The Value of Morphometric Measurements in Risk Assessment for Donor-Site Complications after Microsurgical Breast Reconstruction

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Surgical Procedure
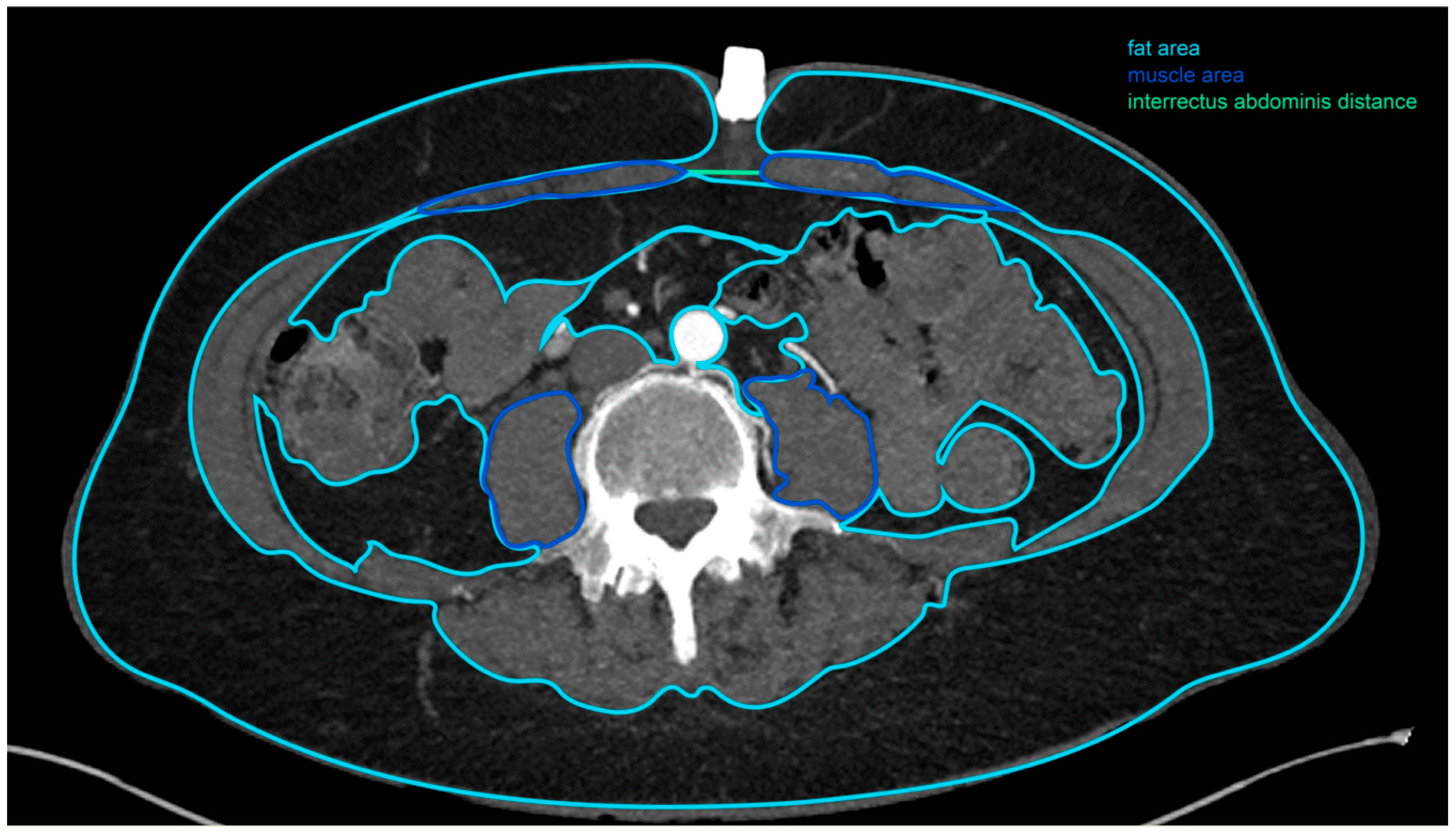
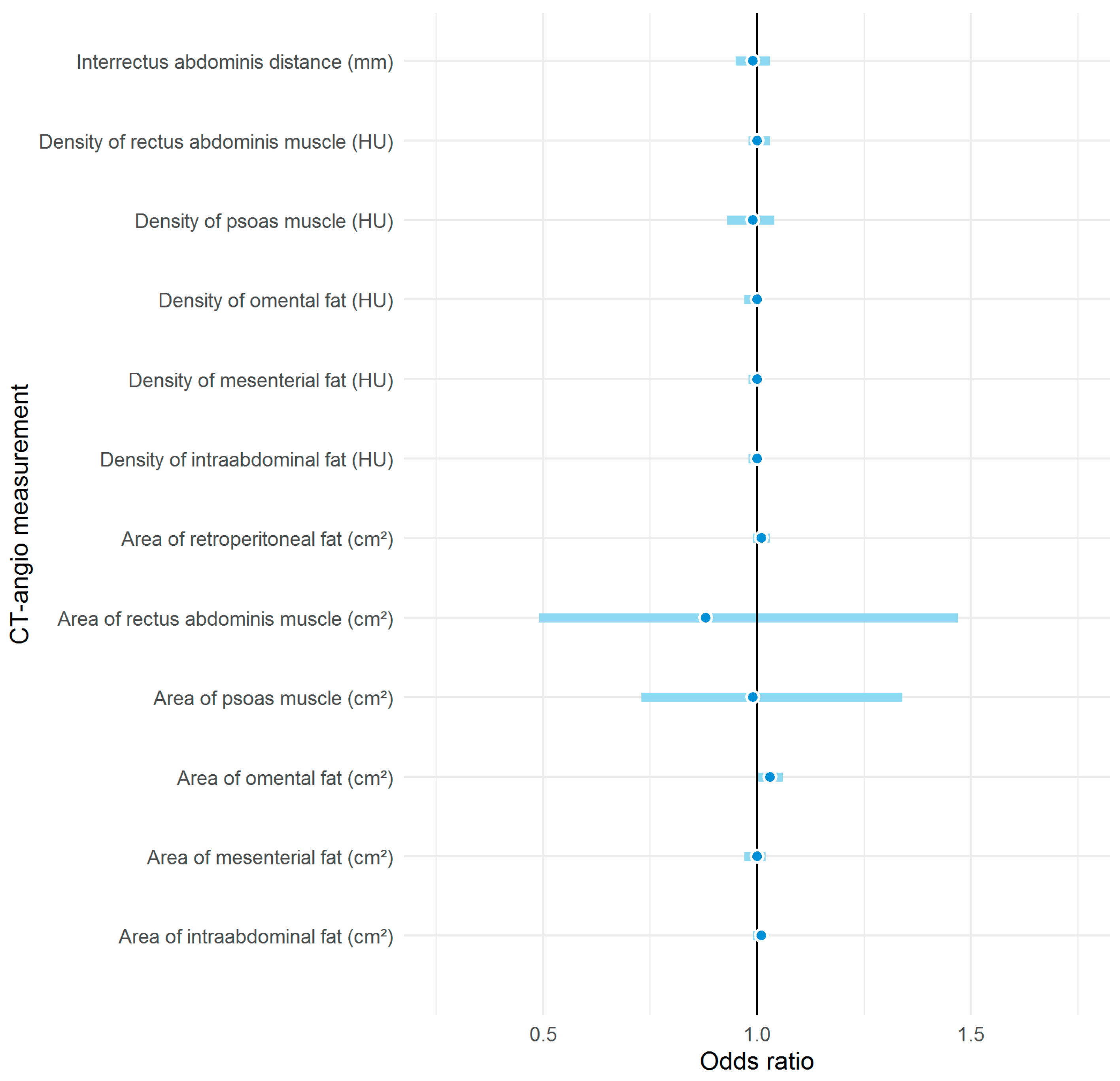
2.2. Computed Tomographic Angiogram Measurements
2.3. Patients
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Donor-Site Complications: Presumed Causes and Impact
4.2. Obesity, BMI, and Areas of Fat as Predictors of Donor-Site Complications
4.3. The Potential of Other Morphometric Measurements
4.4. Personalised Medicine
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winters, Z.E.; Benson, J.R.; Pusic, A.L. A systematic review of the clinical evidence to guide treatment recommendations in breast reconstruction based on patient-reported outcome measures and health-related quality of life. Ann. Surg. 2010, 252, 929–942. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Ma, J.; Goding Sauer, A.; Newman, L.A.; Jemal, A. Breast cancer statistics, 2017, racial disparity in mortality by state. CA Cancer J. Clin. 2017, 67, 439–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rozen, W.M.; Ashton, M.W.; Taylor, G.I. Defining the role for autologous breast reconstruction after mastectomy: Social and oncologic implications. Clin. Breast Cancer 2008, 8, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Colakoglu, S.; Khansa, I.; Curtis, M.S.; Yueh, J.H.; Ogunleye, A.; Haewyon, C.; Tobias, A.M.; Lee, B.T. Impact of complications on patient satisfaction in breast reconstruction. Plast. Reconstr. Surg. 2011, 127, 1428–1436. [Google Scholar] [CrossRef]
- Erdmann-Sager, J.; Wilkins, E.G.; Pusic, A.L.; Qi, J.; Hamill, J.B.; Kim, H.M.; Guldbrandsen, G.E.; Chun, Y.S. Complications and Patient-Reported Outcomes after Abdominally Based Breast Reconstruction: Results of the Mastectomy Reconstruction Outcomes Consortium Study. Plast. Reconstr. Surg. 2018, 141, 271–281. [Google Scholar] [CrossRef]
- Healy, C.; Allen Sr, R.J. The evolution of perforator flap breast reconstruction: Twenty years after the first DIEP flap. J. Reconstr. Microsurg. 2014, 30, 121–126. [Google Scholar]
- Egeberg, A.; Rasmussen, M.K.; Sørensen, J.A. Comparing the donor-site morbidity using DIEP, SIEA or MS-TRAM flaps for breast reconstructive surgery: A meta-analysis. J. Plast. Reconstr. Aesthetic Surg. 2012, 65, 1474–1480. [Google Scholar] [CrossRef]
- Clough, K.B.; O’Donoghue, J.M.; Fitoussi, A.D.; Vlastos, G.; Falcou, M.C. Prospective evaluation of late cosmetic results following breast reconstruction: II. Tram flap reconstruction. Plast. Reconstr. Surg. 2001, 107, 1710–1716. [Google Scholar] [CrossRef]
- Macadam, S.A.; Bovill, E.S.; Buchel, E.W.; Lennox, P.A. Evidence-Based Medicine: Autologous Breast Reconstruction. Plast. Reconstr. Surg. 2017, 139, 204e–229e. [Google Scholar] [CrossRef]
- Dibbs, R.; Trost, J.; DeGregorio, V.; Izaddoost, S. Free Tissue Breast Reconstruction. Semin. Plast. Surg. 2019, 33, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Schaverien, M.V.; McCulley, S.J. Effect of obesity on outcomes of free autologous breast reconstruction: A meta-analysis. Microsurgery 2014, 34, 484–497. [Google Scholar] [CrossRef] [PubMed]
- Levi, B.; Rinkinen, J.; Kidwell, K.M.; Benedict, M.; Stein, I.C.; Lisiecki, J.; Enchakalody, B.; Wang, S.C.; Kozlow, J.H.; Momoh, A.O. Morphomic analysis for preoperative donor site risk assessment in patients undergoing abdominal perforator flap breast reconstruction: A proof of concept study. J. Reconstr. Microsurg. 2014, 30, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Kappos, E.A.; Jaskolka, J.; Butler, K.; O’Neill, A.C.; Hofer, S.O.P.; Zhong, T. Preoperative Computed Tomographic Angiogram Measurement of Abdominal Muscles Is a Valuable Risk Assessment for Bulge Formation after Microsurgical Abdominal Free Flap Breast Reconstruction. Plast. Reconstr. Surg. 2017, 140, 170–177. [Google Scholar] [CrossRef]
- Englesbe, M.J.; Lee, J.S.; He, K.; Fan, L.; Schaubel, D.E.; Sheetz, K.H.; Harbaugh, C.M.; Holcombe, S.A.; Campbell, D.A.; Sonnenday, C.J.; et al. Analytic morphomics, core muscle size, and surgical outcomes. Ann. Surg. 2012, 256, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Ding, Z.; Wu, X.R.; Remer, E.M.; Lian, L.; Stocchi, L.; Li, Y.; McCullough, A.; Remzi, F.H.; Shen, B. Association between high visceral fat area and postoperative complications in patients with Crohn’s disease following primary surgery. Color. Dis. 2016, 18, 163–172. [Google Scholar] [CrossRef]
- Kuritzkes, B.A.; Pappou, E.P.; Kiran, R.P.; Baser, O.; Fan, L.; Guo, X.; Zhao, B.; Bentley-Hibbert, S. Visceral fat area, not body mass index, predicts postoperative 30-day morbidity in patients undergoing colon resection for cancer. Int. J. Color. Dis. 2018, 33, 1019–1028. [Google Scholar] [CrossRef]
- Carioli, G.; Malvezzi, M.; Rodriguez, T.; Bertuccio, P.; Negri, E.; La Vecchia, C. Trends and predictions to 2020 in breast cancer mortality in Europe. Breast 2017, 36, 89–95. [Google Scholar] [CrossRef]
- Kappos, E.A.; Fitzgerald, E.; Haug, M.D.; Quaba, O.; Quaba, A. What Happened after the Poly Implant Prothese Recall? A Prospective Cohort Study of 808 Implants into the Predictive Value of Implant Rupture on Postexchange Complications. Plast. Reconstr. Surg. 2019, 144, 35e–42e. [Google Scholar] [CrossRef]
- Van Wingerden, J.J.; Beets, M.R.; Oostrom, C.A.; Wever, C.F.; Theuvenet, W.J. The Clavien-Dindo classification for post-discharge reconstructive surgery complications and comparison of caregiver registration. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 1418–1433. [Google Scholar] [CrossRef]
- Miyamoto, S.; Nakao, J.; Higashino, T.; Yoshimoto, S.; Hayashi, R.; Sakuraba, M. Clavien-Dindo classification for grading complications after total pharyngolaryngectomy and free jejunum transfer. PLoS ONE 2019, 14, e0222570. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; De Santibanes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, R.; Haug, I.; Lebo, P.; Grohmann, M.; Reischies, F.; Cambiaso-Daniel, J.; Tuca, A.; Rienmüller, T.; Friedl, H.; Spendel, S.; et al. Standardizing the complication rate after breast reduction using the Clavien-Dindo classification. Surgery 2017, 161, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Joseph, W.J.; Cuccolo, N.G.; Baron, M.E.; Chow, I.; Beers, E.H. Frailty predicts morbidity, complications, and mortality in patients undergoing complex abdominal wall reconstruction. Hernia 2020, 24, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Pajula, S.; Jyränki, J.; Tukiainen, E.; Koljonen, V. Complications after lower body contouring surgery due to massive weight loss unaffected by weight loss method. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Lu, S.M.; Nelson, J.A.; Fischer, J.P.; Fosnot, J.; Goldstein, J.; Selber, J.C.; Serletti, J.M.; Wu, L.C. The impact of complications on function, health, and satisfaction following abdominally based autologous breast reconstruction: A prospective evaluation. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 682–692. [Google Scholar] [CrossRef]
- Nahabedian, M.Y.; Momen, B.; Galdino, G.; Manson, P.N. Breast Reconstruction with the free TRAM or DIEP flap: Patient selection, choice of flap, and outcome. Plast. Reconstr. Surg. 2002, 110, 466–475. [Google Scholar] [CrossRef] [Green Version]
- Chang, D.W.; Wang, B.; Robb, G.L.; Reece, G.P.; Miller, M.J.; Evans, G.R.; Langstein, H.N.; Kroll, S.S. Effect of obesity on flap and donor-site complications in free transverse rectus abdominis myocutaneous flap breast reconstruction. Plast. Reconstr. Surg. 2000, 105, 1640–1648. [Google Scholar] [CrossRef] [Green Version]
- Scheflan, M.; Dinner, M.I. The transverse abdominal island flap: Part I. Indications, contraindications, results, and complications. Ann. Plast. Surg. 1983, 10, 24–35. [Google Scholar] [CrossRef]
- Kroll, S.S.; Netscher, D.T. Complications of TRAM flap breast reconstruction in obese patients. Plast. Reconstr. Surg. 1989, 84, 886–892. [Google Scholar] [CrossRef]
- Corrigan, K.E.; Vargas, M.V.; Robinson, H.N.; Gu, A.; Wei, C.; Tyan, P.; Singh, N.; Tappy, E.E.; Moawad, G.N. Impact of Diabetes Mellitus on Postoperative Complications Following Laparoscopic Hysterectomy for Benign Indications. Gynecol. Obstet. Investig. 2019, 84, 583–590. [Google Scholar] [CrossRef]
- Qin, C.; Souza, J.; Aggarwal, A.; Kim, J.Y. Insulin dependence as an independent predictor of perioperative morbidity after ventral hernia repair: A National Surgical Quality Improvement Program analysis of 45,759 patients. Am. J. Surg. 2016, 211, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Samson, S.L.; Garber, A.J. Metabolic syndrome. Endocrinol. Metab. Clin. N. Am. 2014, 43, 1–23. [Google Scholar] [CrossRef]
- Beugels, J.; Meijvogel, J.L.W.; Tuinder, S.M.H.; Tjan-Heijnen, V.C.G.; Heuts, E.M.; Piatkowski, A.; Van Der Hulst, R. The influence of neoadjuvant chemotherapy on complications of immediate DIEP flap breast reconstructions. Breast Cancer Res. Treat. 2019, 176, 367–375. [Google Scholar] [CrossRef] [Green Version]
- Schaverien, M.V.; Munnoch, D.A. Effect of neoadjuvant chemotherapy on outcomes of immediate free autologous breast reconstruction. Eur. J. Surg. Oncol. 2013, 39, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Azzawi, K.; Ismail, A.; Earl, H.; Forouhi, P.; Malata, C.M. Influence of neoadjuvant chemotherapy on outcomes of immediate breast reconstruction. Plast. Reconstr. Surg. 2010, 126, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Narui, K.; Ishikawa, T.; Satake, T.; Adachi, S.; Yamada, A.; Shimada, K.; Shimizu, D.; Kida, K.; Sugae, S.; Ichikawa, Y.; et al. Outcomes of immediate perforator flap reconstruction after skin-sparing mastectomy following neoadjuvant chemotherapy. Eur. J. Surg. Oncol. 2015, 41, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Hamnett, K.E.; Subramanian, A. Breast reconstruction in older patients: A literature review of the decision-making process. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 1325–1334. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, J.; Long, S.; Carter, B.; Bach, S.; McCarthy, K.; Clegg, A. The prevalence of frailty and its association with clinical outcomes in general surgery: A systematic review and meta-analysis. Age Ageing 2018, 47, 793–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seib, C.D.; Rochefort, H.; Chomsky-Higgins, K.; Gosnell, J.E.; Suh, I.; Shen, W.T.; Duh, Q.Y.; Finlayson, E. Association of Patient Frailty with Increased Morbidity after Common Ambulatory General Surgery Operations. JAMA Surg. 2018, 153, 160–168. [Google Scholar] [CrossRef]
- Makary, M.A.; Segev, D.L.; Pronovost, P.J.; Syin, D.; Bandeen-Roche, K.; Patel, P.; Takenaga, R.; Devgan, L.; Holzmueller, C.G.; Tian, J.; et al. Frailty as a predictor of surgical outcomes in older patients. J. Am. Coll. Surg. 2010, 210, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Oakland, K.; Nadler, R.; Cresswell, L.; Jackson, D.; Coughlin, P.A. Systematic review and meta-analysis of the association between frailty and outcome in surgical patients. Ann. R. Coll. Surg. Engl. 2016, 98, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchernof, A.; Despres, J.P. Pathophysiology of human visceral obesity: An update. Physiol. Rev. 2013, 93, 359–404. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, F.X. Obesity: Criteria and classification. Proc. Nutr. Soc. 2000, 59, 505–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levi, B.; Zhang, P.; Lisiecki, J.; Terjimanian, M.N.; Rinkinen, J.; Agarwal, S.; Holcombe, S.A.; Kozlow, J.H.; Wang, S.C.; Kuzon, W.M. Use of morphometric assessment of body composition to quantify risk of surgical-site infection in patients undergoing component separation ventral hernia repair. Plast. Reconstr. Surg. 2014, 133, 559e–566e. [Google Scholar] [CrossRef]
- Parikh, R.M.; Joshi, S.R.; Menon, P.S.; Shah, N.S. Index of central obesity—A novel parameter. Med. Hypotheses 2007, 68, 1272–1275. [Google Scholar] [CrossRef]
- Sugerman, H.; Windsor, A.; Bessos, M.; Wolfe, L. Intra-abdominal pressure, sagittal abdominal diameter and obesity comorbidity. J. Intern. Med. 1997, 241, 71–79. [Google Scholar] [CrossRef]
- Lambert, D.M.; Marceau, S.; Forse, R.A. Intra-abdominal pressure in the morbidly obese. Obes. Surg. 2005, 15, 1225–1232. [Google Scholar] [CrossRef]
- Brauman, D. Diastasis recti: Clinical anatomy. Plast. Reconstr. Surg. 2008, 122, 1564–1569. [Google Scholar] [CrossRef]
- Diebel, L.; Saxe, J.; Dulchavsky, S. Effect of intra-abdominal pressure on abdominal wall blood flow. Am. Surg. 1992, 58, 573, discussion 575–576. [Google Scholar]
- Tjeertes, E.K.; Hoeks, S.E.; Beks, S.B.; Valentijn, T.M.; Hoofwijk, A.G.; Stolker, R.J. Obesity-a risk factor for postoperative complications in general surgery? BMC Anesthesiol. 2015, 15, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modarressi, A.; Muller, C.T.; Montet, X.; Ruegg, E.M.; Pittet-Cuenod, B. DIEP flap for breast reconstruction: Is abdominal fat thickness associated with post-operative complications? J. Plast. Reconstr. Aesthet. Surg. 2017, 70, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.I.; Liu, J. Prospective Evaluation of Obese Patients Undergoing Autologous Abdominal Free Flap Breast Reconstruction. Plastic. Reconstr. Surg. 2018, 142, 120e–125e. [Google Scholar] [CrossRef] [PubMed]
- Klasson, S.; Nyman, J.; Svensson, H.; Velander, P. Smoking increases donor site complications in breast reconstruction with DIEP flap. J. Plast. Surg. Hand Surg. 2016, 50, 331–335. [Google Scholar] [CrossRef]
- Ochoa, O.; Chrysopoulo, M.; Nastala, C.; Ledoux, P.; Pisano, S. Abdominal wall stability and flap complications after deep inferior epigastric perforator flap breast reconstruction: Does body mass index make a difference? Analysis of 418 patients and 639 flaps. Plast. Reconstr. Surg. 2012, 130, 21e–33e. [Google Scholar] [CrossRef]
- Momeni, A.; Ahdoot, M.A.; Kim, R.Y.; Leroux, E.; Galaiya, D.J.; Lee, G.K. Should we continue to consider obesity a relative contraindication for autologous microsurgical breast reconstruction? J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 420–425. [Google Scholar] [CrossRef]
- Papadakis, M.; Schuster, F.; Djedovic, G.; Rahmanian-Schwarz, A. Super obesity is not necessarily a contraindication to deep inferior epigastric perforator flap breast reconstruction. BMJ Case Rep. 2018, 2018. [Google Scholar] [CrossRef]
- Park, J.W.; Lee, H.; Jeon, B.J.; Pyon, J.K.; Mun, G.H. Assessment of the risk of bulge/hernia formation after abdomen-based microsurgical breast reconstruction with the aid of preoperative computed tomographic angiography-derived morphometric measurements. J. Plast. Reconstr. Aesthet. Surg. 2020. [Google Scholar] [CrossRef]
- Cakir, H.; Heus, C.; Van Der Ploeg, T.J.; Houdijk, A.P. Visceral obesity determined by CT scan and outcomes after colorectal surgery; a systematic review and meta-analysis. Int. J. Color. Dis. 2015, 30, 875–882. [Google Scholar] [CrossRef]
- Englesbe, M.J.; Patel, S.P.; He, K.; Lynch, R.J.; Schaubel, D.E.; Harbaugh, C.; Holcombe, S.A.; Wang, S.C.; Segev, D.L.; Sonnenday, C.J. Sarcopenia and mortality after liver transplantation. J. Am. Coll. Surg. 2010, 211, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; He, K.; Harbaugh, C.M.; Schaubel, D.E.; Sonnenday, C.J.; Wang, S.C.; Englesbe, M.J.; Eliason, J.L. Frailty, core muscle size, and mortality in patients undergoing open abdominal aortic aneurysm repair. J. Vasc. Surg. 2011, 53, 912–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winters, H.; Knaapen, L.; Buyne, O.R.; Hummelink, S.; Ulrich, D.J.O.; Van Goor, H.; Van Geffen, E.; Slater, N.J. Pre-operative CT scan measurements for predicting complications in patients undergoing complex ventral hernia repair using the component separation technique. Hernia 2019, 23, 347–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goetz, L.H.; Schork, N.J. Personalized medicine: Motivation, challenges, and progress. Fertil. Steril. 2018, 109, 952–963. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Definition | Example |
|---|---|---|
| I | Deviation from normal postoperative course with no need for pharmacological or surgical interventions. * |
|
| II | Pharmacological treatment required. |
|
| IIIa IIIb | Requiring surgical intervention
|
|
| IV | Life threatening complication. |
|
| V | Death of a patient. |
|
| Clavien–Dindo | Donor Site Complication | Therapeutic Management | Number of Events |
|---|---|---|---|
| I | - Delayed wound healing | - Dressing changes | 3 |
| - Seroma | - Needle aspiration | 2 | |
| Seroma | Observation | 2 | |
| IIIa | - Delayed wound healing | - Vacuum-asissted closure therapy | 1 |
| IIIb | - Seroma | - Surgical seroma evacuation and drainage | 2 |
| - Seroma | - Surgical debridement | 2 | |
| - Postoperative wound infection | - Sclerotherapy and surgical revision | 1 |
| Variable | Normal Weight (n = 44) | Obese (n = 46) | Total | p-Value | |
|---|---|---|---|---|---|
| Area of subcutaneous fat (cm2) | Mean (SD) | 191.3 (53.2) | 348.6 (82.9) | 271.7 (105.3) | 0.000 |
| Area of intraabdominal fat (cm2) | Mean (SD) | 26.1 (28.6) | 67.1 (41.7) | 47.1 (41.2) | 0.000 |
| Area of omental fat (cm2) | Mean (SD) | 8.4 (9.1) | 27.8 (24.1) | 18.3 (20.7) | 0.000 |
| Area of mesenteric fat (cm2) | Mean (SD) | 17.7 (25.7) | 39.3 (26.5) | 28.8 (28.1) | 0.000 |
| Area of retroperitoneal fat (cm2) | Mean (SD) | 29.5 (22.5) | 53.6 (25.3) | 41.8 (26.7) | 0.000 |
| Variable | OR (95% CI, p-Value) | OR (95% CI, p-Value) |
|---|---|---|
| Univariable | Multivariable | |
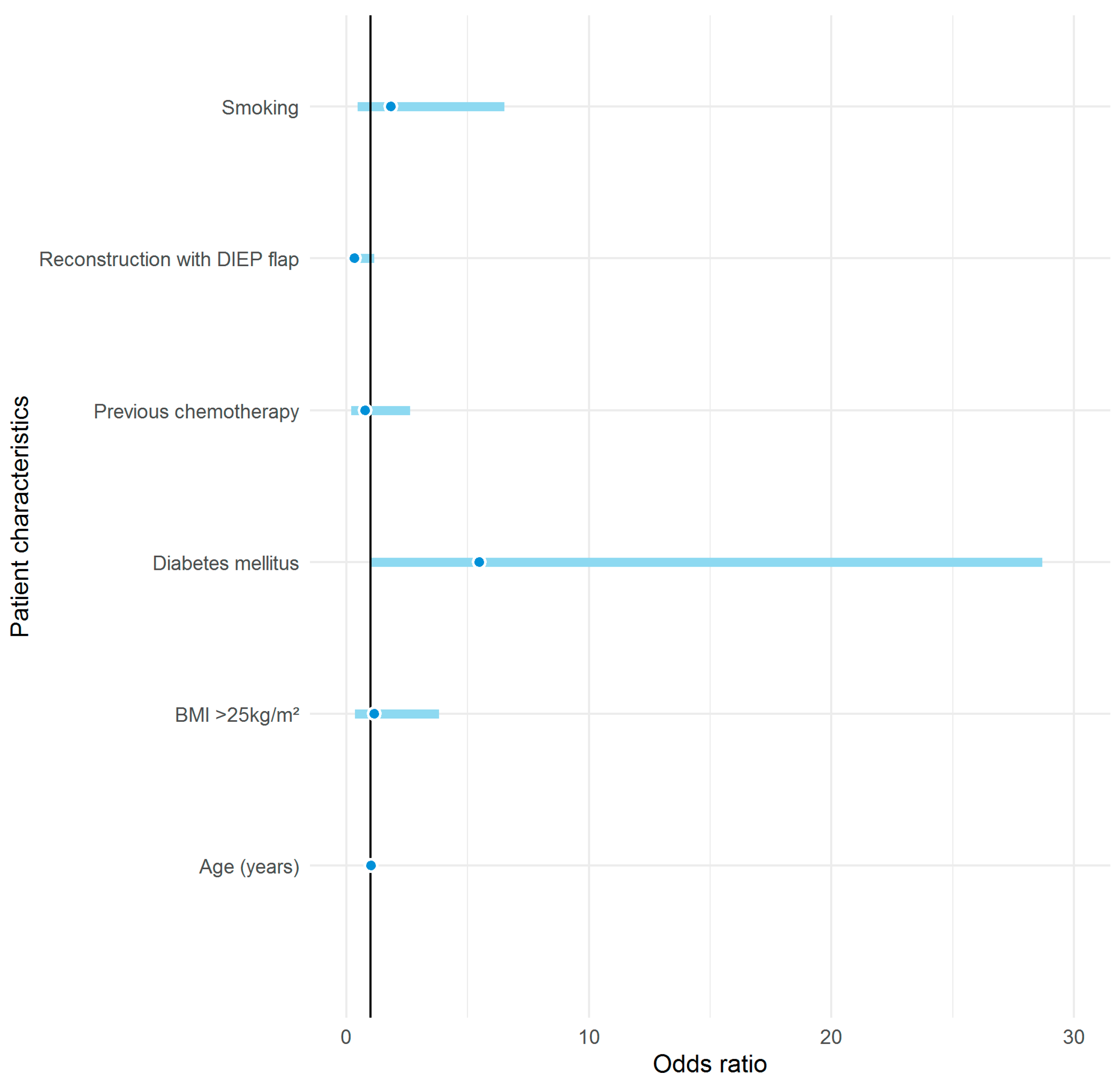
| Diabetes mellitus | 5.47 (1.04–28.77, p = 0.042) | 4.99 (0.84–27.40, p = 0.062) |
| Area of omental fat | 1.03 (1.00–1.06 p = 0.018) | 1.03 (1.00–1.06, p = 0.022) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, M.O.; Handschin, T.M.; Boll, D.T.; Chammartin, F.; Schaefer, D.J.; Haug, M.D.; Kappos, E.A. The Value of Morphometric Measurements in Risk Assessment for Donor-Site Complications after Microsurgical Breast Reconstruction. J. Clin. Med. 2020, 9, 2645. https://doi.org/10.3390/jcm9082645
Meyer MO, Handschin TM, Boll DT, Chammartin F, Schaefer DJ, Haug MD, Kappos EA. The Value of Morphometric Measurements in Risk Assessment for Donor-Site Complications after Microsurgical Breast Reconstruction. Journal of Clinical Medicine. 2020; 9(8):2645. https://doi.org/10.3390/jcm9082645
Chicago/Turabian StyleMeyer, Muriel O., Tristan M. Handschin, Daniel T. Boll, Frédérique Chammartin, Dirk J. Schaefer, Martin D. Haug, and Elisabeth A. Kappos. 2020. "The Value of Morphometric Measurements in Risk Assessment for Donor-Site Complications after Microsurgical Breast Reconstruction" Journal of Clinical Medicine 9, no. 8: 2645. https://doi.org/10.3390/jcm9082645