Hypoxemia Index Associated with Prehospital Intubation in COVID-19 Patients

 , , and
, , and
Abstract
:1. Background
2. Methods
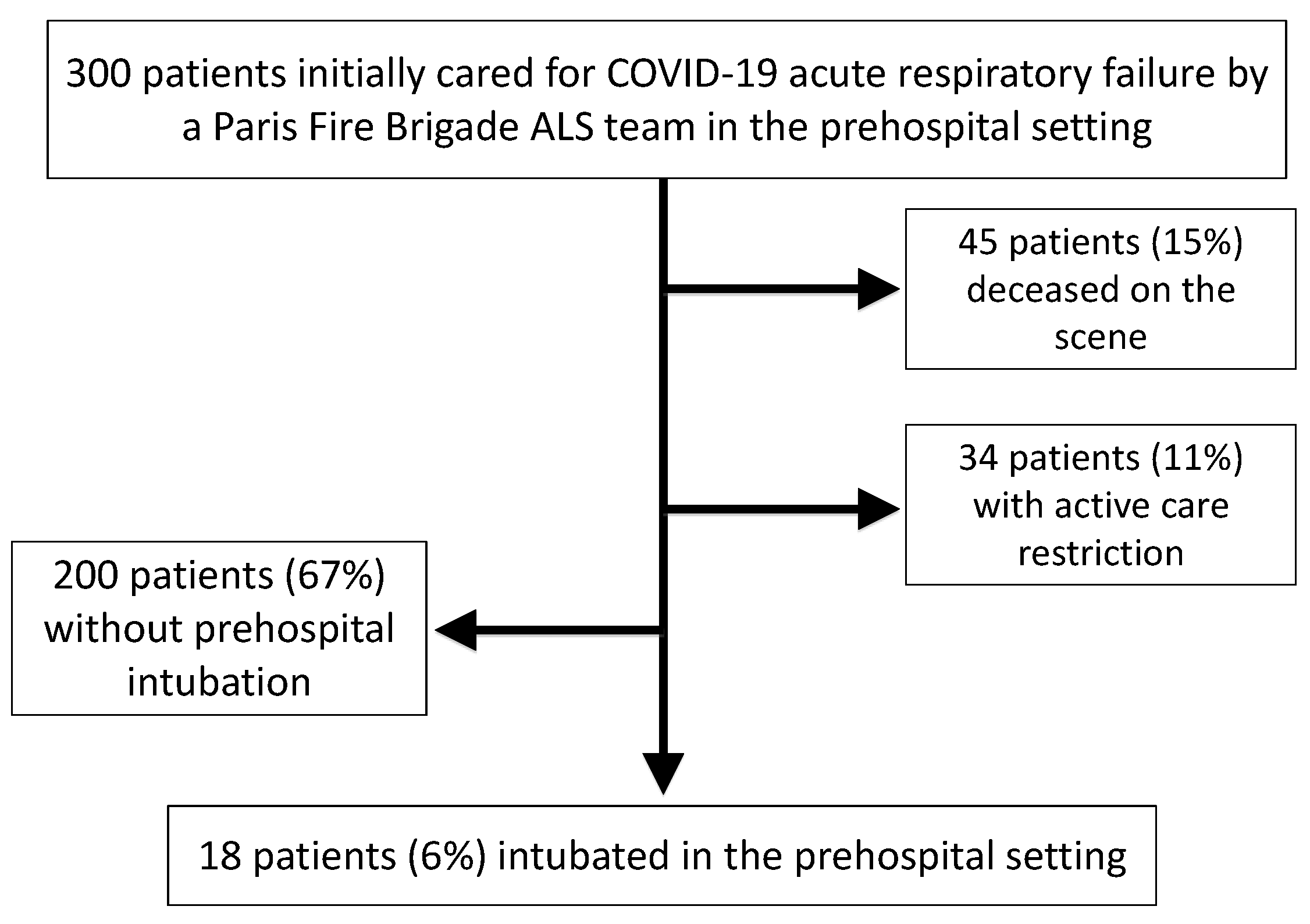
2.1. Design, Setting, and Participants
2.2. Ethical Considerations
2.3. Data Collection
2.4. Statistical Analyses
3. Results
3.1. Study Characteristics
3.2. Main Measurements
3.3. Propensity Score Matching Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bogoch, I.I.; Watts, A.; Thomas-Bachli, A.; Huber, C.; Kraemer, M.U.G.; Khan, K. Potential for Global Spread of a Novel Coronavirus from China. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Bogoch, I.I.; Watts, A.; Thomas-Bachli, A.; Huber, C.; Kraemer, M.U.G.; Khan, K. Pneumonia of Unknown Aetiology in Wuhan, China: Potential for International Spread via Commercial Air Travel. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Stratton, C.W.; Tang, Y.W. The Wuhan SARS-CoV-2-What’s Next for China. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.; Stratton, C.W.; Tang, Y.W. Outbreak of Pneumonia of Unknown Etiology in Wuhan, China: The Mystery and the Miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 20 May 2020).
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Rajgor, D.D.; Lee, M.H.; Archuleta, S.; Bagdasarian, N.; Quek, S.C. The Many Estimates of the COVID-19 Case Fatality Rate. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the Severity of Coronavirus Disease 2019: A Model-Based Analysis. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020. [Google Scholar] [CrossRef]
- Rothan, H.A.; Byrareddy, S.N. The Epidemiology and Pathogenesis of Coronavirus Disease (COVID-19) Outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef]
- Jouffroy, R.; Jost, D.; Prunet, B. Prehospital Pulse Oximetry: A Red Flag for Early Detection of Silent Hypoxemia in COVID-19 Patients. Crit. Care 2020, 24, 313. [Google Scholar] [CrossRef]
- Dhont, S.; Derom, E.; Van Braeckel, E.; Depuydt, P.; Lambrecht, B.N. The Pathophysiology of ‘Happy’ Hypoxemia in COVID-19. Respir. Res. 2020, 21, 198. [Google Scholar] [CrossRef] [PubMed]
- Berger, T.; Green, J.; Horeczko, T.; Hagar, Y.; Garg, N.; Suarez, A.; Panacek, E.; Shapiro, N. Shock Index and Early Recognition of Sepsis in the Emergency Department: Pilot Study. West J. Emerg. Med. 2013, 14, 168–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travers, S.; Jost, D.; Gillard, Y.; Lanoe, V.; Bignand, M.; Domanski, L.; Tourtier, J.P. Out-of-Hospital Cardiac Arrest Phone Detection: Those who Most Need Chest Compressions are the Most Difficult to Recognize. Resuscitation 2014, 85, 1720–1725. [Google Scholar] [CrossRef] [PubMed]
- Orso, D.; Federici, N.; Copetti, R.; Vetrugno, L.; Bove, T. Infodemic and the Spread of Fake News in the COVID-19-Era. Eur. J. Emerg. Med. 2020, 27, 327–328. [Google Scholar] [CrossRef]
- Adnet, F.; Lapostolle, F. International EMS Systems: France. Resuscitation 2004, 63, 7–9. [Google Scholar] [CrossRef]
- Gearing, R.E.; Mian, I.A.; Barber, J.; Ickowicz, A. A Methodology for Conducting Retrospective Chart Review Research in Child and Adolescent Psychiatry. J. Can. Acad. Child. Adolesc. Psychiatry 2006, 15, 126–134. [Google Scholar]
- Youden, W.J. Index for Rating Diagnostic Tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biom. Sept. 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F. Obesity in Patients Younger than 60 Years is a Risk Factor for Covid-19 Hospital Admission. Clin. Infect. Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef] [Green Version]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M. High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring Invasive Mechanical Ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef]
- Vink, E.E.; Bakker, J. Practical Use of Lactate Levels in the Intensive Care. J. Intensive Care Med. 2018, 33, 159–165. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, P.C. Balance Diagnostics for Comparing the Distribution of Baseline Covariates between Treatment Groups in Propensity-Score Matched Samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greene, K.E.; Peters, J.I. Pathophysiology of Acute Respiratory Failure. Clin. Chest Med. 1994, 15, 1–12. [Google Scholar] [PubMed]
- Pandor, A.; Thokala, P.; Goodacre, S.; Poku, E.; Stevens, J.W.; Ren, S.; Cantrell, A.; Perkins, G.D.; Ward, M.; Penn-Ashman, J. Prehospital Non-Invasive Ventilation for Acute Respiratory Failure: A Systematic Review and Cost-Effectiveness Evaluation. Health Technol. Assess. 2015, 19, 1–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence in collaboration with NHS England and NHS Improvement. Managing COVID-19 Symptoms (Including at the End of Life) in the Community: Summary of NICE Guidelines. BMJ 2020, 369, m1461. [Google Scholar] [CrossRef] [Green Version]
- Rome, B.N.; Avorn, J. Drug Evaluation During the Covid-19 Pandemic. N. Engl. J. Med. 2020, 382, 2282–2284. [Google Scholar] [CrossRef]
- Tu, Y.F.; Chien, C.S.; Yarmishyn, A.A.; Lin, Y.Y.; Luo, Y.H.; Lin, Y.T.; Lai, W.Y.; Yang, D.M.; Chou, S.J.; Yang, Y.P.; et al. A Review of SARS-CoV-2 and the Ongoing Clinical Trials. Int. J. Mol. Sci. 2020, 21, 2657. [Google Scholar] [CrossRef] [Green Version]
- He, G.; Han, Y.; Fang, Q.; Zhou, J.; Shen, J.; Li, T.; Pu, Q.; Chen, A.; Qi, Z.; Sun, L.; et al. Clinical experience of high-flow nasal cannula oxygen therapy in severe corona virus disease 2019 (COVID-19) patients. J. Zhejiang Univ. (Med. Sci.) 2020, 49, 232–239. [Google Scholar] [CrossRef]
- Cheung, J.C.; Ho, L.T.; Cheng, J.V.; Cham, E.Y.K.; Lam, K.N. Staff Safety during Emergency Airway Management for COVID-19 in Hong Kong. Lancet Respir. Med. 2020, 8, e19. [Google Scholar] [CrossRef]
- Namendys-Silva, S.A. Respiratory Support for Patients with COVID-19 Infection. Lancet Respir. Med. 2020, 8, e18. [Google Scholar] [CrossRef]
- McEnery, T.; Gough, C.; Costello, R.W. COVID-19: Respiratory Support Outside the Intensive Care Unit. Lancet Respir. Med. 2020, 8, 538–539. [Google Scholar] [CrossRef]
- Alhazzani, W.; Moller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferioli, M.; Cisternino, C.; Leo, V.; Pisani, L.; Palange, P.; Nava, S. Protecting Healthcare Workers from SARS-CoV-2 Infection: Practical Indications. Eur. Respir. Rev. 2020, 29. [Google Scholar] [CrossRef]
- Heinzerling, A.; Stuckey, M.J.; Scheuer, T.; Xu, K.; Perkins, K.M.; Resseger, H.; Magill, S.; Verani, J.R.; Seema Jain, S.; Acosta, M.; et al. Transmission of COVID-19 to Health Care Personnel During Exposures to a Hospitalized Patient-Solano County, California, February 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 472–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthay, M.A.; Aldrich, J.M.; Gotts, J.E. Treatment for Severe Acute Respiratory Distress Syndrome from COVID-19. Lancet Respir. Med. 2020, 8, 433–434. [Google Scholar] [CrossRef] [Green Version]
- Mohr, N.M.; Wu, C.; Ward, M.J.; McNaughton, C.D.; Richardson, K.; Kaboli, P.J. Potentially Avoidable Inter-Facility Transfer from Veterans Health Administration emergency departments: A Cohort Study. BMC Health Serv. Res. 2020, 20, 110. [Google Scholar] [CrossRef]
- Yoder, A.; Bradburn, E.H.; Morgan, M.E.; Vernon, T.M.; Bresz, K.E.; Gross, B.W.; Cook, A.D.; Rogers, F.B. An Analysis of Overtriage and Undertriage by Advanced Life Support Transport in a Mature Trauma System. J. Trauma Acute Care Surg. 2020, 88, 704–709. [Google Scholar] [CrossRef]
- Worster, A.; Bledsoe, R.D.; Cleve, P.; Fernandes, C.M.; Upadhye, S.; Eva, K. Reassessing the Methods of Medical Record Review Studies in Emergency Medicine Research. Ann. Emerg. Med. 2005, 45, 448–451. [Google Scholar] [CrossRef]
- Tagarro, A.; Epalza, C.; Santos, M.; Sanz-Santaeufemia, F.J.; Otheo, E.; Moraleda, C.; Calvo, C. Screening and Severity of Coronavirus Disease 2019 (COVID-19) in Children in Madrid, Spain. JAMA Pediatr. 2020, 55, 1546–1547. [Google Scholar]
- Attanasi, M.; Pasini, S.; Caronni, A.; Pellegrino, G.M.; Faverio, P.; Di Pillo, S.; Cimino, M.M.; Cipolla, G.; Chiarelli, F.; Centanni, S. Inpatient Care during the COVID-19 Pandemic: A Survey of Italian Physicians [Published Online Ahead of Print, 2020 Aug 5]. Respiration 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- El-Boghdadly, K.; Wong, D.J.N.; Owen, R.; Neuman, M.D.; Pocock, S.; Carlisle, J.B.; Johnstone, C.; Andruszkiewicz, P.; Baker, P.A.; Biccard, B.M.; et al. Risks to Healthcare Workers Following Tracheal Intubation of Patients with COVID-19: A Prospective International Multicentre Cohort Study. Anaesthesia 2020. [Google Scholar] [CrossRef]
- Tran, K.; Cimon, K.; Severn, M.; Pessoa-Silva, C.L.; Conly, J. Aerosol Generating Procedures and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A Systematic Review. PLoS ONE 2012, 7, e35797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochwerg, B.; Brochard, L.; Elliott, M.W.; Hess, D.; Hill, N.S.; Nava, S.; Antonelli, M.; Brozek, J.; Conti, G. Official ERS/ATS Clinical Practice Guidelines: Noninvasive Ventilation for Acute Respiratory Failure. Eur. Respir. J. 2017, 50, 1602426. [Google Scholar] [CrossRef] [PubMed]
- Higgs, A.; McGrath, B.A.; Goddard, C.; Rangasami, J.; Suntheralingam, G.; Gale, R.; Cook, T.M. Guidelines for the Management of Tracheal Intubation in Critically Ill Adults. Br. J. Anaesth. 2018, 120, 323–352. [Google Scholar] [CrossRef] [Green Version]
- De Jong, A.; Rolle, A.; Molinari, N.; Paugam-Burtz, C.; Constantin, J.M.; Lefrant, J.Y.; Asehnoune, K.; Jung, B.; Chanques, G.; Azoulay, E.; et al. Cardiac Arrest and Mortality Related to Intubation Procedure in Critically Ill Adult Patients: A Multicenter Cohort Study. Crit. Care Med. 2018, 46, 532–539. [Google Scholar] [CrossRef]
- Sorbello, M.; Morello, G.; Pintaudi, S.; Cataldo, R. COVID-19: Intubation Kit, Intubation Team or Intubation Spots? Anesth. Analg. 2020, 10, 1213. [Google Scholar] [CrossRef]
- Cook, T.M.; El-Boghdadly, K.; McGuire, B.; McNarry, A.F.; Patel, A.; Higgs, A. Consensus Guidelines for Managing the Airway in Patients with COVID-19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia 2020, 75, 785–799. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Population (n = 300) | In-Hospital Admission without Prehospital Intubation (n = 200) | Prehospital Intubation (n = 18) | OR (95% CI) | p Value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age in years | 64 ± 18 | 61 ± 19 | 62 ± 11 | 1.00 (0.98–1.03) | 0.798 |
| Male gender | 166 (55%) | 161 (80%) | 5 (28%) | 0.46 (0.14–0.57) | <10−3 |
| Hypertension | 91 (30%) | 82 (41%) | 9 (50%) | 0.36 (0.58–4.41) | 0.359 |
| Coronaropathy | 22 (7%) | 22 (11%) | 0 (0%) | 0.1 (0.01–8.8 × 1031) | 0.991 |
| Cardiopathy | 34 (11%) | 33 (17%) | 1 (6%) | 0.31 (0.02–1.61) | 0.267 |
| Diabetes mellitus | 56 (19%) | 48 (24%) | 8 (44%) | 2.78 (0.99–7.66) | 0.046 |
| Obesity | 36 (12%) | 32 (16%) | 4 (22%) | 1.60 (0.43–4.85) | 0.438 |
| COPD | 22 (7%) | 22 (11%) | 0 (0%) | 0.1 (0.01–8.8 × 1031) | 0.991 |
| Chronic renal failure | 2 (0.1%) | 0 (0%) | 2 (11%) | 2.06 × 108 (0.1–8.8 × 1031) | 0.991 |
| Immunosuppression | 15 (5%) | 13 (7%) | 2 (11%) | 1.90 (0.28–7.76) | 0.467 |
| Asthma | 22 (7%) | 20 (10%) | 2 (11%) | 1.19 (0.18–4.63) | 0.828 |
| Active smoking | 21 (7%) | 21 (11%) | 0 (0%) | 0.1 (0.01–7.4 × 1032) | 0.991 |
| Prehospital vital signs | |||||
| HR (beats/min) | 96 ± 23 | 95 ± 23 | 108 ± 18 | 1.02 (0.99–1.04) | 0.024 |
| SBP (mm Hg) | 138 ± 24 | 138 ± 24 | 143 ± 26 | 1.01 (0.99–1.03) | 0.411 |
| Body core temperature (°C) | 37.1 (36.1–38.2) | 37.0 (36.1–38.2) | 38.0 (36.6–38.7) | 1.3 (0.94–1.88) | 0.156 |
| Glasgow coma scale | 15 (15–15) | 15 (15–15) | 14 (3–15) | 0.76 (0.68–0.85) | |
| RR (movements/min) | 28 ± 10 | 27 ± 10 | 35 ± 11 | 1.06 (1.02–1.11) | 0.011 |
| Pulse oximetry (%) | 89 (76–98) | 90 (80–98) | 45 (43–56) | 0.90 (0.85–0.94) | <10−3 |
| HI | 3.4 ± 1.9 | 3.6 ± 1.8 | 1.0 ± 1.0 | 0.24 (0.12–0.41) | <10−3 |
| HI <1.3 | 20 (7%) | 9 (5%) | 11 (61%) | 38.38 (11.57–146.54) | <10−3 |
| Norepinephrine administration | 7 (2%) | 3 (0.1%) | 4 (22%) | 18.76 (3.80–103.48) | <10−3 |
| Symptom | n | Percentage (%) |
|---|---|---|
| Dyspnea | 152 | 51 |
| Fever | 135 | 45 |
| Cough | 92 | 31 |
| Chest pain | 50 | 17 |
| Myalgia | 32 | 11 |
| Discomfort | 28 | 9 |
| Diarrhea | 23 | 8 |
| Vomiting | 12 | 4 |
| Anosmia | 11 | 4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jouffroy, R.; Kedzierewicz, R.; Derkenne, C.; Bertho, K.; Scannavino, M.; Frattini, B.; Lemoine, F.; Jost, D.; Prunet, B. Hypoxemia Index Associated with Prehospital Intubation in COVID-19 Patients. J. Clin. Med. 2020, 9, 3025. https://doi.org/10.3390/jcm9093025
Jouffroy R, Kedzierewicz R, Derkenne C, Bertho K, Scannavino M, Frattini B, Lemoine F, Jost D, Prunet B. Hypoxemia Index Associated with Prehospital Intubation in COVID-19 Patients. Journal of Clinical Medicine. 2020; 9(9):3025. https://doi.org/10.3390/jcm9093025
Chicago/Turabian StyleJouffroy, Romain, Romain Kedzierewicz, Clement Derkenne, Kilian Bertho, Marine Scannavino, Benoit Frattini, Frederic Lemoine, Daniel Jost, and Bertrand Prunet. 2020. "Hypoxemia Index Associated with Prehospital Intubation in COVID-19 Patients" Journal of Clinical Medicine 9, no. 9: 3025. https://doi.org/10.3390/jcm9093025