Chronic Spontaneous Urticaria and Type 1 Diabetes Mellitus—Does Quality of Life Impairment Always Reflect Health Danger?

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zuberbier, T.; Aberer, W.; Asero, R.; Abdul Latiff, A.H.; Baker, D.; Ballmer-Weber, B.; Bernstein, J.A.; Bindslev-Jensen, C.; Brzoza, Z.; Buense Bedrikow, R.; et al. The EAACI/GA2LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy 2018, 73, 1393–1414. [Google Scholar] [CrossRef] [PubMed]
- Brzoza, Z.; Badura-Brzoza, K.; Młynek, A.; Magerl, M.; Baiardini, I.; Canonica, G.W.; Weller, K.; Kocatürk, E.; Kalogeromitros, D.; Zalewska-Janowska, A.; et al. Adaptation and initial results of the Polish version of the GA2LEN Chronic Urticaria Quality Of Life Questionnaire (CU-Q2oL). J. Dermatol. Sci. 2011, 62, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.A.; Lang, D.M.; Khan, D.A.; Craig, T.; Dreyfus, D.; Hsieh, F.; Sheikh, J.; Weldon, D.; Zuraw, B.; Bernstein, D.I.; et al. The diagnosis and management of acute and chronic urticaria: 2014 update. J. Allergy Clin. Immunol. 2014, 133, 1270–1277.e66. [Google Scholar] [CrossRef]
- Zuberbier, T.; Balke, M.; Worm, M.; Edenharter, G.; Maurer, M. Epidemiology of urticaria: A representative cross-sectional population survey. Clin. Exp. Dermatol. 2010, 35, 869–873. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Report on Diabetes. 2016. Available online: http://www.who.int/iris/handle/10665/204871 (accessed on 26 January 2019).
- Federation ID. IDF Diabetes Atlas teB; International Diabetes Federation: Brussels, Belgium, 2017; Available online: http://www.diabetesatlas.org/ (accessed on 17 October 2019).
- Imkampe, A.-K.; Gulliford, M.C. Trends in Type 1 diabetes incidence in the UK in 0- to 14-year-olds and in 15- to 34-year-olds, 1991–2008. Diabet. Med. 2011, 28, 811–814. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.J.; Laffel, L.M.; Domenger, C.; Danne, T.; Phillip, M.; Mazza, C.; Hanas, R.; Waldron, S.; Beck, R.W.; Calvi-Gries, F.; et al. Factors associated with diabetes-specific health-related quality of life in youth with type 1 diabetes: The global teens study. Diabetes Care 2017, 40, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Diabetology, C. 2018 Guidelines on the management of diabetic patients. A position of Diabetes Poland. Clin. Diabetol. 2018, 7, 1–90. [Google Scholar] [CrossRef]
- Cappuccio, A.; Limonta, T.; Parodi, A.; Cristaudo, A.; Bugliaro, F.; Cannavò, S.; Rossi, O.; Gurioli, C.; Vignoli, A.; Parente, R.; et al. Living with Chronic Spontaneous Urticaria in Italy: A Narrative Medicine Project to Improve the Pathway of Patient Care. Acta Derm. Venereol. 2017, 97, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Nettis, E.; Foti, C.; Ambrifi, M.; Baiardini, I.; Bianchi, L.; Borghi, A.; Caminati, M.; Canonica, G.W.; Casciaro, M.; Colli, L.; et al. Urticaria: Recommendations from the Italian Society of Allergology, Asthma and Clinical Immunology and the Italian Society of Allergological, Occupational and Environmental Dermatology. Clin. Mol. Allergy 2020, 18, 8. [Google Scholar] [CrossRef]
- Baiardini, I.; Giardini, A.; Pasquali, M.; Dignetti, P.; Guerra, L.; Specchia, C.; Braido, F.; Majani, G.; Canonica, G.W. Quality of life and patients’ satisfaction in chronic urticaria and respiratory allergy. Allergy 2003, 58, 621–623. [Google Scholar] [CrossRef]
- O’Donnell, B.F.; Lawlor, F.; Simpson, J.; Morgan, M.; Greaves, M.W. The impact of chronic urticaria on the quality of life. Br. J. Dermatol. 1997, 136, 197–201. Available online: http://www.ncbi.nlm.nih.gov/pubmed/9068731 (accessed on 26 January 2019).
- Poon, E.; Seed, P.T.; Greaves, M.W.; Kobza-Black, A. The extent and nature of disability in different urticarial conditions. Br. J. Dermatol. 1999, 140, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Ayala, F.; Nino, M.; Fabbrocini, G.; Panariello, L.; Balato, N.; Foti, C.; Tosti, A.; Corazza, M.; Valsecchi, R.H.; Gola, M.; et al. Quality of life and contact dermatitis: A disease-specific questionnaire. Dermat. Contact Atopic Occup. Drug 2010, 21, 84–90. Available online: http://www.ncbi.nlm.nih.gov/pubmed/20233546 (accessed on 13 July 2020). [CrossRef]
- Marron, S.E.; Chernyshov, P.V.; Tomas-Aragones, L. Quality-of-Life Research in Acne Vulgaris: Current Status and Future Directions. Am. J. Clin. Dermatol. 2019, 20, 527–538. [Google Scholar] [CrossRef]
- Elbuluk, N.; Ezzedine, K. Quality of Life, Burden of Disease, Co-morbidities, and Systemic Effects in Vitiligo Patients. Dermatol. Clin. 2017, 35, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B.; Roman-Urrestarazu, A. Health-related quality of life in paediatric patients with TYPE 1 diabetes mellitus using insulin infusion systems. A Systematic review and meta-analysis. PLoS ONE 2019, 14, e0217655. [Google Scholar] [CrossRef]
- Diabetes Control and Complications Trial Research Group. Influence of intensive diabetes treatment on quality-of-life outcomes in the Diabetes Control and Complications Trial. Diabetes Care 1996, 19, 195–203. [Google Scholar] [CrossRef]
- Hahl, J.; Hämäläinen, H.; Sintonen, H.; Simell, T.; Arinen, S.; Simell, O. Health-related quality of life in type 1 diabetes without or with symptoms of long-term complications. Qual. Life Res. 2002, 11, 427–436. [Google Scholar] [CrossRef]
- Jacobson, A.M.; Braffett, B.H.; Cleary, P.A.; Gubitosi-Klug, R.A.; Larkin, M.E. The long-term effects of type 1 diabetes treatment and complications on health-related quality of life: A 23-year follow-up of the diabetes control and complications/epidemiology of diabetes interventions and complications cohort. Diabetes Care 2013, 36, 3131–3138. [Google Scholar] [CrossRef] [Green Version]
- Hoey, H.; Aanstoot, H.J.; Chiarelli, F.; Daneman, D.; Danne, T.; Dorchy, H.; Fitzgerald, M.; Garandeau, P.; Greene, S.; Holl, R.; et al. Good metabolic control is associated with better quality of life in 2,101 adolescents with type 1 diabetes. Diabetes Care 2001, 24, 1923–1928. [Google Scholar] [CrossRef] [Green Version]
- Cooke, D.; Bond, R.; Lawton, J.; Rankin, D.; Heller, S.; Clark, M.; Speight, J. Modeling predictors of changes in glycemic control and diabetes-specific quality of life amongst adults with type 1 diabetes 1 year after structured education in flexible, intensive insulin therapy. J. Behav. Med. 2015, 38, 817–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stahl-Pehe, A.; Landwehr, S.; Lange, K.S.; Bächle, C.; Castillo, K.; Yossa, R.; Lüdtke, J.; Holl, R.W.; Rosenbauer, J. Impact of quality of life (QoL) on glycemic control (HbA1c) among adolescents and emerging adults with long-duration type 1 diabetes: A prospective cohort-study. Pediatr. Diabetes 2017, 18, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Sparring, V.; Nyström, L.; Wahlström, R.; Jonsson, P.M.; Östman, J.; Burström, K. Diabetes duration and health-related quality of life in individuals with onset of diabetes in the age group 15–34 years-A Swedish population-based study using EQ-5D. BMC Public Health 2013, 13, 377. [Google Scholar] [CrossRef] [PubMed]
- Weldon, D. Quality of life in patients with urticaria and angioedema: Assessing burden of disease. Allergy Asthma Proc. 2014, 35, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Weldon, D.R. Quality of life in patients with urticaria. Allergy Asthma Proc. 2006, 27, 96–99. Available online: http://www.ncbi.nlm.nih.gov/pubmed/16724624 (accessed on 17 October 2019).
- Speight, J.; Reaney, M.D.; Barnard, K.D. Not all roads lead to Rome—A review of quality of life measurement in adults with diabetes. Diabet. Med. 2009, 26, 315–327. [Google Scholar] [CrossRef]
- Tang, T.S.; Yusuf, F.L.A.; Polonsky, W.H.; Fisher, L. Assessing quality of life in diabetes: II–Deconstructing measures into a simple framework. Diabetes Res. Clin. Pract. 2017, 126, 286–302. [Google Scholar] [CrossRef]
- Ware, J.E.; Gandek, B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. J. Clin. Epidemiol. 1998, 51, 903–912. [Google Scholar] [CrossRef]
- Młynek, A.; Zalewska-Janowska, A.; Martus, P.; Staubach, P.; Zuberbier, T.; Maurer, M. How to assess disease activity in patients with chronic urticaria? Allergy Eur. J. Allergy Clin. Immunol. 2008, 63, 777–780. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [Green Version]
- Dias, G.A.C.; Pires, G.V.; do Valle, S.O.R.; Dortas Júnior, S.D.; Levy, S.; França, A.T.; Baiardini, I.; Canonica, W.G. Impact of chronic urticaria on the quality of life of patients followed up at a university hospital. An. Bras. Dermatol. 2016, 91, 754–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pherwani, A.; Gadhia, S.; Bansode, G. The impact of chronic urticaria on the quality of life in Indian patients. Indian J. Dermatol. 2012, 57, 110. [Google Scholar] [CrossRef] [PubMed]
- Melendez-Ramirez, L.Y.; Richards, R.J.; Cefalu, W.T. Complications of type 1 diabetes. Endocrinol. Metab. Clin. N. Am. 2010, 39, 625–640. [Google Scholar] [CrossRef] [PubMed]
- Saylor, J.; Hanna, K.M.; Calamaro, C.J. Experiences of College Students Who Are Newly Diagnosed With Type 1 Diabetes Mellitus. J. Pediatr. Nurs. 2019, 44, 74–80. [Google Scholar] [CrossRef]
- Beattie, P.E.; Lewis-Jones, M.S. A comparative study of impairment of quality of life in children with skin disease and children with other chronic childhood diseases. Br. J. Dermatol. 2006, 155, 145–151. [Google Scholar] [CrossRef]
- Caine, N.; Harrison, S.C.; Sharples, L.D.; Wallwork, J. Prospective study of quality of life before and after coronary artery bypass grafting. BMJ 1991, 302, 511–516. [Google Scholar] [CrossRef] [Green Version]
- Costa, L.; Vieira, S. Quality of life of adolescents with type 1 diabetes. Clinics 2015, 70, 173–179. [Google Scholar] [CrossRef]
- Nielsen, H.B.; Ovesen, L.L.; Mortensen, L.H.; Lau, C.J.; Joensen, L.E. Type 1 diabetes, quality of life, occupational status and education level—A comparative population-based study. Diabetes Res. Clin. Pract. 2016, 121, 62–68. [Google Scholar] [CrossRef]
- Rubin, R.R.; Peyrot, M. Quality of life and diabetes. Diabetes Metab. Res. Rev. 1999, 15, 205–218. Available online: http://www.ncbi.nlm.nih.gov/pubmed/10441043 (accessed on 27 January 2019). [CrossRef]
- Audureau, E.; Rican, S.; Coste, J. Worsening trends and increasing disparities in health-related quality of life: Evidence from two French population-based cross-sectional surveys, 1995–2003. Qual. Life Res. 2013, 22, 13–26. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S.; Girgus, J.S. The emergence of gender differences in depression during adolescence. Psychol. Bull. 1994, 115, 424–443. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8016286 (accessed on 27 January 2019). [CrossRef] [PubMed]
- Bartman, W.; Nabrdalik, K.; Kwiendacz, H.; Sawczyn, T.; Tomasik, A.; Pierzchala, K.; Adamczyk-Sowa, M.; Machowska-Majchrzak, A.; Labuz-Roszak, B.; Grzeszczak, W.; et al. Association between carotid plaque score and microvascular complications of type 2 diabetes. Polish Arch. Intern. Med. 2017, 127, 418–422. [Google Scholar] [CrossRef] [Green Version]
- Nazimek-Siewniak, B.; Moczulski, D.; Grzeszczak, W. Risk of macrovascular and microvascular complications in Type 2 diabetes: Results of longitudinal study design. J. Diabetes Complicat. 2002, 16, 271–276. [Google Scholar] [CrossRef]
- Várkonyi, T.; Kempler, P. Sexual dysfunction in diabetes. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2014; Volume 126, pp. 223–232. [Google Scholar] [CrossRef]
- Jackson, G. Sexual dysfunction and diabetes. Int. J. Clin. Pract. 2004, 58, 258–362. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| M (%) | F (%) | Age | Duration of the Disease | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Range | Mean (Years) | SD | Range | |||
| T1DM (n = 66) | 34 (52%) | 32 (48%) | 36.3 | 11.1 | 18–59 | 16.9 | 9.45 | 0.1–42 |
| CSU (n = 51) | 17 (33%) | 34 (67%) | 35.8 | 8.53 | 19–49 | 3.84 | 6.84 | 0.17–30 |
| p | 0.05 | 0.80 | 0.00 | |||||
| T1DM | CSU | p | |||
|---|---|---|---|---|---|
| Median | Range | Median | Range | ||
| MH | 62 | 52–76 | 64 | 56–76 | 0.31 |
| VT | 60 | 45–70 | 60 | 45–70 | 0.64 |
| GH | 42.5 | 28–52 | 40 | 30–54 | 0.55 |
| BP | 75 | 20–100 | 75 | 30–100 | 0.90 |
| PF | 95 | 89–100 | 95 | 85–100 | 0.71 |
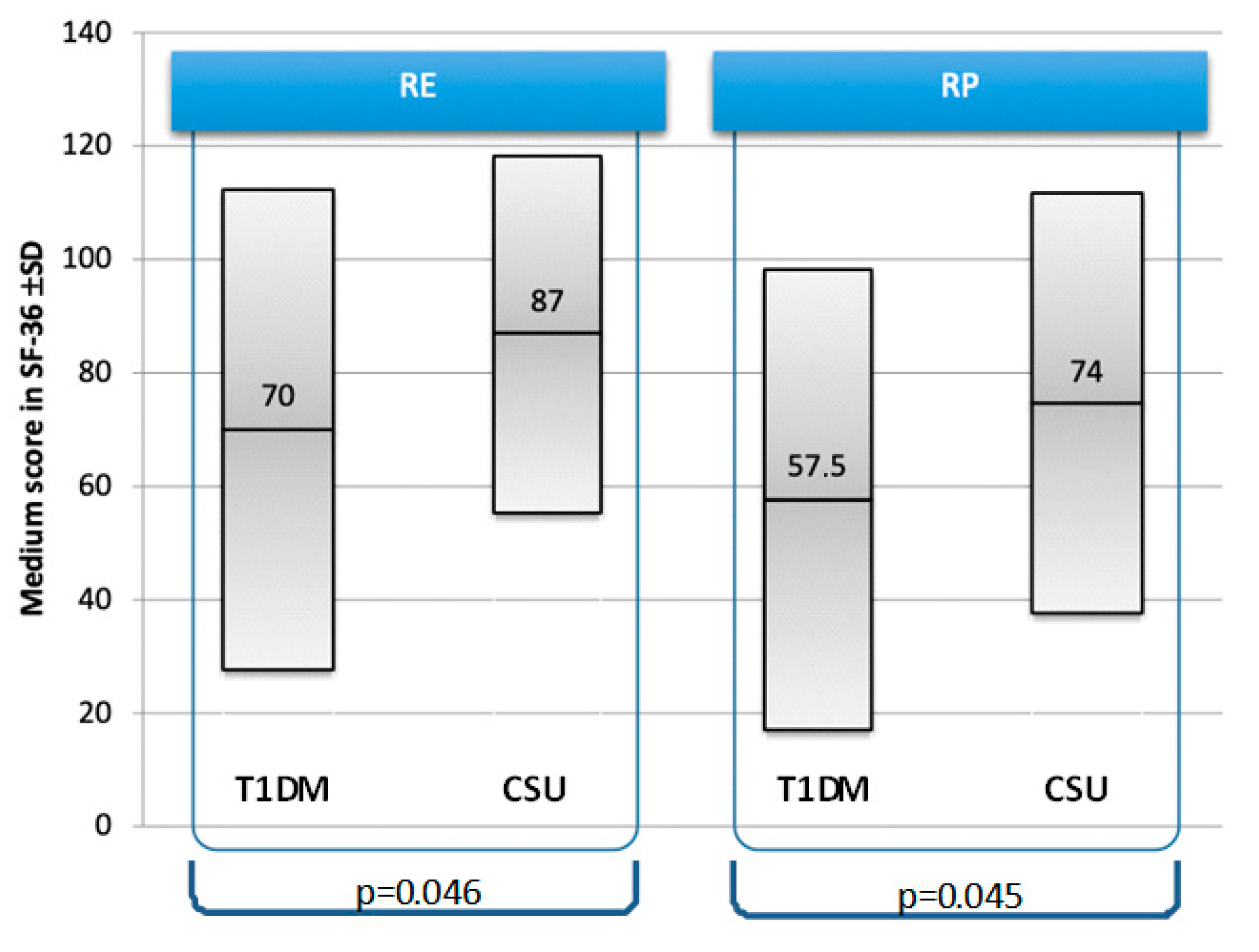
| RE | 100 | 66.7–100 | 100 | 100–100 | 0.17 |
| RP | 75 | 0–100 | 100 | 50–100 | 0.14 |
| SF | 100 | 50–100 | 72.5 | 37.5–100 | 0.03 |
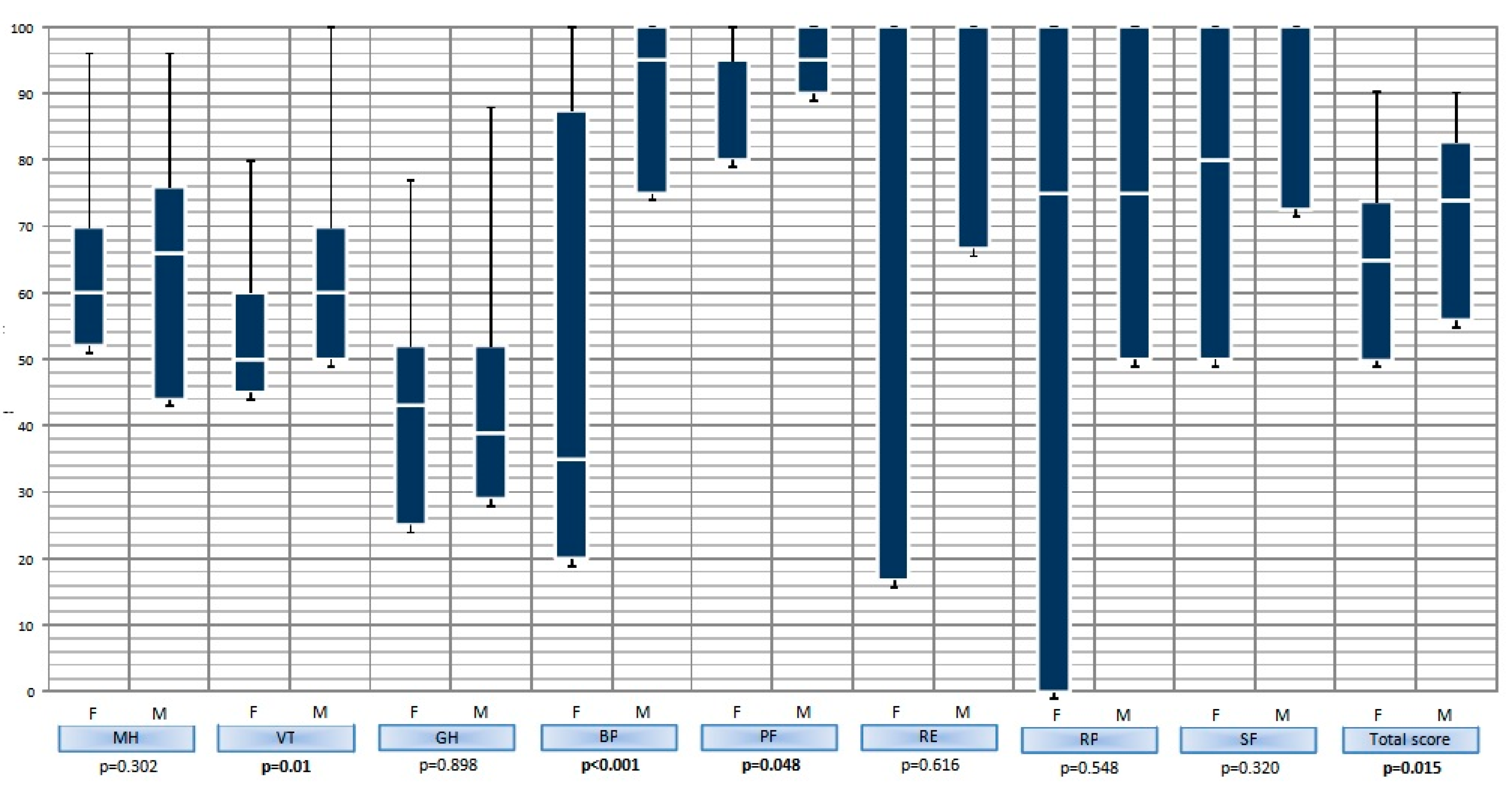
| SF-M | 100 | 72.5–100 | 75 | 37.5–87.5 | 0.03 |
| SF-F | 80 | 50–100 | 72.5 | 37.5–100 | 0.31 |
| Ts | 69.3 | 52.1–77.6 | 73.4 | 53.7–82.4 | 0.32 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brzoza, Z.; Nabrdalik, K.; Moos, L.; Kwiendacz, H.; Badura-Brzoza, K.; Jarolim, H.; Kapeluszna, K.; Gumprecht, J. Chronic Spontaneous Urticaria and Type 1 Diabetes Mellitus—Does Quality of Life Impairment Always Reflect Health Danger? J. Clin. Med. 2020, 9, 2505. https://doi.org/10.3390/jcm9082505
Brzoza Z, Nabrdalik K, Moos L, Kwiendacz H, Badura-Brzoza K, Jarolim H, Kapeluszna K, Gumprecht J. Chronic Spontaneous Urticaria and Type 1 Diabetes Mellitus—Does Quality of Life Impairment Always Reflect Health Danger? Journal of Clinical Medicine. 2020; 9(8):2505. https://doi.org/10.3390/jcm9082505
Chicago/Turabian StyleBrzoza, Zenon, Katarzyna Nabrdalik, Lukasz Moos, Hanna Kwiendacz, Karina Badura-Brzoza, Hanna Jarolim, Katarzyna Kapeluszna, and Janusz Gumprecht. 2020. "Chronic Spontaneous Urticaria and Type 1 Diabetes Mellitus—Does Quality of Life Impairment Always Reflect Health Danger?" Journal of Clinical Medicine 9, no. 8: 2505. https://doi.org/10.3390/jcm9082505