Sarcopenia Index as a Predictor of Clinical Outcomes in Older Patients with Coronary Artery Disease

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
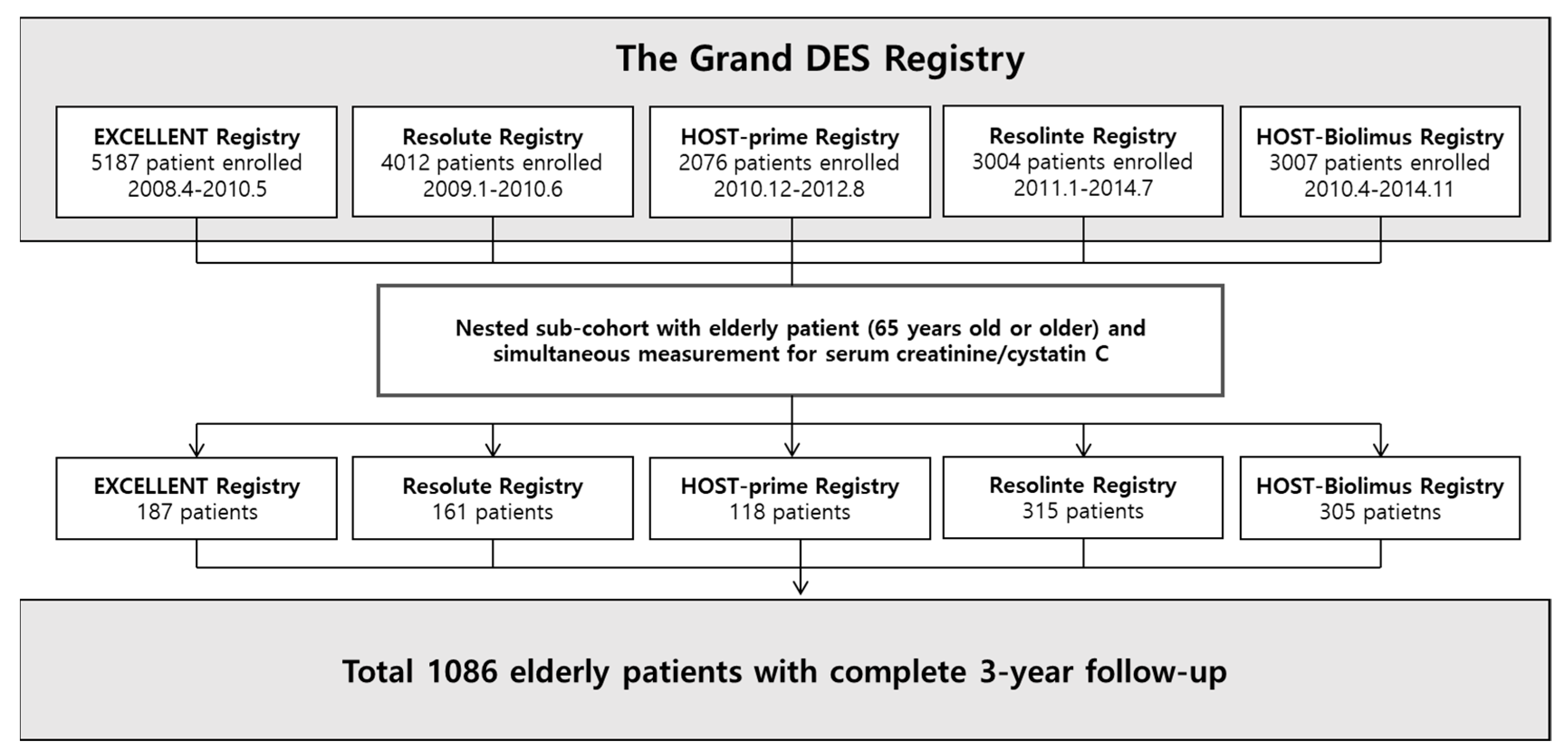
2.1. Study Population
2.2. Demographic and Laboratory Data
2.3. PCI Procedure and Follow-Up
2.4. Outcomes
2.5. Statistical Analyses
3. Results
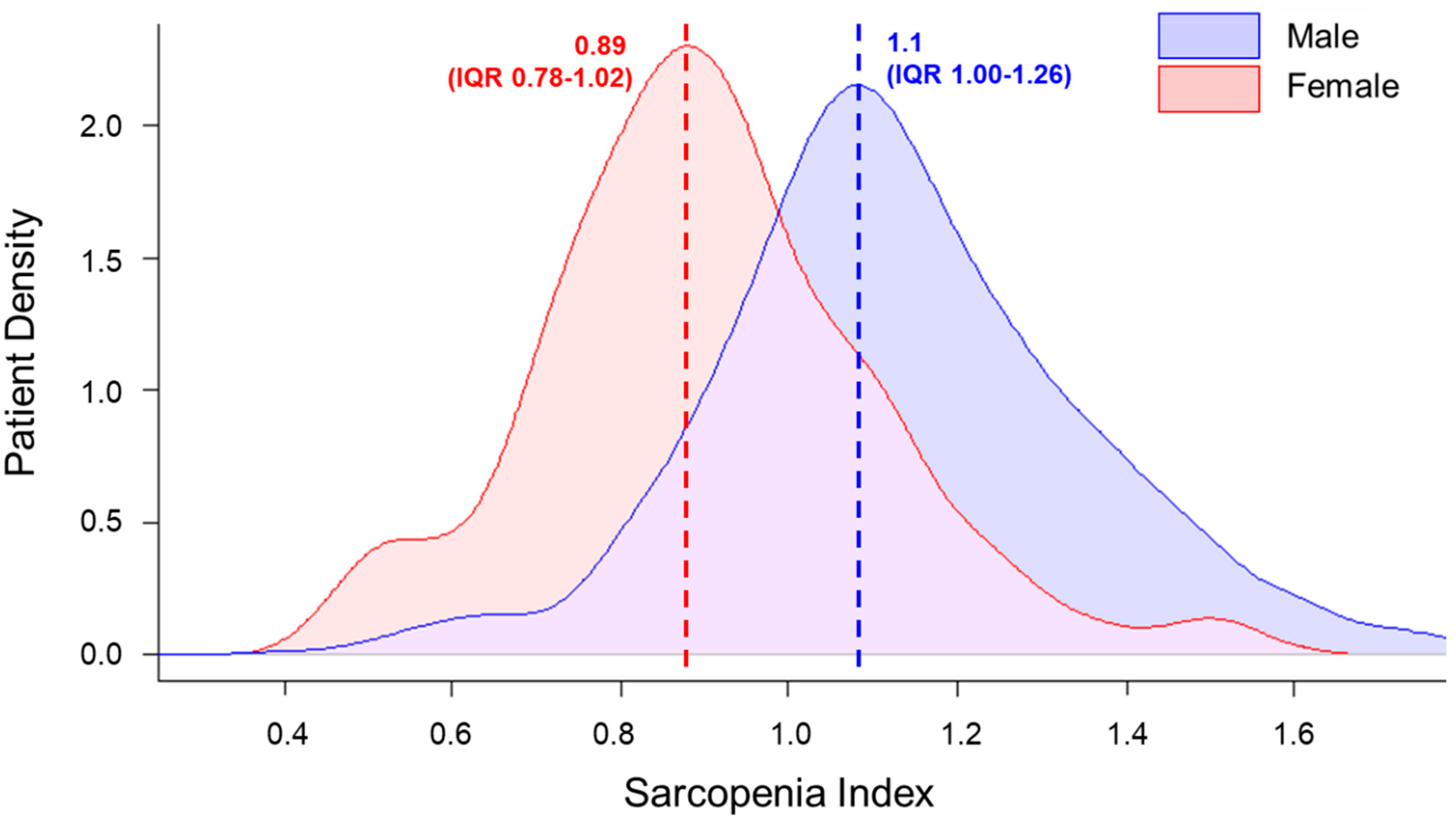
3.1. Patient Characteristics and Sarcopenia Index
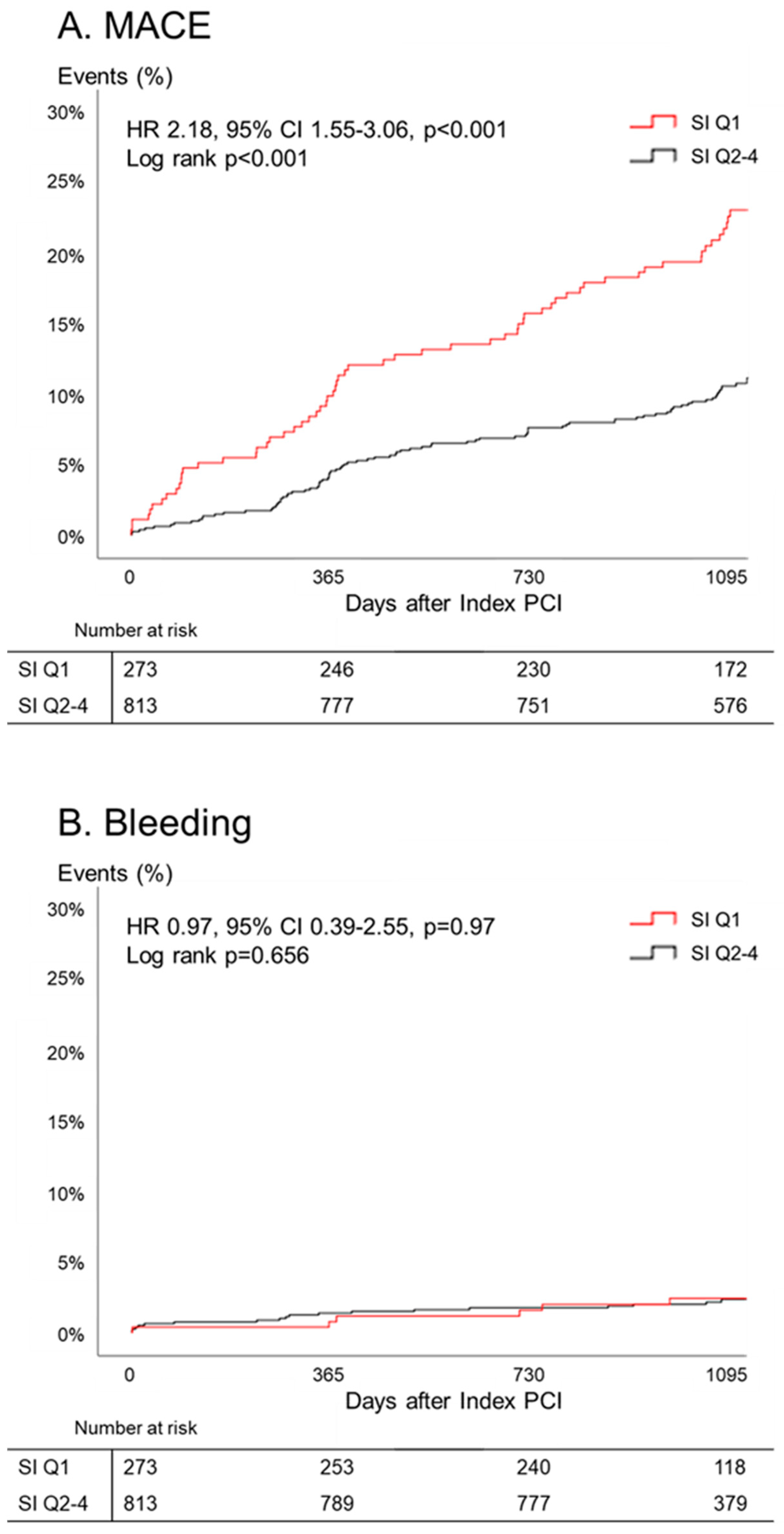
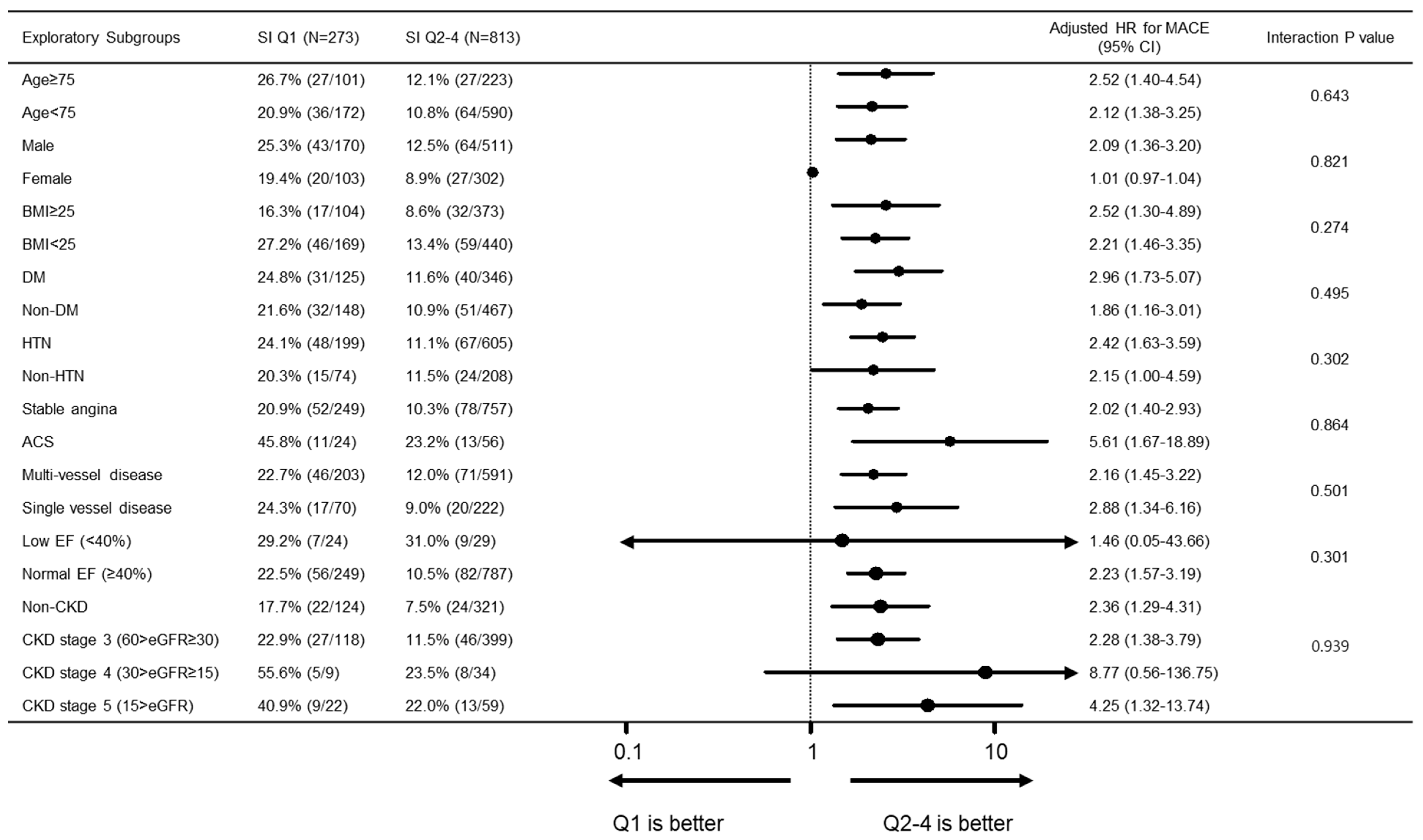
3.2. Clinical Outcomes during 3-Year Follow-Up
3.3. Additive Risk Predictive Value of Sarcopenia Index
4. Discussion
4.1. Sarcopenia Index as a Surrogate for Muscle Mass
4.2. Association between Low Sarcopenia Index and Prognosis of CAD
4.3. Potential Role of Sarcopenia Index in the Management of CAD
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Yanishi, M.; Kinoshita, H.; Tsukaguchi, H.; Kimura, Y.; Koito, Y.; Sugi, M.; Matsuda, T. The creatinine/cystatin C ratio provides effective evaluation of muscle mass in kidney transplant recipients. Int. Urol. Nephrol. 2018, 51, 79–83. [Google Scholar] [CrossRef]
- Osaka, T.; Hamaguchi, M.; Hashimoto, Y.; Ushigome, E.; Tanaka, M.; Yamazaki, M.; Fukui, M. Decreased the creatinine to cystatin C ratio is a surrogate marker of sarcopenia in patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2018, 139, 52–58. [Google Scholar] [CrossRef]
- Kashani, K.; Frazee, E.N.; Kukrálová, L.; Sarvottam, K.; Herasevich, V.; Young, P.M.; Kashyap, R.; Lieske, J.C. Evaluating Muscle Mass by Using Markers of Kidney Function. Crit. Care Med. 2017, 45, e23–e29. [Google Scholar] [CrossRef]
- Barreto, E.F.; Kanderi, T.; DiCecco, S.R.; Lopez-Ruiz, A.; Poyant, J.O.; Mara, K.C.; Heimgartner, J.; Gajic, O.; Rule, A.D.; Nystrom, E.M.; et al. Sarcopenia Index Is a Simple Objective Screening Tool for Malnutrition in the Critically Ill. J. Parenter. Enter. Nutr. 2018, 43, 780–788. [Google Scholar] [CrossRef]
- Suzuki, K.; Furuse, H.; Tsuda, T.; Masaki, Y.; Okazawa, S.; Kambara, K.; Inomata, M.; Miwa, T.; Matsui, S.; Kashii, T.; et al. Utility of creatinine/cystatin C ratio as a predictive marker for adverse effects of chemotherapy in lung cancer: A retrospective study. J. Int. Med. Res. 2015, 43, 573–582. [Google Scholar] [CrossRef] [Green Version]
- Schutten, J.C.; Neto, A.G.; Navis, G.J.; Gansevoort, R.; Bakker, S.; Kootstra-Ros, J.E.; Danel, R.M.; Goorman, F.; Gans, R.O.B.; De Borst, M.H.; et al. Lower Plasma Magnesium, Measured by Nuclear Magnetic Resonance Spectroscopy, is Associated with Increased Risk of Developing Type 2 Diabetes Mellitus in Women: Results from a Dutch Prospective Cohort Study. J. Clin. Med. 2019, 8, 169. [Google Scholar] [CrossRef] [Green Version]
- Goel, K.; Gulati, R.; Reeder, G.S.; Lennon, R.J.; Lewis, B.R.; Behfar, A.; Sandhu, G.S.; Rihal, C.S.; Singh, M. Low Body Mass Index, Serum Creatinine, and Cause of Death in Patients Undergoing Percutaneous Coronary Intervention. J. Am. Hear. Assoc. 2016, 5, e003633. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.; Park, K.W.; Ki, Y.-J.; Park, J.; Rhee, T.; Kim, C.-H.; Han, J.-K.; Yang, H.-M.; Kang, H.-J.; Koo, B.-K.; et al. Development and Validation of an Ischemic and Bleeding Risk Evaluation Tool in East Asian Patients Receiving Percutaneous Coronary Intervention. Thromb. Haemost. 2019, 119, 1182–1193. [Google Scholar] [CrossRef]
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Tamura, M.K.; Feldman, H.I. KDOQI US Commentary on the 2012 KDIGO Clinical Practice Guideline for the Evaluation and Management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Garcia, H.M.; McFadden, E.; Farb, A.; Mehran, R.; Stone, G.W.; Spertus, J.; Onuma, Y.; Morel, M.-A.; Van Es, G.-A.; Zuckerman, B.; et al. Standardized End Point Definitions for Coronary Intervention Trials: The Academic Research Consortium-2 Consensus Document. Eur. Heart J. 2018, 137, 2635–2650. [Google Scholar] [CrossRef]
- Bovill, E.G.; Terrin, M.L.; Stump, D.C.; Berke, A.D.; Frederick, M.; Collen, D.; Feit, F.; Gore, J.M.; Hillis, L.D.; Lambrew, C.T.; et al. Hemorrhagic Events during Therapy with Recombinant Tissue-Type Plasminogen Activator, Heparin, and Aspirin for Acute Myocardial Infarction. Ann. Intern. Med. 1991, 115, 256–265. [Google Scholar] [CrossRef]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia; Regional Office for the Western Pacific: Sydney, Australia, 2000. [Google Scholar]
- Stevens, L.A.; Schmid, C.H.; Greene, T.; Li, L.; Beck, G.J.; Joffe, M.M.; Froissart, M.; Kusek, J.W.; Zhang, Y.; Coresh, J.; et al. Factors other than glomerular filtration rate affect serum cystatin C levels. Kidney Int. 2009, 75, 652–660. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-W.; Jung, H.-W.; Kim, C.-H.; Kim, K.-I.; Chin, H.J.; Lee, H. A New Equation to Estimate Muscle Mass from Creatinine and Cystatin C. PLoS ONE 2016, 11, e0148495. [Google Scholar] [CrossRef]
- Kashani, K.; Sarvottam, K.; Pereira, N.L.; Barreto, E.F.; Kennedy, C.C. The sarcopenia index: A novel measure of muscle mass in lung transplant candidates. Clin. Transplant. 2018, 32, e13182. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.M.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachex Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Diago, C.A.A.; García-Unzueta, M.T.; Lavin, B.A.; Guerra, A.R.; Agüero, J.; Ramos, L.; Muñoz, P. The Ratio Serum Creatinine/Serum Cystatin C (a Surrogate Marker of Muscle Mass) as a Predictor of Hospitalization in Chronic Obstructive Pulmonary Disease Outpatients. Respiration 2018, 97, 302–309. [Google Scholar] [CrossRef]
- Ko, B.-J.; Chang, Y.; Jung, H.S.; Yun, K.E.; Kim, C.-W.; Park, H.S.; Chung, E.C.; Shin, H.; Ryu, S. Relationship Between Low Relative Muscle Mass and Coronary Artery Calcification in Healthy Adults. Arter. Thromb. Vasc. Boil. 2016, 36, 1016–1021. [Google Scholar] [CrossRef] [Green Version]
- Campos, A.M.; Moura, F.A.; Santos, S.N.; Freitas, W.M.; Sposito, A.C. Sarcopenia, but not excess weight or increased caloric intake, is associated with coronary subclinical atherosclerosis in the very elderly. Atherosclerosis 2017, 258, 138–144. [Google Scholar] [CrossRef]
- Gonçalves, P.; Ferreira, J.; Aguiar, C.; Seabra-Gomes, R. TIMI, PURSUIT, and GRACE Risk Scores: Sustained Prognostic Value and Interaction with Revascularization in NSTE-ACS. ACC Curr. J. Rev. 2005, 14, 4. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2019, 41, 407–477. [Google Scholar] [CrossRef]
- Rolland, Y.; Czerwinski, S.; Van Kan, G.A.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [Green Version]
- Clegg, A.P.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K.; Iliffe, S. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Landi, F.; Vellas, B.; Bernabei, R.; Marzetti, E. Sarcopenia and Physical Frailty: Two Sides of the Same Coin. Front. Aging Neurosci. 2014, 6. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Nobili, A.; Vitale, G. Frailty and sarcopenia: From theory to clinical implementation and public health relevance. Eur. J. Intern. Med. 2016, 35, 1–9. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Faculty Opinions recommendation of Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: Cochrane Systematic Review and Meta-Analysis. Facial Opin. Post Publ. Peer Rev. Biomed. Lit. 2016, 67, 1–12. [Google Scholar] [CrossRef]
- Lawler, P.R.; Filion, K.B.; Eisenberg, M.J. Efficacy of exercise-based cardiac rehabilitation post–myocardial infarction: A systematic review and meta-analysis of randomized controlled trials. Am. Heart J. 2011, 162, 571–584. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (N = 1086) | SI Q1 (N = 273) | SI Q2–4 (N = 813) | p Value |
|---|---|---|---|---|
| SI | 1.05 ± 0.24 | 0.79 ± 0.15 | 1.13 ± 0.21 | <0.001 |
| Age, years | 72.3 ± 5.4 | 73.5 ± 6.1 | 71.9 ± 5.1 | <0.001 |
| BMI, kg/m2 | 24.62 ± 2.95 | 24.2 ± 3.0 | 24.7 ± 2.9 | 0.013 |
| Male | 681 (62.7%) | 170 (62.3%) | 511 (62.9%) | 0.863 |
| Diabetes mellitus | 471 (43.4%) | 125 (45.8%) | 346 (42.6%) | 0.352 |
| Hypertension | 804 (74.0%) | 199 (72.9%) | 605 (74.4%) | 0.620 |
| Dyslipidemia | 801 (73.8%) | 196 (71.8%) | 605 (74.4%) | 0.394 |
| Chronic kidney disease | 68 (6.3%) | 20 (7.3%) | 48 (5.9%) | 0.401 |
| Prior stroke | 116 (10.7%) | 28 (10.3%) | 88 (10.8%) | 0.793 |
| Peripheral vessel disease | 40 (3.7%) | 13 (4.8%) | 27 (3.3%) | 0.274 |
| Current smoker | 154 (14.2%) | 42 (15.4%) | 112 (13.8%) | 0.510 |
| Prior myocardial infarction | 95 (8.8%) | 28 (10.3%) | 67 (8.2%) | 0.308 |
| Prior congestive heart failure | 30 (2.8%) | 9 (3.3%) | 21 (2.6%) | 0.534 |
| LVEF, % | 59.3 ± 9.7 | 57.7 ± 12.0 | 59.8 ± 8.7 | 0.004 |
| LV dysfunction (EF < 40%) | 53 (4.9%) | 24 (8.4%) | 29 (3.6%) | 0.001 |
| Prior percutaneous coronary intervention | 211 (19.4%) | 54 (19.8%) | 157 (19.3%) | 0.865 |
| Prior coronary bypass surgery | 54 (5.0%) | 16 (5.9%) | 38 (4.7%) | 0.435 |
| Prior revascularization | 238 (21.9%) | 60 (22.0%) | 178 (21.9%) | 0.977 |
| Family history of CAD | 105 (9.7%) | 19 (7.0%) | 86 (10.6%) | 0.080 |
| Presentations | ||||
| Stable angina | 743 (68.4%) | 167 (61.2%) | 576 (70.8%) | 0.026 |
| Unstable angina | 214 (19.7%) | 64 (23.4%) | 150 (18.5%) | |
| NSTEMI | 50 (4.6%) | 13 (4.8%) | 37 (4.6%) | |
| STEMI | 30 (2.8%) | 11 (4.0%) | 19 (2.3%) | |
| Silent ischemia | 49 (4.5%) | 18 (6.6%) | 31 (3.8%) | |
| Angiographic findings | ||||
| Extent of angiographic disease | ||||
| 1VD | 292 (26.9%) | 70 (25.6%) | 222 (27.3%) | 0.787 |
| 2VD | 382 (35.2%) | 95 (34.8%) | 287 (35.3%) | |
| 3VD | 412 (37.9%) | 108 (39.6%) | 304 (37.4%) | |
| Left main disease | 123 (11.3%) | 24 (8.8%) | 99 (12.2%) | 0.127 |
| At least 1 bifurcation | 666 (61.3%) | 166 (60.8%) | 500 (61.5%) | 0.838 |
| At least 1 long lesion | 433 (44.3%) | 121 (44.3%) | 312 (38.4%) | 0.083 |
| At least 1 small vessel | 605 (55.7%) | 163 (59.7%) | 442 (54.4%) | 0.124 |
| Stent number | 1.8 ± 1.1 | 1.9 ± 1.1 | 1.8 ± 1.1 | 0.09 |
| Total stent length, mm | 44.7 ± 39.9 | 47.0 ± 30.1 | 44.0 ± 29.8 | 0.141 |
| Clinical Outcomes | Total (N = 1086) | SI Q1 (N = 273) | SI Q2–4 (N = 813) | Unadjusted HR (95% CI) | p Value | Adjusted HR *(95% CI) | p Value |
|---|---|---|---|---|---|---|---|
| MACE | 154 (14.2%) | 63 (23.1%) | 91 (11.2%) | 2.23 (1.62–3.07) | <0.001 | 2.18 (1.55–3.06) | <0.001 |
| All-cause death | 81 (7.5%) | 43 (15.8%) | 38 (4.7%) | 3.60 (2.33–5.57) | <0.001 | 3.48 (2.17–5.58) | <0.001 |
| Cardiovascular death | 43 (4.0%) | 23 (8.4%) | 20 (2.5%) | 3.64 (2.00–6.63) | <0.001 | 3.02 (1.61–5.68) | 0.001 |
| Non-cardiovascular death | 38 (3.5%) | 20 (7.3%) | 18 (2.2%) | 3.55 (1.88–6.71) | <0.001 | 3.69 (1.89–7.23) | <0.001 |
| MI | 15 (1.4%) | 4 (1.5%) | 11 (1.4%) | 1.15 (0.37–3.61) | 0.81 | 1.16 (0.35-3.81) | 0.81 |
| Target lesion revascularization | 128 (11.8%) | 29 (10.6%) | 99 (12.2%) | 0.91 (0.60–1.38) | 0.67 | 0.96 (0.63–1.46) | 0.96 |
| All bleeding | 25 (2.3%) | 7 (2.6%) | 18 (2.2%) | 1.22 (0.51–2.92) | 0.66 | 0.97 (0.37–2.55) | 0.97 |
| Model 1. SS | Model 2. SS + Age | Model 3. SS + SI | Model 4. SS + Age + SI | |
|---|---|---|---|---|
| C statistics (95% CI) | 0.49 (0.43–0.56) | 0.56 (0.49–0.63) | 0.60 (0.53–0.68) | 0.62 (0.55–0.69) |
| p value | Reference * | <0.001 | <0.001 | <0.001 |
| NRI (95% CI), Continuous | 0.076 (−0.074–0.185) | 0.144 (−0.026–0.265) | 0.102 (0.015–0.284) | |
| p value | 0.312 | 0.106 | 0.020 | |
| IDI (95% CI) | 0.010 (0.000–0.043) | 0.016 (0.000–0.067) | 0.023 (0.001–0.086) | |
| p value | 0.073 | 0.060 | 0.007 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.S.; Park, K.W.; Kang, J.; Ki, Y.-J.; Chang, M.; Han, J.-K.; Yang, H.-M.; Kang, H.-J.; Koo, B.-K.; Kim, H.-S. Sarcopenia Index as a Predictor of Clinical Outcomes in Older Patients with Coronary Artery Disease. J. Clin. Med. 2020, 9, 3121. https://doi.org/10.3390/jcm9103121
Lee HS, Park KW, Kang J, Ki Y-J, Chang M, Han J-K, Yang H-M, Kang H-J, Koo B-K, Kim H-S. Sarcopenia Index as a Predictor of Clinical Outcomes in Older Patients with Coronary Artery Disease. Journal of Clinical Medicine. 2020; 9(10):3121. https://doi.org/10.3390/jcm9103121
Chicago/Turabian StyleLee, Hak Seung, Kyung Woo Park, Jeehoon Kang, You-Jeong Ki, Mineok Chang, Jung-Kyu Han, Han-Mo Yang, Hyun-Jae Kang, Bon-Kwon Koo, and Hyo-Soo Kim. 2020. "Sarcopenia Index as a Predictor of Clinical Outcomes in Older Patients with Coronary Artery Disease" Journal of Clinical Medicine 9, no. 10: 3121. https://doi.org/10.3390/jcm9103121