S.; Zajac, J.; Grossmann, M. Patients Presenting with Severe Hypotonic Hyponatremia: Etiological Factors, Assessment, and Outcomes. Hosp. Pract. 2009, 37, 128–136. [Google Scholar] [CrossRef]
- Peri, A.; Thompson, C.J.; Verbalis, J.G. (Eds.) Disorders of Fluid and Electrolyte Metabolism; Frontiers of Hormone Research; S. Karger AG: Berlin, Germany, 2019; Volume 52, ISBN 978-3-318-06382-0. [Google Scholar]
- Pirzada, N.A.; Ali, I.I. Central pontine myelinolysis. Mayo Clin. Proc. 2001, 76, 559–562. [Google Scholar] [CrossRef] [Green Version]
- MacMillan, T.E.; Cavalcanti, R.B. Outcomes in Severe Hyponatremia Treated With and Without Desmopressin. Am. J. Med. 2018, 131, 317. [Google Scholar] [CrossRef] [PubMed]
- Ward, F.L.; Tobe, S.W.; Naimark, D.M.J. The Role of Desmopressin in the Management of Severe, Hypovolemic Hyponatremia: A Single-Center, Comparative Analysis. Can. J. Kidney Heal. Dis. 2018, 5, 2054358118761051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrahy, A.; Dineen, R.; Hannon, A.M.; Cuesta, M.; Tormey, W.; Sherlock, M.; Thompson, C.J. Continuous Versus Bolus Infusion of Hypertonic Saline in the Treatment of Symptomatic Hyponatremia Caused by SIAD. J. Clin. Endocrinol. Metab. 2019, 104, 3595–3602. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, O.; Cuesta, M.; Tormey, W.T.; Sherlock, M.; Williams, D.J.; Thompson, C.J.; Garrahy, A. 109 Hyponatraemia in Older Patients is Often Untreated, Despite Greater Mortality Burden; Results of A Prospective Cohort Study. Age Ageing 2020, 49, i34–i36. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, N.; Lee, K.E.; Gwak, H.S. Risk factors for sodium overcorrection in non-hypovolemic hyponatremia patients treated with tolvaptan. Eur. J. Clin. Pharmacol. 2020. [Google Scholar] [CrossRef]
- Sterns, R.H. Disorders of Plasma Sodium—Causes, Consequences, and Correction. N. Engl. J. Med. 2015, 372, 55–65. [Google Scholar] [CrossRef] [Green Version]
- Adrogué, H.J.; Madias, N.E. Hyponatremia. N. Engl. J. Med. 2000, 342, 1581–1589. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N = 30 (100%) | |
|---|---|
| Age, years | 72 (60–80) |
| Sex female, n (%) | 15 (50%) |
| Clinical markers of hypovolemia | |
| Blood pressure ≤ 90/60 mmHg, n (%) | 7 (23%) |
| Heart rate ≥ 90 bpm, n (%) | 12 (40%) |
| Decreased internal jugular vein pulse height (n = 22), n (%) | 22 (100%) |
| Orthostatic symptoms (n = 20), n (%) | 14 (70%) |
| Biochemical serum parameters | |
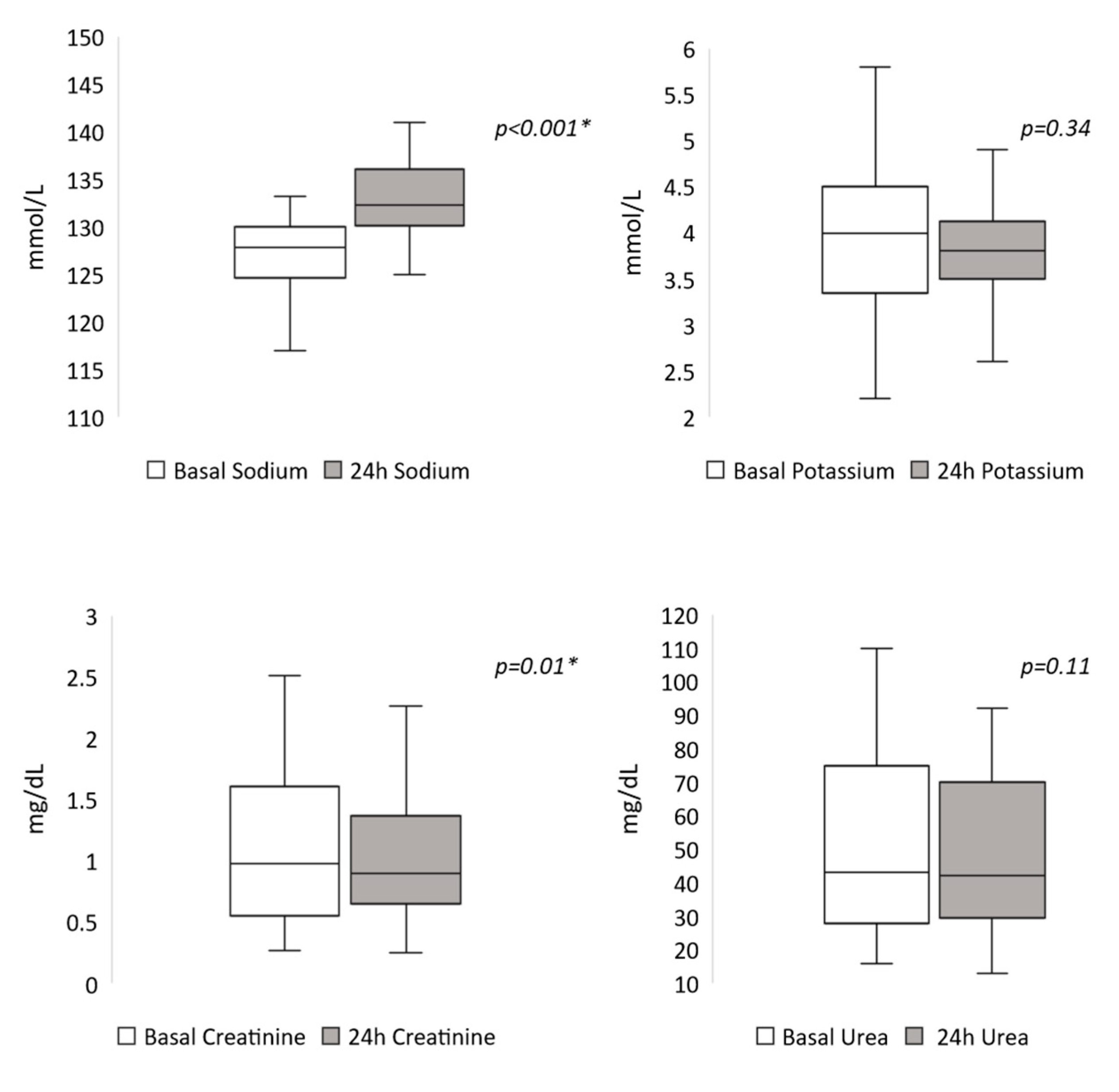
| Sodium mmol/L | 128 (125–130) |
| Potassium mmol/L | 4 (3.4–4.5) |
| Creatinine mg/dL | 0.98 (0.55–1.61) |
| Urea mg/dL | 43 (27.7–75) |
| Risk Factors for Osmotic demyelination syndrome, n (%) | 23 (78%) |
| Malnutrition, n (%) | 18 (60%) |
| Hypokalemia, n (%) | 9 (30%) |
| Alcoholism, n (%) | 2 (7%) |
| Liver disease, n (%) | 1 (3%) |
| Location of the patients | |
| Emergency room, n (%) | 16 (53%) |
| Hospitalization ward, n (%) | 14 (47%) |
| Type of isotonic saline solution | |
| NaCl 0.9%, n (%) | 25 (83%) |
| NaCl 0.81%, n (%) | 5 (17%) |
| Etiology of hypovolemia | |
| Unknown, n (%) | 8 (27%) |
| Gastrointestinal losses, n (%) | 13 (43%) |
| Urinary losses, n (%) | 17 (57%) |
| Blood loss n (%) | 2 (7%) |
| 24-h SNa ∆ ≥ 8 mmol/L | 24-h SNa ∆ ≥ 6 mmol/L | |||||
|---|---|---|---|---|---|---|
| Yes (n = 10) | No (n = 20) | p * | Yes (n = 15) | No (n = 15) | p * | |
| Female, % | 70 | 40 | 0.12 | 67 | 33 | 0.68 |
| Male, % | 30 | 60 | 33 | 67 | ||
| Age, years | 72 (47–84) | 75 (60–79) | 0.681 | 72 (51–83) | 72 (60–77) | 0.967 |
| Weight, kg | 53 (49–61) | 61 (53–72) | 0.067 | 58 (49–65) | 58 (53–72) | 0.187 |
| Basal serum sodium, mmol/L | 125 (122–127) | 129 (127–131) | 0.044 * | 125 (122–131) | 129 (127–130) | 0.067 |
| Basal serum sodium ≤ 120 mmol/L, % | 10 | 10 | 1 | 13.3 | 6.7 | 1 |
| Risk factors for osmotic demyelination syndrome, % | 80 | 75 | 0.76 | 73.3 | 80 | 0.66 |
| Malnutrition, % | 60 | 60 | 1 | 53 | 67 | 0.45 |
| Hypokalemia, % | 30 | 30 | 1 | 27 | 34 | 1 |
| Alcoholism, % | 0 | 10 | 0.3 | 0 | 13 | 0.14 |
| Liver disease, % | 0 | 5 | 0.47 | 0 | 7 | 0.3 |
| Duration of hyponatremia | ||||||
| Acute, % | 30 | 15 | 0.372 | 33 | 7 | 0.169 |
| Chronic, % | 70 | 85 | 67 | 93 | ||
| Location of patients | ||||||
| Emergency room, % | 50 | 45 | 1 | 60 | 33 | 0.272 |
| Hospitalization ward, % | 50 | 55 | 40 | 67 | ||
| Associated potassium chloride treatment, % | 30 | 30 | 1 | 27 | 33 | 1 |
| Type of isotonic saline solution | ||||||
| NaCl 0.9%, % | 90 | 80 | 0.64 | 93 | 73 | 0.33 |
| NaCl 0.81%, % | 10 | 20 | 7 | 27 | ||
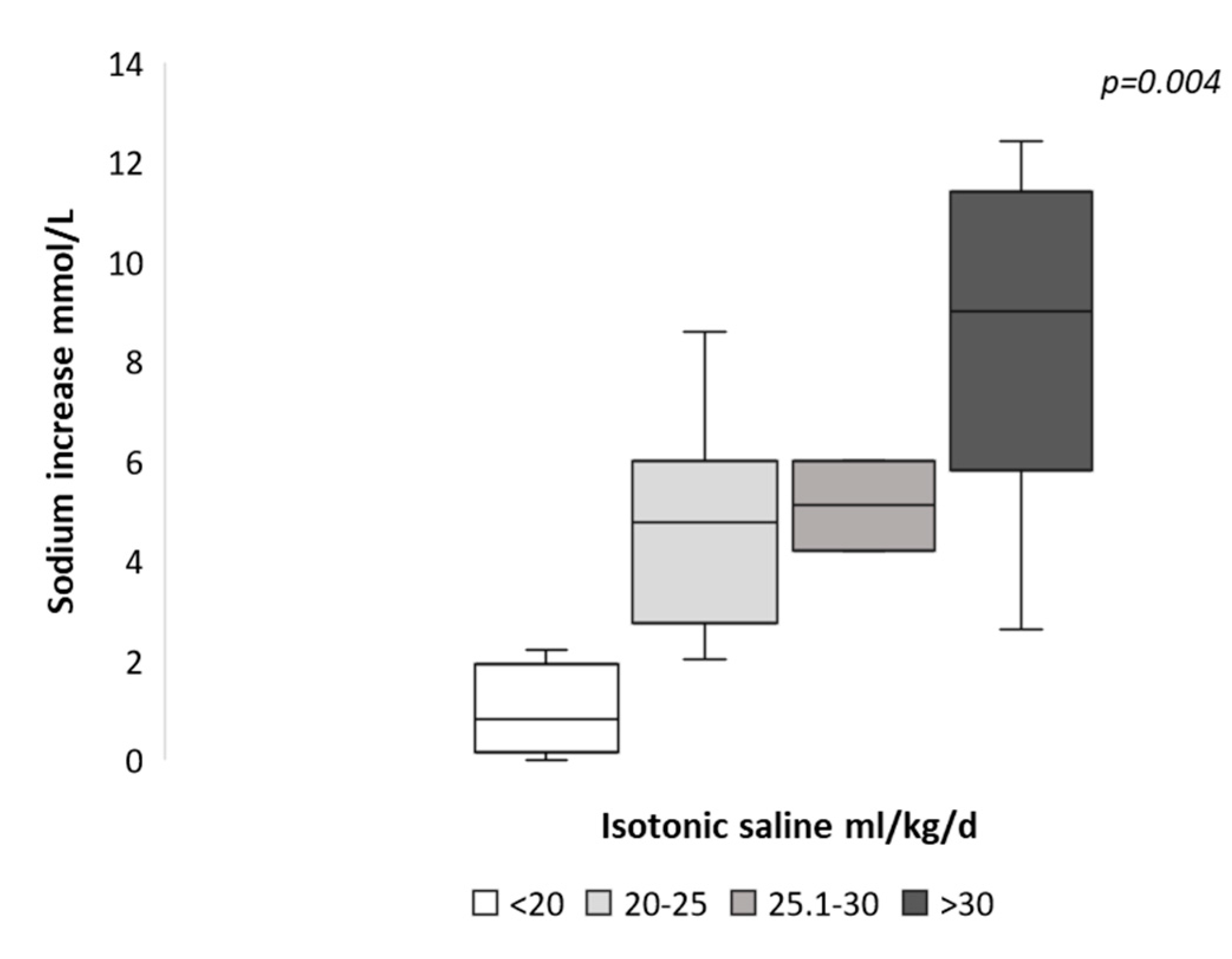
| Isotonic saline solution dose, mL/kg/24 h | 32 (29–37) | 23 (20–30) | 0.005 * | 31 (25–33) | 21 (17–29) | 0.006 * |
| Sensitivity (95% CI) | Specificity (95% CI) | Positive Predictive Value (95% CI) | Negative Predictive Value (95% CI) | Odd Ratio (95% CI) * | p * | |
|---|---|---|---|---|---|---|
| SNa ∆ ≥ 8 | ||||||
| Isotonic saline dose: | ||||||
| ≥30 mL/kg/24 h | 80% (50–100) | 80% (60–100) | 67% (36–98) | 89% (72–100) | 16 (2.5–95.1) | 0.004 * |
| ≥22 mL/kg/24 h | 100% (95–100) | 45% (21–69) | 48% (24–71) | 100% (94–100) | - | - |
| SNa ∆ ≥ 6 | ||||||
| Isotonic saline dose: | ||||||
| ≥29 mL/kg/24 h | 67% (39–94) | 80% (55–100) | 77% (50–100) | 71% (46–95) | 13 (2.2–72.1) | 0.007 * |
| ≥22 mL/kg/24 h | 100% (97–100) | 60% (32–88) | 71.4% (50–93) | 100% (94–100) | - | - |
| SNa ∆ ≥ 6 ** | ||||||
| Isotonic saline dose: ≥29 mL/kg/24 h | 73% (42–100) | 75% (46–100) | 73% (42–100) | 75% (46–100) | 8 (1.2–51.5) | 0.029 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Sánchez, J.G.; Meneses, D.; Álvarez-Escolá, C.; Cuesta, M.; Calle-Pascual, A.L.; Runkle, I. The Effect of the Dose of Isotonic Saline on the Correction of Serum Sodium in the Treatment of Hypovolemic Hyponatremia. J. Clin. Med. 2020, 9, 3567. https://doi.org/10.3390/jcm9113567
Ruiz-Sánchez JG, Meneses D, Álvarez-Escolá C, Cuesta M, Calle-Pascual AL, Runkle I. The Effect of the Dose of Isotonic Saline on the Correction of Serum Sodium in the Treatment of Hypovolemic Hyponatremia. Journal of Clinical Medicine. 2020; 9(11):3567. https://doi.org/10.3390/jcm9113567
Chicago/Turabian StyleRuiz-Sánchez, Jorge Gabriel, Diego Meneses, Cristina Álvarez-Escolá, Martin Cuesta, Alfonso Luis Calle-Pascual, and Isabelle Runkle. 2020. "The Effect of the Dose of Isotonic Saline on the Correction of Serum Sodium in the Treatment of Hypovolemic Hyponatremia" Journal of Clinical Medicine 9, no. 11: 3567. https://doi.org/10.3390/jcm9113567