Role of Cardiac Computed Tomography for Etiology Evaluation of Newly Diagnosed Heart Failure with Reduced Ejection Fraction

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
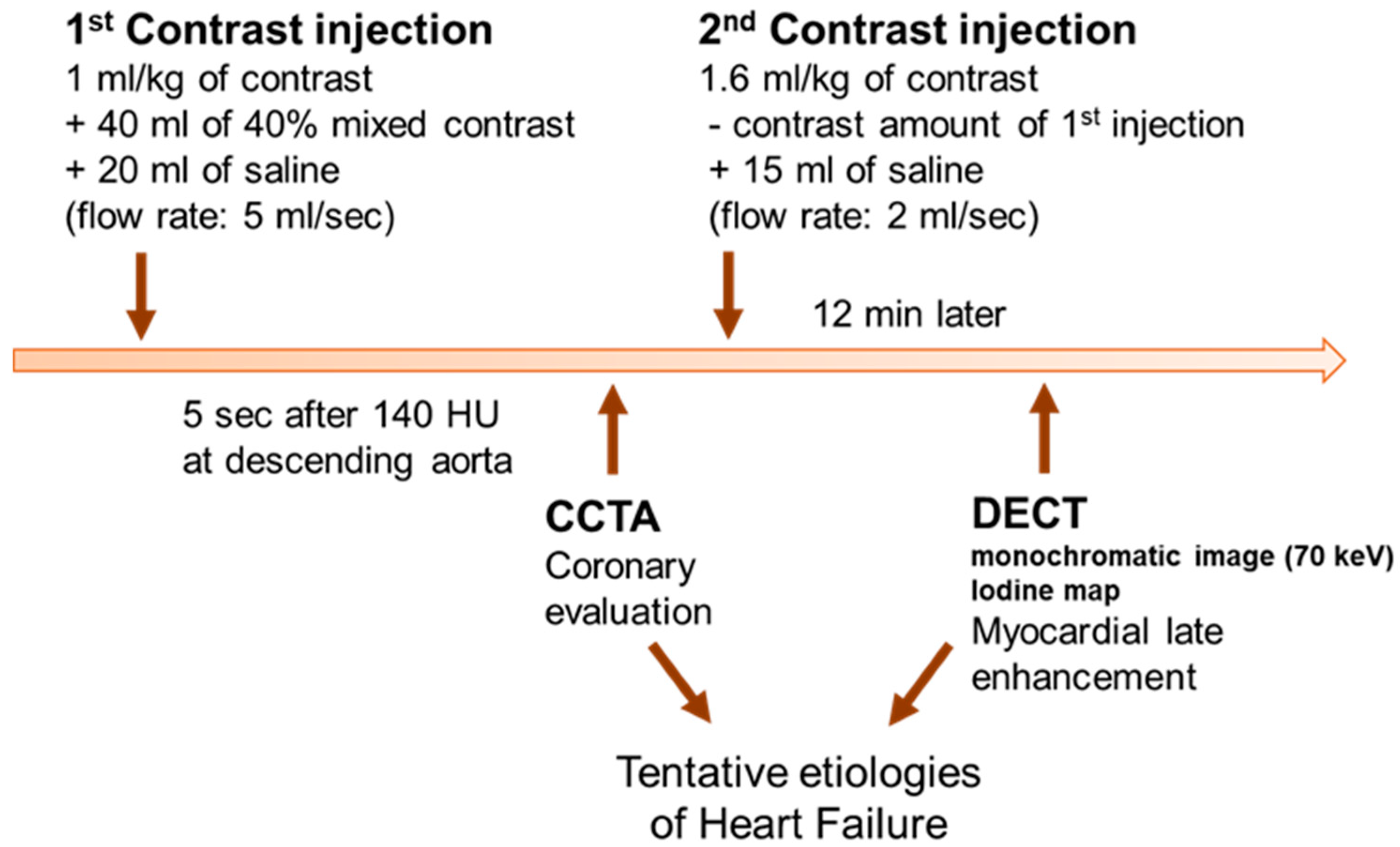
2.2. Cardiac CT
2.3. Image Analysis
2.4. Clinical Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Safety of Combined CT
3.3. Cardiac CT Findings
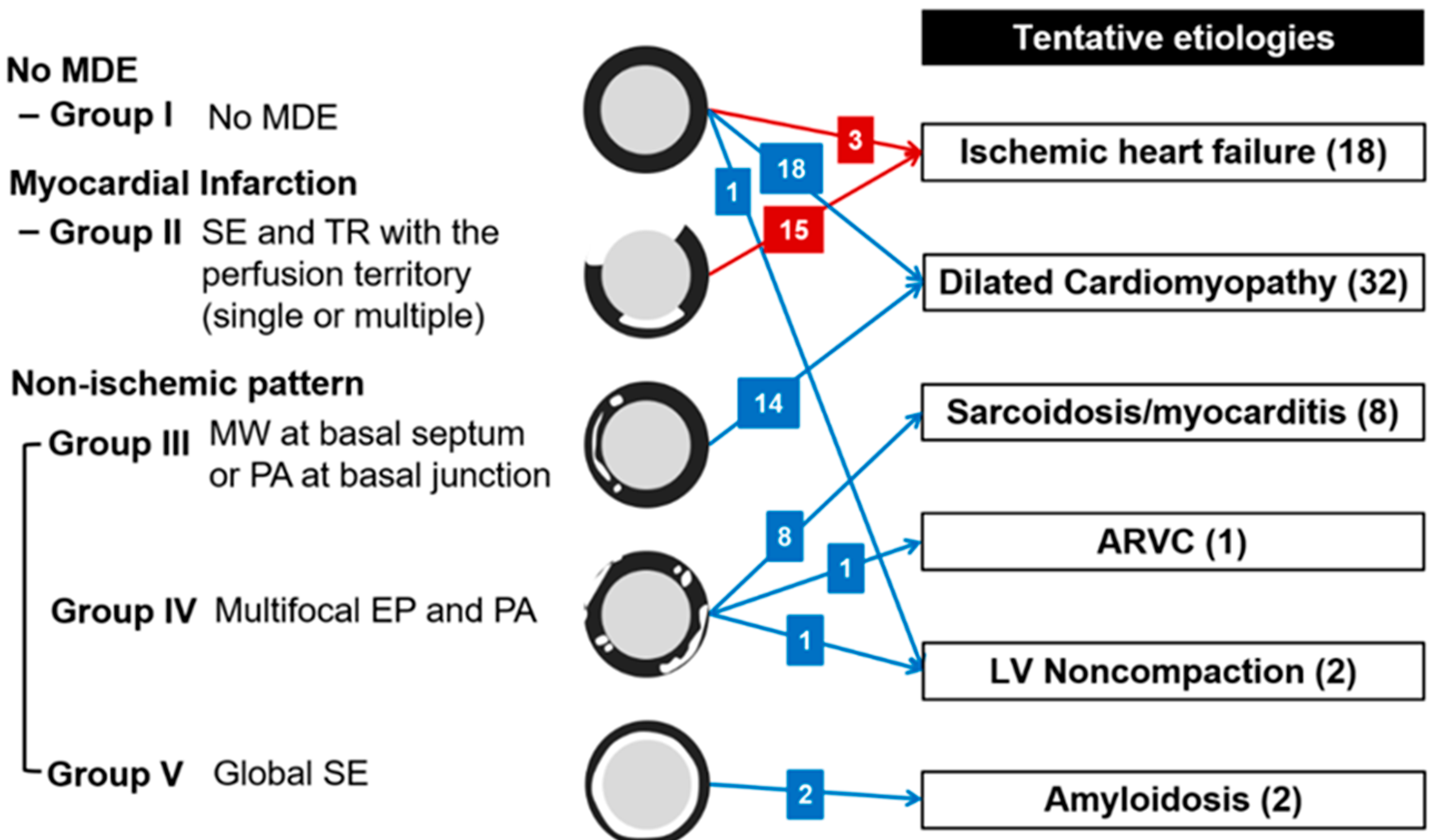
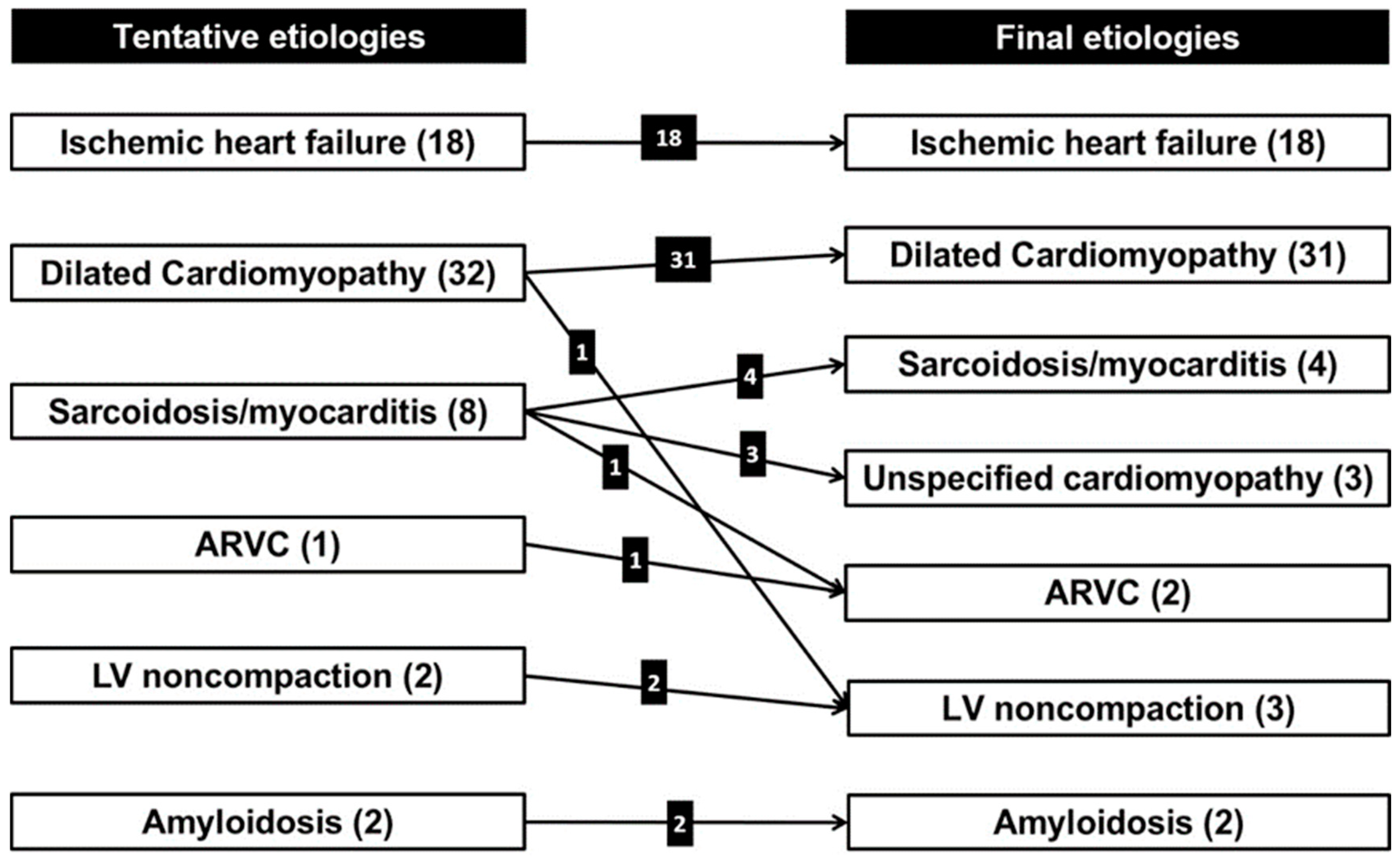
3.4. Tentative Etiologies of HF from Cardiac CT
3.5. Final Etiologies of HF from Clinical Decisions and Concordance Between Tentative and Final Etiologies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the european society of cardiology (ESC)developed with the special contribution of the heart failure association (HFA) of the esc. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Youn, J.C.; Han, S.; Ryu, K.H. Temporal trends of hospitalized patients with heart failure in Korea. Korean Circ. J. 2017, 47, 16–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, H.M.; Park, M.S.; Youn, J.C. Update on heart failure management and future directions. Korean J. Intern. Med. 2019, 34, 11–43. [Google Scholar] [CrossRef] [PubMed]
- Stewart Coats, A.J. Common co-morbidities in heart failure–diabetes, functional mitral regurgitation and sleep apnoea. Int. J. Heart Fail. 2019, 1, 25–41. [Google Scholar] [CrossRef]
- Karamitsos, T.D.; Francis, J.M.; Myerson, S.; Selvanayagam, J.B.; Neubauer, S. The role of cardiovascular magnetic resonance imaging in heart failure. J. Am. Coll. Cardiol. 2009, 54, 1407–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.J.; Cho, H.J.; Kim, M.S.; Kang, J.; Kim, K.H.; Kim, D.; Seo, S.M.; Yang, J.H.; Cha, M.J.; Choi, J.I.; et al. Focused update of 2016 Korean society of heart failure guidelines for the management of chronic heart failure. Int. J. Heart Fail. 2019, 1, 4–24. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, M.S.; Yoo, B.S.; Park, S.J.; Park, J.J.; Shin, M.S.; Youn, J.C.; Lee, S.E.; Jang, S.Y.; Choi, S.; et al. KSHF guidelines for the management of acute heart failure: Part II. Treatment of acute heart failure. Korean Circ. J. 2019, 49, 22–45. [Google Scholar] [CrossRef]
- Lee, H.Y.; Oh, B.H. Paradigm shifts of heart failure therapy: Do we need another paradigm? Int. J. Heart Fail. 2020, 2. [Google Scholar] [CrossRef]
- Miller, J.M.; Rochitte, C.E.; Dewey, M.; Arbab-Zadeh, A.; Niinuma, H.; Gottlieb, I.; Paul, N.; Clouse, M.E.; Shapiro, E.P.; Hoe, J.; et al. Diagnostic performance of coronary angiography by 64-row CT. N. Engl. J. Med. 2008, 359, 2324–2336. [Google Scholar] [CrossRef] [Green Version]
- Gheorghiade, M.; Bonow, R.O. Chronic heart failure in the United States: A manifestation of coronary artery disease. Circulation 1998, 97, 282–289. [Google Scholar] [CrossRef]
- Patel, M.R.; White, R.D.; Abbara, S.; Bluemke, D.A.; Herfkens, R.J.; Picard, M.; Shaw, L.J.; Silver, M.; Stillman, A.E.; Udelson, J.; et al. 2013 ACCF/ACR/ASE/ASNC/SCCT/SCMR appropriate utilization of cardiovascular imaging in heart failure: A joint report of the American College of Radiology Appropriateness Criteria Committee and the American College of Cardiology Foundation appropriate use criteria task force. J. Am. Coll. Cardiol. 2013, 61, 2207–2231. [Google Scholar]
- Gerber, B.L.; Belge, B.; Legros, G.J.; Lim, P.; Poncelet, A.; Pasquet, A.; Gisellu, G.; Coche, E.; Vanoverschelde, J.L. Characterization of acute and chronic myocardial infarcts by multidetector computed tomography: Comparison with contrast-enhanced magnetic resonance. Circulation 2006, 113, 823–833. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Ma, X.; Delano, M.C.; Jiang, T.; Zhang, C.; Liu, Y.; Zhang, Z. Assessment of myocardial fibrosis and coronary arteries in hypertrophic cardiomyopathy using combined arterial and delayed enhanced CT: Comparison with MR and coronary angiography. Eur. Radiol. 2013, 23, 1034–1043. [Google Scholar] [CrossRef]
- Lee, H.J.; Im, D.J.; Youn, J.C.; Chang, S.; Suh, Y.J.; Hong, Y.J.; Kim, Y.J.; Hur, J.; Choi, B.W. Assessment of myocardial delayed enhancement with cardiac computed tomography in cardiomyopathies: A prospective comparison with delayed enhancement cardiac magnetic resonance imaging. Int. J. Cardiovasc. Imaging 2017, 33, 577–584. [Google Scholar] [CrossRef]
- Mendoza, D.D.; Weigold, W.G. Evaluation of myocardial viability by multidetector CT. J. Cardiovasc. Comput. Tomogr. 2009, 3, S2–S12. [Google Scholar] [CrossRef]
- Wichmann, J.L.; Arbaciauskaite, R.; Kerl, J.M.; Frellesen, C.; Bodelle, B.; Lehnert, T.; Monsefi, N.; Vogl, T.J.; Bauer, R.W. Evaluation of monoenergetic late iodine enhancement dual-energy computed tomography for imaging of chronic myocardial infarction. Eur. Radiol. 2014, 24, 1211–1218. [Google Scholar] [CrossRef]
- Chang, S.; Han, K.; Youn, J.C.; Im, D.J.; Kim, J.Y.; Suh, Y.J.; Hong, Y.J.; Hur, J.; Kim, Y.J.; Choi, B.W.; et al. Utility of dual-energy CT-based monochromatic imaging in the assessment of myocardial delayed enhancement in patients with cardiomyopathy. Radiology 2018, 287, 442–451. [Google Scholar] [CrossRef]
- Ohta, Y.; Kitao, S.; Yunaga, H.; Fujii, S.; Mukai, N.; Yamamoto, K.; Ogawa, T. Myocardial delayed enhancement CT for the evaluation of heart failure: Comparison to MRI. Radiology 2018, 288, 682–691. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.J.; Kim, R.J. The role of cardiac MR in new-onset heart failure. Curr. Cardiol. Rep. 2011, 13, 185–193. [Google Scholar] [CrossRef]
- Nacif, M.S.; Kawel, N.; Lee, J.J.; Chen, X.; Yao, J.; Zavodni, A.; Sibley, C.T.; Lima, J.A.; Liu, S.; Bluemke, D.A.; et al. Interstitial myocardial fibrosis assessed as extracellular volume fraction with low-radiation-dose cardiac CT. Radiology 2012, 264, 876–883. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation 2013, 128, 240–327. [Google Scholar] [CrossRef] [PubMed]
- Cury, R.C.; Abbara, S.; Achenbach, S.; Agatston, A.; Berman, D.S.; Budoff, M.J.; Dill, K.E.; Jacobs, J.E.; Maroules, C.D.; Rubin, G.D.; et al. Cad-rads(tm) coronary artery disease-reporting and data system. An expert consensus document of the society of cardiovascular computed tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. J. Cardiovasc. Comput. Tomogr. 2016, 10, 269–281. [Google Scholar]
- Cummings, K.W.; Bhalla, S.; Javidan-Nejad, C.; Bierhals, A.J.; Gutierrez, F.R.; Woodard, P.K. A pattern-based approach to assessment of delayed enhancement in nonischemic cardiomyopathy at MR imaging. Radiographics 2009, 29, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Shaw, L.K.; O’Connor, C.M. A standardized definition of ischemic cardiomyopathy for use in clinical research. J. Am. Coll. Cardiol. 2002, 39, 210–218. [Google Scholar] [CrossRef] [Green Version]
- Mahrholdt, H.; Wagner, A.; Judd, R.M.; Sechtem, U.; Kim, R.J. Delayed enhancement cardiovascular magnetic resonance assessment of non-ischaemic cardiomyopathies. Eur. Heart J. 2005, 26, 1461–1474. [Google Scholar] [CrossRef]
- Ahn, S.S.; Kim, Y.J.; Hur, J.; Lee, H.J.; Kim, T.H.; Choe, K.O.; Choi, B.W. CT detection of subendocardial fat in myocardial infarction. AJR Am. J. Roentgenol. 2009, 192, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Zuccarino, F.; Vollmer, I.; Sanchez, G.; Navallas, M.; Pugliese, F.; Gayete, A. Left ventricular noncompaction: Imaging findings and diagnostic criteria. AJR Am. J. Roentgenol. 2015, 204, 519–530. [Google Scholar] [CrossRef]
- Halliburton, S.S.; Abbara, S.; Chen, M.Y.; Gentry, R.; Mahesh, M.; Raff, G.L.; Shaw, L.J.; Hausleiter, J. SCCT guidelines on radiation dose and dose-optimization strategies in cardiovascular CT. J. Cardiovasc. Comput. Tomogr. 2011, 5, 198–224. [Google Scholar] [CrossRef] [Green Version]
- Birnie, D.H.; Sauer, W.H.; Bogun, F.; Cooper, J.M.; Culver, D.A.; Duvernoy, C.S.; Judson, M.A.; Kron, J.; Mehta, D.; Cosedis Nielsen, J.; et al. HRS expert consensus statement on the diagnosis and management of arrhythmias associated with cardiac sarcoidosis. Heart Rhythm 2014, 11, 1305–1323. [Google Scholar] [CrossRef]
- De Cobelli, F.; Pieroni, M.; Esposito, A.; Chimenti, C.; Belloni, E.; Mellone, R.; Canu, T.; Perseghin, G.; Gaudio, C.; Maseri, A.; et al. Delayed gadolinium-enhanced cardiac magnetic resonance in patients with chronic myocarditis presenting with heart failure or recurrent arrhythmias. J. Am. Coll. Cardiol. 2006, 47, 1649–1654. [Google Scholar] [CrossRef] [Green Version]
- Marcus, F.I.; McKenna, W.J.; Sherrill, D.; Basso, C.; Bauce, B.; Bluemke, D.A.; Calkins, H.; Corrado, D.; Cox, M.G.; Daubert, J.P.; et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: Proposed modification of the task force criteria. Circulation 2010, 121, 1533–1541. [Google Scholar] [CrossRef]
- Zemrak, F.; Ahlman, M.A.; Captur, G.; Mohiddin, S.A.; Kawel-Boehm, N.; Prince, M.R.; Moon, J.C.; Hundley, W.G.; Lima, J.A.; Bluemke, D.A.; et al. The relationship of left ventricular trabeculation to ventricular function and structure over a 9.5-year follow-up: The mesa study. J. Am. Coll. Cardiol. 2014, 64, 1971–1980. [Google Scholar] [CrossRef] [Green Version]
- Doshi, D.; Ben-Yehuda, O.; Bonafede, M.; Josephy, N.; Karmpaliotis, D.; Parikh, M.A.; Moses, J.W.; Stone, G.W.; Leon, M.B.; Schwartz, A.; et al. Underutilization of coronary artery disease testing among patients hospitalized with new-onset heart failure. J. Am. Coll. Cardiol. 2016, 68, 450–458. [Google Scholar] [CrossRef]
- Levine, A.; Hecht, H.S. Cardiac CT angiography in congestive heart failure. J. Nucl. Med. 2015, 56 (Suppl. 4), 46S–51S. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | 62.6 ± 16.1 |
|---|---|
| Male gender | 31 (49.2%) |
| BMI, kg/m2 | 24.1 ± 5.0 |
| Inpatient: Outpatient | 47 (74.6%): 16 (25.4%) |
| NYHA class | |
| Class I | 4 (6.3%) |
| Class II | 40 (63.5%) |
| Class III | 17 (27.0%) |
| Class IV | 2 (3.2%) |
| Laboratory findings | |
| White blood cell (×103/μL) | 7.1 ± 2.1 |
| Hemoglobin (g/dL) | 13.5 ± 2.47 |
| Albumin (g/dL) | 3.8 ± 0.6 |
| Cholesterol (mg/dL) | 149.6 ± 36.9 |
| Sodium (mmol/L) | 140.1 ± 2.6 |
| eGFR (mL/min/1.73 m2) | 86.7 ± 16.8 |
| Creatinine (mg/dL) | 0.8 ± 0.2 |
| NT-proBNP (pg/mL) | 4802.4 ± 6124.1 |
| Clinical history | |
| Hypertension | 32 (50.8%) |
| Diabetes mellitus | 23 (36.5%) |
| Dyslipidemia | 8 (12.7%) |
| Current/ex-smoker | 13 (20.6%)/8 (12.7%) |
| Alcohol | 16 (25.4%) |
| Echocardiography findings | |
| LVEDD, mm | 64.3 ± 6.7 |
| LVEF, % | 28.3 ± 8.2 |
| Fractional shortening, % | 21.8 ± 12.6 |
| Observer 1 | Observer 2 | Kappa | ||
|---|---|---|---|---|
| CAD | No significant CAD | 43 | 44 | 0.806 |
| 1-vessel disease | 6 | 7 | ||
| 2-vessel disease | 8 | 6 | ||
| 3-vessel disease | 6 | 6 | ||
| MDE | No | 21 | 22 | 0.806 |
| Infarction | 15 | 16 | ||
| Non-ischemic | 27 | 25 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Im, D.J.; Youn, J.-C.; Lee, H.-J.; Nam, K.; Suh, Y.J.; Hong, Y.J.; Hur, J.; Kim, Y.J.; Choi, B.W.; Kang, S.-M. Role of Cardiac Computed Tomography for Etiology Evaluation of Newly Diagnosed Heart Failure with Reduced Ejection Fraction. J. Clin. Med. 2020, 9, 2270. https://doi.org/10.3390/jcm9072270
Im DJ, Youn J-C, Lee H-J, Nam K, Suh YJ, Hong YJ, Hur J, Kim YJ, Choi BW, Kang S-M. Role of Cardiac Computed Tomography for Etiology Evaluation of Newly Diagnosed Heart Failure with Reduced Ejection Fraction. Journal of Clinical Medicine. 2020; 9(7):2270. https://doi.org/10.3390/jcm9072270
Chicago/Turabian StyleIm, Dong Jin, Jong-Chan Youn, Hye-Jeong Lee, Kyungsun Nam, Young Joo Suh, Yoo Jin Hong, Jin Hur, Young Jin Kim, Byoung Wook Choi, and Seok-Min Kang. 2020. "Role of Cardiac Computed Tomography for Etiology Evaluation of Newly Diagnosed Heart Failure with Reduced Ejection Fraction" Journal of Clinical Medicine 9, no. 7: 2270. https://doi.org/10.3390/jcm9072270