Should We Perform Old-For-Old Kidney Transplantation during the COVID-19 Pandemic? The Risk for Post-Operative Intensive Stay

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Outcome Measures
2.2. Statistical Analysis
3. Results
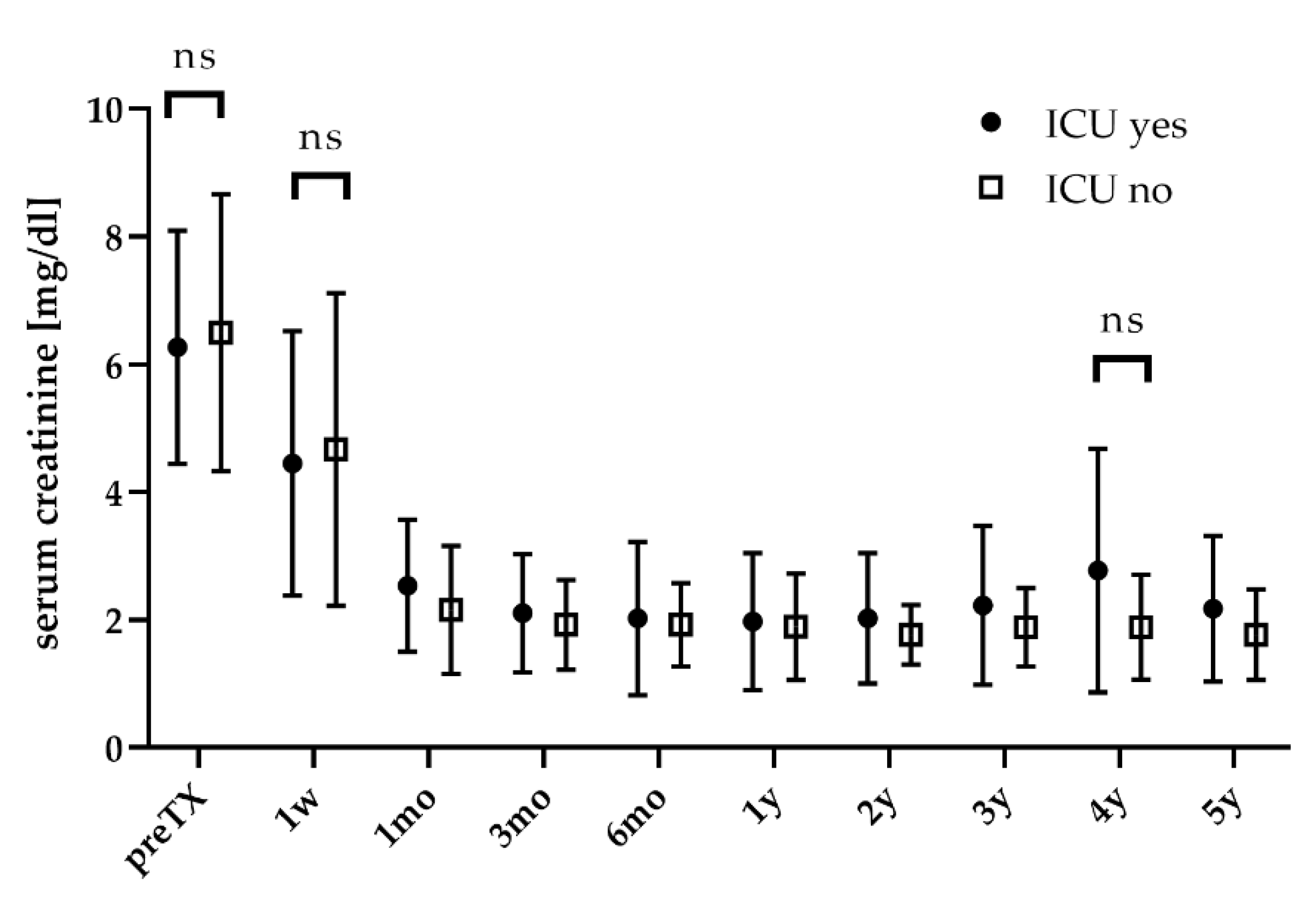
3.1. Overall Results Regarding ICU Admission
3.2. Donor- and Recipient-Age-Dependent Comparison
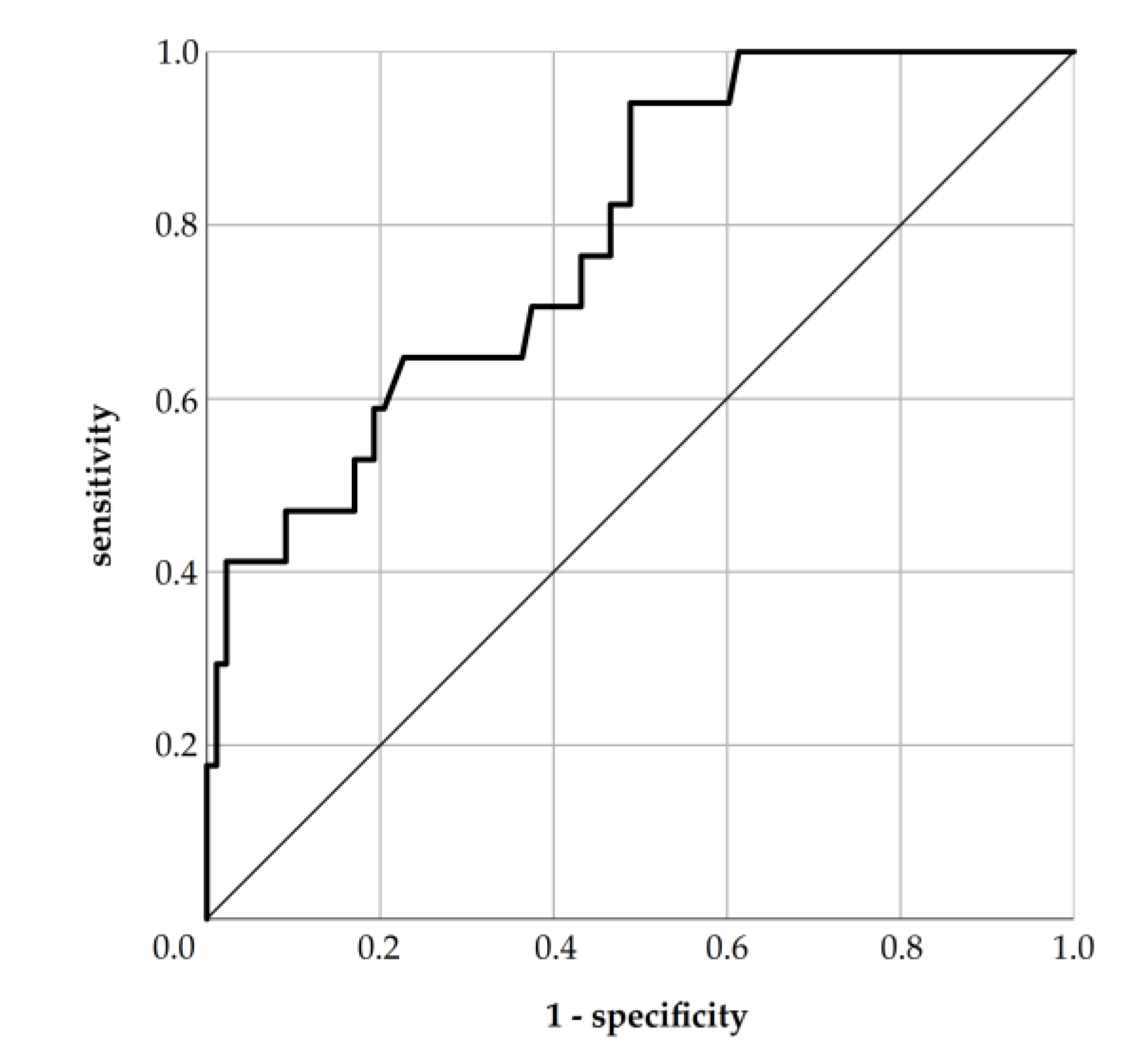
3.3. Risk Model for ICU Stay
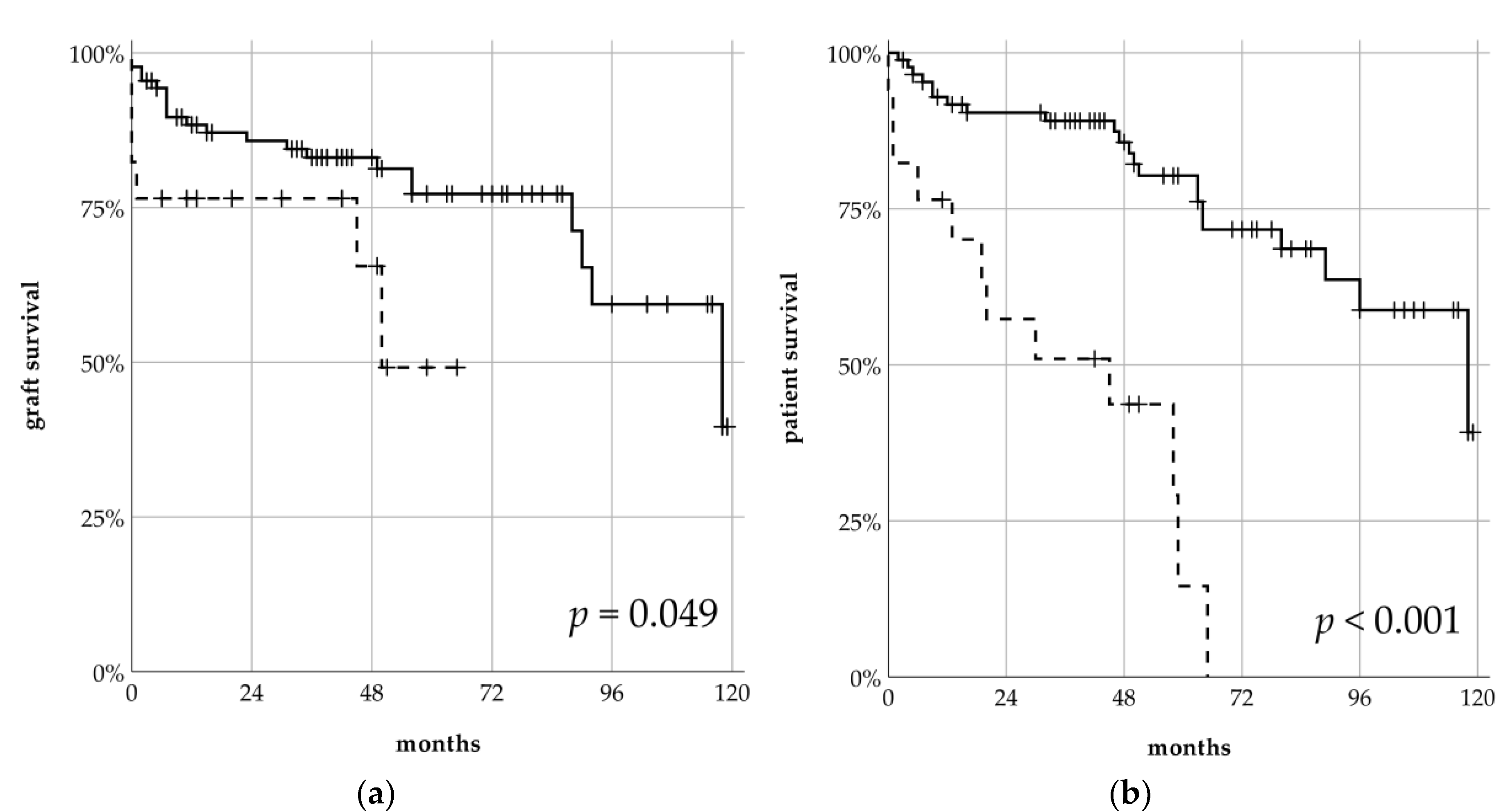
3.4. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
Appendix A.1. Risk Model for ICU Admission
- HN: presence of hypertensive nephropathy (binary: no = 0, yes = 1)
- CAD: presence of coronary artery disease (binary: no = 0, yes = 1)
- BMI: body-mass-index in kg/m2 (continuous)


{kind=link}
{kind=link}
{kind=link}
| ICU Yes | ICU No | ∑ | |
|---|---|---|---|
| risk model: ICU yes | 16 | 43 | 59 |
| risk model: ICU no | 1 | 45 | 46 |
| ∑ | 17 | 88 | 105 |
Appendix A.2. Graft and Patient Survival Stratified for Donor and Recipient Age
| Donors: Very Old-For-Old vs. Old-For-Old | Recipients: Old-For-Very Old vs. Old-For-Old | |||||
|---|---|---|---|---|---|---|
| Very Old (n = 28) |
Old (n = 77) | p | Very Old (n = 47) | Old (n = 58) | p | |
| Graft Survival | n.s. | n.s. | ||||
| 1 year | 22 (78%) | 61 (86%) | 37 (87%) | 46 (82%) | ||
| 5 years | 11 (78%) | 25 (72%) | 18 (73%) | 18 (75%) | ||
| 9 years | 2 (58%) | 6 (41%) | 108 (60%) | 4 (35%) | ||
| Patient Survival | n.s. | n.s. | ||||
| 1 year | 25 (78%) | 63 (90%) | 39 (82%) | 49 (87%) | ||
| 5 years | 12 (74%) | 28 (59%) | 21 (60%) | 19 (63%) | ||
| 9 years | 1 (36%) | 6 (54%) | 2 (55%) | 5 (33%) | ||
Appendix A.3. Underlying Renal Diseases
| ∑ (n = 105) | ICU Yes (n = 17) | ICU No (n = 88) | p-Value | |
|---|---|---|---|---|
| ADPKD | 11 (10.5%) | 2 (11.8%) | 9 (10.2%) | n.s. |
| amyloidosis | 3 (2.9%) | - | 3 (3.4%) | n.s. |
| analgesic nephropathy | 3 (2.9%) | 1 (5.9%) | 2 (2.3%) | n.s. |
| chronic glomerulonephritis | 23 (21.9%) | 1 (5.9%) | 22 (25%) | n.s. |
| cardiac cirrhosis | 1 (1%) | 1 (1.1%) | n.s. | |
| diabetic nephropathy | 17 (16.2%) | 2 (11.8%) | 15 (17%) | n.s. |
| FSGS | 2 (1.9%) | - | 2 (2.3%) | n.s. |
| goodpasture syndrome | 2 (1.9%) | - | 2 (2.3%) | n.s. |
| hypertensive nephropathy | 15 (14.3%) | 6 (35.3%) | 9 (10.2%) | <0.05 |
| IgA nephropathy | 3 (2.9%) | - | 3 (3.4%) | n.s. |
| kidney cirrhosis | 8 (7.6%) | 2 (11.8%) | 6 (6.8%) | n.s. |
| nephrosclerosis | 7 (6.7%) | 2 (11.8%) | 5 (5.7%) | n.s. |
| other cystic disease | 3 (2.9%) | 1 (5.9%) | 2 (2.2%) | n.s. |
| renal cell carcinoma | 2 (1.9%) | 1 (5.9%) | 1 (1.1%) | n.s. |
| vascular nephropathy | 7 (6.7%) | 3 (17.6%) | 4 (4.5%) | n.s. |
| vasculitis | 2 (1.9%) | 1 (5.9%) | 1 (1.1%) | n.s. |
| not known | 13 (12.5%) | - | 13 (14.8%) | n.s. |
References
- Kumar, D.; Manuel, O.; Natori, Y.; Egawa, H.; Grossi, P.; Han, S.-H.; Fernández-Ruiz, M.; Humar, A. COVID-19: A global transplant perspective on successfully navigating a pandemic. Arab. Archaeol. Epigr. 2020. [Google Scholar] [CrossRef] [Green Version]
- Gori, A.; Dondossola, D.; Antonelli, B.; Mangioni, D.; Alagna, L.; Reggiani, P.; Bandera, A.; Rossi, G. Coronavirus disease 2019 and transplantation: A view from the inside. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2020. [Google Scholar] [CrossRef]
- Nacoti, M.; Ciocca, A.; Giupponi, A.; Brambillasca, P.; Lussana, F.; Pisano, M.; Goisis, G.; Bonacina, D.; Fazzi, F.; Naspro, R.; et al. At the Epicenter of the Covid-19 Pandemic and Humanitarian Crises in Italy: Changing Perspectives on Preparation and Mitigation; NEJM Catalyst: Waltham, MA, USA, 2020. [Google Scholar]
- Stahel, P.F. How to risk-stratify elective surgery during the COVID-19 pandemic? Patient Saf. Surg. 2020, 14, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Phua, J.; Weng, L.; Ling, L.; Egi, M.; Lim, C.-M.; Divatia, J.V.; Shrestha, B.R.; Arabi, Y.M.; Ng, J.; Gomersall, C.D.; et al. Intensive care management of coronavirus disease 2019 (COVID-19): Challenges and recommendations. Lancet Respir. Med. 2020, 8, 506–517. [Google Scholar] [CrossRef]
- Stensland, K.D.; Morgan, T.M.; Moinzadeh, A.; Lee, C.T.; Briganti, A.; Catto, J.W.; Canes, D. Considerations in the Triage of Urologic Surgeries During the COVID-19 Pandemic. Eur. Urol. 2020, 77, 663–666. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Chiang, T.P.-Y.; Werbel, W.A.; Durand, C.M.; Avery, R.; Getsin, S.N.; Jackson, K.R.; Kernodle, A.B.; Rasmussen, S.E.V.P.; Massie, A.B.; et al. Early impact of COVID-19 on transplant center practices and policies in the United States. Arab. Archaeol. Epigr. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akalin, E.; Azzi, Y.; Bartash, R.; Seethamraju, H.; Parides, M.; Hemmige, V.; Ross, M.; Forest, S.; Goldstein, Y.D.; Ajaimy, M.; et al. Covid-19 and Kidney Transplantation. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ritschl, P.; Nevermann, N.; Wiering, L.; Wu, H.H.; Morodor, P.; Brandl, A.; Hillebrandt, K.; Tacke, F.; Friedersdorff, F.; Schlomm, T.; et al. Solid organ transplantation programs facing lack of empiric evidence in the COVID-19 pandemic: A By-proxy Society Recommendation Consensus approach. Arab. Archaeol. Epigr. 2020. [Google Scholar] [CrossRef]
- Angelico, R.; Trapani, S.; Manzia, T.M.; Lombardini, L.; Tisone, G.; Cardillo, M. The COVID-19 outbreak in Italy: Initial implications for organ transplantation programs. Arab. Archaeol. Epigr. 2020. [Google Scholar] [CrossRef]
- Kronbichler, A.; Gauckler, P.; Windpessl, M.; Shin, J.I.; Jha, V.; Rovin, B.H.; Oberbauer, R. COVID-19: implications for immunosuppression in kidney disease and transplantation. Nat. Rev. Nephrol. 2020, 1–3. [Google Scholar] [CrossRef]
- Maggiore, U.; Abramowicz, D.; Crespo, M.; Mariat, C.; Mjoen, G.; Peruzzi, L.; Sever, M.S.; Oniscu, G.C.; Hilbrands, L.; Watschinger, B. How should I manage immunosuppression in a kidney transplant patient with COVID-19? An Era-Edta Descartes expert opinion. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2020. [Google Scholar] [CrossRef] [PubMed]
- American Society of, T. FAQs for Organ Transplantation. Available online: https://www.myast.org/sites/default/files/internal/COVID19%20FAQ%20Tx%20Centers%2005.11.2020.pdf (accessed on 18 May 2020).
- Ribal, M.J.; Cornford, P.; Briganti, A.; Knoll, T.; Gravas, S.; Babjuk, M.; Harding, C.; Breda, A.; Bex, A.; Rassweiler, J.J.; et al. European Association of Urology Guidelines Office Rapid Reaction Group: An Organisation-wide Collaborative Effort to Adapt the European Association of Urology Guidelines Recommendations to the Coronavirus Disease 2019 Era. Eur. Urol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Garcia, G.G.; World Kidney Day Steering Committee 2012; Harden, P.; Chapman, J. The global role of kidney transplantation. J. Nephrol. 2012, 25, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreyer, G.J.; De Fijter, J.W. Transplanting the Elderly: Mandatory Age- and Minimal Histocompatibility Matching. Front. Immunol. 2020, 11, 359. [Google Scholar] [CrossRef] [Green Version]
- Lehner, L.J.; Kleinsteuber, A.; Halleck, F.; Khadzhynov, D.; Schrezenmeier, E.; Duerr, M.; Eckardt, K.-U.; Budde, K.; Staeck, O. Assessment of the Kidney Donor Profile Index in a European cohort. Nephrol. Dial. Transplant. 2018, 33, 1465–1472. [Google Scholar] [CrossRef]
- Giessing, M.; Fuller, T.F.; Friedersdorff, F.; Deger, S.; Wille, A.; Neumayer, H.-H.; Schmidt, D.; Budde, K.; Liefeldt, L. Outcomes of transplanting deceased-donor kidneys between elderly donors and recipients. J. Am. Soc. Nephrol. 2008, 20, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Frei, U.; Noeldeke, J.; Machold-Fabrizii, V.; Arbogast, H.; Margreiter, R.; Fricke, L.; Voiculescu, A.; Kliem, V.; Ebel, H.; Albert, U.; et al. Prospective Age-Matching in Elderly Kidney Transplant Recipients—A 5-Year Analysis of the Eurotransplant Senior Program. Arab. Archaeol. Epigr. 2007, 8, 50. [Google Scholar] [CrossRef]
- Quast, L.S.; Grzella, S.; Lengenfeld, T.; Pillokeit, N.; Hummels, M.; Zgoura, P.; Westhoff, T.H.; Viebahn, R.; Schenker, P. Outcome of Kidney Transplantation Using Organs From Brain-dead Donors Older Than 75 Years. Transplant. Proc. 2020, 52, 119–126. [Google Scholar] [CrossRef]
- Jacobi, J.; Beckmann, S.; Heller, K.; Hilgers, K.F.; Apel, H.; Spriewald, B.; Eckardt, K.-U.; Amann, K.U. Deceased Donor Kidney Transplantation in the Eurotransplant Senior Program (ESP): A Single-Center Experience from 2008 to 2013. Ann. Transplant. 2016, 21, 94–104. [Google Scholar] [CrossRef] [Green Version]
- Boesmueller, C.; Biebl, M.; Scheidl, S.; Öllinger, R.; Margreiter, C.; Pratschke, J.; Margreiter, R.; Schneeberger, S. Long-Term Outcome in Kidney Transplant Recipients Over 70 Years in the Eurotransplant Senior Kidney Transplant Program: A Single Center Experience. Transplantation 2011, 92, 210–216. [Google Scholar] [CrossRef]
- Wolters, H.; Bahde, R.; Vowinkel, T.; Unser, J.; Anthoni, C.; Hölzen, J.P.; Suwelack, B.; Senninger, N. Prognostic factors for kidney allograft survival in the Eurotransplant Senior Program. Ann. Transplant. 2014, 19, 201–209. [Google Scholar] [CrossRef]
- Chavalitdhamrong, D.; Gill, J.; Takemoto, S.; Madhira, B.R.; Cho, Y.W.; Shah, T.; Bunnapradist, S. Patient and Graft Outcomes from Deceased Kidney Donors Age 70 Years and Older: An Analysis of the Organ Procurement Transplant Network/United Network of Organ Sharing Database. Transplantation 2008, 85, 1573–1579. [Google Scholar] [CrossRef] [Green Version]
- Bentas, W.; Jones, J.; Karaoguz, A.; Tilp, U.; Probst, M.; Scheuermann, E.; Hauser, I.A.; Jonas, D.; Gossmann, J. Renal transplantation in the elderly: surgical complications and outcome with special emphasis on the Eurotransplant Senior Programme. Nephrol. Dial. Transplant. 2008, 23, 2043–2051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallinat, A.; Feldkamp, T.; Schaffer, R.; Radunz, S.; Treckmann, J.W.; Minor, T.; Witzke, O.; Paul, A.; Sotiropoulos, G.C. Single-Center Experience With Kidney Transplantation Using Deceased Donors Older Than 75 Years. Transplantation 2011, 92, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Abrol, N.; Kashyap, R.; Frank, R.D.; Iyer, V.N.; Dean, P.G.; Stegall, M.D.; Prieto, M.; Kashani, K.B.; Taner, T. Preoperative Factors Predicting Admission to the Intensive Care Unit After Kidney Transplantation. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 285–293. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, F.G.R.; Lombardi, F.; Pacheco, E.S.; De Sandes-Freitas, T.V.; Viana, L.A.; Junior, H.T.-S.; Medina-Pestana, J.O.; Bafi, A.T.; Machado, F.R. Clinical Features of Kidney Transplant Recipients Admitted to the Intensive Care Unit. Prog. Transplant. 2017, 28, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Marques, I.; Caires, R.A.; Machado, D.; Goldenstein, P.; Rodrigues, C.; Pegas, J.; De Paula, F.; David-Neto, E.; Costa, M. Outcomes and Mortality in Renal Transplant Recipients Admitted to the Intensive Care Unit. Transplant. Proc. 2015, 47, 2694–2699. [Google Scholar] [CrossRef]
- Cai, F.; Wang, M.; Wu, X.D.; Xu, X.M.; Su, X.; Shi, Y. Body mass index is associated with the risk of ICU admission and death among patients with pneumonia: A systematic review and meta-analysis. Int. J. Clin. Exp. Med. 2016, 9, 5269–5278. [Google Scholar]
- Pepper, D.J.; Sun, J.; Welsh, J.; Cui, X.; Suffredini, A.F.; Eichacker, P.Q. Increased body mass index and adjusted mortality in ICU patients with sepsis or septic shock: A systematic review and meta-analysis. Crit. Care 2016, 20, 181. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Li, Z.; Yang, T.; Wang, M.; Xi, X. Is body mass index associated with outcomes of mechanically ventilated adult patients in intensive critical units? A systematic review and meta-analysis. PLoS ONE 2018, 13, e0198669. [Google Scholar] [CrossRef] [Green Version]
- Banack, H.R.; Stokes, A. The ‘obesity paradox’ may not be a paradox at all. Int. J. Obes. 2017, 41, 1162–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonopoulos, A.S.; Tousoulis, D. The molecular mechanisms of obesity paradox. Cardiovasc. Res. 2017, 113, 1074–1086. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, M.; Sato, T.; Miyazaki, M.; Matsushima, M.; Sato, H.; Taguma, Y.; Ito, S. Increased risk of cardiovascular events and mortality among non-diabetic chronic kidney disease patients with hypertensive nephropathy: The Gonryo study. Hypertens. Res. 2011, 34, 1106–1110. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Snyder, J.J.; Gilbertson, D.; Matas, A.J. Diabetes mellitus after kidney transplantation in the United States. Arab. Archaeol. Epigr. 2003, 3, 178–185. [Google Scholar] [CrossRef]
- Cosio, F.G.; Pesavento, T.E.; Kim, S.; Osei, K.; Henry, M.; Ferguson, R.M. Patient survival after renal transplantation: IV. Impact of post-transplant diabetes. Kidney Int. 2002, 62, 1440–1446. [Google Scholar] [CrossRef]
- Kuo, H.-T.; Sampaio, M.S.; Vincenti, F.; Bunnapradist, S. Associations of Pretransplant Diabetes Mellitus, New-Onset Diabetes After Transplant, and Acute Rejection With Transplant Outcomes: An Analysis of the Organ Procurement and Transplant Network/United Network for Organ Sharing (OPTN/UNOS) Database. Am. J. Kidney Dis. 2010, 56, 1127–1139. [Google Scholar] [CrossRef]
- Held, P.J.; Kahan, B.D.; Hunsicker, L.G.; Liska, D.; Wolfe, R.A.; Port, F.K.; Gaylin, D.S.; García, J.R.; Agodoa, L.; Krakauer, H. The Impact of HLA Mismatches on the Survival of First Cadaveric Kidney Transplants. N. Engl. J. Med. 1994, 331, 765–770. [Google Scholar] [CrossRef]


| ∑ (n = 105) | ICU Yes (n = 17) | ICU No (n = 88) | p | |
|---|---|---|---|---|
| Recipient | ||||
| age (year) | 69 (65; 82) | 71 (65; 80) | 69 (65; 82) | n.s. |
| male gender | 68 (64.8%) | 10 (58.8%) | 58 (65.9%) | n.s. |
| BMI (kg/m2) | 26.3 (19.2; 37.9) | 24.2 (19.3; 31) | 26.7 (19.2; 37.9) | 0.014 |
| Pre-transplant | ||||
| hypertension | 101 (96.2%) | 17 (100%) | 84 (95.5%) | n.s. |
| CAD | 42 (40%) | 11 (64.7%) | 31 (35.2%) | 0.031 |
| diabetes | 41 (39%) | 6 (35.3%) | 35 (39.8%) | n.s. |
| history of smoking | 18 (17.1%) | 2 (11.8%) | 16 (18.2%) | n.s. |
| Cause for ESKD | ||||
| chronic GN | 23 (18.9%) | 1 (5.9%) | 22 (25%) | n.s. |
| diabetic NP | 17 (13.9%) | 2 (11.8%) | 15 (17%) | n.s. |
| hypertensive NP | 15 (12.3%) | 6 (35.3%) | 9 (10.2%) | 0.015 |
| other * | 50 (47.6%) | 9 (52.9%) | 46 (52.2%) | n.s. |
| time on dialysis (d) | 918.5 (2; 3830) | 1384 (484; 3830) | 855.5 (12; 3302) | n.s. |
| hemodialysis | 84 (80%) | 16 (94.1%) | 68 (77.3%) | n.s. |
| first Tx | 101 (96.2%) | 17 (100%) | 84 (95.5%) | n.s. |
| Graft | ||||
| donor age (year) | 71 (65; 85) | 71 (66; 82) | 71 (65; 85) | n.s. |
| HLA-mismatches | 4 (1; 6) | 4 (1; 6) | 4 (1; 6) | n.s. |
| CIT (min) | 571.8 (181.2; 1236) | 667.8 (228; 1166.4) | 552.3 (181.2; 1236) | 0.053 |
| ∑ (n = 105) | ICU Yes (n = 17) | ICU No (n = 88) | p-Value | |
|---|---|---|---|---|
| Transplantation | ||||
| operating time (min) | 184 (116; 436) | 212 (129; 268) | 180 (116; 436) | n.s. |
| WIT (min) | 46.5 (21; 126) | 47 (35; 70) | 46 (21; 126) | n.s. |
| complications | 12 (11.4%) | 2 (11.8%) | 10 (11.4%) | n.s. |
| Postoperative | ||||
| complications | n.s. | |||
| none | 42 (40%) | 5 (29.4%) | 37 (42%) | n.s. |
| minor | 28 (26.7%) | 3 (17.6%) | 25 (28.4%) | n.s. |
| major | 35 (33.3%) | 9 (52.9%) | 26 (29.5%) | n.s. |
| length of stay | 19 (8–66) | 21.5 (12–66) | 18 (8–62) | n.s. |
| Graft Function | ||||
| DGF rate | 42 (40%) | 9 (52.9%) | 33 (37.5%) | n.s. |
| Donors: Very Old-For-Old vs. Old-For-Old | Recipients: Old-For-Very Old vs. Old-For-Old | |||||
|---|---|---|---|---|---|---|
| Very Old (n = 28) | Old (n = 77) | p | Very Old (n = 47) | Old (n = 58) | p | |
| Transplantation | ||||||
| operating time | 180 (120; 281) | 188 (116; 436) | n.s. | 190 (128; 268) | 181 (116; 436) | n.s. |
| WIT (min) | 46 (21; 126) | 49.5 (32; 85) | n.s. | 48 (32; 104) | 46 (21; 126) | n.s. |
| complications | 4 (14.3%) | 8 (10.4%) | n.s. | 6 (12.8%) | 6 (10.3%) | n.s. |
| Postoperative | ||||||
| ICU admission | 6 (21.4%) | 11 (14.3%) | n.s. | 10 (21.3%) | 7 (12.1%) | n.s. |
| Clavien–Dindo | n.s. | n.s. | ||||
| none | 13 (46.4%) | 29 (37.7%) | 16 (34%) | 26 (44.8%) | ||
| minor | 10 (35.7%) | 18 (23.4%) | 13 (27.7%) | 15 (25.9%) | ||
| major | 5 (17.9%) | 30 (39%) | 18 (38.3%) | 17 (29.3%) | ||
| length of stay | 16 (12; 46) | 20 (8; 66) | 0.028 | 20 (10; 66) | 18.5 (8; 65) | |
| Graft Function | ||||||
| DGF | 14 (50%) | 28 (36.4%) | n.s. | 19 (40.4%) | 23 (39.7%) | n.s. |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| BMI | 0.80 (0.68; 0.94) | 0.008 |
| hypertensive nephropathy | 4 (1.02; 15.67) | 0.046 |
| coronary artery disease | 4.46 (1.32; 15.07) | 0.016 |
| Variable | HR (95% CI) | p-Value |
|---|---|---|
| Graft Loss | ||
| number of Tx | 9.66 (2.48; 37.69) | 0.001 |
| HLA-mismatches | 1.53 (1.03; 2.27) | 0.033 |
| serum creatinine 1 mo | 1.37 (1.01; 1.87) | 0.04 |
| Patient Death | ||
| pre-transplant diabetes | 2.22 (1.02; 4.86) | 0.046 |
| ICU admission | 4.72 (2.02; 11.03) | <0.001 |
| Frei [19] n = 1406 | Quast [20] n = 217 | Bahde [23] n = 89 | Jacobi [21] n = 89 | Our Results n = 105 | |
|---|---|---|---|---|---|
| Graft Survival | |||||
| 1-year | 75% | 76.4% 1 | n.a. | 87% | 84% |
| 5-year | 47% | 57.3% 1 | 77% | 63% | 73% |
| Patient Survival | |||||
| 1-year | 86% | 88.2% 1 | n.a. | 87% | 85% |
| 5-year | 60% | 71.8% 1 | 69.8% | 63% | 62% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeuschner, P.; Sester, U.; Stöckle, M.; Saar, M.; Zompolas, I.; El-Bandar, N.; Liefeldt, L.; Budde, K.; Öllinger, R.; Ritschl, P.; et al. Should We Perform Old-For-Old Kidney Transplantation during the COVID-19 Pandemic? The Risk for Post-Operative Intensive Stay. J. Clin. Med. 2020, 9, 1835. https://doi.org/10.3390/jcm9061835
Zeuschner P, Sester U, Stöckle M, Saar M, Zompolas I, El-Bandar N, Liefeldt L, Budde K, Öllinger R, Ritschl P, et al. Should We Perform Old-For-Old Kidney Transplantation during the COVID-19 Pandemic? The Risk for Post-Operative Intensive Stay. Journal of Clinical Medicine. 2020; 9(6):1835. https://doi.org/10.3390/jcm9061835
Chicago/Turabian StyleZeuschner, Philip, Urban Sester, Michael Stöckle, Matthias Saar, Ilias Zompolas, Nasrin El-Bandar, Lutz Liefeldt, Klemens Budde, Robert Öllinger, Paul Ritschl, and et al. 2020. "Should We Perform Old-For-Old Kidney Transplantation during the COVID-19 Pandemic? The Risk for Post-Operative Intensive Stay" Journal of Clinical Medicine 9, no. 6: 1835. https://doi.org/10.3390/jcm9061835