Cardiogenic Shock Clinical Presentation, Management, and In-Hospital Outcomes in Patients Admitted to the Acute Cardiac Care Unit of a Tertiary Hospital: Does Gender Play a Role?

 ,
,
Abstract
:1. Introduction
2. Material and Methods
Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Clinical Presentation
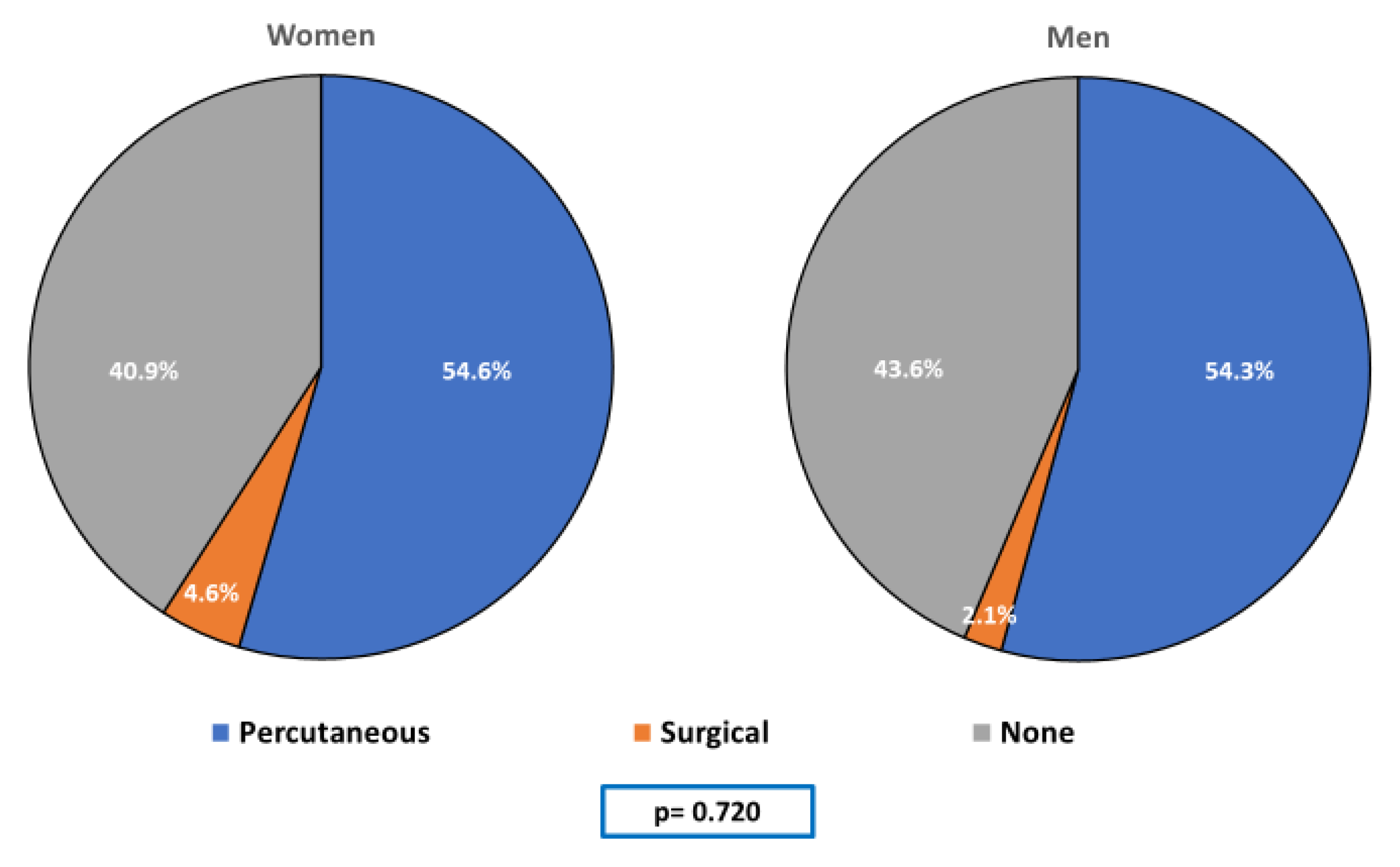
3.3. Therapeutic Management
3.4. In-Hospital Prognosis
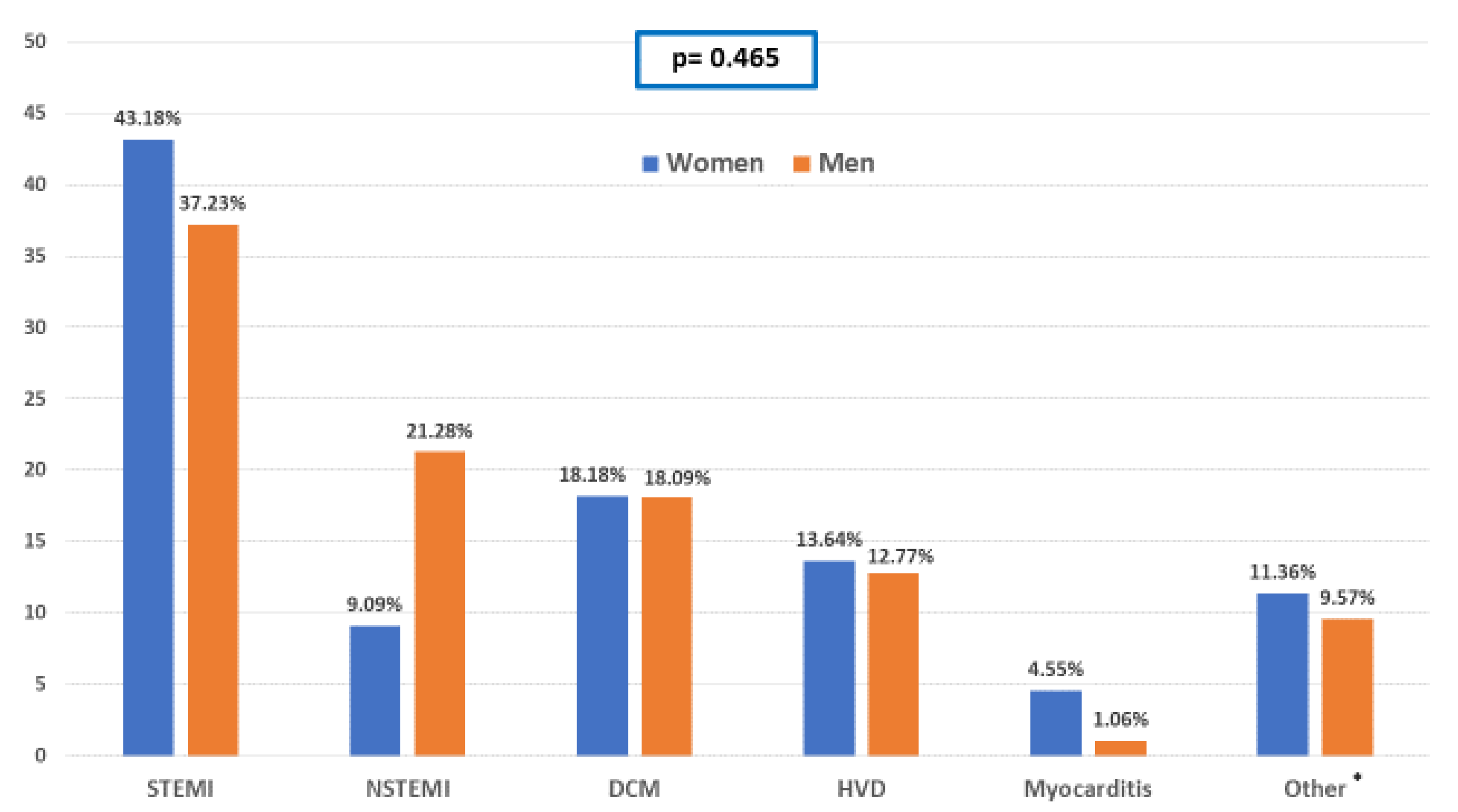
3.5. AMI-Related Episodes of CS
3.6. Non-AMI-Related Episodes of CS
3.7. Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vahdatpour, C.; Collins, D.; Goldberg, S. Cardiogenic Shock. J. Am. Heart Assoc. 2019, 8, e011991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary management of cardiogenic shock: A scientific statement from de American Heart Association. Circulation 2017, 136, e232–e268. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Ohman, E.M.; De Waha-Thiele, S.; Zeymer, U.; Desch, S. Management of cardiogenic shock complicating myocardial infarction: An update 2019. Eur. Heart J. 2019, 40, 2671–2683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Dzavik, V.; Buller, C.E.; Aylward, P.; Col, J.; White, H.D.; SHOCK Investigators. Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction. JAMA 2006, 295, 2511–2515. [Google Scholar] [CrossRef] [Green Version]
- Aissaoui, N.; Puymirat, E.; Tabone, X.; Charbonnier, B.; Schiele, F.; Lefevre, T.; Durand, E.; Blanchard, D.; Simon, T.; Cambou, J.-P.; et al. Improved outcome of cardiogenic shock at the acute stage of myocardial infarction: A report from the USIK 1995, USIC 2000, and FAST-MI French nationwide registries. Eur. Heart J. 2012, 33, 2535–2543. [Google Scholar] [CrossRef]
- Rathod, K.S.; Koganti, S.; Iqbal, M.B.; Jain, A.K.; Kalra, S.S.; Astroulakis, Z.; Lim, P.; Rakhit, R.; Dalby, M.C.; Lockie, T.; et al. Contemporary trends in cardiogenic shock: Incidence, intra-aortic balloon pump utilisation and outcomes from the London Heart Attack Group. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 16–27. [Google Scholar] [CrossRef]
- Thiele, H.; Akin, I.; Sandri, M.; Fuernau, G.; De Waha, S.; Meyer-Saraei, R.; Nordbeck, P.; Geisler, T.; Landmesser, U.; Skurk, C.; et al. PCI strategies in patients with acute myocardial infarction and cardiogenic shock. N. Engl. J. Med. 2017, 377, 2419–2432. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.; Mulvagh, S.L.; Merz, C.N.; Buring, J.E.; Manson, J.E. Cardiovascular Disease in Women: Clinical Perspectives. Circ. Res. 2016, 118, 1273–1293. [Google Scholar] [CrossRef]
- Liakos, M.; Parikh, P.B. Gender Disparities in Presentation, Management, and Outcomes of Acute Myocardial Infarction. Curr. Cardiol. Rep. 2018, 20, 64. [Google Scholar] [CrossRef]
- Wong, S.C.; Sleeper, L.A.; Monrad, E.S.; Menegus, M.A.; Palazzo, A.; Dzavik, V.; Jacobs, A.; Jiang, X.; Hochman, J.S.; SHOCK Investigators. Absence of gender differences in clinical outcomes in patients with cardiogenic shock complicating acute myocardial infarction. A report from the SHOCK Trial Registry. J. Am. Coll. Cardiol. 2001, 38, 1395–1401. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Joseph, S.M.; Brisco, M.A.; Colvin, M.; Grady, K.L.; Walsh, M.N.; Cook, J.L.; GenVAD Working Group. Women with Cardiogenic Shock Derive Greater Benefit From Early Mechanical Circulatory Support: An Update From the cVAD Registry. J. Interv. Cardiol. 2016, 29, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Blomkalns, A.L.; Chen, A.Y.; Hochman, J.S.; Peterson, E.D.; Trynosky, K.; Diercks, D.B.; Brogan, G.X., Jr.; Boden, W.E.; Roe, M.T.; Ohman, E.M.; et al. Gender disparities in the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: Large-scale observations from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the American College of Cardiology/American Heart Association Guidelines) National Quality Improvement Initiative. J. Am. Coll. Cardiol. 2005, 45, 832–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glaser, R.; Herrmann, H.C.; Murphy, S.A.; Demopoulos, L.A.; DiBattiste, P.M.; Cannon, C.P.; Braunwald, E. Benefit of an early invasive management strategy in women with acute coronary syndromes. JAMA 2002, 288, 3124–3129. [Google Scholar] [CrossRef] [Green Version]
- Gharacholou, S.M.; Alexander, K.P.; Chen, A.Y.; Wang, T.Y.; Melloni, C.; Gliber, W.B.; Pollack, C.V., Jr.; Ohman, E.M.; Peterson, E.D.; Roe, M.T. Implications and reasons for the lack of use of reperfusion therapy in patients with ST-segment elevation myocardial infarction: Findings from the CRUSADE initiative. Am. Heart J. 2010, 159, 757–763. [Google Scholar] [CrossRef]
- Habal, M.V.; Axsom, K.; Farr, M. Advanced Therapies for Advanced Heart Failure in Women. Heart Fail. Clin. 2019, 15, 97–107. [Google Scholar] [CrossRef]
- Abrahamyan, L.; Sahakyan, Y.; Wijeysundera, H.C.; Krahn, M.; Rac, V.E. Gender Differences in Utilization of Specialized Heart Failure Clinics. J. Womens Health 2018, 27, 623–629. [Google Scholar] [CrossRef]
- Hopper, I.; Kotecha, D.; Chin, K.L.; Mentz, R.J.; Von Lueder, T.G. Comorbidities in Heart Failure: Are There Gender Differences? Curr. Heart Fail. Rep. 2016, 13, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Fengler, K.; Fuernau, G.; Desch, S.; Eitel, I.; Neumann, F.J.; Olbrich, H.G.; De Waha, A.; De Waha, S.; Richardt, G.; Hennersdorf, M.; et al. Gender differences in patients with cardiogenic shock complicating myocardial infarction: A substudy of the IABP-SHOCK II-trial. Clin. Res. Cardiol. 2015, 104, 71–78. [Google Scholar] [CrossRef]
- Isorni, M.A.; Aissaoui, N.; Angoulvant, D.; Bonello, L.; Lemesle, G.; Delmas, C.; Henry, P.; Schiele, F.; Ferrières, J.; Simon, T.; et al. Temporal trends in clinical characteristics and management according to sex in patients with cardiogenic shock after acute myocardial infarction: The FAST-MI programme. Arch. Cardiovasc. Dis. 2018, 111, 555–563. [Google Scholar] [CrossRef]
- Kolte, D.; Khera, S.; Aronow, W.S.; Mujib, M.; Palaniswamy, C.; Sule, S.; Jain, D.; Gotsis, W.; Ahmed, A.; Frishman, W.H.; et al. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States. J. Am. Heart Assoc. 2014, 3, e000590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collado-Lledó, E.; Llaó, I.; Rivas-Lasarte, M.; González-Fernández, V.; Noriega, F.J.; Hernández-Pérez, F.J.; Alegre, O.; Sionis, A.; Lidón, R.M.; Viana-Tejedor, A.; et al. Clinical picture, management and risk stratification in patients with cardiogenic shock: Does gender matter? BMC Cardiovasc. Disord. 2020, 20, 189. [Google Scholar] [CrossRef] [PubMed]
- Kunadian, V.; Qiu, W.; Bawamia, B.; Veerasamy, M.; Jamieson, S.; Zaman, A. Gender comparisons in cardiogenic shock during ST elevation myocardial infarction treated by primary percutaneous coronary intervention. Am. J. Cardiol. 2013, 112, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Qadir, H.M.; Ivanov, J.; Austin, P.C.; Tu, J.V.; Džavík, V. Sex differences in the management and outcomes of Ontario patients with cardiogenic shock complicating acute myocardial infarction. Can. J. Cardiol. 2013, 29, 691–696. [Google Scholar] [CrossRef] [Green Version]
- Anderson, M.L.; Peterson, E.D.; Peng, S.A.; Wang, T.Y.; Ohman, E.M.; Bhatt, D.L.; Saucedo, J.F.; Roe, M.T. Differences in the profile, treatment, and prognosis of patients with cardiogenic shock by myocardial infarction classification: A report from NCDR. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 708–715. [Google Scholar] [CrossRef] [Green Version]
- Huded, C.P.; Johnson, M.; Kravitz, K.; Menon, V.; Abdallah, M.; Gulett, T.C.; Hantz, S.; Ellis, S.G.; Podolsky, S.R.; Meldon, S.W.; et al. 4-Step Protocol for Disparities in STEMI Care and Outcomes in Women. J. Am. Coll. Cardiol. 2018, 71, 2122–2132. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Women (n = 44) | Men (n = 94) | p Value | |
|---|---|---|---|
| Age (years) | 75.96 (11.33) | 70.81 (12.09) | 0.019 |
| Smoking history | 13 (29.55%) | 61 (64.89%) | 0.001 |
| Hypertension | 34 (77.27%) | 58 (61.70%) | 0.071 |
| Dyslipidaemia | 23 (52.27%) | 49 (52.13%) | 0.987 |
| Diabetes | 16 (36.36%) | 39 (41.49%) | 0.567 |
| BMI | 26.63 (0.759) | 25.91 (0.373) | 0.341 |
| COPD | 1 (2.27%) | 11 (11.70%) | 0.067 |
| CKD | 6 (13.64%) | 21 (22.34%) | 0.230 |
| Previous MI | 4 (9.30%) | 27 (28.72%) | 0.012 |
| Heart failure | 8 (19.05%) | 29 (30.85%) | 0.153 |
| Stroke | 3 (6.82%) | 5 (5.32%) | 0.725 |
| Peripheral arteriopathy | 2 (4.55%) | 13 (13.83%) | 0.102 |
| Women | Men | p Value | |
|---|---|---|---|
| Mental confusion | 47.73% | 47.87% | 0.987 |
| Cold distal extremities | 70.45% | 68.09% | 0.779 |
| Systolic blood pressure at admission (mmHg) | 88.84 | 91.16 | 0.576 |
| Diastolic blood pressure at admission (mmHg) | 54.66 | 52.20 | 0.390 |
| Heart rate at admission (bpm) | 92.02 | 91.02 | 0.824 |
| Lactate levels at admission (mmol/L) | 5.95 | 5.48 | 0.539 |
| Creatinine levels at admission (µmol/L) | 145.32 | 165.45 | 0.285 |
| Estimated glomerular filtrate rate at admission (mL/min) | 39.57 | 46.85 | 0.156 |
| Acute kidney disease at admission | 81.8 | 78.7 | 0.674 |
| LVEF | 33.57% | 28.42% | 0.037 |
| Sudden cardiac arrest during hospitalization | 24.47% | 15.91% | 0.256 |
| Length of stay (days) | 15.23 | 13.86 | 0.851 |
| Women | Men | p Value | |
|---|---|---|---|
| Dobutamine | 38.64% | 74.47% | 0.001 |
| Noradrenaline | 88.64% | 97.87% | 0.021 |
| Levosimendan | 6.82% | 22.34% | 0.025 |
| Adrenaline | 9.09% | 14.89% | 0.346 |
| Dopamine | 22.73% | 12.77% | 0.136 |
| Invasive mechanical ventilation | 47.73% | 56.38% | 0.342 |
| Non-invasive mechanical ventilation | 13.64% | 12.77% | 0.887 |
| Renal replacement therapy | 11.36% | 20.21% | 0.201 |
| Swan Ganz catheter placement | 9.09% | 3.19% | 0.141 |
| Any mechanical circulatory support | 68.18% | 59.57% | 0.331 |
| IABP | 29.55% | 37.23% | 0.377 |
| ECMO | 2.27% | 4.26% | 0.561 |
| Impella® | 0.00% | 5.32% | 0.119 |
| Levitronix Centrimag® | 2.27% | 2.13% | 0.957 |
| In-hospital mortality rate | 47.73% | 47.87% | 0.987 |
| Cardiovascular cause of death | 85.71% | 79.55% | 0.549 |
| Odds Ratio | 95% Confidence Interval | p Value | |
|---|---|---|---|
| Gender (male) | 1.11 | 0.44–2.83 | 0.814 |
| Age * | 1.06 | 1.03–1.11 | 0.001 |
| Previous MI | 0.81 | 0.31–2.10 | 0.660 |
| Dobutamine use | 1.80 | 0.74–4.38 | 0.196 |
| Noradrenaline use | 4.09 | 0.40–41.73 | 0.235 |
| LEVF ** | 0.99 | 0.96–1.02 | 0.480 |
| Lactate levels at admission (mmol/L) *** | 1.18 | 1.07–1.30 | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jerónimo, A.; Ferrández-Escarabajal, M.; Ferrera, C.; Noriega, F.J.; Diz-Díaz, J.; Fernández-Jiménez, R.; McInerney, A.; Fernández-Ortiz, A.; Viana-Tejedor, A. Cardiogenic Shock Clinical Presentation, Management, and In-Hospital Outcomes in Patients Admitted to the Acute Cardiac Care Unit of a Tertiary Hospital: Does Gender Play a Role? J. Clin. Med. 2020, 9, 3117. https://doi.org/10.3390/jcm9103117
Jerónimo A, Ferrández-Escarabajal M, Ferrera C, Noriega FJ, Diz-Díaz J, Fernández-Jiménez R, McInerney A, Fernández-Ortiz A, Viana-Tejedor A. Cardiogenic Shock Clinical Presentation, Management, and In-Hospital Outcomes in Patients Admitted to the Acute Cardiac Care Unit of a Tertiary Hospital: Does Gender Play a Role? Journal of Clinical Medicine. 2020; 9(10):3117. https://doi.org/10.3390/jcm9103117
Chicago/Turabian StyleJerónimo, Adrian, Marcos Ferrández-Escarabajal, Carlos Ferrera, Francisco J. Noriega, Jesús Diz-Díaz, Rodrigo Fernández-Jiménez, Angela McInerney, Antonio Fernández-Ortiz, and Ana Viana-Tejedor. 2020. "Cardiogenic Shock Clinical Presentation, Management, and In-Hospital Outcomes in Patients Admitted to the Acute Cardiac Care Unit of a Tertiary Hospital: Does Gender Play a Role?" Journal of Clinical Medicine 9, no. 10: 3117. https://doi.org/10.3390/jcm9103117