Hormonal Blood Pressure Regulation during General Anesthesia Using a Standardized Propofol Dosage in Children and Adolescents Seems Not to Be Affected by Body Weight

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Induction and Maintenance of Anesthesia
2.2. Monitoring
2.3. Measurement of Hormone Levels
2.4. Statistical Analysis
3. Results
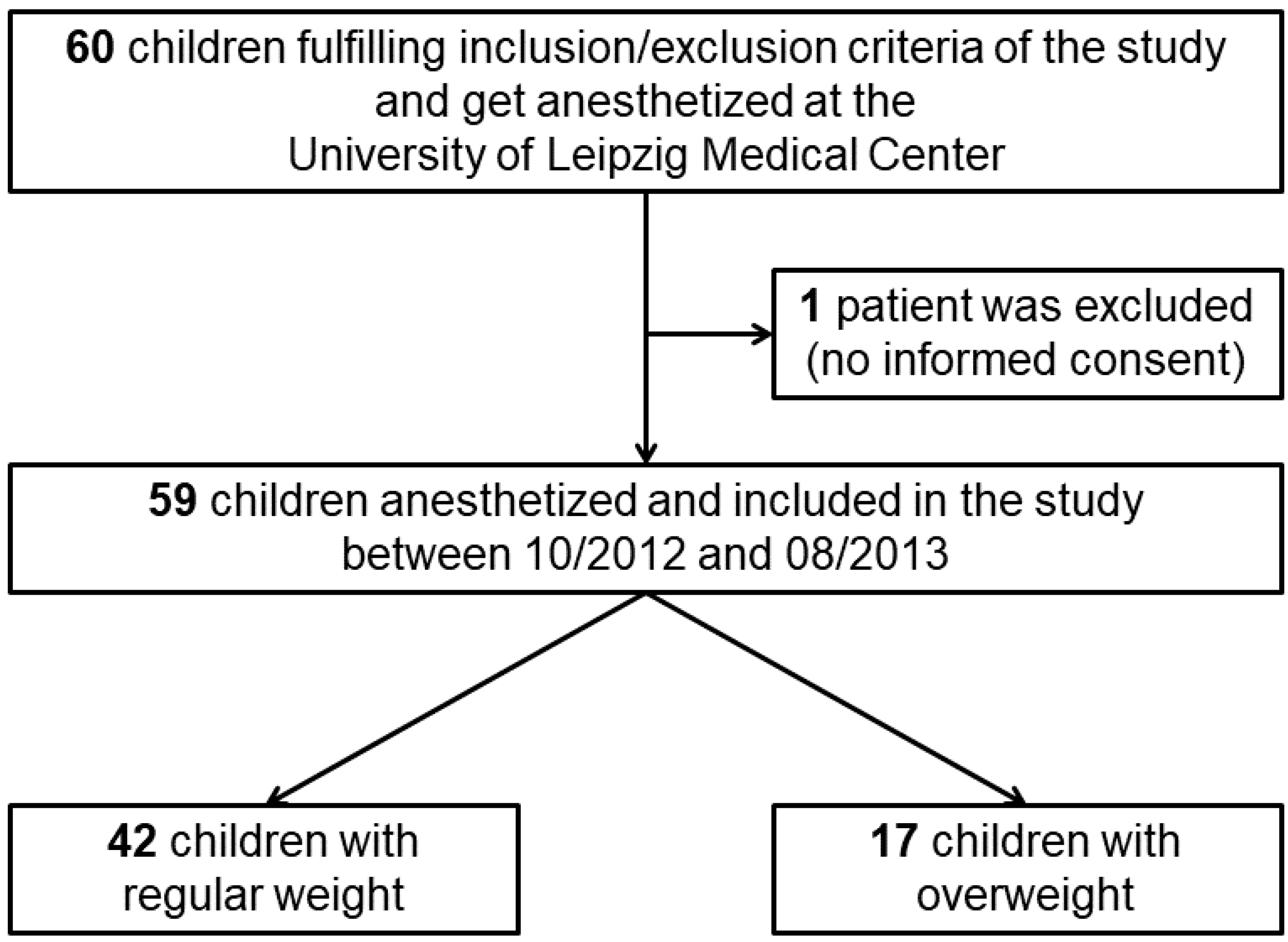
3.1. Demographics and Anesthesia-Related Parameters
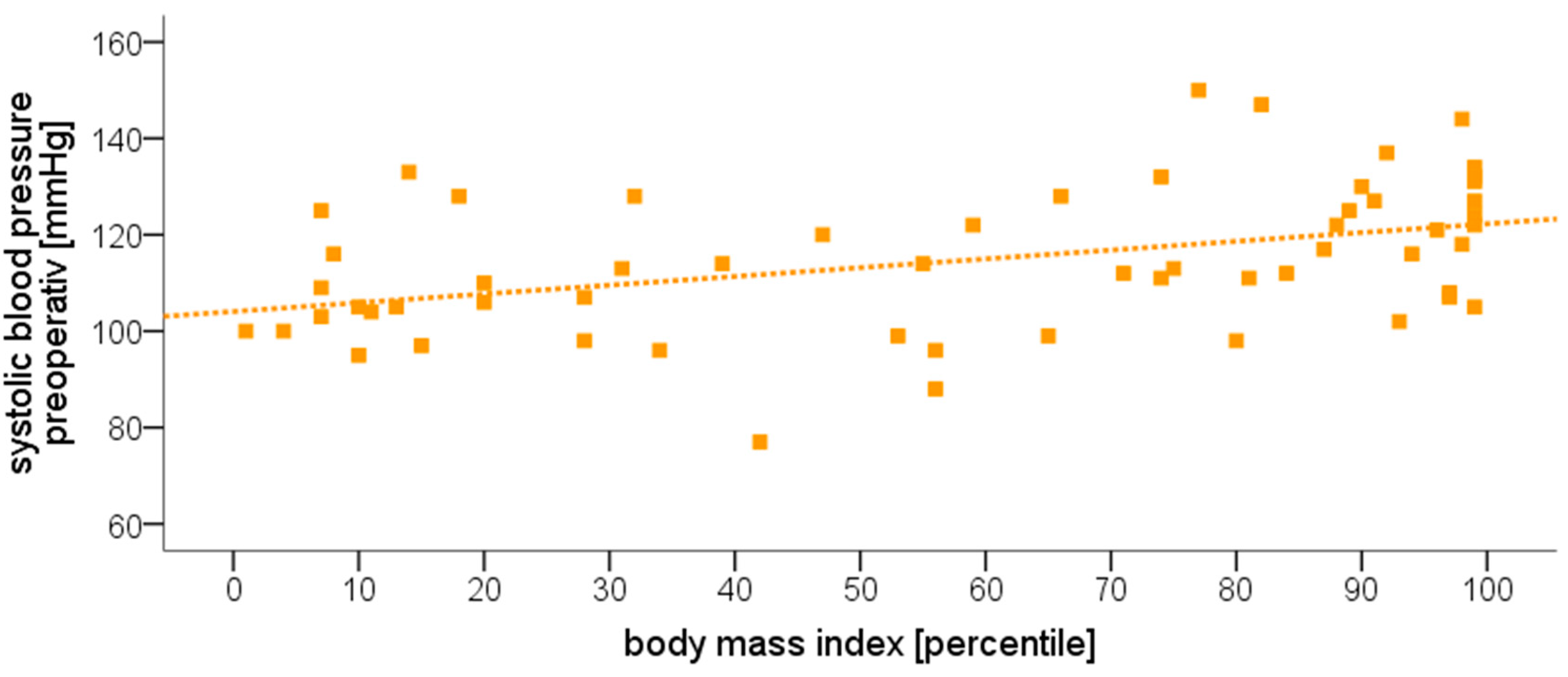
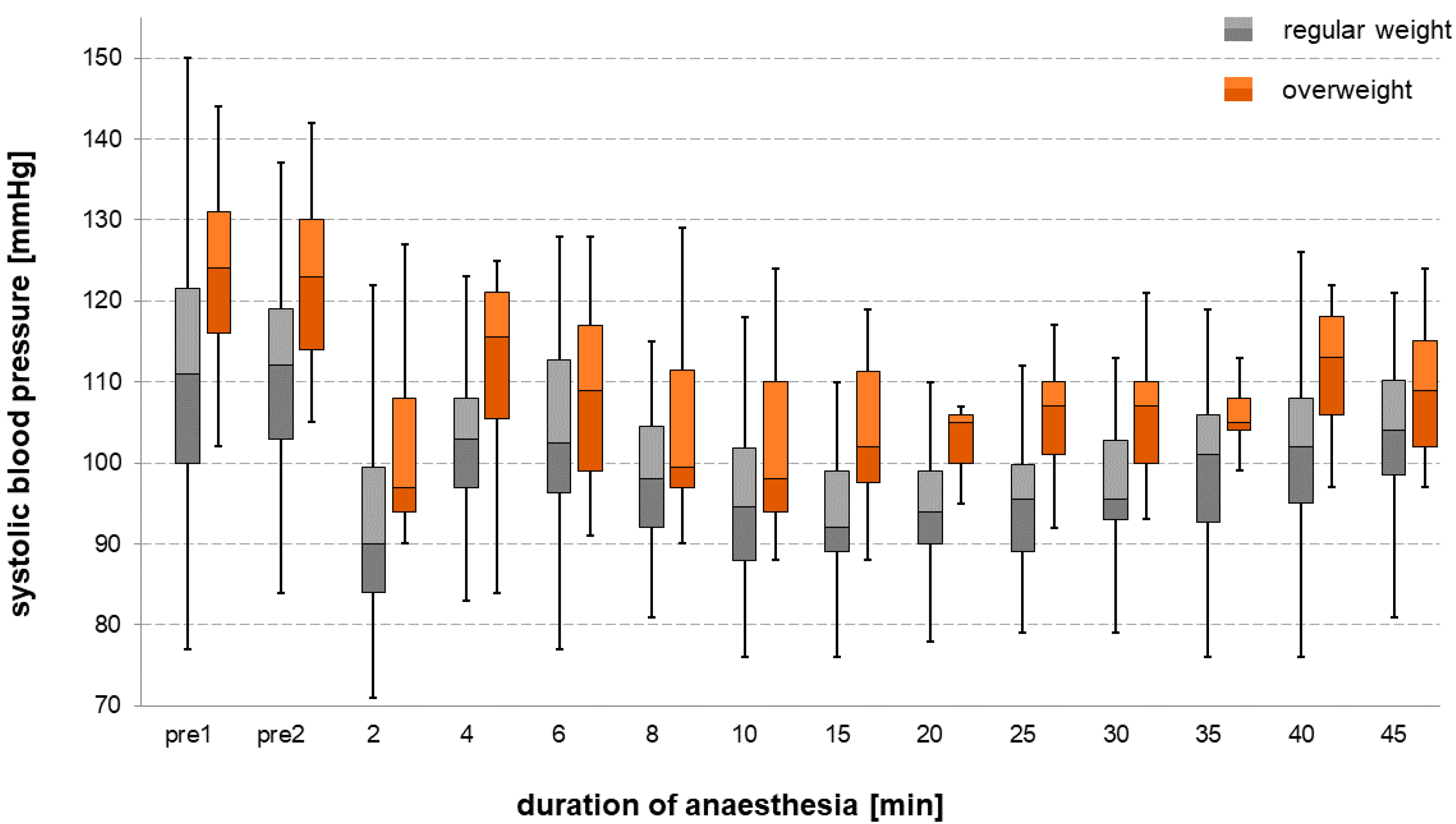
3.2. Blood Pressure
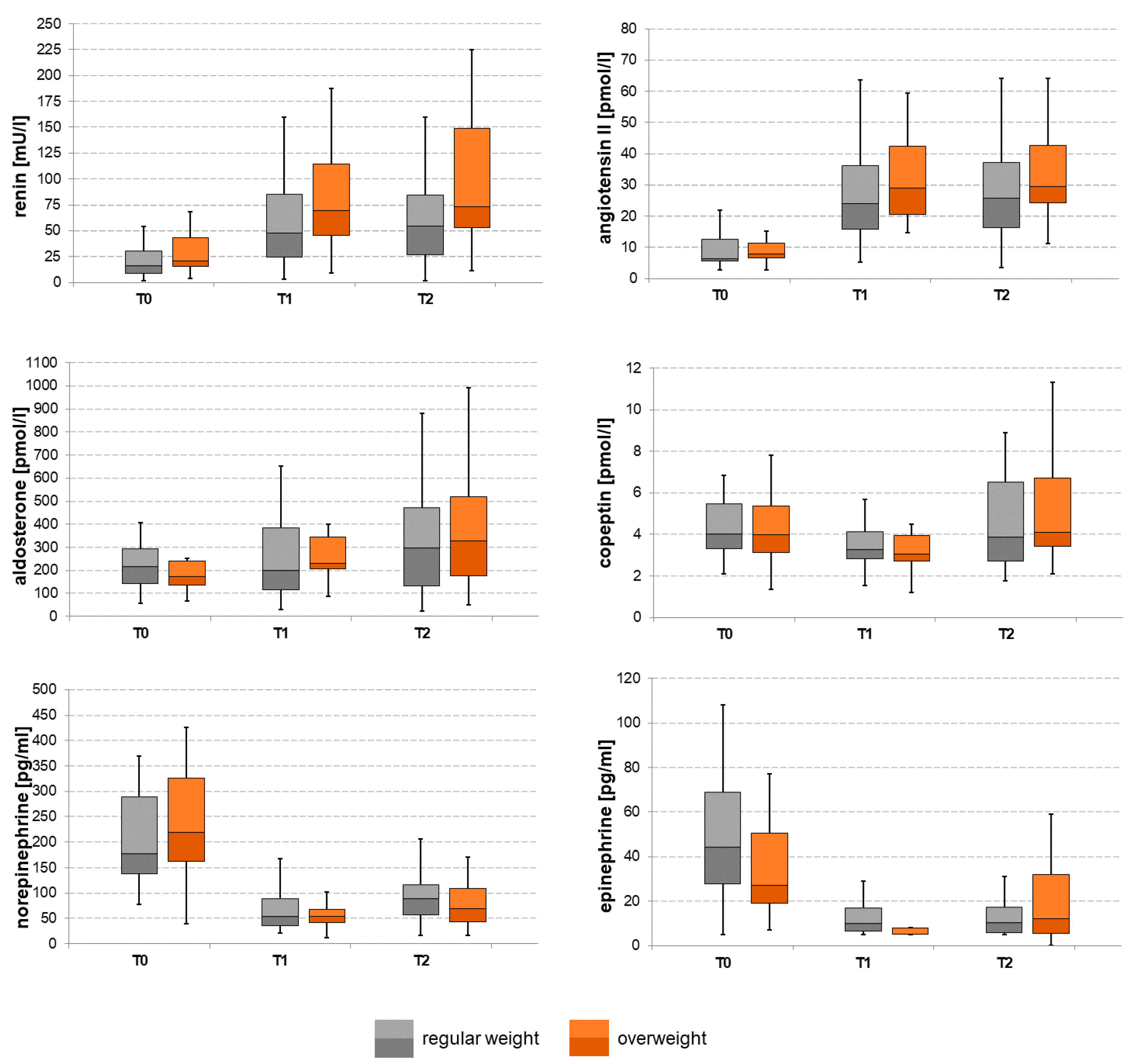
3.3. Changes in Hormone Levels During the Course of Anesthesia
3.4. Limitations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Goh, A.-C.N.; Bagshaw, O.; Courtman, S. A follow-up survey of total intravenous anesthesia usage in children in the U.K. and Ireland. Paediatr. Anaesth. 2019, 29, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Lauder, G.R. Total intravenous anesthesia will supercede inhalational anesthesia in pediatric anesthetic practice. Paediatr. Anaesth. 2015, 25, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Apfel, C.C.; Heidrich, F.M.; Jukar-Rao, S.; Jalota, L.; Hornuss, C.; Whelan, R.P.; Zhang, K.; Cakmakkaya, O.S. Evidence-based analysis of risk factors for postoperative nausea and vomiting. Br. J. Anaesth. 2012, 109, 742–753. [Google Scholar] [CrossRef] [Green Version]
- Gan, T.J.; Diemunsch, P.; Habib, A.S.; Kovac, A.; Kranke, P.; Meyer, T.A.; Watcha, M.; Chung, F.; Angus, S.; Apfel, C.C.; et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesth. Analg. 2014, 118, 85–113. [Google Scholar] [CrossRef] [Green Version]
- Chidambaran, V.; Costandi, A.; D’Mello, A. Propofol: A review of its role in pediatric anesthesia and sedation. CNS Drugs 2015, 29, 543–563. [Google Scholar] [CrossRef] [PubMed]
- Nafiu, O.O.; Kheterpal, S.; Morris, M.; Reynolds, P.I.; Malviya, S.; Tremper, K.K. Incidence and risk factors for preincision hypotension in a noncardiac pediatric surgical population. Paediatr. Anaesth. 2009, 19, 232–239. [Google Scholar] [CrossRef] [Green Version]
- Graaff, J.C.d.; Pasma, W.; van Buuren, S.; Duijghuisen, J.J.; Nafiu, O.O.; Kheterpal, S.; van Klei, W.A. Reference values for noninvasive blood pressure in children during anesthesia: A multicentered retrospective observational cohort study. Anesthesiology 2016, 125, 904–913. [Google Scholar] [CrossRef] [Green Version]
- Habre, W.; Disma, N.; Virag, K.; Becke, K.; Hansen, T.G.; Jöhr, M.; Leva, B.; Morton, N.S.; Vermeulen, P.M.; Zielinska, M.; et al. Incidence of severe critical events in paediatric anaesthesia (APRICOT): A prospective multicentre observational study in 261 hospitals in Europe. Lancet Respir. Med. 2017, 5, 412–425. [Google Scholar] [CrossRef]
- Aun, C.S.; Short, S.M.; Leung, D.H.; Oh, T.E. Induction dose-response of propofol in unpremedicated children. Br. J. Anaesth. 1992, 68, 64–67. [Google Scholar] [CrossRef]
- McFarlan, C.S.; Anderson, B.J.; Short, T.G. The use of propofol infusions in paediatric anaesthesia: A practical guide. Paediatr. Anaesth. 1999, 9, 209–216. [Google Scholar] [CrossRef]
- Olutoye, O.A.; Yu, X.; Govindan, K.; Tjia, I.M.; East, D.L.; Spearman, R.; Garcia, P.J.; Coulter-Nava, C.; Needham, J.; Abrams, S.; et al. The effect of obesity on the ED (95) of propofol for loss of consciousness in children and adolescents. Anesth. Analg. 2012, 115, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Nafiu, O.O.; Maclean, S.; Blum, J.; Kheterpal, S.; Cowan, A.; Tremper, K.K. High BMI in children as a risk factor for intraoperative hypotension. Eur. J. Anaesthesiol. 2010, 27, 1065–1068. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.J.; Holford, N.H. What is the best size predictor for dose in the obese child? Paediatr. Anaesth. 2017, 27, 1176–1184. [Google Scholar] [CrossRef]
- Claeys, M.A.; Gepts, E.; Camu, F. Haemodynamic changes during anaesthesia induced and maintained with propofol. Br. J. Anaesth. 1988, 60, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Minami, K.; Yanagihara, N.; Segawa, K.; Tsutsui, M.; Shigematsu, A.; Izumi, F. Inhibitory effects of propofol on catecholamine secretion and uptake in cultured bovine adrenal medullary cells. Naunyn Schmiedebergs Arch. Pharmacol. 1996, 353, 572–578. [Google Scholar] [CrossRef]
- Engeli, S.; Negrel, R.; Sharma, A.M. Physiology and pathophysiology of the adipose tissue renin-angiotensin system. Hypertension 2000, 35, 1270–1277. [Google Scholar] [CrossRef]
- Shatat, I.F.; Flynn, J.T. Relationships between renin, aldosterone, and 24-hour ambulatory blood pressure in obese adolescents. Pediatr. Res. 2011, 69, 336–340. [Google Scholar] [CrossRef] [Green Version]
- Weise, M.; Eisenhofer, G.; Merke, D.P. Pubertal and gender-related changes in the sympathoadrenal system in healthy children. J. Clin. Endocrinol. Metab. 2002, 87, 5038–5043. [Google Scholar] [CrossRef] [Green Version]
- Jerez, S.; Scacchi, F.; Sierra, L.; Karbiner, S.; Bruno, M.P. de Vascular hyporeactivity to angiotensin II and noradrenaline in a rabbit model of obesity. J. Cardiovasc. Pharmacol. 2012, 59, 49–57. [Google Scholar] [CrossRef]
- Smith, I.; Kranke, P.; Murat, I.; Smith, A.; O’Sullivan, G.; Søreide, E.; Spies, C.; In’t Veld, B. Perioperative fasting in adults and children: Guidelines from the European Society of Anaesthesiology. Eur. J. Anaesthesiol. 2011, 28, 556–569. [Google Scholar] [CrossRef]
- Eisenhofer, G.; Goldstein, D.S.; Stull, R.; Keiser, H.R.; Sunderland, T.; Murphy, D.L.; Kopin, I.J. Simultaneous liquid-chromatographic determination of 3,4-dihydroxyphenylglycol, catecholamines, and 3,4-dihydroxyphenylalanine in plasma, and their responses to inhibition of monoamine oxidase. Clin. Chem. 1986, 32, 2030–2033. [Google Scholar] [CrossRef]
- Lenders, J.W.; Eisenhofer, G.; Armando, I.; Keiser, H.R.; Goldstein, D.S.; Kopin, I.J. Determination of metanephrines in plasma by liquid chromatography with electrochemical detection. Clin. Chem. 1993, 39, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Tebar, W.R.; Ritti-Dias, R.M.; Farah, B.Q.; Zanuto, E.F.; Vanderlei, L.C.M.; Christofaro, D.G.D. High blood pressure and its relationship to adiposity in a school-aged population: Body mass index vs. waist circumference. Hypertens. Res. 2018, 41, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Stewart, M.; Scattoloni, J.; Tazhibi, G.; Nafiu, O.O. Association of elevated preoperative blood pressure with preincision hypotension in pediatric surgical patients. Paediatr. Anaesth. 2016, 26, 844–851. [Google Scholar] [CrossRef] [Green Version]
- Masuo, K.; Mikami, H.; Itoh, M.; Ogihara, T.; Tuck, M.L. Sympathetic activity and body mass index contribute to blood pressure levels. Hypertens. Res. 2000, 23, 303–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mameli, C.; Krakauer, N.Y.; Krakauer, J.C.; Bosetti, A.; Ferrari, C.M.; Moiana, N.; Schneider, L.; Borsani, B.; Genoni, T.; Zuccotti, G. The association between a body shape index and cardiovascular risk in overweight and obese children and adolescents. PLoS ONE 2018, 13, e0190426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becton, L.J.; Shatat, I.F.; Flynn, J.T. Hypertension and obesity: Epidemiology, mechanisms and clinical approach. Indian J. Pediatr. 2012, 79, 1056–1061. [Google Scholar] [CrossRef]
- Lapage, K.G.; Wouters, P.F. The patient with hypertension undergoing surgery. Curr. Opin. Anaesthesiol. 2016, 29, 397–402. [Google Scholar] [CrossRef]
- Morgenthaler, N.G.; Struck, J.; Jochberger, S.; Dünser, M.W. Copeptin: Clinical use of a new biomarker. Trends Endocrinol. Metab. 2008, 19, 43–49. [Google Scholar] [CrossRef]
- Ebert, T.J.; Muzi, M.; Berens, R.; Goff, D.; Kampine, J.P. Sympathetic responses to induction of anesthesia in humans with propofol or etomidate. Anesthesiology 1992, 76, 725–733. [Google Scholar] [CrossRef]
- Hoka, S.; Yamaura, K.; Takenaka, T.; Takahashi, S. Propofol-induced increase in vascular capacitance is due to inhibition of sympathetic vasoconstrictive activity. Anesthesiology 1998, 89, 1495–1500. [Google Scholar] [CrossRef] [PubMed]
- Boillot, A.; Laurant, P.; Berthelot, A.; Barale, F. Effects of propofol on vascular reactivity in isolated aortae from normotensive and spontaneously hypertensive rats. Br. J. Anaesth. 1999, 83, 622–629. [Google Scholar] [CrossRef]
- Philbin, D.M.; Rosow, C.E.; Schneider, R.C.; Koski, G.; D’Ambra, M.N. Fentanyl and sufentanil anesthesia revisited: How much is enough? Anesthesiology 1990, 73, 5–11. [Google Scholar] [CrossRef]
- Bali, A.; Singh, N.; Jaggi, A.S. Renin-angiotensin system in pain: Existing in a double life? J. Renin Angiotensin Aldosterone Syst. 2014, 15, 329–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauermann, E.; Blum, C.A.; Lurati Buse, G.; Bandschapp, O.; Ruppen, W. Time course of copeptin during a model of experimental pain and hyperalgesia: A randomised volunteer crossover trial. Eur. J. Anaesthesiol. 2017, 34, 306–314. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group “Regular Weight” | Group “Overweight” | p-Value (1) | ||
|---|---|---|---|---|
| n | 42 | 17 | ||
| Sex | Male (%) | 19 (45.2%) | 11 (64.7%) | 0.252(2) |
| Female (%) | 23 (54.8%) | 6 (35.3%) | ||
| Age (years) | 12.5 (10–14) | 12 (9–14) | 0.775 | |
| Height (cm) | 158 (141–165) | 164 (149–171) | 0.162 | |
| percentile | 55 (28–78) | 87 (40–96) | 0.008 | |
| Weight (kg) | 48.5 (33.5–54.5) | 71.0 (53.8–80.6) | <0.001 | |
| percentile | 45.5 (25–70) | 98 (95–99) | <0.001 | |
| BMI (kg/m2) | 18.2 (15.7–20.8) | 25.8 (23.0–29.4) | <0.001 | |
| percentile | 41 (14–74) | 98 (94–99) | <0.001 | |
| ASA (n (%)) | 1 | 29 (69.0%) | 9 (52.9%) | 0.368(2) |
| 2 | 13 (31.0%) | 8 (47.1%) | ||
| Type of surgery (n (%)) | Ortho/trauma surgery | 32 (76.2%) | 15 (88.2) | 0.478(2) |
| General surgery | 10 (23.8%) | 2 (11.8%) | ||
| Group “Regular Weight” | Group “Overweight” | p-Value (1) | |
|---|---|---|---|
| Duration of anesthesia (min) | 118 (88–162) | 116 (103–139) | 0.847 |
| Duration of surgery (min) | 61 (42–110) | 60 (53–79) | 0.913 |
| Start of surgery (min after induction of anesthesia) | 29.5 (25.8–37.3) | 33.0 (28.5–41.0) | 0.180 |
| Propofol dosage for induction of anesthesia (mg/kg*BW) | 3.2 (3.2–3.3) | 2.0 (2.0–2.1) | <0.001 |
| Propofol cumulative up to 45 min (mg/kg*BW) | 11.6 (10.9–12.2) | 10.2 (9.6–11.6) | 0.005 |
| Fentanyl dosage at induction (µg/kg*BW) | 2.0 (2.0–2.1) | 2.0 (2.0–2.1) | 0.966 |
| Fentanyl cumulative up to 45 min (µg/kg*BW) | 3.7 (3.0–4.3) | 3.2 (2.9–3.9) | 0.170 |
| Crystalloid (mL/kg*BW) | 7.4 (5.4–8.9) | 4.5 (3.2–5.7) | <0.001 |
| Crystalloid cumulative up to 45 min (mL) | 350 (200–450) | 350 (175–450) | 0.781 |
| Correlation of Preoperative Systolic Blood Pressure with Preoperative Levels of | Spearman’s Rank Correlation Coefficient (ρ) | p-Value |
|---|---|---|
| Renin (mU/L) | 0.158 | 0.240 |
| Angiotensin II (adj.) (pmol/L) | 0.121 | 0.369 |
| Aldosterone (pmol/L) | 0.274 | 0.039 |
| Copeptin (pmol/L) | −0.193 | 0.155 |
| Epinephrine (pg/mL) | 0.141 | 0.324 |
| Norepinephrine (pg/mL) | 0.485 | <0.001 |
| Correlation of Body Mass Index with Preoperative Levels of | Spearman’s Rank Correlation Coefficient (ρ) | p-Value |
|---|---|---|
| Renin (mU/L) | 0.363 | 0.005 |
| Angiotensin II (adj.) (pmol/L) | 0.082 | 0.545 |
| Aldosterone (pmol/L) | 0.146 | 0.277 |
| Copeptin (pmol/L) | −0.226 | 0.094 |
| Epinephrine (pg/mL) | −0.055 | 0.701 |
| Norepinephrine (pg/mL) | 0.019 | 0.180 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hempel, G.; Maier, A.-M.; Piegeler, T.; Stehr, S.N.; Kratzsch, J.; Höhne, C. Hormonal Blood Pressure Regulation during General Anesthesia Using a Standardized Propofol Dosage in Children and Adolescents Seems Not to Be Affected by Body Weight. J. Clin. Med. 2020, 9, 2129. https://doi.org/10.3390/jcm9072129
Hempel G, Maier A-M, Piegeler T, Stehr SN, Kratzsch J, Höhne C. Hormonal Blood Pressure Regulation during General Anesthesia Using a Standardized Propofol Dosage in Children and Adolescents Seems Not to Be Affected by Body Weight. Journal of Clinical Medicine. 2020; 9(7):2129. https://doi.org/10.3390/jcm9072129
Chicago/Turabian StyleHempel, Gunther, Anne-Marie Maier, Tobias Piegeler, Sebastian N. Stehr, Jürgen Kratzsch, and Claudia Höhne. 2020. "Hormonal Blood Pressure Regulation during General Anesthesia Using a Standardized Propofol Dosage in Children and Adolescents Seems Not to Be Affected by Body Weight" Journal of Clinical Medicine 9, no. 7: 2129. https://doi.org/10.3390/jcm9072129