Core Outcome Measurement Instruments for Clinical Trials of Total Knee Arthroplasty: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Selection
2.1.1. Search Strategy
2.1.2. Inclusion and Exclusion Criteria
2.2. Quality Assessment and Data Extraction
2.3. Characteristics of the Instruments
2.4. Psychometric Qualities
2.5. Overall Quality
2.6. Statistical Analysis
3. Results
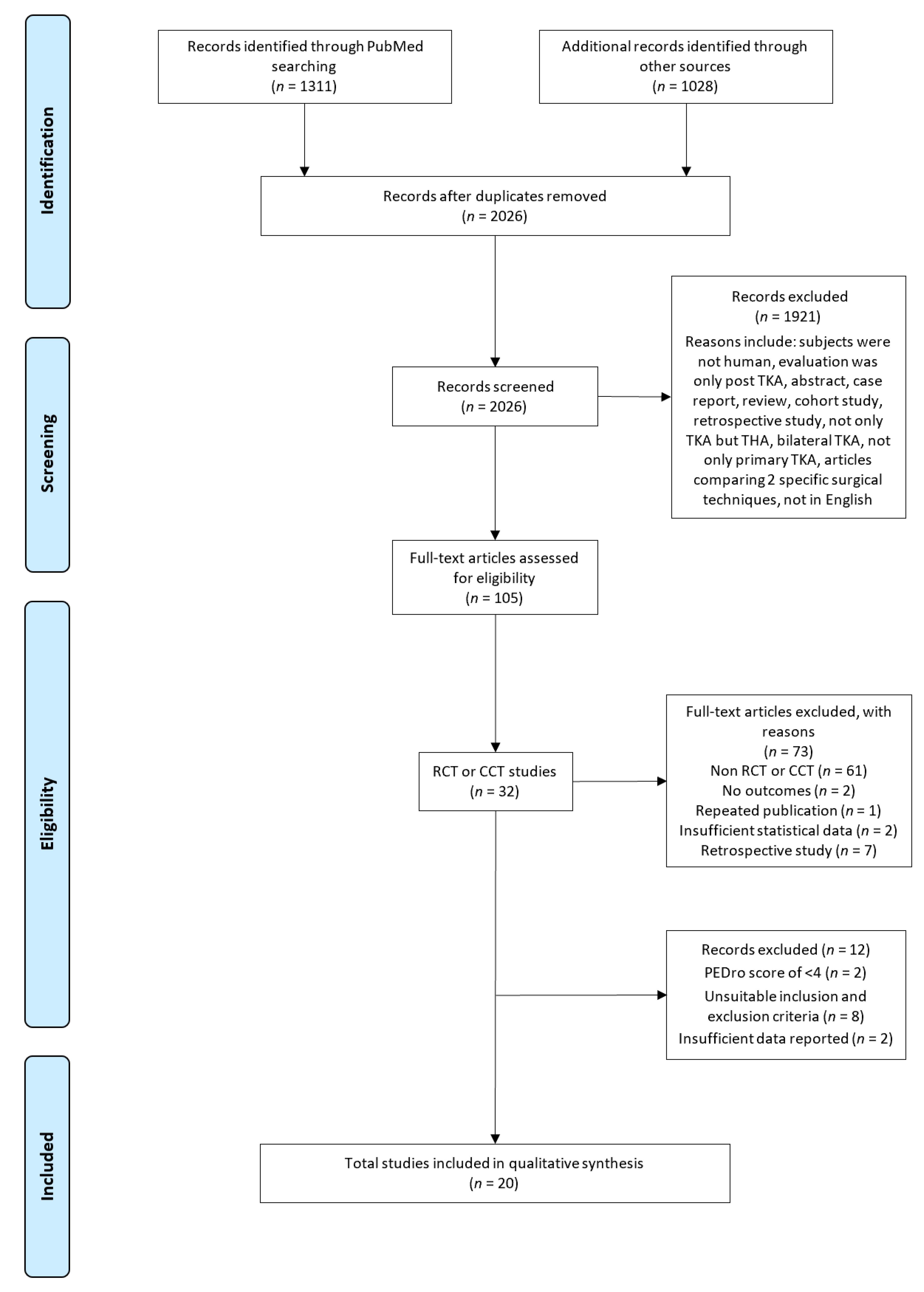
3.1. Study Selection
3.2. Study Characteristics
3.3. Description of Outcomes
3.4. Risk of Bias Within Studies
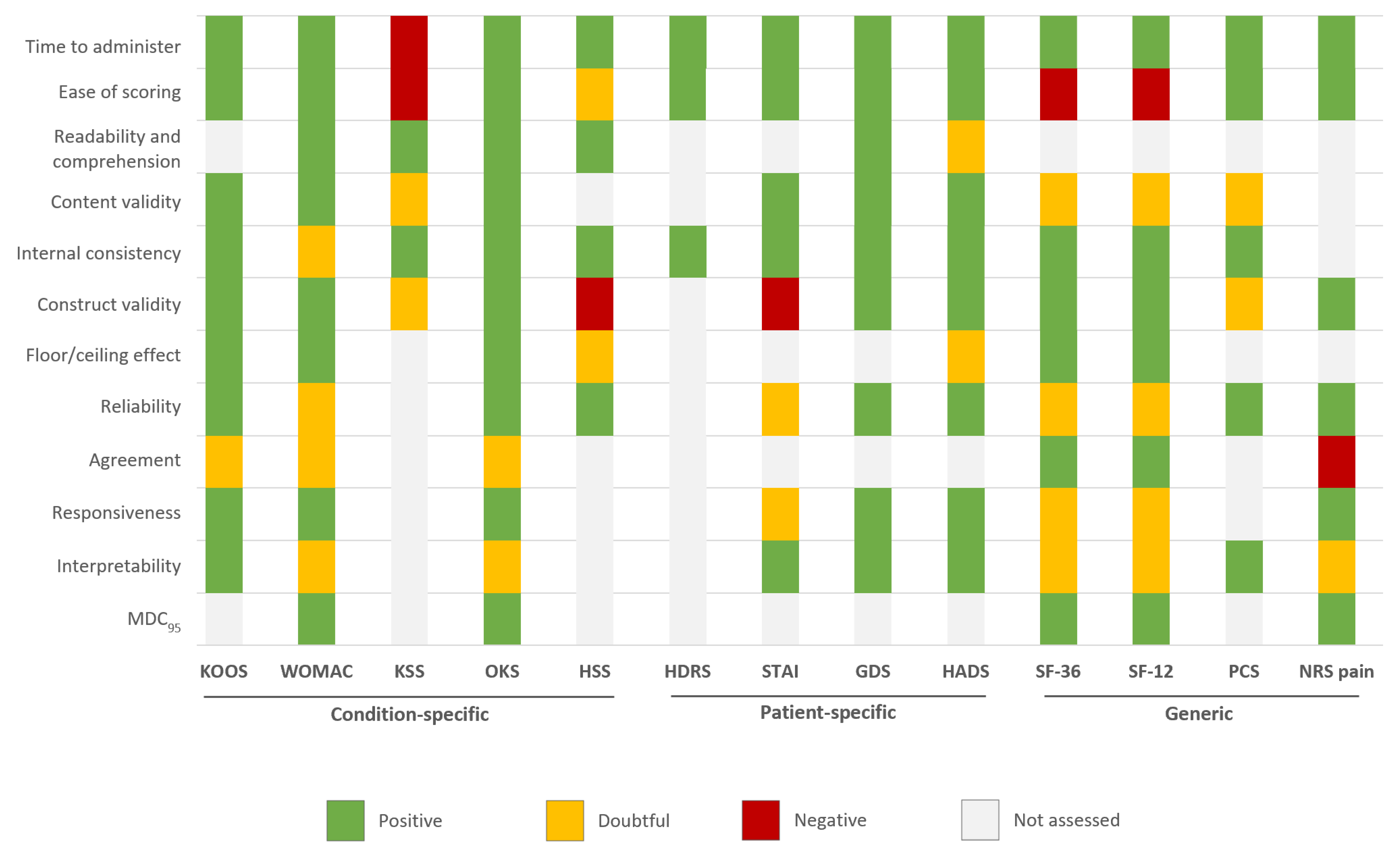
3.5. Psychometric Qualities of Tools
3.5.1. Content Validity
3.5.2. Internal Consistency
3.5.3. Construct Validity
3.5.4. Floor/Ceiling Effects
3.5.5. Reliability
3.5.6. Agreement
3.5.7. Responsiveness
3.5.8. Interpretability
3.5.9. Practical Burden
3.5.10. Cultural Adaptation
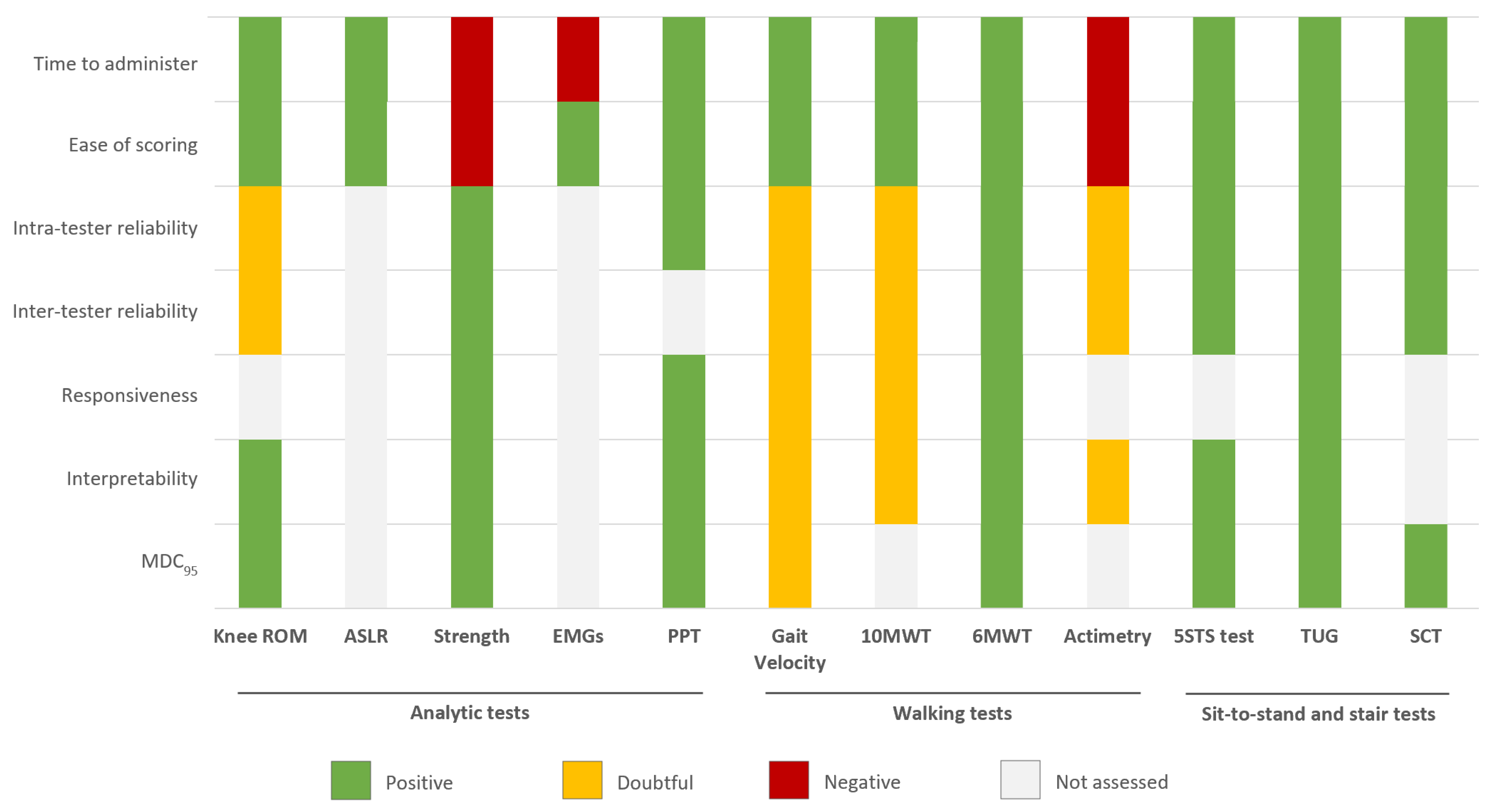
3.6. Psychometric Qualities of Physical Tests
3.6.1. Reliability
3.6.2. Responsiveness
3.6.3. Interpretability
3.6.4. Practical Burden
3.7. Overall Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Performance-Based Tests | Equipment/Space | Measure | Description/Instructions |
|---|---|---|---|
| Walking tests | |||
| 10MWT | Stopwatch 10 m (33 ft) marked walkway with an additional 2 m at each end for acceleration and deceleration. | Speed (m/s) | Walk as quickly but as safely as possible to a mark 10 m away starting off launched. Regular walking aid is allowed. |
| 6MWT | Timer/stopwatch Flat, hard-surfaced indoor walkway of 30 m marked with 1 m intervals. Chair or stool for resting | Distance (m) | The maximum distance that can be walked over a 6-min interval is recorded. Rest periods are allowed but included in the time Standardized encouragement (e.g., “keep going you are doing really well”) can be given at minute intervals. Regular walking aid is allowed. Practice test not needed in most clinical settings but if performed then at least 1 h rest should be allowed before the second test. The greatest distance is then recorded. |
| Sit-to-stand tests | |||
| 5STS test | Timer/stopwatch Straight back chair preferably without arms with approximately 43 cm (17 inch) seat height | Time (s) | From the sitting position with arms crossed at chest, stand up (sit down) as fast as possible for a total of five stands (i.e., test ends in standing). Fastest time of two trials is recorded in seconds. Same chair is required for re-testing. |
| TUG | Stopwatch Standard chair with armrests (approx. 46 cm (18 inch) seat height with 65 cm (26 inch) arm rest height) Marked 3 m (10 ft) walkway with turn point at end | Time (s) | Time to rise from a standard armchair, walk as quickly but as safely as possible distance of 3 m, turn, walk back to the chair and sit down. Usual footwear and regular walking aids allowed and recorded. Fastest of two trials is recorded in seconds. Same chair is needed for re-testing. |
| Stair tests | |||
| SCT | Stopwatch Flight of 12 stairs with 18 cm (7 inch) step height and handrails | Time (s) | Ascend and descend flight of 12 stairs as quickly as safe and comfortable. One handrail allowed but encouraged to only use legs. Total time to ascend and descend steps for one trial is recorded to nearest 100th second. |
| Reference | 1 * | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total (/10) | Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Winters et al., 2014 [34] | Y | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 4 | Moderate |
| Smith et al., 2014 [35] | Y | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 | Moderate |
| Bade et al., 2014 [36] | Y | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 | Moderate |
| Abdel et al., 2014 [37] | Y | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | High |
| Jenkins et al., 2014 [38] | Y | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | High |
| Thomas et al., 2014 [39] | Y | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 | Moderate |
| Huber et al., 2015 [40] | Y | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | High |
| Calatayud et al., 2017 [41] | Y | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | High |
| Bistolfi et al., 2017 [42] | Y | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 4 | Moderate |
| Hadlandsmyth et al., 2017 [43] | Y | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 4 | Moderate |
| Cooper et al., 2017 [44] | Y | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 | Moderate |
| Bonnefoy-Mazure et al., 2017 [45] | Y | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 | Moderate |
| Loyd et al., 2017 [46] | Y | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | High |
| Lin et al., 2018. [47] | Y | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | High |
| Husby et al., 2018 [48] | Y | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 | High |
| Paravlic et al., 2019 [49] | Y | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | High |
| Indelli et al., 2019 [50] | Y | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 6 | High |
| Jiang et al., 2019 [51] | Y | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 | Moderate |
| Liljensøe et al., 2019 [52] | Y | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 7 | High |
| Skoffer et al., 2019 [53] | Y | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 | High |
| Tool | Translations/Adaptations |
|---|---|
| Condition-specific | |
| KOOS | Available in English. The KOOS has been translated into Arabic, Austria-German, Bengali, Czech, Chinese, Croatian, Dutch, Danish, Estonian, Finnish, Filipino, French, Greek, Icelandic, Italian, Japanese, Korean, Latvian, Lithuanian, Malay, Norwegian, Persian, Portuguese, Polish, Romanian, Russian, Slovakian, Singapore English, Slovenian, Spanish, Swedish, Thai, Turkish, Ukrainian, Vietnamese, Welsh, and Zulu. |
| WOMAC | Available in English. The WOMAC has been translated into Arabic, German, French, Hebrew, Italian, Japanese, Singapore, Spanish, Korean, and Swedish. |
| KSS | Available in English. The KSS has been translated into French, German, Chinese, Portuguese, Dutch, and Turkish. |
| OKS | Available in English. The KSS has been translated into French, German, Chinese, Portuguese, Dutch, and Turkish. French, Portuguese, German, Danish, Thai, Estonian, Finnish, Greek, Indonesian, Japanese, Chinese, Russian, Arabic, Serbian, Swedish, Italian, Turkish, Malay, Welsh, Polish, Korean, Spanish. |
| HSS | Available in English and French |
| Patient-specific | |
| HDRS | Available in English. The HDRS has been translated into many languages such as Arabic, Bulgarian, Croatian, French, German, Georgian, Hebrew, Italian, Japanese, Russian, Spanish, |
| STAI | Available in English. The STAI has been translated into more than 48 languages |
| GDS | Available in English. The GDS has been translated into Arabic, Chinese, Creole, Danish, Dutch, Farsi, French, French Canadian, German, Greek, Hebrew, Hindi, Hungarian, Icelandic, Italian, Japanese, Korean, Lithuanian, Malay, Maltese, Norwegian, Portuguese, Romanian, Russian, Serbian, Spanish, Swedish, Thai, Turkish, Vietnamese, and Yiddish. |
| HADS | Available in English, as well as all other languages of Western Europe and many of Eastern Europe and Scandinavia, along with some African and Far East languages, including Arabic, Chinese, Danish, Dutch, Finnish, French, German, Hebrew, Hungarian, Italian, Japanese, Korean, Norwegian, Portuguese, Spanish, Swedish, Thai, and Urdu. |
| Generic | |
| SF-36 | Available in English. The SF-36 has been translated into more than 161 languages (Chinese, Dutch, Danish, French, Iranian, Italian, Japanese, Kiswahili, Norwegian, Portuguese, Spanish, and Swedish) |
| SF-12 | Available in English. The SF-36 has been translated into more than 141 languages. |
| PCS | Available in English and French |
| NRS pain | No translation needed. |
| Tool (References) | Time to Administer | Ease of Scoring | Readability and Comprehension | Content Validity | Internal Consistency | Construct Validity | Floor/Ceiling Effect | Reliability | Agree-ment | Respon-Siveness | Interpret-Ability | MDC95 | Positively Rated Qualities, no |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Condition-specific | |||||||||||||
| KOOS [37,40,73,78,79] | + | + | + | + | + | + §§§ | + | ø | + | + | 9 | ||
| WOMAC [8,18,34,63,79,89] | + | + | + | + | ø | + | + § | ø | ø | + | ø | + 0.5–1.3 pts | 8 |
| KSS [29,70] | - | - | + | ø | + * | ø | 2 | ||||||
| OKS [13,30,42,90] | + | + | + | + | + | + | + §§§§ | + | ø | + | ø | + 4.15 pts | 10 |
| HSS [51,69] | + | ø | + | + | - | ø | + | 3 | |||||
| Patient-specific | |||||||||||||
| HDRS | 0 | ||||||||||||
| STAI [72] | + | + | + | + | - | ø # | ø ˩ | + | 5 | ||||
| GDS [73] | + | + | + | + | + | + | + | + | + | 9 | |||
| HADS [10,17,52,82,87] | + | + | ø | + | + ** | + | ø | + | + | + | 8 | ||
| Generic | |||||||||||||
| SF-36 [7,8,27,34,35,75,88] | + | - | ø | + | + | + § and §§ | ø | + | ø | ø | + 2.0–7.8 pts | 6 | |
| SF-12 [7,28,34,38,88] | + | - | ø | + | + | + § and §§ | ø | + | ø | ø | + 3.8–5.4 pts | 6 | |
| PCS [82] | + | + | ø | + | ø | + | + | 5 | |||||
| NRS pain [83] | + | + | + | + | - | + | ø | + 1.33 pts | 6 | ||||
| Physical Test (References) | Domains ˥ | Necessary Equipment ǂ | Time to Administer (min) | Ease of Scoring | Intra-Tester Reliability | Inter-Tester Reliability | Respon-Siveness | Interpret-Ability | MDC95 | Positively Rated Qualities, no |
|---|---|---|---|---|---|---|---|---|---|---|
| Analytic tests | ||||||||||
| Knee ROM [90,99] | Articular limitation | Goniometer | + < 5 | + | ø | ø | + | + 6.6–10 ° | 4 | |
| ASLR [93] | Quadriceps strength | Goniometer or measuring tape | + < 5 | + | 2 | |||||
| Strength [87] | Lower extremity strength | Isometric or isokinetic dynamometer | −15–30 | + | + | + | + | + | + 5.1–9.3% * | 6 |
| EMGs | Neuromotor activation | Surface electromyography | −15–30 | - | 0 | |||||
| PPT [86] | Knee pain measure | Handheld pressure algometer | + < 5 | + | + | + | + | + 1.19–1.26 lb | 6 | |
| Performance-based tests | ||||||||||
| Walking tests | ||||||||||
| Gait velocity [100,101] | Patients’ functional mobility | Stopwatch, 30 m hallway | + < 5 | + | ø | ø | ø | ø | ø | 2 |
| 10MWT [91,102] | Patients’ functional mobility | Stopwatch, 15 m hallway | + < 5 | + | ø | ø | ø | ø | 2 | |
| 6MWT [89,91,102] | Patients’ functional mobility | 30 m course marked off in meters, stopwatch | + 10 | + | + | + | + | + | + 61.34 m | 6 |
| Actimetry [103] | Patients’ physical activity | Accelerometer | - or NA | - | ø | ø | ø | 0 | ||
| Sit-to-stand tests | ||||||||||
| 5STS test [84,104,105] | Lower extremity strength and balance | Chair, stopwatch | + < 5 | + | + | + | + | + 2.1–2.38 s | 6 | |
| TUG [91,92,94,102,104] | Patients’ functional mobility | Armchair, stopwatch | + < 5 | + | + | + | + | + | + 1.10–2.27 s | 7 |
| Stair tests | ||||||||||
| SCT [27,88,95] | Patients’ functional mobility | Regular stairwell, stopwatch | + < 5 | + | + | + | + 3.2–5.49 s | 5 | ||
References
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- O’Neill, T.W.; McCabe, P.S.; McBeth, J. Update on the epidemiology, risk factors and disease outcomes of osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2018, 32, 312–326. [Google Scholar] [CrossRef]
- Cleveland, R.J.; Alvarez, C.; Schwartz, T.A.; Losina, E.; Renner, J.B.; Jordan, J.M.; Callahan, L.F. The impact of painful knee osteoarthritis on mortality: A community–based cohort study with over 24 years of follow–up. Osteoarthr. Cartil. 2018. [Google Scholar] [CrossRef] [Green Version]
- Deveza, L.A.; Loeser, R.F. Is osteoarthritis one disease or a collection of many? Rheumatol. Oxf. Engl. 2018, 57, iv34–iv42. [Google Scholar] [CrossRef] [Green Version]
- Karsdal, M.A.; Bihlet, A.; Byrjalsen, I.; Alexandersen, P.; Ladel, C.; Michaels, M.; Andersen, J.R.; Riis, B.J.; Kraus, V.; Bay-Jensen, A.C.; et al. OA phenotypes, rather than disease stage, drive structural progression—Identification of structural progressors from 2 phase III randomized clinical studies with symptomatic knee OA. Osteoarthr. Cartil. 2015, 23, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, L.; Hagen, K.B.; Bijlsma, J.W.J.; Andreassen, O.; Christensen, P.; Conaghan, P.G.; Doherty, M.; Geenen, R.; Hammond, A.; Kjeken, I.; et al. EULAR recommendations for the non–pharmacological core management of hip and knee osteoarthritis. Ann. Rheum. Dis. 2013, 72, 1125–1135. [Google Scholar] [CrossRef] [Green Version]
- Lapane, K.L.; Yang, S.; Driban, J.B.; Liu, S.-H.; Dubé, C.E.; McAlindon, T.E.; Eaton, C.B. Effects of prescription nonsteroidal antiinflammatory drugs on symptoms and disease progression among patients with knee osteoarthritis. Arthritis Rheumatol. Hoboken NJ 2015, 67, 724–732. [Google Scholar] [CrossRef] [Green Version]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [Green Version]
- Maradit Kremers, H.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of Total Hip and Knee Replacement in the United States. J. Bone Jt. Surg. Am. 2015, 97, 1386–1397. [Google Scholar] [CrossRef] [Green Version]
- Colas, S.; Occean, B.-V.; Rudnichi, A.; Dray-Spira, R.; Zureik, M. Étude d’utilisation des prothèses articulaires de genou en France entre 2008 et 2013. Rev. DÉpidémiologie St. Publique 2016, 64, S23. [Google Scholar] [CrossRef]
- Bellamy, N. Osteoarthritis clinical trials: Candidate variables and clinimetric properties. J. Rheumatol. 1997, 24, 768–778. [Google Scholar]
- Bellamy, N.; Kirwan, J.; Boers, M.; Brooks, P.; Strand, V.; Tugwell, P.; Altman, R.; Brandt, K.; Dougados, M.; Lequesne, M. Recommendations for a core set of outcome measures for future phase III clinical trials in knee, hip, and hand osteoarthritis. Consensus development at OMERACT III. J. Rheumatol. 1997, 24, 799–802. [Google Scholar]
- Pisoni, C.; Giardini, A.; Majani, G.; Maini, M. International Classification of Functioning, Disability and Health (ICF) core sets for osteoarthritis. A useful tool in the follow-up of patients after joint arthroplasty. Eur. J. Phys. Rehabil. Med. 2008, 44, 377–385. [Google Scholar]
- World Health Organization. Regional Office for Europe Guidelines for the clinical investigation of drugs used in rheumatic diseases: European drug guidelines. Cph. Eur. Leag. Rheum. 1985, 49. [Google Scholar]
- Allen, K.D.; Bierma-Zeinstra, S.M.A.; Foster, N.E.; Golightly, Y.M.; Hawker, G. OARSI Clinical Trials Recommendations: Design and conduct of implementation trials of interventions for osteoarthritis. Osteoarthr. Cartil. 2015, 23, 826–838. [Google Scholar] [CrossRef] [Green Version]
- Lequesne, M.; Brandt, K.; Bellamy, N.; Moskowitz, R.; Menkes, C.J.; Pelletier, J.P.; Altman, R. Guidelines for testing slow acting drugs in osteoarthritis. J. Rheumatol. Suppl. 1994, 41, 65–71. [Google Scholar]
- Ramkumar, P.N.; Harris, J.D.; Noble, P.C. Patient–reported outcome measures after total knee arthroplasty: A systematic review. Bone Jt. Res. 2015, 4, 120–127. [Google Scholar] [CrossRef]
- King, S.W.; Cunningham, C.M.; Royeca, J.M.; Madegowda, R.; Sha, S.; Pandit, H. Patient–reported outcome measures review: Are current outcomes assessment tools sensitive enough to assess the reasons for patients’ “unhappiness”? J. Arthrosc. Jt. Surg. 2020. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice, 3rd ed.; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Rogers, J.C.; Irrgang, J.J. Measures of adult lower extremity function: The American Academy of Orthopedic Surgeons Lower Limb Questionnaire, The Activities of Daily Living Scale of the Knee Outcome Survey (ADLS), Foot Function Index (FFI), Functional Assessment System (FAS), Harris Hip Score (HHS), Index of Severity for Hip Osteoarthritis (ISH), Index of Severity for Knee Osteoarthritis (ISK), Knee Injury and Osteoarthritis Outcome Score (KOOS), and Western Ontario and McMaster Universities Osteoarthritis Index (WOMACTM). Arthritis Care Res. 2003, 49, S67–S84. [Google Scholar] [CrossRef]
- Sun, Y.; Stürmer, T.; Günther, K.P.; Brenner, H. Reliability and validity of clinical outcome measurements of osteoarthritis of the hip and knee—A review of the literature. Clin. Rheumatol. 1997, 16, 185–198. [Google Scholar] [CrossRef]
- Garratt, A.M.; Brealey, S.; Gillespie, W.J. DAMASK Trial Team Patient–assessed health instruments for the knee: A structured review. Rheumatol. Oxf. Engl. 2004, 43, 1414–1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veenhof, C.; Bijlsma, J.W.J.; van den Ende, C.H.M.; van Dijk, G.M.; Pisters, M.F.; Dekker, J. Psychometric evaluation of osteoarthritis questionnaires: A systematic review of the literature. Arthritis Rheum. 2006, 55, 480–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alviar, M.J.; Olver, J.; Brand, C.; Tropea, J.; Hale, T.; Pirpiris, M.; Khan, F. Do patient–reported outcome measures in hip and knee arthroplasty rehabilitation have robust measurement attributes? A systematic review. J. Rehabil. Med. 2011, 43, 572–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F. PRISMA–IPD Development Group Preferred Reporting Items for Systematic Review and Meta-Analyses of individual participant data: The PRISMA–IPD Statement. JAMA 2015, 313, 1657–1665. [Google Scholar] [CrossRef]
- Moseley, A.M.; Herbert, R.D.; Sherrington, C.; Maher, C.G. Evidence for physiotherapy practice: A survey of the Physiotherapy Evidence Database (PEDro). Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Almeida, G.J.; Schroeder, C.A.; Gil, A.B.; Fitzgerald, G.K.; Piva, S.R. Interrater reliability and validity of the stair ascend/descend test in subjects with total knee arthroplasty. Arch. Phys. Med. Rehabil. 2010, 91, 932–938. [Google Scholar] [CrossRef] [Green Version]
- Bot, S.; Terwee, C.; van der Windt, D.; Bouter, L.; Dekker, J.; De Vet, H. Psychometric evaluation of self–report questionnaires: The development of a checklist. Second Workshop Res. Methodol. 2003. [Google Scholar]
- Lohr, K.N.; Aaronson, N.K.; Alonso, J.; Burnam, M.A.; Patrick, D.L.; Perrin, E.B.; Roberts, J.S. Evaluating quality–of–life and health status instruments: Development of scientific review criteria. Clin. Ther. 1996, 18, 979–992. [Google Scholar] [CrossRef]
- Bombardier, C.; Tugwell, P. Methodological considerations in functional assessment. J. Rheumatol. Suppl. 1987, 14, 6–10. [Google Scholar]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2010, 19, 539–549. [Google Scholar] [CrossRef] [Green Version]
- Bot, S.D.M.; Terwee, C.B.; van der Windt, D.A.W.M.; Bouter, L.M.; Dekker, J.; de Vet, H.C.W. Clinimetric evaluation of shoulder disability questionnaires: A systematic review of the literature. Ann. Rheum. Dis. 2004, 63, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winters, J.D.; Christiansen, C.L.; Stevens-Lapsley, J.E. Preliminary investigation of rate of torque development deficits following total knee arthroplasty. Knee 2014, 21, 382–386. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.W.; Marcus, R.L.; Peters, C.L.; Pelt, C.E.; Tracy, B.L.; LaStayo, P.C. Muscle force steadiness in older adults before and after total knee arthroplasty. J. Arthroplast. 2014, 29, 1143–1148. [Google Scholar] [CrossRef]
- Bade, M.J.; Kittelson, J.M.; Kohrt, W.M.; Stevens-Lapsley, J.E. Predicting functional performance and range of motion outcomes after total knee arthroplasty. Am. J. Phys. Med. Rehabil. 2014, 93, 579–585. [Google Scholar] [CrossRef] [Green Version]
- Abdel, M.P.; Parratte, S.; Blanc, G.; Ollivier, M.; Pomero, V.; Viehweger, E.; Argenson, J.-N.A. No benefit of patient–specific instrumentation in TKA on functional and gait outcomes: A randomized clinical trial. Clin. Orthop. 2014, 472, 2468–2476. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, D.; Rodriguez, J.; Ranawat, A.; Alexiades, M.; Deshmukh, A.; Fukunaga, T.; Greiz, M.; Rathod, P.; McHugh, M. A randomized, controlled, prospective study evaluating the effect of patellar eversion on functional outcomes in primary total knee arthroplasty. J. Bone Jt. Surg. Am. 2014, 96, 851–858. [Google Scholar] [CrossRef] [Green Version]
- Thomas, A.C.; Judd, D.L.; Davidson, B.S.; Eckhoff, D.G.; Stevens-Lapsley, J.E. Quadriceps/hamstrings co-activation increases early after total knee arthroplasty. Knee 2014, 21, 1115–1119. [Google Scholar] [CrossRef] [Green Version]
- Huber, E.O.; Roos, E.M.; Meichtry, A.; de Bie, R.A.; Bischoff-Ferrari, H.A. Effect of preoperative neuromuscular training (NEMEX-TJR) on functional outcome after total knee replacement: An assessor–blinded randomized controlled trial. BMC Musculoskelet. Disord. 2015, 16, 101. [Google Scholar] [CrossRef] [Green Version]
- Calatayud, J.; Casaña, J.; Ezzatvar, Y.; Jakobsen, M.D.; Sundstrup, E.; Andersen, L.L. High–intensity preoperative training improves physical and functional recovery in the early post–operative periods after total knee arthroplasty: A randomized controlled trial. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2017, 25, 2864–2872. [Google Scholar] [CrossRef]
- Bistolfi, A.; Bettoni, E.; Aprato, A.; Milani, P.; Berchialla, P.; Graziano, E.; Massazza, G.; Lee, G.C. The presence and influence of mild depressive symptoms on post–operative pain perception following primary total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2017, 25, 2792–2800. [Google Scholar] [CrossRef] [PubMed]
- Hadlandsmyth, K.; Sabic, E.; Zimmerman, M.B.; Sluka, K.A.; Herr, K.A.; Clark, C.R.; Noiseux, N.O.; Callaghan, J.J.; Geasland, K.M.; Embree, J.L.; et al. Relationships among pain intensity, pain–related distress, and psychological distress in pre–surgical total knee arthroplasty patients: A secondary analysis. Psychol. Health Med. 2017, 22, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Cooper, N.A.; Rakel, B.A.; Zimmerman, B.; Tonelli, S.M.; Herr, K.A.; Clark, C.R.; Noiseux, N.O.; Callaghan, J.J.; Sluka, K.A. Predictors of multidimensional functional outcomes after total knee arthroplasty. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2017, 35, 2790–2798. [Google Scholar] [CrossRef]
- Bonnefoy-Mazure, A.; Martz, P.; Armand, S.; Sagawa, Y.; Suva, D.; Turcot, K.; Miozzari, H.H.; Lübbeke, A. Influence of Body Mass Index on Sagittal Knee Range of Motion and Gait Speed Recovery 1-Year After Total Knee Arthroplasty. J. Arthroplast. 2017, 32, 2404–2410. [Google Scholar] [CrossRef]
- Loyd, B.J.; Jennings, J.M.; Judd, D.L.; Kim, R.H.; Wolfe, P.; Dennis, D.A.; Stevens-Lapsley, J.E. Influence of Hip Abductor Strength on Functional Outcomes Before and After Total Knee Arthroplasty: Post Hoc Analysis of a Randomized Controlled Trial. Phys. Ther. 2017, 97, 896–903. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Lee, S.-Y.; Su, W.-R.; Kao, C.-C.; Tai, T.-W.; Chen, T.-B. Effects of nurse-led lower extremity strength training on knee function recovery in patients who underwent total knee replacement. J. Clin. Nurs. 2018, 27, 1836–1845. [Google Scholar] [CrossRef]
- Husby, V.S.; Foss, O.A.; Husby, O.S.; Winther, S.B. Randomized controlled trial of maximal strength training vs. standard rehabilitation following total knee arthroplasty. Eur. J. Phys. Rehabil. Med. 2018, 54, 371–379. [Google Scholar] [CrossRef]
- Paravlic, A.H.; Pisot, R.; Marusic, U. Specific and general adaptations following motor imagery practice focused on muscle strength in total knee arthroplasty rehabilitation: A randomized controlled trial. PLoS ONE 2019, 14, e0221089. [Google Scholar] [CrossRef] [Green Version]
- Indelli, P.F.; Risitano, S.; Hall, K.E.; Leonardi, E.; Migliore, E. Effect of polyethylene conformity on total knee arthroplasty early clinical outcomes. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2019, 27, 1028–1034. [Google Scholar] [CrossRef]
- Jiang, H.-H.; Jian, X.-F.; Shangguan, Y.-F.; Qing, J.; Chen, L.-B. Effects of Enhanced Recovery After Surgery in Total Knee Arthroplasty for Patients Older Than 65 Years. Orthop. Surg. 2019, 11, 229–235. [Google Scholar] [CrossRef]
- Liljensøe, A.; Laursen, J.O.; Bliddal, H.; Søballe, K.; Mechlenburg, I. Weight Loss Intervention Before Total Knee Replacement: A 12-Month Randomized Controlled Trial. Scand. J. Surg. SJS Off. Organ. Finn. Surg. Soc. Scand. Surg. Soc. 2019, 1457496919883812. [Google Scholar] [CrossRef] [Green Version]
- Skoffer, B.; Maribo, T.; Mechlenburg, I.; Korsgaard, C.G.; Søballe, K.; Dalgas, U. Efficacy of preoperative progressive resistance training in patients undergoing total knee arthroplasty: 12–month follow–up data from a randomized controlled trial. Clin. Rehabil. 2019, 34, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Toksvig-Larsen, S. Knee injury and Osteoarthritis Outcome Score (KOOS)—Validation and comparison to the WOMAC in total knee replacement. Health Qual. Life Outcomes 2003, 1, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Groot, I.B.; Favejee, M.M.; Reijman, M.; Verhaar, J.A.; Terwee, C.B. The Dutch version of the knee injury and osteoarthritis outcome score: A validation study. Health Qual. Life Outcomes 2008, 6, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandek, B.; Ware, J.E. Validity and Responsiveness of the Knee Injury and Osteoarthritis Outcome Score: A Comparative Study Among Total Knee Replacement Patients. Arthritis Care Res. 2017, 69, 817–825. [Google Scholar] [CrossRef]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [Green Version]
- Ornetti, P.; Parratte, S.; Gossec, L.; Tavernier, C.; Argenson, J.-N.; Roos, E.M.; Guillemin, F.; Maillefert, J.F. Cross-cultural adaptation and validation of the French version of the Knee injury and Osteoarthritis Outcome Score (KOOS) in knee osteoarthritis patients. Osteoarthr. Cartil. 2008, 16, 423–428. [Google Scholar] [CrossRef] [Green Version]
- Bombardier, C.; Melfi, C.A.; Paul, J.; Green, R.; Hawker, G.; Wright, J.; Coyte, P. Comparison of a generic and a disease–specific measure of pain and physical function after knee replacement surgery. Med. Care 1995, 33, AS131–CAS144. [Google Scholar]
- McConnell, S.; Kolopack, P.; Davis, A.M. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): A review of its utility and measurement properties. Arthritis Rheum. 2001, 45, 453–461. [Google Scholar] [CrossRef]
- Angst, F.; Aeschlimann, A.; Stucki, G. Smallest detectable and minimal clinically important differences of rehabilitation intervention with their implications for required sample sizes using WOMAC and SF–36 quality of life measurement instruments in patients with osteoarthritis of the lower extremities. Arthritis Rheum. 2001, 45, 384–391. [Google Scholar] [CrossRef]
- Dunbar, M.J.; Robertsson, O.; Ryd, L.; Lidgren, L. Appropriate questionnaires for knee arthroplasty. Results of a survey of 3600 patients from The Swedish Knee Arthroplasty Registry. J. Bone Jt. Surg. Br. 2001, 83, 339–344. [Google Scholar] [CrossRef]
- Stratford, P.W.; Kennedy, D.M.; Woodhouse, L.J.; Spadoni, G.F. Measurement properties of the WOMAC LK 3.1 pain scale. Osteoarthr. Cartil. 2007, 15, 266–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noble, P.C.; Scuderi, G.R.; Brekke, A.C.; Sikorskii, A.; Benjamin, J.B.; Lonner, J.H.; Chadha, P.; Daylamani, D.A.; Scott, W.N.; Bourne, R.B. Development of a new Knee Society scoring system. Clin. Orthop. 2012, 470, 20–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Culliton, S.E.; Bryant, D.M.; MacDonald, S.J.; Hibbert, K.M.; Chesworth, B.M. Validity and Internal Consistency of the New Knee Society Knee Scoring System. Clin. Orthop. 2018, 476, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Fitzpatrick, R.; Murray, D.; Carr, A. Questionnaire on the perceptions of patients about total knee replacement. J. Bone Jt. Surg. Br. 1998, 80-B, 63–69. [Google Scholar] [CrossRef]
- Harris, K.; Dawson, J.; Gibbons, E.; Lim, C.R.; Beard, D.J.; Fitzpatrick, R.; Price, A.J. Systematic review of measurement properties of patient-reported outcome measures used in patients undergoing hip and knee arthroplasty. Patient Relat. Outcome Meas. 2016, 7, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, F.; Ye, H.; Zhang, Y.; Liu, X.; Lei, T.; Li, S.-C. Extension from inpatients to outpatients: Validity and reliability of the Oxford Knee Score in measuring health outcomes in patients with knee osteoarthritis. Int. J. Rheum. Dis. 2011, 14, 206–210. [Google Scholar] [CrossRef]
- Beard, D.J.; Harris, K.; Dawson, J.; Doll, H.; Murray, D.W.; Carr, A.J.; Price, A.J. Meaningful changes for the Oxford hip and knee scores after joint replacement surgery. J. Clin. Epidemiol. 2015, 68, 73–79. [Google Scholar] [CrossRef]
- Jourdan, C.; Poiraudeau, S.; Descamps, S.; Nizard, R.; Hamadouche, M.; Anract, P.; Boisgard, S.; Galvin, M.; Ravaud, P. Comparison of patient and surgeon expectations of total hip arthroplasty. PLoS ONE 2012, 7, e30195. [Google Scholar] [CrossRef]
- Neuprez, A.; Delcour, J.-P.; Fatemi, F.; Gillet, P.; Mawet, M.; François, G.; Bruyère, O.; Crielaard, J.-M.; Gosset, C.; Reginster, J.-Y. Development and validation of the French version of a tool assessing patient’s expectations in lower limb osteoarthritis. J. Orthop. 2015, 12, 46–57. [Google Scholar] [CrossRef] [Green Version]
- Julian, L.J. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS–A). Arthritis Care Res. 2011, 63, S467–S472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smarr, K.L.; Keefer, A.L. Measures of depression and depressive symptoms: Beck Depression Inventory–II (BDI–II), Center for Epidemiologic Studies Depression Scale (CES–D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire–9 (PHQ–9). Arthritis Care Res. 2011, 63, S454–S466. [Google Scholar] [CrossRef]
- Axford, J.; Butt, A.; Heron, C.; Hammond, J.; Morgan, J.; Alavi, A.; Bolton, J.; Bland, M. Prevalence of anxiety and depression in osteoarthritis: Use of the Hospital Anxiety and Depression Scale as a screening tool. Clin. Rheumatol. 2010, 29, 1277–1283. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Spinhoven, P.; Ormel, J.; Sloekers, P.P.; Kempen, G.I.; Speckens, A.E.; Van Hemert, A.M. A validation study of the Hospital Anxiety and Depression Scale (HADS) in different groups of Dutch subjects. Psychol. Med. 1997, 27, 363–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perneger, T.V.; Leplège, A.; Etter, J.F.; Rougemont, A. Validation of a French–language version of the MOS 36–Item Short Form Health Survey (SF-36) in young healthy adults. J. Clin. Epidemiol. 1995, 48, 1051–1060. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A. Comparison of the short form–12 (SF–12) health status questionnaire with the SF–36 in patients with knee osteoarthritis who have replacement surgery. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2016, 24, 2620–2626. [Google Scholar] [CrossRef]
- Escobar, A.; Quintana, J.M.; Bilbao, A.; Aróstegui, I.; Lafuente, I.; Vidaurreta, I. Responsiveness and clinically important differences for the WOMAC and SF-36 after total knee replacement. Osteoarthr. Cartil. 2007, 15, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Conner-Spady, B.L.; Marshall, D.A.; Bohm, E.; Dunbar, M.J.; Noseworthy, T.W. Comparing the validity and responsiveness of the EQ–5D–5L to the Oxford hip and knee scores and SF-12 in osteoarthritis patients 1 year following total joint replacement. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2018, 27, 1311–1322. [Google Scholar] [CrossRef]
- Gandhi, S.K.; Salmon, J.W.; Zhao, S.Z.; Lambert, B.L.; Gore, P.R.; Conrad, K. Psychometric evaluation of the 12–item short–form health survey (SF–12) in osteoarthritis and rheumatoid arthritis clinical trials. Clin. Ther. 2001, 23, 1080–1098. [Google Scholar] [CrossRef]
- Youngcharoen, P.; Aree-Ue, S.; Saraboon, Y. Validation of pain catastrophizing scale Thai version in older adults with knee osteoarthritis. Innov. Aging 2017, 1, 871. [Google Scholar] [CrossRef] [Green Version]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test–retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J. Pain Res. 2018, 11, 851–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unver, B.; Kalkan, S.; Yuksel, E.; Kahraman, T.; Karatosun, V. Reliability of the 50–foot walk test and 30–sec chair stand test in total knee arthroplasty. Acta Ortop. Bras. 2015, 23, 184–187. [Google Scholar] [CrossRef] [Green Version]
- Bellamy, N. Outcome measurement in osteoarthritis clinical trials. J. Rheumatol. Suppl. 1995, 43, 49–51. [Google Scholar] [PubMed]
- Mutlu, E.K.; Ozdincler, A.R. Reliability and responsiveness of algometry for measuring pressure pain threshold in patients with knee osteoarthritis. J. Phys. Ther. Sci. 2015, 27, 1961–1965. [Google Scholar] [CrossRef] [Green Version]
- Lienhard, K.; Lauermann, S.P.; Schneider, D.; Item-Glatthorn, J.F.; Casartelli, N.C.; Maffiuletti, N.A. Validity and reliability of isometric, isokinetic and isoinertial modalities for the assessment of quadriceps muscle strength in patients with total knee arthroplasty. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2013, 23, 1283–1288. [Google Scholar] [CrossRef]
- Tolk, J.J.; Janssen, R.P.A.; Prinsen, C.A.C.; Latijnhouwers, D.A.J.M.; van der Steen, M.C.; Bierma-Zeinstra, S.M.A.; Reijman, M. The OARSI core set of performance-based measures for knee osteoarthritis is reliable but not valid and responsive. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2019, 27, 2898–2909. [Google Scholar] [CrossRef]
- Ateef, M.; Kulandaivelan, S.; Tahseen, S. Test–Retest Reliability and Correlates of 6–Minute Walk Test in Patients with Primary Osteoarthritis of Knees. Available online: https://link.galegroup.com/apps/doc/A578163738/AONE?sid=lms (accessed on 2 January 2020).
- Lavernia, C.; D’Apuzzo, M.; Rossi, M.D.; Lee, D. Accuracy of knee range of motion assessment after total knee arthroplasty. J. Arthroplast. 2008, 23, 85–91. [Google Scholar] [CrossRef]
- Kennedy, D.M.; Stratford, P.W.; Wessel, J.; Gollish, J.D.; Penney, D. Assessing stability and change of four performance measures: A longitudinal study evaluating outcome following total hip and knee arthroplasty. BMC Musculoskelet. Disord. 2005, 6, 3. [Google Scholar] [CrossRef] [Green Version]
- Yuksel, E.; Kalkan, S.; Cekmece, S.; Unver, B.; Karatosun, V. Assessing Minimal Detectable Changes and Test–Retest Reliability of the Timed Up and Go Test and the 2–Minute Walk Test in Patients With Total Knee Arthroplasty. J. Arthroplast. 2017, 32, 426–430. [Google Scholar] [CrossRef]
- Ishii, Y.; Noguchi, H.; Sato, J.; Ishii, H.; Yamamoto, T.; Sakurai, T.; Toyabe, S.-I. Clinical relevance of active straight leg raising, standing up, and walking after total knee arthroplasty in a cross–sectional study. Eur. J. Orthop. Surg. Traumatol. Orthop. Traumatol. 2018, 28, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.; Anwer, S.; Brismée, J.-M. The reliability and minimal detectable change of Timed Up and Go test in individuals with grade 1–3 knee osteoarthritis. BMC Musculoskelet. Disord. 2015, 16, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobson, F.; Hinman, R.S.; Roos, E.M.; Abbott, J.H.; Stratford, P.; Davis, A.M.; Buchbinder, R.; Snyder-Mackler, L.; Henrotin, Y.; Thumboo, J.; et al. OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1042–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagby, R.M.; Ryder, A.G.; Schuller, D.R.; Marshall, M.B. The Hamilton Depression Rating Scale: Has the gold standard become a lead weight? Am. J. Psychiatry 2004, 161, 2163–2177. [Google Scholar] [CrossRef] [PubMed]
- Roussel, N.A.; Nijs, J.; Truijen, S.; Smeuninx, L.; Stassijns, G. Low back pain: Clinimetric properties of the Trendelenburg test, active straight leg raise test, and breathing pattern during active straight leg raising. J. Manip. Physiol. Ther. 2007, 30, 270–278. [Google Scholar] [CrossRef]
- de Vet, H.C.W.; Terwee, C.B.; Knol, D.L.; Bouter, L.M. When to use agreement versus reliability measures. J. Clin. Epidemiol. 2006, 59, 1033–1039. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, T.L.; Christensen, M.; Christensen, S.S.; Olsen, M.; Bandholm, T. Reliability of knee joint range of motion and circumference measurements after total knee arthroplasty: Does tester experience matter? Physiother. Res. Int. J. Res. Clin. Phys. Ther. 2010, 15, 126–134. [Google Scholar] [CrossRef]
- Motyl, J.M.; Driban, J.B.; McAdams, E.; Price, L.L.; McAlindon, T.E. Test–retest reliability and sensitivity of the 20–meter walk test among patients with knee osteoarthritis. BMC Musculoskelet. Disord. 2013, 14, 166. [Google Scholar] [CrossRef] [Green Version]
- Ornetti, P.; Maillefert, J.-F.; Laroche, D.; Morisset, C.; Dougados, M.; Gossec, L. Gait analysis as a quantifiable outcome measure in hip or knee osteoarthritis: A systematic review. Jt. Bone Spine Rev. Rhum. 2010, 77, 421–425. [Google Scholar] [CrossRef]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age–and gender–related test performance in community–dwelling elderly people: Six–Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar]
- Almeida, G.J.; Irrgang, J.J.; Fitzgerald, G.K.; Jakicic, J.M.; Piva, S.R. Reliability of Physical Activity Measures During Free–Living Activities in People After Total Knee Arthroplasty. Phys. Ther. 2016, 96, 898–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huber, E.O.; Meichtry, A.; de Bie, R.A.; Bastiaenen, C.H. Construct validity of change scores of the Chair Stand Test versus Timed Up and Go Test, KOOS questionnaire and the isometric muscle strength test in patients with severe knee osteoarthritis undergoing total knee replacement. Man. Ther. 2016, 21, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Medina-Mirapeix, F.; Vivo-Fernández, I.; López-Cañizares, J.; García-Vidal, J.A.; Benítez-Martínez, J.C.; Del Baño-Aledo, M.E. Five times sit-to-stand test in subjects with total knee replacement: Reliability and relationship with functional mobility tests. Gait Posture 2018, 59, 258–260. [Google Scholar] [CrossRef] [PubMed]



| Author | Year of Publication | Country | Journal § | Sample Size | Number of Centers, Study Design | Primary Outcome | PEDro Score˥ |
|---|---|---|---|---|---|---|---|
| Winters et al. [34] | 2014 | USA | Knee | nE = 35, nC = 23 | 1, CCT | Quadriceps and hamstrings isometric strength assessment | 4 |
| Smith et al. [35] | 2014 | USA | J Arthroplasty | nE = 13, nC = 11 | 1, CCT | Quadriceps muscle strength by isokinetic dynamometer | 5 |
| Bade et al. [36] | 2014 | USA | Am J Phys Med Rehabil | nE = 34, nC = 30 | 1, RCT | Knee ROM | 5 |
| Abdel et al. [37] | 2014 | USA | Clin Orthop Relat Res | nE = 20, nC = 20 | 1, RCT | KSS, KOOS, SF-12 | 7 |
| Jenkins et al. [38] | 2014 | USA | J Bone Joint Surg Am | nE = 60, nC = 60 | 1, RCT | Quadriceps isometric strength assessment | 7 |
| Thomas et al. [39] | 2014 | USA | Knee | nE = 10, nC = 10 | 1, CCT | Quadriceps and hamstrings isometric strength assessment | 5 |
| Huber et al. [40] | 2015 | Switzerland | BMC Musculoskelet Disord | nE = 22, nC = 23 | 1, RCT | CST | 7 |
| Calatayud et al. [41] | 2017 | Spain | Knee Surg Sports Traumatol Arthrosc | nE = 25, nC = 25 | 1, RCT | WOMAC | 7 |
| Bistolfi et al. [42] | 2017 | Italy | Knee Surgery Sports Traummatol Arthrosc | nE = 23, nC = 44 | 1, CCT | HDRS | 4 |
| Hadlandsmyth et al. [43] | 2017 | USA | Psychol Health Med | nE = 173, nC = 173 | 1, RCT | NRS pain | 4 |
| Cooper et al. [44] | 2017 | USA | J Orthop Res | nE = 62, nC = 62 | 1, CCT | KOOS, gait velocity and physical activity level using accelerometry | 5 |
| Bonnefoy-Mazure et al. [45] | 2017 | Switzerland | J Arthroplasty | nE = 79, nC = 32 | 1, CCT | Gait velocity and knee ROM | 5 |
| Loyd et al. [46] | 2017 | USA | Phys. Ther | nE = 84, nC = 78 | 4, RCT | Strength testing by isokinetic dynamometer | 7 |
| Lin et al. [47] | 2018 | Taiwan | J. Clin. Nurs | nE = 100, nC = 100 | 1, RCT | KOOS | 7 |
| Husby et al. [48] | 2018 | Norway | Eur J Phys Rehabil Med | nE = 21, nC = 20 | 1, RCT | Quadriceps and hamstring muscle strength | 6 |
| Paravlic et al. [49] | 2019 | Slovenia | PLoS ONE | nE = 17, nC = 17 | 1, RCT | Quadriceps and hamstring muscle strength | 7 |
| Indelli et al. [50] | 2019 | USA | Knee Surg Sports Traumatol Arthrosc | nE = 50, nC = 50 | 1, RCT | ROM, KSS, OKS | 6 |
| Jiang et al. [51] | 2019 | China | Orthop Surg | nE = 109, nC = 147 | 1, CCT | NRS pain, KSS, ROM | 5 |
| Liljensøe et al. [52] | 2019 | Denmark | Scand J. Surg | nE = 38, nC = 38 | 1, RCT | SF-36 | 7 |
| Skoffer et al. [53] | 2019 | Danmark | Clin Rehabil | nE = 30, nC = 29 | 1, CCT | 5STS test | 8 |
| Abbreviation | Full Name | Used as Primary or Secondary Outcomes | Number of Times Used |
|---|---|---|---|
| Questionnaires | |||
| KOOS | Knee injury and Osteoarthritis Outcomes Score | Primary | 6 |
| WOMAC | Western Ontario and McMaster Universities Osteoarthritis index | Primary | 2 |
| KSS | New Knee Society Score | Primary | 4 |
| OKS | Oxford Knee Score | Primary | 1 |
| HSS | Hospital for Special Surgery | Secondary | 1 |
| HDRS | Hamilton Depression Rating Scale | Primary and secondary | 1 |
| STAI | State-Trait Anxiety Index | Secondary | 2 |
| GDS | Geriatric Depression Scale | Secondary | 2 |
| HADS | Hospital Anxiety and Depression Scale | Secondary | 1 |
| SF-36 | MOS Short Form 36 | Primary and secondary | 6 |
| SF-12 | MOS Short Form 12 | Secondary | 2 |
| PCS | Pain Catastrophizing Score | Secondary | 2 |
| NRS pain | Pain intensity by Numeric Rating Scale | Primary and secondary | 8 |
| Physical tests | |||
| Knee ROM | Knee Range Of Motion | Primary and secondary | 8 |
| ASLR | Active Straight Leg Raise | Secondary | 1 |
| Strength | Strength testing of knee flexor/extensor by isometric or isokinetic dynamometer | Primary and secondary | 8 |
| EMG | Quadriceps/hamstrings co-activation and on/off timing using electromyography | Secondary | 1 |
| PPT | Pressure Pain Threshold | Secondary | 1 |
| Gait velocity | Gait Velocity (self-paced) | Primary and secondary | 4 |
| 10MWT | Maximum walking speed/10-m walk test (fast-paced) | Secondary | 1 |
| 6MWT | Six-Minute Walk test | Secondary | 4 |
| Actimetry | Physical activity level with average steps/day using accelerometry | Primary and secondary | 2 |
| 5STS test | Five Times Sit-To-Stand Test | Primary and secondary | 4 |
| TUG | Timed Up and Go Test | Primary and secondary | 6 |
| SCT | Stair Climbing Time | Secondary | 2 |
| Tool (References) | Target Population # | Domains ˥ | No. of Scales ˩ | No. of Items | No. of Response Options | Range of Scores | Time to Administer (min) | Mode of Administration | Cultural/Adaptation ǂ | Copyright |
|---|---|---|---|---|---|---|---|---|---|---|
| Condition-specific | ||||||||||
| KOOS [54,55,56,57,58] | Knee OA | Pain, other disease-specific symptoms, ADL function, sport and recreation, function, knee related QoL | 5 | 42 | 5 | P: 0–36 Sy: 0–28 A: 0–68 SP: 0–16 Q: 0–16 | 10 | Self-administered | Many languages | No |
| WOMAC [54,59,60,61,62,63] | Knee OA | Pain, physical function, stiffness | 3 | 24 | 5 | P: 0–20 S: 0–8 PF: 0–68 | 5-10 | Self-administered | Many languages | No |
| KSS [64,65] | Knee OA | Pain, expectation, satisfaction, physical function | 4 | 34 | Varies | O: 0–100 Sa: 0–40 Ex: 0–15 F: 0–100 | 15 | Interview based and examination | English French German Chinese Portuguese Dutch Turkish | Yes |
| OKS [66,67,68,69] | Knee OA | Pain and physical function | 1 | 12 | 5 | 12–60 | 10 | Self-administered | Many languages | Yes |
| HSS [70,71] | TKA | Expectation | 1 | 19 | 5 | 0-100 | 5-10 | Self-administered | English French | No |
| Patient-specific | ||||||||||
| HDRS | Depressed patients | Depression | 1 | 17 | Varies | 0–53 | 20–30 | Interview based | Many languages | Yes |
| STAI [72] | General population | Anxiety | 2 | 40 | 4 | S-A: 20–80 T-A: 20–80 | 10 | Self-administered | Many languages | Yes |
| GDS [73] | Elderly | Depression | 1 | 30 | 2 | 0–30 | 5–10 | Self-administered | Many languages | No |
| HADS [72,73,74,75,76] | General population | Anxiety and depression | 2 | 14 | 4 | A: 0–21 D: 0–21 | 5–10 | Self-administered | Many languages | Yes |
| Generic | ||||||||||
| SF-36 [23,24,61,62,77,78,79] | General population | Pain, physical/mental/social function, general health | 8 | 36 | Varies | 0–100 PCS: 0–100 MCS: 0–100 | 10 | Self-administered | Many languages | No |
| SF-12 [24,62,78,80,81] | General population | Pain, physical/mental/social function, general health | 2 | 12 | Varies | 0–100 PCS: 0–100 MCS: 0–100 | 5 | Self-administered | Many languages | No |
| PCS [82] | General population | Pain catastrophizing | 1 | 13 | 5 | 0–52 R: 0–16 M: 0–12 H: 0–24 | 5 | Self-administered | English French | Yes |
| NRS pain [83] | General population | Pain severity | 1 | 1 | 11 | 0–10 | 1 | Self-administered | No translation needed | No |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reynaud, V.; Verdilos, A.; Pereira, B.; Boisgard, S.; Costes, F.; Coudeyre, E. Core Outcome Measurement Instruments for Clinical Trials of Total Knee Arthroplasty: A Systematic Review. J. Clin. Med. 2020, 9, 2439. https://doi.org/10.3390/jcm9082439
Reynaud V, Verdilos A, Pereira B, Boisgard S, Costes F, Coudeyre E. Core Outcome Measurement Instruments for Clinical Trials of Total Knee Arthroplasty: A Systematic Review. Journal of Clinical Medicine. 2020; 9(8):2439. https://doi.org/10.3390/jcm9082439
Chicago/Turabian StyleReynaud, Vivien, Anargyros Verdilos, Bruno Pereira, Stéphane Boisgard, Frédéric Costes, and Emmanuel Coudeyre. 2020. "Core Outcome Measurement Instruments for Clinical Trials of Total Knee Arthroplasty: A Systematic Review" Journal of Clinical Medicine 9, no. 8: 2439. https://doi.org/10.3390/jcm9082439