Clinical Management of Diabetes Mellitus in the Era of COVID-19: Practical Issues, Peculiarities and Concerns

 , and
, and
Abstract
:1. Introduction
2. Literature Search Strategy and Selection Criteria
3. The Association between DM and COVID-19
3.1. Causality
3.2. Clinical Course of SARS-CoV2 Infection in Patients with DM
3.3. Mechanisms for the Increased Risk and Severity Associated with COVID-19 in DM
3.4. Role of Glycemic Control for COVID-19 Outcomes
- (i)
- Both hyperglycemia and hypoglycemia may disrupt an already malfunctioning innate immune system in patients with DM, increasing their susceptibility to infections [70]. Studies in poorly controlled subjects with T2DM have shown attenuated increases in plasma levels of cytokines and adhesion molecules after the administration of endotoxin in vivo [79]. These defects can be partly restored after adequate glycemic control, highlighting the importance of optimal glucose management for the maintenance of appropriate immune function in DM during infections [80].
- (ii)
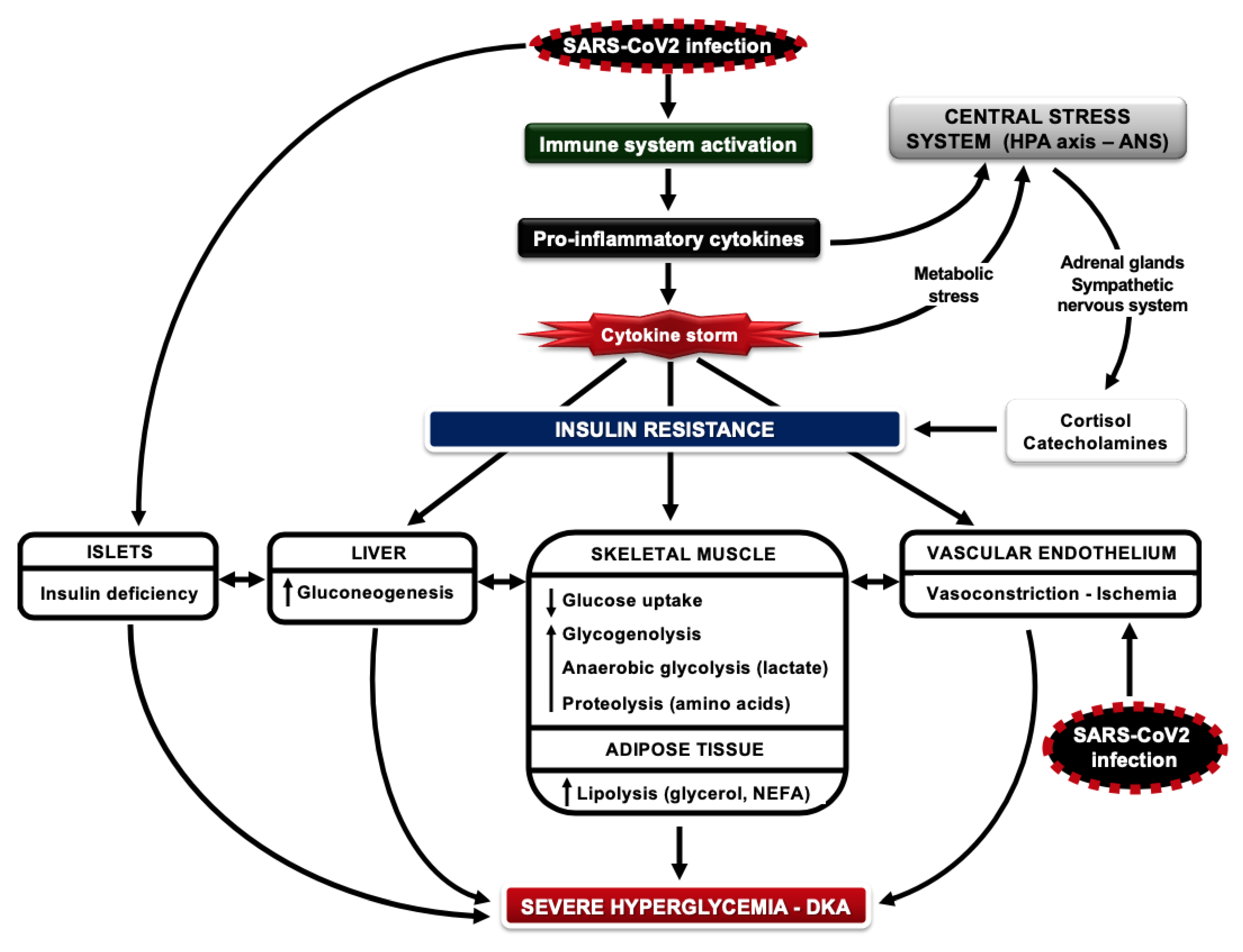
- T2DM is an inflammatory disease characterized by the increased production of proinflammatory cytokines from adipose tissue/endothelial cells and insulin resistance in the liver/muscle/adipose tissue, along with inadequate β-cell function; by the time of clinical diagnosis, at least 50% of β-cell mass has been lost due to progressive destruction by oxidative stress, generated from the elevated levels of glucose and NEFAs in the circulation (glucotoxicity and lipotoxicity) [81]. In type 1 DM (T1DM), although it results from the primary loss of β-cell mass due to autoimmune processes with consecutive insulin deficiency, residual β-cell function may be retained in some individuals for years after clinical diagnosis; it should be noted that insulin resistance and an inflammatory state are also features of this type of DM [82,83,84]. In the presence of insulin resistance, poor glycemic control reflects relative insulin insufficiency for the corresponding metabolic needs; insulin resistance and the shortage of insulin may promote a catabolic state. In the course of COVID-19 infection, insulin requirements increase dramatically due to the “cytokine storm” and high insulin resistance [27]. Considering the fact that SARS-CoV2 may also directly attack the islets, severe insulin deficiency aggravates the catabolic state, generating massive increases in circulating glucose and NEFAs; these will lead to severe ketoacidosis or a hyperglycemic hyperosmolar state and multi-organ failure [27,85] (Figure 1).
- (iii)
- Hyperglycemia can be toxic for cells that take up glucose passively and independently of insulin, such as those of the central/peripheral nervous system, hepatocytes, endothelial/epithelial cells and pancreatic β-cells. Glucose overload increases oxidative stress, advanced glycation end-product formation and apoptosis, leading to cellular damage and severe clinical complications during critical illness. Glucose toxicity has been linked to the development of liver/kidney dysfunction, neuropathy, endothelial damage, susceptibility to bacterial infections and respiratory tract dysfunction [86]. Regarding COVID-19, an important issue to consider is the glucose overload of airway surface epithelial cells. Low glucose concentrations in the airway surface are an important part of normal lung defense against infections; high concentrations of glucose in airway epithelial cells could therefore predispose to bacterial growth and pulmonary infections [87]. Protection from neuropathy during critical illness also has important clinical implications, such as a shorter duration of mechanical ventilation and ICU hospitalization [86]. In a study in surgical ICU patients with and without DM, intensive glycemic control with insulin (targeting blood glucose levels between 4.4–6.1 mmol/L) reduced hospital-acquired infections and lethal sepsis, neuropathy, acute renal failure, blood transfusions and the risk of multiple organ failure and death versus conventional insulin treatment (blood glucose levels 10–11.1 mmol/L); these beneficial effects were attributed to the decrease in hyperglycemia and not to insulin use [88]. Similar results were reported in medical ICU patients with DM, including those with respiratory infections and septic shock, under intensive or conventional glycemic control with insulin: the lowest mortality occurred among patients with blood glucose levels between 3.9–5.5 mmol/L and increased consistently with blood glucose levels above this range, with the highest mortality at blood glucose levels ≥ 10 mmol/L [89]. Although these studies provided convincing evidence to support the significance of good glycemic control during critical illness, they both reported frequent hypoglycemic episodes in the group assigned to intensive glucose management. The question of which is the safest range of blood glucose levels for “benefit without harm” was finally answered by the NICE-SUGAR trial in medical ICU patients on intensive (blood glucose levels 4.5–6 mmol/L) vs. conventional glycemic control (blood glucose levels 8–10 mmol/L) by intravenous insulin: mortality in the latter group was actually lower than in the former group; the reason was more frequent episodes of moderate or severe hypoglycemia in the intensive treatment group, which was associated strongly with the risk of death [90]. Therefore, a target range of moderate hyperglycemia between 8–10 mmol/L is both effective and safe to reduce glucose toxicity, hypoglycemia risk and mortality during critical illness.
- (iv)
- Severe hyperglycemia may promote osmotic effects on cells, fluid shifts and electrolyte disturbances which, along with the diarrhea that occasionally accompanies COVID-19 infection, can lead to severe dehydration, decreases in tissue blood flow and ischemia, severe defects in cellular metabolism and ketosis [86,88]. It should be noted that in T2DM, endothelial dysfunction and impaired insulin-stimulated blood flow in major tissues, like adipose tissue and skeletal muscle, are already present early during the course of the disease and long before clinical diagnosis, playing a significant role in the pathophysiology of metabolic dysregulation [91,92]. Endothelial dysfunction is further aggravated in people with DM because SARS-CoV2 infection induces endotheliitis in several organs as a direct consequence of viral involvement and of the host inflammatory response [54].
- (v)
- Hypoglycemia (blood glucose levels < 3.9 mmol/L) is the most frequent acute complication of DM and the main obstacle to achieving optimal glycemic control; it is associated mostly with the use of insulin and sulfonylureas [93]. In patients with T1DM, hypoglycemia is very common and unpredictable; it can be severe when associated with unawareness of the preliminary warning symptoms, predisposing patients to life-threatening complications [94]. In addition to weakening the body’s defensive mechanisms to infections by depriving white blood cells and the brain of their main fuel [70,72], hypoglycemia can also impair autonomic function, cause vasoconstriction and ischemia, prolong the QT interval, predisposing to fatal cardiac arrhythmias especially at night during sleep, and has been associated with fatal outcomes in critically ill patients [95].
4. General Recommendations for the Prevention of COVID-19 in Patients with DM
5. General Recommendations for the Management of Hyperglycemia in Patients with DM and COVID-19
5.1. Special Considerations for T1DM
5.2. Special Considerations for T2DM
5.2.1. Glycemic Goals
5.2.2. Glucose Monitoring
5.2.3. Pharmacological Treatment
5.2.4. Impact of COVID-19 Treatment on Glucose Metabolism
6. Knowledge Gaps and Questions to Be Answered
- Are patients with DM more susceptible than the general population to contracting SARS-CoV2, or is their susceptibility mainly limited to the increased severity of infection?
- Is the association of DM with adverse COVID-19 outcomes independent of coexisting risk factors such as advanced age and cardiovascular and kidney disease?
- Which antidiabetic drugs, if any, could interfere with COVID-19 prognosis, by either positively or negatively modulating clinical outcomes?
- Are SGLT2 inhibitors adequately safe for DM patients with COVID-19? Are they associated with better survival and cardiovascular and renal protection?
- What are the optimal glycemic targets for optimizing outcomes in patients with mild and severe forms of COVID-19?
- What are the exact clinical and biochemical characteristics of patients with T2DM (age, obesity, glycemic control, T2DM-related complications, insulin resistance, subclinical inflammation) which may serve as prognostic markers and determine poor prognosis in COVID-19?
- Based on their pathophysiological milieu, are patients with DM expected to gain particular benefits from specific antiviral therapeutic approaches (immunomodulatory, cytokine-targeted or other)?
- What is the immune response of people with DM infected with SARS-CoV2? Do they develop protective antibodies against the virus?
- Will the vaccines under development be equally safe and effective in DM patients as in the general population?
7. Concluding Remarks
Author Contributions
Funding
Conflicts of Interest
References
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19–11 March 2020. 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 19 May 2020).
- Coronavirus Disease (COVID-19). Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200518-covid-19-sitrep-119.pdf?sfvrsn=4bd9de25_4 (accessed on 19 May 2020).
- Hussain, A.; Bhowmik, B.; do Vale Moreira, N.C. COVID-19 and Diabetes: Knowledge in Progress. Diabetes Res. Clin. Pr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Holmes, L., Jr.; Enwere, M.; Williams, J.; Ogundele, B.; Chavan, P.; Piccoli, T.; Chinacherem, C.; Comeaux, C.; Pelaez, L.; Okundaye, O.; et al. Black-White Risk Differentials in COVID-19 (SARS-COV2) Transmission, Mortality and Case Fatality in the United States: Translational Epidemiologic Perspective and Challenges. Int. J. Environ. Res. Public Health 2020, 17, 4322. [Google Scholar] [CrossRef]
- Alsan, M.; Stantcheva, S.; Yang, D.; Cutler, D. Disparities in Coronavirus 2019 Reported Incidence, Knowledge, and Behavior Among US Adults. JAMA Netw. Open 2020, 3, e2012403. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, L.; Ogunwole, S.M.; Cooper, L.A. Historical Insights on Coronavirus Disease 2019 (COVID-19), the 1918 Influenza Pandemic, and Racial Disparities: Illuminating a Path Forward. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Price-Haywood, E.G.; Burton, J.; Fort, D.; Seoane, L. Hospitalization and Mortality among Black Patients and White Patients with Covid-19. N. Engl. J. Med. 2020, 382, 2534–2543. [Google Scholar] [CrossRef] [PubMed]
- Gold, J.A.W.; Szablewski, C.M.; Wong, K.K.; Patel, P.R.; Rossow, J.; Silva, J.d.; Natarajan, P.; Morris, S.B.; Fanfair, R.N.; Bruce, B.B.; et al. Characteristics and Clinical Outcomes of Adult Patients Hospitalized with COVID-19-Georgia, March 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 545–550. [Google Scholar] [CrossRef]
- West, C.P.; Montori, V.M.; Sampathkumar, P. COVID-19 Testing: The Threat of False-Negative Results. Mayo Clin. Proc. 2020, 95, 1127–1129. [Google Scholar] [CrossRef]
- Watson, J.; Whiting, P.F.; Brush, J.E. Interpreting a covid-19 test result. BMJ 2020, 369, m1808. [Google Scholar] [CrossRef]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020. [Google Scholar] [CrossRef]
- Wolfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Muller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [Green Version]
- False-Negative Results of Initial RT-PCR Assays for COVID-19: A Systematic Review. Available online: https://www.medrxiv.org/content/10.1101/2020.04.16.20066787v1 (accessed on 11 July 2020).
- Arulkumaran, N.; Brealey, D.; Howell, D.; Singer, M. Use of non-invasive ventilation for patients with COVID-19: A cause for concern? Lancet Respir. Med. 2020, 8, e45. [Google Scholar] [CrossRef]
- WHO—World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-Ncov) Infection Is Suspected: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/330893 (accessed on 11 July 2020).
- Arentz, M.; Yim, E.; Klaff, L.; Lokhandwala, S.; Riedo, F.X.; Chong, M.; Lee, M. Characteristics and Outcomes of 21 Critically Ill Patients With COVID-19 in Washington State. JAMA 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in coronavirus disease 2019 patients: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Northwell, C.-R.C.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020. [Google Scholar] [CrossRef]
- Bode, B.; Garrett, V.; Messler, J.; McFarland, R.; Crowe, J.; Booth, R.; Klonoff, D.C. Glycemic Characteristics and Clinical Outcomes of COVID-19 Patients Hospitalized in the United States. J. Diabetes Sci. Technol. 2020. [Google Scholar] [CrossRef]
- Bornstein, S.R.; Dalan, R.; Hopkins, D.; Mingrone, G.; Boehm, B.O. Endocrine and metabolic link to coronavirus infection. Nat. Rev. Endocrinol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Bindom, S.M.; Lazartigues, E. The sweeter side of ACE2: Physiological evidence for a role in diabetes. Mol. Cell Endocrinol. 2009, 302, 193–202. [Google Scholar] [CrossRef]
- Liu, F.; Long, X.; Zhang, B.; Zhang, W.; Chen, X.; Zhang, Z. ACE2 Expression in Pancreas May Cause Pancreatic Damage After SARS-CoV-2 Infection. Clin. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef]
- Ma, R.C.W.; Holt, R.I.G. COVID-19 and diabetes. Diabet. Med. 2020, 37, 723–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Bornstein, S.R.; Rubino, F.; Khunti, K.; Mingrone, G.; Hopkins, D.; Birkenfeld, A.L.; Boehm, B.; Amiel, S.; Holt, R.I.; Skyler, J.S.; et al. Practical recommendations for the management of diabetes in patients with COVID-19. Lancet Diabetes Endocrinol. 2020, 8, 546–550. [Google Scholar] [CrossRef]
- Angelidi, A.M.; Belanger, M.J.; Mantzoros, C.S. COVID-19 and diabetes mellitus: What we know, how our patients should be treated now, and what should happen next. Metabolism 2020, 154245. [Google Scholar] [CrossRef] [PubMed]
- Katulanda, P.; Dissanayake, H.A.; Ranathunga, I.; Ratnasamy, V.; Wijewickrama, P.S.A.; Yogendranathan, N.; Gamage, K.K.K.; de Silva, N.L.; Sumanatilleke, M.; Somasundaram, N.P.; et al. Prevention and management of COVID-19 among patients with diabetes: An appraisal of the literature. Diabetologia 2020, 1–13. [Google Scholar] [CrossRef]
- Kar, P.; Jones, K.L.; Horowitz, M.; Deane, A.M. Management of critically ill patients with type 2 diabetes: The need for personalised therapy. World J. Diabetes 2015, 6, 693–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maddaloni, E.; Buzzetti, R. Covid-19 and diabetes mellitus: Unveiling the interaction of two pandemics. Diabetes Metab. Res. Rev. 2020, e33213321. [Google Scholar] [CrossRef]
- Fadini, G.P.; Morieri, M.L.; Longato, E.; Avogaro, A. Prevalence and impact of diabetes among people infected with SARS-CoV-2. J. Endocrinol. Investig. 2020. [Google Scholar] [CrossRef] [Green Version]
- CDC. Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions among Patients with Coronavirus Disease 2019 in United States, 12 February–28 March, 2020. CDC COVID-19 Response Team. 2020. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/mm6913e2htm (accessed on 11 July 2020).
- Menke, A.; Casagrande, S.; Geiss, L.; Cowie, C.C. Prevalence of and Trends in Diabetes Among Adults in the United States, 1988–2012. JAMA 2015, 314, 1021–1029. [Google Scholar] [CrossRef] [Green Version]
- Marik, P.E.; Bellomo, R. Stress hyperglycemia: An essential survival response! Crit. Care 2013, 17, 305. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.K.; Feng, Y.; Yuan, M.Y.; Yuan, S.Y.; Fu, H.J.; Wu, B.Y.; Sun, G.Z.; Yang, G.R.; Zhang, X.L.; Wang, L.; et al. Plasma glucose levels and diabetes are independent predictors for mortality and morbidity in patients with SARS. Diabet. Med. 2006, 23, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.K.; Lin, S.S.; Ji, X.J.; Guo, L.M. Binding of SARS coronavirus to its receptor damages islets and causes acute diabetes. Acta Diabetol. 2010, 47, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Letko, M.; Marzi, A.; Munster, V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roca-Ho, H.; Riera, M.; Palau, V.; Pascual, J.; Soler, M.J. Characterization of ACE and ACE2 Expression within Different Organs of the NOD Mouse. Int. J. Mol. Sci. 2017, 18, 563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caso, F.; Costa, L.; Ruscitti, P.; Navarini, L.; Del Puente, A.; Giacomelli, R.; Scarpa, R. Could Sars-coronavirus-2 trigger autoimmune and/or autoinflammatory mechanisms in genetically predisposed subjects? Autoimmun. Rev. 2020, 19, 102524. [Google Scholar] [CrossRef]
- Abu-Ashour, W.; Twells, L.; Valcour, J.; Randell, A.; Donnan, J.; Howse, P.; Gamble, J.M. The association between diabetes mellitus and incident infections: A systematic review and meta-analysis of observational studies. BMJ Open Diabetes Res. Care 2017, 5, e000336. [Google Scholar] [CrossRef]
- Kornum, J.B.; Thomsen, R.W.; Riis, A.; Lervang, H.H.; Schonheyder, H.C.; Sorensen, H.T. Type 2 diabetes and pneumonia outcomes: A population-based cohort study. Diabetes Care 2007, 30, 2251–2257. [Google Scholar] [CrossRef] [Green Version]
- Garbati, M.A.; Fagbo, S.F.; Fang, V.J.; Skakni, L.; Joseph, M.; Wani, T.A.; Cowling, B.J.; Peiris, M.; Hakawi, A. A Comparative Study of Clinical Presentation and Risk Factors for Adverse Outcome in Patients Hospitalised with Acute Respiratory Disease Due to MERS Coronavirus or Other Causes. PLoS ONE 2016, 11, e0165978. [Google Scholar] [CrossRef] [Green Version]
- Allard, R.; Leclerc, P.; Tremblay, C.; Tannenbaum, T.N. Diabetes and the severity of pandemic influenza A (H1N1) infection. Diabetes Care 2010, 33, 1491–1493. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020. [Google Scholar] [CrossRef]
- Chen, Y.; Gong, X.; Wang, L.; Guo, J. Effects of hypertension, diabetes and coronary heart disease on COVID-19 diseases severity: A systematic review and meta-analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Huang, I.; Lim, M.A.; Pranata, R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia—A systematic review, meta-analysis, and meta-regression. Diabetes Metab. Syndr. 2020, 14, 395–403. [Google Scholar] [CrossRef]
- Cariou, B.; Hadiadi, S.; Wargny, M.; Pichelin, M.; AlSalameh, A.; Allix, I.; Amadou, C.; Arnault, G.; Baudoux, F.; Bauduceau, B.; et al. Phenotypic characteristics and prognosis of inpatients with COVID-19 and diabetes: The CORONADO study. Diabetologia 2020, 63, 1500–1515. [Google Scholar] [CrossRef] [PubMed]
- Shi, Q.; Zhang, X.; Jiang, F.; Zhang, X.; Hu, N.; Bimu, C.; Feng, J.; Yan, S.; Guan, Y.; Xu, D.; et al. Clinical Characteristics and Risk Factors for Mortality of COVID-19 Patients With Diabetes in Wuhan, China: A Two-Center, Retrospective Study. Diabetes Care 2020, 43, 1382–1391. [Google Scholar] [CrossRef] [PubMed]
- Mehra, M.R.; Desai, S.S.; Kuy, S.; Henry, T.D.; Patel, A.N. Cardiovascular Disease, Drug Therapy, and Mortality in Covid-19. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Dryden, M.; Baguneid, M.; Eckmann, C.; Corman, S.; Stephens, J.; Solem, C.; Li, J.; Charbonneau, C.; Baillon-Plot, N.; Haider, S. Pathophysiology and burden of infection in patients with diabetes mellitus and peripheral vascular disease: Focus on skin and soft-tissue infections. Clin. Microbiol. Infect. 2015, 21, S27–S32. [Google Scholar] [CrossRef] [Green Version]
- Pearson-Stuttard, J.; Blundell, S.; Harris, T.; Cook, D.G.; Critchley, J. Diabetes and infection: Assessing the association with glycaemic control in population-based studies. Lancet Diabetes Endocrinol. 2016, 4, 148–158. [Google Scholar] [CrossRef]
- Gan, Y.H. Host susceptibility factors to bacterial infections in type 2 diabetes. PLoS Pathog. 2013, 9, e1003794. [Google Scholar] [CrossRef]
- Jafar, N.; Edriss, H.; Nugent, K. The Effect of Short-Term Hyperglycemia on the Innate Immune System. Am. J. Med. Sci. 2016, 351, 201–211. [Google Scholar] [CrossRef]
- Kolahian, S.; Leiss, V.; Nurnberg, B. Diabetic lung disease: Fact or fiction? Rev. Endocr. Metab. Disord. 2019, 20, 303–319. [Google Scholar] [CrossRef]
- Delamaire, M.; Maugendre, D.; Moreno, M.; Le Goff, M.C.; Allannic, H.; Genetet, B. Impaired leucocyte functions in diabetic patients. Diabet Med. 1997, 14, 29–34. [Google Scholar] [CrossRef]
- Hypertension and Diabetes Delay the Viral Clearance in COVID-19 Patients. Available online: https://www.medrxiv.org/content/10.1101/2020.03.22.20040774v1 (accessed on 11 July 2020).
- Fernandez-Real, J.M.; Valdes, S.; Manco, M.; Chico, B.; Botas, P.; Campo, A.; Casamitjana, R.; Delgado, E.; Salvador, J.; Fruhbeck, G.; et al. Surfactant protein d, a marker of lung innate immunity, is positively associated with insulin sensitivity. Diabetes Care 2010, 33, 847–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, E.H.; Baines, D.L. Airway Glucose Homeostasis: A New Target in the Prevention and Treatment of Pulmonary Infection. Chest 2018, 153, 507–514. [Google Scholar] [CrossRef]
- Imai, Y.; Kuba, K.; Rao, S.; Huan, Y.; Guo, F.; Guan, B.; Yang, P.; Sarao, R.; Wada, T.; Leong-Poi, H.; et al. Angiotensin-converting enzyme 2 protects from severe acute lung failure. Nature 2005, 436, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Lau, A.; So, H.C. Exploring diseases/traits and blood proteins causally related to expression of ACE2, the putative receptor of SARS-CoV-2: A Mendelian Randomization analysis highlights tentative relevance of diabetes-related traits. Diabetes Care 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.03.04.20031237v2.full.pdf (accessed on 11 July 2020). [CrossRef] [PubMed]
- Pal, R.; Bhadada, S.K. Should anti-diabetic medications be reconsidered amid COVID-19 pandemic? Diabetes Res. Clin. Pr. 2020, 163, 108146. [Google Scholar] [CrossRef]
- Danser, A.H.J.; Epstein, M.; Batlle, D. Renin-Angiotensin System Blockers and the COVID-19 Pandemic: At Present There Is No Evidence to Abandon Renin-Angiotensin System Blockers. Hypertension 2020. [Google Scholar] [CrossRef] [Green Version]
- Bloomgarden, Z.T. Inflammation and insulin resistance. Diabetes Care 2003, 26, 1619–1623. [Google Scholar] [CrossRef] [Green Version]
- Lemkes, B.A.; Hermanides, J.; Devries, J.H.; Holleman, F.; Meijers, J.C.; Hoekstra, J.B. Hyperglycemia: A prothrombotic factor? J. Thromb. Haemost. 2010, 8, 1663–1669. [Google Scholar] [CrossRef]
- Tentolouris, A.; Eleftheriadou, I.; Tzeravini, E.; Tsilingiris, D.; Paschou, S.A.; Siasos, G.; Tentolouris, N. Endothelium as a Therapeutic Target in Diabetes Mellitus: From Basic Mechanisms to Clinical Practice. Curr. Med. Chem. 2020, 27, 1089–1131. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am. J. Hematol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muniyappa, R.; Gubbi, S. COVID-19 Pandemic, Corona Viruses, and Diabetes Mellitus. Am. J. Physiol. Endocrinol. Metab. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calder, P.C. Fuel utilization by cells of the immune system. Proc. Nutr. Soc. 1995, 54, 65–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calder, P.C.; Dimitriadis, G.; Newsholme, P. Glucose metabolism in lymphoid and inflammatory cells and tissues. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 531–540. [Google Scholar] [CrossRef]
- Dungan, K.M.; Braithwaite, S.S.; Preiser, J.C. Stress hyperglycaemia. Lancet 2009, 373, 1798–1807. [Google Scholar] [CrossRef]
- Maratou, E.; Dimitriadis, G.; Kollias, A.; Boutati, E.; Lambadiari, V.; Mitrou, P.; Raptis, S.A. Glucose transporter expression on the plasma membrane of resting and activated white blood cells. Eur. J. Clin. Investig. 2007, 37, 282–290. [Google Scholar] [CrossRef]
- Hill, M.A.; Mantzoros, C.; Sowers, J.R. Commentary: COVID-19 in patients with diabetes. Metabolism 2020, 107, 154217. [Google Scholar] [CrossRef]
- MacIntyre, E.J.; Majumdar, S.R.; Gamble, J.M.; Minhas-Sandhu, J.K.; Marrie, T.J.; Eurich, D.T. Stress hyperglycemia and newly diagnosed diabetes in 2124 patients hospitalized with pneumonia. Am. J. Med. 2012, 125, 1036.e17–1036.e23. [Google Scholar] [CrossRef]
- Zhu, L.; She, Z.G.; Cheng, X.; Qin, J.J.; Zhang, X.J.; Cai, J.; Lei, F.; Wang, H.; Xie, J.; Wang, W.; et al. Association of Blood Glucose Control and Outcomes in Patients with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metab. 2020. [Google Scholar] [CrossRef]
- Newsholme, E.A.; Dimitriadis, G. Integration of biochemical and physiologic effects of insulin on the control of blood glucose concentrations. Exp. Clin. Endocrinol. Diabetes 2001, 109, S122–S134. [Google Scholar] [CrossRef]
- Inzucchi, S.E. Clinical practice. Management of hyperglycemia in the hospital setting. N. Engl. J. Med. 2006, 355, 1903–1911. [Google Scholar] [CrossRef] [PubMed]
- Inzucchi, S.E.; Siegel, M.D. Glucose control in the ICU--how tight is too tight? N. Engl. J. Med. 2009, 360, 1346–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreasen, A.S.; Pedersen-Skovsgaard, T.; Berg, R.M.; Svendsen, K.D.; Feldt-Rasmussen, B.; Pedersen, B.K.; Moller, K. Type 2 diabetes mellitus is associated with impaired cytokine response and adhesion molecule expression in human endotoxemia. Intensive Care Med. 2010, 36, 1548–1555. [Google Scholar] [CrossRef] [PubMed]
- Kousathana, F.; Georgitsi, M.; Lambadiari, V.; Giamarellos-Bourboulis, E.J.; Dimitriadis, G.; Mouktaroudi, M. Defective production of interleukin-1 beta in patients with type 2 diabetes mellitus: Restoration by proper glycemic control. Cytokine 2017, 90, 177–184. [Google Scholar] [CrossRef]
- Ceriello, A.; Motz, E. Is oxidative stress the pathogenic mechanism underlying insulin resistance, diabetes, and cardiovascular disease? The common soil hypothesis revisited. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 816–823. [Google Scholar] [CrossRef] [Green Version]
- Kaul, K.; Apostolopoulou, M.; Roden, M. Insulin resistance in type 1 diabetes mellitus. Metabolism 2015, 64, 1629–1639. [Google Scholar] [CrossRef]
- Alnek, K.; Kisand, K.; Heilman, K.; Peet, A.; Varik, K.; Uibo, R. Increased Blood Levels of Growth Factors, Proinflammatory Cytokines, and Th17 Cytokines in Patients with Newly Diagnosed Type 1 Diabetes. PLoS ONE 2015, 10, e0142976. [Google Scholar] [CrossRef]
- Yu, M.G.; Keenan, H.A.; Shah, H.S.; Frodsham, S.G.; Pober, D.; He, Z.; Wolfson, E.A.; D’Eon, S.; Tinsley, L.J.; Bonner-Weir, S.; et al. Residual beta cell function and monogenic variants in long-duration type 1 diabetes patients. J. Clin. Investig. 2019, 129, 3252–3263. [Google Scholar] [CrossRef] [Green Version]
- Dimitriadis, G.; Mitrou, P.; Lambadiari, V.; Maratou, E.; Raptis, S.A. Insulin effects in muscle and adipose tissue. Diabetes Res. Clin. Pr. 2011, 93, S52–S59. [Google Scholar] [CrossRef]
- Van den Berghe, G. How does blood glucose control with insulin save lives in intensive care? J. Clin. Investig. 2004, 114, 1187–1195. [Google Scholar] [CrossRef] [Green Version]
- Philips, B.J.; Meguer, J.X.; Redman, J.; Baker, E.H. Factors determining the appearance of glucose in upper and lower respiratory tract secretions. Intensive Care Med. 2003, 29, 2204–2210. [Google Scholar] [CrossRef]
- Van den Berghe, G.; Wouters, P.; Weekers, F.; Verwaest, C.; Bruyninckx, F.; Schetz, M.; Vlasselaers, D.; Ferdinande, P.; Lauwers, P.; Bouillon, R. Intensive insulin therapy in critically ill patients. N. Engl. J. Med. 2001, 345, 1359–1367. [Google Scholar] [CrossRef]
- Krinsley, J.S. Glycemic control, diabetic status, and mortality in a heterogeneous population of critically ill patients before and during the era of intensive glycemic management: Six and one-half years experience at a university-affiliated community hospital. Semin. Thorac. Cardiovasc. Surg. 2006, 18, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Investigators, N.-S.S.; Finfer, S.; Chittock, D.R.; Su, S.Y.; Blair, D.; Foster, D.; Dhingra, V.; Bellomo, R.; Cook, D.; Dodek, P.; et al. Intensive versus conventional glucose control in critically ill patients. N. Engl. J. Med. 2009, 360, 1283–1297. [Google Scholar] [CrossRef] [Green Version]
- Dimitriadis, G.; Lambadiari, V.; Mitrou, P.; Maratou, E.; Boutati, E.; Panagiotakos, D.B.; Economopoulos, T.; Raptis, S.A. Impaired postprandial blood flow in adipose tissue may be an early marker of insulin resistance in type 2 diabetes. Diabetes Care 2007, 30, 3128–3130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambadiari, V.; Mitrou, P.; Maratou, E.; Raptis, A.; Raptis, S.A.; Dimitriadis, G. Increases in muscle blood flow after a mixed meal are impaired at all stages of type 2 diabetes. Clin. Endocrinol. (Oxf.) 2012, 76, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Liatis, S.; Mylona, M.; Kalopita, S.; Papazafiropoulou, A.; Karamagkiolis, S.; Melidonis, A.; Xilomenos, A.; Ioannidis, I.; Kaltsas, G.; Lanaras, L.; et al. Hypoglycaemia requiring medical assistance in patients with diabetes: A prospective multicentre survey in tertiary hospitals. Diabetes Metab. 2015, 41, 126–131. [Google Scholar] [CrossRef]
- Khunti, K.; Davies, M.; Majeed, A.; Thorsted, B.L.; Wolden, M.L.; Paul, S.K. Hypoglycemia and risk of cardiovascular disease and all-cause mortality in insulin-treated people with type 1 and type 2 diabetes: A cohort study. Diabetes Care 2015, 38, 316–322. [Google Scholar] [CrossRef] [Green Version]
- Wernly, B.; Jirak, P.; Lichtenauer, M.; Franz, M.; Kabisch, B.; Schulze, P.C.; Braun, K.; Muessig, J.; Masyuk, M.; Paulweber, B.; et al. Hypoglycemia but Not Hyperglycemia Is Associated with Mortality in Critically Ill Patients with Diabetes. Med. Princ. Pr. 2019, 28, 186–192. [Google Scholar] [CrossRef]
- Sardu, C.; D’Onofrio, N.; Balestrieri, M.L.; Barbieri, M.; Rizzo, M.R.; Messina, V.; Maggi, P.; Coppola, N.; Paolisso, G.; Marfella, R. Outcomes in Patients With Hyperglycemia Affected by Covid-19: Can We Do More on Glycemic Control? Diabetes Care 2020. [Google Scholar] [CrossRef]
- Wang, A.; Zhao, W.; Xu, Z.; Gu, J. Timely blood glucose management for the outbreak of 2019 novel coronavirus disease (COVID-19) is urgently needed. Diabetes Res. Clin. Pr. 2020, 162, 108118. [Google Scholar] [CrossRef]
- International Society of, P.; Adolescent, D. Summary of recommendations regarding COVID-19 in children with diabetes: Keep Calm and Mind your Diabetes Care and Public Health Advice. Pediatr. Diabetes 2020, 21, 413–414. [Google Scholar] [CrossRef]
- Ebekozien, O.A.; Noor, N.; Gallagher, M.P.; Alonso, G.T. Type 1 Diabetes and COVID-19: Preliminary Findings From a Multicenter Surveillance Study in the U.S. Diabetes Care 2020. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Lu, J.; Gu, W.; Zhang, Y.; Liu, J.; Ning, G. Care for diabetes with COVID-19: Advice from China. J. Diabetes 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uijtendaal, E.V.; Zwart-van Rijkom, J.E.; de Lange, D.W.; Lalmohamed, A.; van Solinge, W.W.; Egberts, T.C. Influence of a strict glucose protocol on serum potassium and glucose concentrations and their association with mortality in intensive care patients. Crit. Care 2015, 19, 270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentile, S.; Strollo, F.; Ceriello, A. The Need for Diabetes Care Customization in the ICU at the Time of SARS-CoV-2 Outbreak. Diabetes 2020, 1–3. [Google Scholar] [CrossRef]
- Krinsley, J.S.; Preiser, J.C. Time in blood glucose range 70 to 140 mg/dl >80% is strongly associated with increased survival in non-diabetic critically ill adults. Crit. Care 2015, 19, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceriello, A.; Monnier, L.; Owens, D. Glycaemic variability in diabetes: Clinical and therapeutic implications. Lancet Diabetes Endocrinol. 2019, 7, 221–230. [Google Scholar] [CrossRef] [Green Version]
- Chao, W.C.; Tseng, C.H.; Wu, C.L.; Shih, S.J.; Yi, C.Y.; Chan, M.C. Higher glycemic variability within the first day of ICU admission is associated with increased 30-day mortality in ICU patients with sepsis. Ann. Intensive Care 2020, 10, 17. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, A.; Prince, L.R.; Novodvorsky, P.; Bernjak, A.; Thomas, M.R.; Birch, L.; Lambert, D.; Kay, L.J.; Wright, F.J.; Macdonald, I.A.; et al. Effect of Hypoglycemia on Inflammatory Responses and the Response to Low-Dose Endotoxemia in Humans. J. Clin. Endocrinol. Metab. 2019, 104, 1187–1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sapp, J.L.; Alqarawi, W.; MacIntyre, C.J.; Tadros, R.; Steinberg, C.; Roberts, J.D.; Laksman, Z.; Healey, J.S.; Krahn, A.D. Guidance on Minimizing Risk of Drug-Induced Ventricular Arrhythmia During Treatment of COVID-19: A Statement from the Canadian Heart Rhythm Society. Can. J. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Spallone, V.; Ziegler, D.; Freeman, R.; Bernardi, L.; Frontoni, S.; Pop-Busui, R.; Stevens, M.; Kempler, P.; Hilsted, J.; Tesfaye, S.; et al. Cardiovascular autonomic neuropathy in diabetes: Clinical impact, assessment, diagnosis, and management. Diabetes Metab. Res. Rev. 2011, 27, 639–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tentolouris, A.; Vlachakis, P.; Tzeravini, E.; Eleftheriadou, I.; Tentolouris, N. SGLT2 Inhibitors: A Review of Their Antidiabetic and Cardioprotective Effects. Int. J. Environ. Res. Public Health 2019, 16, 2965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- Fitchett, D.; Zinman, B.; Wanner, C.; Lachin, J.M.; Hantel, S.; Salsali, A.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Inzucchi, S.E.; et al. Heart failure outcomes with empagliflozin in patients with type 2 diabetes at high cardiovascular risk: Results of the EMPA-REG OUTCOME(R) trial. Eur. Heart J. 2016, 37, 1526–1534. [Google Scholar] [CrossRef] [Green Version]
- Kosiborod, M.; Lam, C.S.P.; Kohsaka, S.; Kim, D.J.; Karasik, A.; Shaw, J.; Tangri, N.; Goh, S.Y.; Thuresson, M.; Chen, H.; et al. Cardiovascular Events Associated With SGLT-2 Inhibitors Versus Other Glucose-Lowering Drugs: The CVD-REAL 2 Study. J. Am. Coll. Cardiol. 2018, 71, 2628–2639. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [Green Version]
- Barchetta, I.; Ciccarelli, G.; Barone, E.; Cimini, F.A.; Ceccarelli, V.; Bertoccini, L.; Sentinelli, F.; Tramutola, A.; Del Ben, M.; Angelico, F.; et al. Greater circulating DPP4 activity is associated with impaired flow-mediated dilatation in adults with type 2 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1087–1094. [Google Scholar] [CrossRef]
- Zheng, T.; Gao, Y.; Baskota, A.; Chen, T.; Ran, X.; Tian, H. Increased plasma DPP4 activity is predictive of prediabetes and type 2 diabetes onset in Chinese over a four-year period: Result from the China National Diabetes and Metabolic Disorders Study. J. Clin. Endocrinol. Metab. 2014, 99, E2330–E2334. [Google Scholar] [CrossRef] [Green Version]
- Iacobellis, G. COVID-19 and diabetes: Can DPP4 inhibition play a role? Diabetes Res. Clin. Pr. 2020, 162, 108125. [Google Scholar] [CrossRef]
- Raj, V.S.; Mou, H.; Smits, S.L.; Dekkers, D.H.; Muller, M.A.; Dijkman, R.; Muth, D.; Demmers, J.A.; Zaki, A.; Fouchier, R.A.; et al. Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC. Nature 2013, 495, 251–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohnuma, K.; Takahashi, N.; Yamochi, T.; Hosono, O.; Dang, N.H.; Morimoto, C. Role of CD26/dipeptidyl peptidase IV in human T cell activation and function. Front. Biosci. 2008, 13, 2299–2310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barchetta, I.; Gisella Cavallo, M.; Giorgio Baroni, M. COVID-19 and diabetes: Is this association driven by the DPP4 receptor? Potential clinical and therapeutic implications. Diabetes Res. Clin. Pr. 2020, 108165. [Google Scholar] [CrossRef] [PubMed]
- Kokic Males, V. Letter to the Editor in response to the article “COVID-19 and diabetes: Can DPP4 inhibition play a role?”. Diabetes Res. Clin. Pr. 2020, 108163. [Google Scholar] [CrossRef] [PubMed]
- Pitocco, D.; Tartaglione, L.; Viti, L.; Di Leo, M.; Pontecorvi, A.; Caputo, S. SARS-CoV-2 and DPP4 inhibition: Is it time to pray for Janus Bifrons? Diabetes Res. Clin. Pr. 2020, 108162. [Google Scholar] [CrossRef]
- Li, K.; Wohlford-Lenane, C.L.; Channappanavar, R.; Park, J.E.; Earnest, J.T.; Bair, T.B.; Bates, A.M.; Brogden, K.A.; Flaherty, H.A.; Gallagher, T.; et al. Mouse-adapted MERS coronavirus causes lethal lung disease in human DPP4 knockin mice. Proc. Natl. Acad. Sci. USA 2017, 114, E3119–E3128. [Google Scholar] [CrossRef] [Green Version]
- Fan, C.; Wu, X.; Liu, Q.; Li, Q.; Liu, S.; Lu, J.; Yang, Y.; Cao, Y.; Huang, W.; Liang, C.; et al. A Human DPP4-Knockin Mouse’s Susceptibility to Infection by Authentic and Pseudotyped MERS-CoV. Viruses 2018, 10, 448. [Google Scholar] [CrossRef] [Green Version]
- Qi, F.; Qian, S.; Zhang, S.; Zhang, Z. Single cell RNA sequencing of 13 human tissues identify cell types and receptors of human coronaviruses. Biochem. Biophys. Res. Commun. 2020, 526, 135–140. [Google Scholar] [CrossRef]
- Willemen, M.J.; Mantel-Teeuwisse, A.K.; Straus, S.M.; Meyboom, R.H.; Egberts, T.C.; Leufkens, H.G. Use of dipeptidyl peptidase-4 inhibitors and the reporting of infections: A disproportionality analysis in the World Health Organization VigiBase. Diabetes Care 2011, 34, 369–374. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Cai, X.; Han, X.; Ji, L. DPP-4 inhibitors and risk of infections: A meta-analysis of randomized controlled trials. Diabetes Metab. Res. Rev. 2016, 32, 391–404. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, M.; Nikolic, D.; Patti, A.M.; Mannina, C.; Montalto, G.; McAdams, B.S.; Rizvi, A.A.; Cosentino, F. GLP-1 receptor agonists and reduction of cardiometabolic risk: Potential underlying mechanisms. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 2814–2821. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Yuan, G.; Cheng, F.; Zhang, J.; Guo, X. Mast Cell and M1 Macrophage Infiltration and Local Pro-Inflammatory Factors Were Attenuated with Incretin-Based Therapies in Obesity-Related Glomerulopathy. Metab. Syndr. Relat. Disord. 2017, 15, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Koliaki, C.; Katsilambros, N. Important Considerations for the Treatment of Patients with Diabetes Mellitus and Heart Failure from a Diabetologist’s Perspective: Lessons Learned from Cardiovascular Outcome Trials. Int. J. Environ. Res. Public Health 2019, 17, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloomgarden, Z. Glycemic control and the heart: It matters how you get there. J. Diabetes 2016, 8, 453–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceriello, A. Thiazolidinediones as anti-inflammatory and anti-atherogenic agents. Diabetes Metab. Res. Rev. 2008, 24, 14–26. [Google Scholar] [CrossRef]
- Penlioglou, T.; Papachristou, S.; Papanas, N. COVID-19 and Diabetes Mellitus: May Old Anti-diabetic Agents Become the New Philosopher’s Stone? Diabetes 2020, 1–3. [Google Scholar] [CrossRef]
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med. 2020, 8, e21. [Google Scholar] [CrossRef]
- Soler, M.J.; Ye, M.; Wysocki, J.; William, J.; Lloveras, J.; Batlle, D. Localization of ACE2 in the renal vasculature: Amplification by angiotensin II type 1 receptor blockade using telmisartan. Am. J. Physiol. Ren. Physiol. 2009, 296, F398–F405. [Google Scholar] [CrossRef] [Green Version]
- Ferrario, C.M.; Jessup, J.; Chappell, M.C.; Averill, D.B.; Brosnihan, K.B.; Tallant, E.A.; Diz, D.I.; Gallagher, P.E. Effect of angiotensin-converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin-converting enzyme 2. Circulation 2005, 111, 2605–2610. [Google Scholar] [CrossRef] [Green Version]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor Recognition by the Novel Coronavirus from Wuhan: An Analysis Based on Decade-Long Structural Studies of SARS Coronavirus. J. Virol. 2020, 94. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Ye, Y.; Gong, H.; Wu, J.; Yuan, J.; Wang, S.; Yin, P.; Ding, Z.; Kang, L.; Jiang, Q.; et al. The effects of different angiotensin II type 1 receptor blockers on the regulation of the ACE-AngII-AT1 and ACE2-Ang(1–7)-Mas axes in pressure overload-induced cardiac remodeling in male mice. J. Mol. Cell Cardiol. 2016, 97, 180–190. [Google Scholar] [CrossRef]
- Henry, C.; Zaizafoun, M.; Stock, E.; Ghamande, S.; Arroliga, A.C.; White, H.D. Impact of angiotensin-converting enzyme inhibitors and statins on viral pneumonia. In Baylor University Medical Center Proceedings; Taylor & Francis: Abingdon, UK, 2018; Volume 31, pp. 419–423. [Google Scholar] [CrossRef]
- American College of Cardiology. HFSA/ACC/AHA Statement Addresses Concerns re: Using RAAS Antagonists in COVID-19. Available online: https://www.acc.org/latest-in-cardiology/articles/2020/03/17/08/59/hfsa-acc-aha-statement-addresses-concerns-re-using-raas-antagonists-in-covid-19 (accessed on 17 March 2020).
- European Society of Cardiology. Position Statement of the ESC Council on Hypertension on ACE-Inhibitors and Angiotensin Receptor Blockers. Available online: https://www.escardio.org/Councils/Council-on-Hypertension-(CHT)/News/position-statement-of-the-esc-council-on-hypertension-on-ace-inhibitors-and-ang (accessed on 13 March 2020).
- Day, M. Covid-19: Ibuprofen should not be used for managing symptoms, say doctors and scientists. BMJ 2020, 368, m1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinott, E.; Kozer, E.; Shapira, Y.; Bar-Haim, A.; Youngster, I. Ibuprofen use and clinical outcomes in COVID-19 patients. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sodhi, M.; Etminan, M. Safety of Ibuprofen in Patients With COVID-19: Causal or Confounded? Chest 2020. [Google Scholar] [CrossRef] [PubMed]
- CBC. Available online: https://www.cbc.ca/news/health/ibuprofen-covid-19-novel-coronavirus-1.5501496 (accessed on 11 July 2020).
- Alhazzani, W.; Moller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolilekas, L.; Loverdos, K.; Giannakaki, S.; Vlassi, L.; Levounets, A.; Zervas, E.; Gaga, M. Can steroids reverse the severe COVID-19 induced “cytokine storm”? J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fadel, R.; Morrison, A.R.; Vahia, A.; Smith, Z.R.; Chaudhry, Z.; Bhargava, P.; Miller, J.; Kenney, R.M.; Alangaden, G.; Ramesh, M.S.; et al. Early Short Course Corticosteroids in Hospitalized Patients with COVID-19. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- So, C.; Ro, S.; Murakami, M.; Imai, R.; Jinta, T. High-dose, short-term corticosteroids for ARDS caused by COVID-19: A case series. Respirol. Case Rep. 2020, 8, e00596. [Google Scholar] [CrossRef]
- Yuan, M.; Xu, X.; Xia, D.; Tao, Z.; Yin, W.; Tan, W.; Hu, Y.; Song, C. Effects of Corticosteroid Treatment for Non-Severe COVID-19 Pneumonia: A Propensity Score-Based Analysis. Shock 2020. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Liu, J.; Zhou, Y.; Zhao, X.; Zhao, Q.; Liu, J. The effect of corticosteroid treatment on patients with coronavirus infection: A systematic review and meta-analysis. J. Infect. 2020, 81, e13–e20. [Google Scholar] [CrossRef] [PubMed]
- Randomised Evaluation of COVID-19 Therapy (RECOVERY). Low-Cost Dexamethasone Reduces Death by up to One Third in Hospitalised Patients with Severe Respiratory Complications of COVID-19. 2020. Available online: https://www.recoverytrial.net/news/low-cost-dexamethasone-reduces-death-by-up-to-one-third-in-hospitalised-patients-with-severe-respiratory-complications-of-covid-19 (accessed on 9 July 2020).
- National Institutes of Health. COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 9 July 2020).
- Clore, J.N.; Thurby-Hay, L. Glucocorticoid-induced hyperglycemia. Endocr. Pr. 2009, 15, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, G.; Leighton, B.; Parry-Billings, M.; Sasson, S.; Young, M.; Krause, U.; Bevan, S.; Piva, T.; Wegener, G.; Newsholme, E.A. Effects of glucocorticoid excess on the sensitivity of glucose transport and metabolism to insulin in rat skeletal muscle. Biochem. J. 1997, 321, 707–712. [Google Scholar] [CrossRef] [Green Version]
- Weir, E.K.; Thenappan, T.; Bhargava, M.; Chen, Y. Does vitamin D deficiency increase the severity of COVID-19? Clin. Med. (Lond.) 2020. [Google Scholar] [CrossRef]
- Jakovac, H. COVID-19 and vitamin D-Is there a link and an opportunity for intervention? Am. J. Physiol. Endocrinol. Metab. 2020, 318, E589. [Google Scholar] [CrossRef]
- Teymoori-Rad, M.; Shokri, F.; Salimi, V.; Marashi, S.M. The interplay between vitamin D and viral infections. Rev. Med. Virol. 2019, 29, e2032. [Google Scholar] [CrossRef]
- Xu, J.; Yang, J.; Chen, J.; Luo, Q.; Zhang, Q.; Zhang, H. Vitamin D alleviates lipopolysaccharideinduced acute lung injury via regulation of the reninangiotensin system. Mol. Med. Rep. 2017, 16, 7432–7438. [Google Scholar] [CrossRef] [Green Version]
- Ali, N. Role of vitamin D in preventing of COVID-19 infection, progression and severity. J. Infect. Public Health 2020. [Google Scholar] [CrossRef]
- Facchiano, A.; Facchiano, A.; Bartoli, M.; Ricci, A.; Facchiano, F. Reply to Jakovac: About COVID-19 and vitamin D. Am. J. Physiol. Endocrinol. Metab. 2020, 318, E838. [Google Scholar] [CrossRef]
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K.; et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab. Res. Rev. 2020, e3319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, B.; Gutierrez, B.; Mekaru, S.; Sewalk, K.; Goodwin, L.; Loskill, A.; Cohn, E.L.; Hswen, Y.; Hill, S.C.; Cobo, M.M.; et al. Epidemiological data from the COVID-19 outbreak, real-time case information. Sci. Data 2020, 7, 106. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Diabetes Pharmacotherapy | Clinical Recommendation | Special Considerations in the Setting of COVID-19 |
|---|---|---|
| Insulin |
|
|
| Metformin |
|
|
| Sulfonylureas |
|
|
| Sodium glucose co-transporter 2 (SGLT2) inhibitors (dapagliflozin, canagliflozin, empagliflozin) |
|
|
| Dipeptidyl peptidase 4 (DPP-4) inhibitors (alogliptin, vildagliptin, sitagliptin, saxagliptin, linagliptin) |
|
|
| Glucagon-like peptide 1 receptor (GLP-1R) agonists (liraglutide, dulaglutide, semaglutide, exenatide-extended release, lixisenatide, albiglutide) |
|
|
| Thiazolidinediones (pioglitazone) |
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koliaki, C.; Tentolouris, A.; Eleftheriadou, I.; Melidonis, A.; Dimitriadis, G.; Tentolouris, N. Clinical Management of Diabetes Mellitus in the Era of COVID-19: Practical Issues, Peculiarities and Concerns. J. Clin. Med. 2020, 9, 2288. https://doi.org/10.3390/jcm9072288
Koliaki C, Tentolouris A, Eleftheriadou I, Melidonis A, Dimitriadis G, Tentolouris N. Clinical Management of Diabetes Mellitus in the Era of COVID-19: Practical Issues, Peculiarities and Concerns. Journal of Clinical Medicine. 2020; 9(7):2288. https://doi.org/10.3390/jcm9072288
Chicago/Turabian StyleKoliaki, Chrysi, Anastasios Tentolouris, Ioanna Eleftheriadou, Andreas Melidonis, George Dimitriadis, and Nikolaos Tentolouris. 2020. "Clinical Management of Diabetes Mellitus in the Era of COVID-19: Practical Issues, Peculiarities and Concerns" Journal of Clinical Medicine 9, no. 7: 2288. https://doi.org/10.3390/jcm9072288