Post-Laser Twin Anemia Polycythemia Sequence: Diagnosis, Management, and Outcome in an International Cohort of 164 Cases

 , , , , , , , , , , , ,
, , , , , , , , , , , ,
Abstract
:1. Introduction
2. Experimental Section
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Center | Country | Post-Laser TAPS Cases |
|---|---|---|
| Leiden University Medical Center | The Netherlands | 66 |
| Children’s Hospital V. Buzzi Milan | Italy | 17 |
| Necker-Enfants Malades Hospital Paris | France | 16 |
| Leuven University Hospital | Belgium | 13 |
| Center Medico-Chirurgical Obstetrical Strasbourg | France | 10 |
| Mount Sinai Hospital Toronto | Canada | 10 |
| Saint George’s Hospital London | United Kingdom | 5 |
| Birmingham Women’s and Children’s NHS Foundation Trust | United Kingdom | 5 |
| Medical University of Graz | Austria | 3 |
| Mater Hospital Brisbane | Australia | 4 |
| University of Texas McGovern Medical School at Houston | United States of America | 4 |
| V.I. Kulakov National Medical Research Center of Obstetrics, Gynecology and Perinatology Moscow | Russia | 4 |
| Karolinska University Hospital Stockholm | Sweden | 3 |
| Hospital Universitari Vall d’Hebron Barcelona | Spain | 2 |
| Brugmann University Hospital | Belgium | 1 |
| University Medical Center Hamburg-Eppendorf | Germany | 1 |
Appendix B
| Death † (n = 60/304) | Alive † (n = 244/304) | Univariate Analysis OR (95% CI) | SE | p | Multivariate Analysis OR (95% CI) | SE | p | |
|---|---|---|---|---|---|---|---|---|
| GA at diagnosis TAPS | 23.3 ± 3.3 | 23.7 ± 3.7 | 1.0 (0.9–1.1) | 0.1 | 0.623 | |||
| GA at laser TTTS | 20.1 ± 2.4 | 20.8 ± 3.3 | 0.9 (0.8–1.0) | 0.1 | 0.233 | |||
| Days between TTTS laser and TAPS | 20.9 ± 18.4 | 21.8 ± 23.1 | 1.0 (1.0–1.0) | 0.0 | 0.829 | |||
| Quintero stage for TTTS ‡ | ||||||||
| 1 | 3/35 (9) | 32/35 (91) | - * | - * | ||||
| 2 | 27/140 (19) | 113/140 (81) | 2.5 (0.7–8.5) | 0.6 | 0.139 | 1.7 (0.4–6.9) | 0.7 | 0.439 |
| 3 | 27/111 (24) | 84/111(76) | 3.6 (1.1–12.0) | 0.6 | 0.039 | 3.5 (0.9–13.2) | 0.7 | 0.069 |
| 4 | 2/10 (20) | 8/10 (80) | 2.8 (0.2–32.4) | 1.3 | 0.418 | 3.4 (0.3–33.6) | 1.2 | 0.298 |
| Antenatal TAPS stage | ||||||||
| 1 | 6/47 (13) | 41/47 (87) | - * | - * | ||||
| 2 | 12/122 (10) | 110/122 (90) | 0.9 (0.3–3.2) | 0.6 | 0.864 | 0.8 (0.2–3.2) | 0.7 | 0.790 |
| 3 | 14/56 (25) | 50/56 (75) | 2.6 (0.7–9.1) | 0.6 | 0.136 | 2.6 (0.6–10.3) | 0.7 | 0.182 |
| 4 | 20/46 (44) | 26/46 (55) | 6.1 (1.8–20.4) | 0.6 | 0.003 | 6.1 (1.4–26.0) | 0.7 | 0.015 |
| TAPS recipient | 17/158 (11) | 146/158 (89) | - * | - * | ||||
| TAPS donor | 43/146 (30) | 103/146 (70) | 3.7 (2.2–6.3) | 0.3 | <0.001 | 4.2 (2.1–8.3) | 0.3 | <0.001 |
| Persistence of TTTS-TAPS donor-role, no § | 25/162 (15) | 137/162 (85) | - * | |||||
| Persistence of TTTS-TAPS donor-role, yes § | 34/137 (25) | 103/137 (77) | 1.8 (1.0–3.5) | 0.3 | 0.061 | |||
| Antenatal therapy | ||||||||
| Expectant management | 27/124 (22) | 97/124 (78) | - * | |||||
| Delivery | 4/18 (22) | 14/18 (78) | 1.4 (0.3–4.2) | 0.6 | 0.622 | |||
| IUT (± PET) | 16/81 (20) | 72/81 (82) | 0.9 (0.4–1.9) | 0.4 | 0.893 | |||
| Laser surgery | 9/44 (21) | 38/44 (79) | 1.0 (0.3–2.8) | 0.5 | 0.942 | |||
| Selective feticide (co-twin) | 0/11 (0) | 11/11 (100) | 0.3 (0.0–2.9) | 1.1 | 0.330 | |||
| GA at birth | 29.5 ± 5.0 | 31.6 ± 3.1 | 0.8 (0.7–1.0) | 0.1 | 0.006 | 0.8 (0.7–0.9) | 0.1 | 0.001 |
| SNM † (139/429) | No SNM † (290/429) | Univariate Analysis OR (95% CI) | SE | p | Multivariate Analysis OR (95% CI) | SE | p | |
|---|---|---|---|---|---|---|---|---|
| GA at diagnosis TAPS | 24.5 ± 3.1 | 23.4 ± 4.0 | 0.9 (0.8–1.0) | 0.1 | 0.090 | |||
| GA at laser TTTS | 21.1 ± 2.6 | 20.6 ± 3.6 | 0.9 (0.8–1.0) | 0.1 | 0.261 | |||
| Days between TTTS laser and TAPS | 22.3 ± 21.9 | 22.1 ± 23.9 | 1.0 (1.0–1.0) | 0.0 | 0.987 | |||
| Quintero stage for TTTS | ||||||||
| 1 | 8/34 (24) | 26/34 (76) | - * | - * | ||||
| 2 | 64/123 (52) | 59/123 (48) | 3.2 (1.1–9.7) | 0.6 | 0.038 | 2.8 (0.9–9.0) | 0.6 | 0.066 |
| 3 | 28/89 (32) | 61/89 (68) | 1.3 (0.4–4.2) | 0.6 | 0.617 | 1.3 (0.4–3.9) | 0.6 | 0.690 |
| 4 | 3/10 (30) | 3/10 (70) | 1.3 (0.2–9.3) | 1.0 | 0.782 | 1.1 (0.1–10.0) | 1.1 | 0.959 |
| Antenatal TAPS stage | ||||||||
| 1 | 18/45 (40) | 30/45 (60) | - * | |||||
| 2 | 41/112 (37) | 71/112 (63) | 1.0 (0.4–2.5) | 0.5 | 0.970 | |||
| 3 | 16/45 (36) | 29/45 (64) | 0.7 (0.2–2.2) | 0.6 | 0.570 | |||
| 4 | 17/32 (53) | 15/32 (47) | 1.6 (0.5–5.0) | 0.6 | 0.381 | |||
| TAPS recipient | 54/145(37) | 91/145 (63) | - * | |||||
| TAPS donor | 51/118 (43) | 67/118 (57) | 1.1 (0.8–1.5) | 0.2 | 0.568 | |||
| Persistence of TTTS-TAPS donor-role, no | 47/139 (34) | 92/139 (66) | - * | |||||
| Persistence of TTTS-TAPS donor-role, yes | 58/120 (48) | 62/120 (52) | 1.6 (0.9–3.0) | 0.3 | 0.116 | |||
| Antenatal therapy | ||||||||
| Expectant management | 34/100 (34) | 66/100 (66) | - * | |||||
| Delivery | 9/17 (53) | 8/17 (47) | 2.1 (0.6–8.1) | 0.7 | 0.270 | |||
| IUT (± PET) | 34/72 (47) | 38/72 (53) | 1.7 (0.8–3.7) | 0.4 | 0.158 | |||
| Laser surgery | 12/37 (32) | 25/37 (68) | 1.1 (0.4–2.9) | 0.5 | 0.851 | |||
| Selective feticide | 3/11 (27) | 8/11 (73) | 0.7 (0.2–3.2) | 0.7 | 0.720 | |||
| GA at birth | 29.4 ± 2.6 | 32.9 ± 2.8 | 1.5 (1.3–1.7) | 0.1 | <0.001 | 1.5 (1.3–1.7) | 0.1 | <0.001 |
| Severe growth restriction, no | 81/200 (41) | 119/200 (60) | - * | |||||
| Severe growth restriction, yes | 24/62 (39) | 38/62 (61) | 1.3 (0.8–2.2) | 0.3 | 0.351 | |||
| Postnatal TAPS, no | 23/58 (40) | 35/58 (60) | - * | |||||
| Postnatal TAPS, yes | 64/151 (42) | 87/151(58) | 1.1 (0.5–2.5) | 0.4 | 0.800 |
References
- Lopriore, E.; Middeldorp, J.M.; Oepkes, D.; Kanhai, H.H.; Walter, F.J.; Vandenbussche, F.P. Twin anemia-polycythemia sequence in two monochorionic twin pairs without oligo-polyhydramnios sequence. Placenta 2007, 28, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Slaghekke, F.; Lopriore, E.; Lewi, L.; Middeldorp, J.M.; van Zwet, E.W.; Weingertner, A.S.; Klumper, F.J.; Dekoninck, P.; Devlieger, R.; Kilby, M.D.; et al. Fetoscopic laser coagulation of the vascular equator versus selective coagulation for twin-to-twin transfusion syndrome: An open-label randomised controlled trial. Lancet 2014, 383, 2144–2151. [Google Scholar] [CrossRef]
- Lewi, L.; Jani, J.; Blickstein, I.; Huber, A.; Gucciardo, L.; Van Mieghem, T.; Done, E.; Boes, A.S.; Hecher, K.; Gratacos, E.; et al. The outcome of monochorionic diamniotic twin gestations in the era of invasive fetal therapy: A prospective cohort study. Am. J. Obstet. Gynecol. 2008, 199, 514. [Google Scholar] [CrossRef] [PubMed]
- Lewi, L.; Jani, J.; Cannie, M.; Robyr, R.; Ville, Y.; Hecker, K.; Gratacos, E.; Vandecruys, H.; Vandecaveye, V.; Dymarkowski, S.; et al. Intertwin anastomoses in monochorionic placentas after fetoscopic laser coagulation for twin-to-twin transfusion syndrome: Is there more than meets the eye? Am. J. Obstet. Gynecol. 2006, 194, 790–795. [Google Scholar] [CrossRef]
- Knijnenburg, P.J.C.; Slaghekke, F.; Tollenaar, L.S.A.; van Klink, J.M.; Zhao, D.P.; Middeldorp, J.M.; Haak, M.C.; Klumper, F.J.; Oepkes, D.; Lopriore, E. Incidence of and Risk Factors for Residual Anastomoses in Twin-Twin Transfusion Syndrome Treated with Laser Surgery: A 15-Year Single-Center Experience. Fetal. Diagn. Ther. 2019, 45, 13–20. [Google Scholar] [CrossRef]
- Slaghekke, F.; Lewi, L.; Middeldorp, J.M.; Weingertner, A.S.; Klumper, F.J.; Dekoninck, P.; Devlieger, R.; Lanna, M.M.; Deprest, J.; Favre, R.; et al. Residual anastomoses in twin-twin transfusion syndrome after laser: The Solomon randomized trial. Am. J. Obstet. Gynecol. 2014, 211, 285 e1–285 e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tollenaar, L.S.; Slaghekke, F.; Middeldorp, J.M.; Klumper, F.J.; Haak, M.C.; Oepkes, D.; Lopriore, E. Twin Anemia Polycythemia Sequence: Current Views on Pathogenesis, Diagnostic Criteria, Perinatal Management, and Outcome. Twin Res. Hum. Genet. 2016, 19, 222–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tollenaar, L.S.A.; Slaghekke, F.; Lewi, L.; Colmant, C.; Lanna, M.M.; Weingertner, A.S.; Ryan, G.; Arevalo, S.; Tavares de Sousa, M. Spontaneous Twin Anemia Polycythemia Sequence: Management and Outcome in a Large International Cohort of 249 Cases. Submitted.
- Slaghekke, F.; Pasman, S.; Veujoz, M.; Middeldorp, J.M.; Lewi, L.; Devlieger, R.; Favra, R.; Lopriore, E.; Oepkes, D. Middle cerebral artery peak systolic velocity to predict fetal hemoglobin levels in twin anemia-polycythemia sequence. Ultrasound Obstet. Gynecol. 2015, 46, 432–436. [Google Scholar] [CrossRef] [Green Version]
- Lopriore, E.; Slaghekke, F.; Oepkes, D.; Middeldorp, J.M.; Vandenbussche, F.P.; Walther, F.J. Hematological characteristics in neonates with twin anemia-polycythemia sequence (TAPS). Prenat. Diagn. 2010, 30, 251–255. [Google Scholar]
- Lopriore, E.; Slaghekke, F.; Middeldorp, J.M.; Klumper, F.J.; Van Lith, J.M.; Walther, F.J.; Oepkes, D. Accurate and simple evaluation of vascular anastomoses in monochorionic placentas using colored dye. J. Vis. Exp. 2011, 55, e3208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trieu, N.T.; Weingertner, A.S.; Guerra, F.; Dautun, D.; Kohler, M.; Vayssiere, C.; Nisand, I.; Favre, R. Evaluation of the measurement of the middle cerebral artery peak systolic velocity before and after placental laser coagulation in twin-to-twin transfusion syndrome. Prenat. Diagn. 2012, 32, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Slaghekke, F.; Kist, W.J.; Oepkes, D.; Pasman, S.A.; Middeldorp, J.M.; Klumper, F.J.; Walther, F.J.; Vandenbussche, F.P.; Lopriore, E. Twin anemia-polycythemia sequence: Diagnostic criteria, classification, perinatal management and outcome. Fetal Diagn. Ther. 2010, 27, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.J.; Ternberg, J.L.; Feigin, R.D.; Keating, J.P.; Marshall, R.; Barton, L.; Brotherton, T.; Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann. Surg. 1978, 187, 1–7. [Google Scholar] [CrossRef] [PubMed]
- An international classification of retinopathy of prematurity. The Committee for the Classification of Retinopathy of Prematurity. Arch. Ophthalmol. 1984, 74, 127–133. [Google Scholar]
- Volpe, J.J. Intraventricular hemorrhage and brain injury in the premature infant. Diagn. Progn. Prev. Clin. Perinatol. 1989, 16, 387–411. [Google Scholar] [CrossRef]
- Levene, M.I. Measurement of the growth of the lateral ventricles in preterm infants with real-time ultrasound. Arch. Dis. Child. 1981, 56, 900–904. [Google Scholar] [CrossRef] [Green Version]
- De Vries, L.S.; Eken, P.; Dubowitz, L.M. The spectrum of leukomalacia using cranial ultrasound. Behav. Brain Res. 1992, 49, 1–6. [Google Scholar] [CrossRef]
- Hoftiezer, L.; Hof, M.H.P.; Dijs-Elsinga, J.; Hogeveen, M.; Hukkelhoven, C.; van Lingen, R.A. From population reference to national standard: New and improved birthweight charts. Am. J. Obstet. Gynecol. 2019, 220, 383. [Google Scholar] [CrossRef]
- Lopriore, E.; Hecher, K.; Vandenbussche, F.P.; van den Wijngaard, J.P.; Klumper, F.J.; Oepkes, D. Fetoscopic laser treatment of twin-to-twin transfusion syndrome followed by severe twin anemia-polycythemia sequence with spontaneous resolution. Am. J. Obstet. Gynecol. 2008, 198, e4–e7. [Google Scholar] [CrossRef]
- Khalil, A.; Rodgers, M.; Baschat, A.; Bhide, A.; Gratacos, E.; Hecher, K.; Kilby, M.D.; Lewi, L.; Nicolaides, K.H.; Oepkes, D.; et al. ISUOG Practice Guidelines: Role of ultrasound in twin pregnancy. Ultrasound Obstet. Gynecol. 2016, 47, 247–263. [Google Scholar]
- Slaghekke, F.; van Klink, J.M.; Koopman, H.M.; Middeldorp, J.M.; Oepkes, D.; Lopriore, E. Neurodevelopmental outcome in twin anemia-polycythemia sequence after laser surgery for twin-twin transfusion syndrome. Ultrasound Obstet. Gynecol. 2014, 44, 316–321. [Google Scholar] [CrossRef]
- Senat, M.V.; Deprest, J.; Boulvain, M.; Paupe, A.; Winer, N.; Ville, Y. Endoscopic laser surgery versus serial amnioreduction for severe twin-to-twin transfusion syndrome. N. Engl. J Med. 2004, 351, 136–144. [Google Scholar] [CrossRef]
- De, Villiers, S.F.; Slaghekke, F.; Middeldorp, J.M.; Walther, F.J.; Oepkes, D.; Lopriore, E. Placental characteristics in monochorionic twins with spontaneous versus post-laser twin anemia-polycythemia sequence. Placenta 2013, 34, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Lopriore, E.; Oepkes, D.; van den Wijngaard, J.P.; van Gemert, M.J.; Middeldorp, J.M.; Vandenbussche, F.P. Twin anemia-polycythemia sequence (TAPS) without a cause. Prenat. Diagn. 2008, 28, 559–560. [Google Scholar] [CrossRef] [PubMed]
- Tollenaar, L.S.A.; Slaghekke, F.; Lewi, L.; Ville, Y.; Lanna, M.; Weingertner, A.; Ryan, G.; Arevalo, S.; Khalil, A.; Brock, C.O.; et al. Treatment and outcome in 370 cases with spontaneous or post-laser twin anemia polycythemia sequence managed in 17 different fetal therapy centers. Ultrasound Obstet. Gynecol. 2020. [Google Scholar] [CrossRef]

| Post-Laser TAPS (N = 164 Pregnancies, 328 Fetuses) | |
|---|---|
| Gravidity | 2 (1–3) |
| Parity | 0 (0–1) |
| Antenatal diagnosis of TAPS | 151/164 (92) |
| Location of placenta | |
| Anterior | 72/164 (44) |
| Posterior | 86/164 (52) |
| Other † | 6/164 (4) |
| TTTS stage ‡ | |
| Q1 | 20/159 (13) |
| Q2 | 75/159 (47) |
| Q3 | 59/159 (37) |
| Q4 | 5/159 (3) |
| Solomon technique for TTTS laser | 60/164 (37) |
| GA at laser for TTTS | 20.6 (18.0–23.0) |
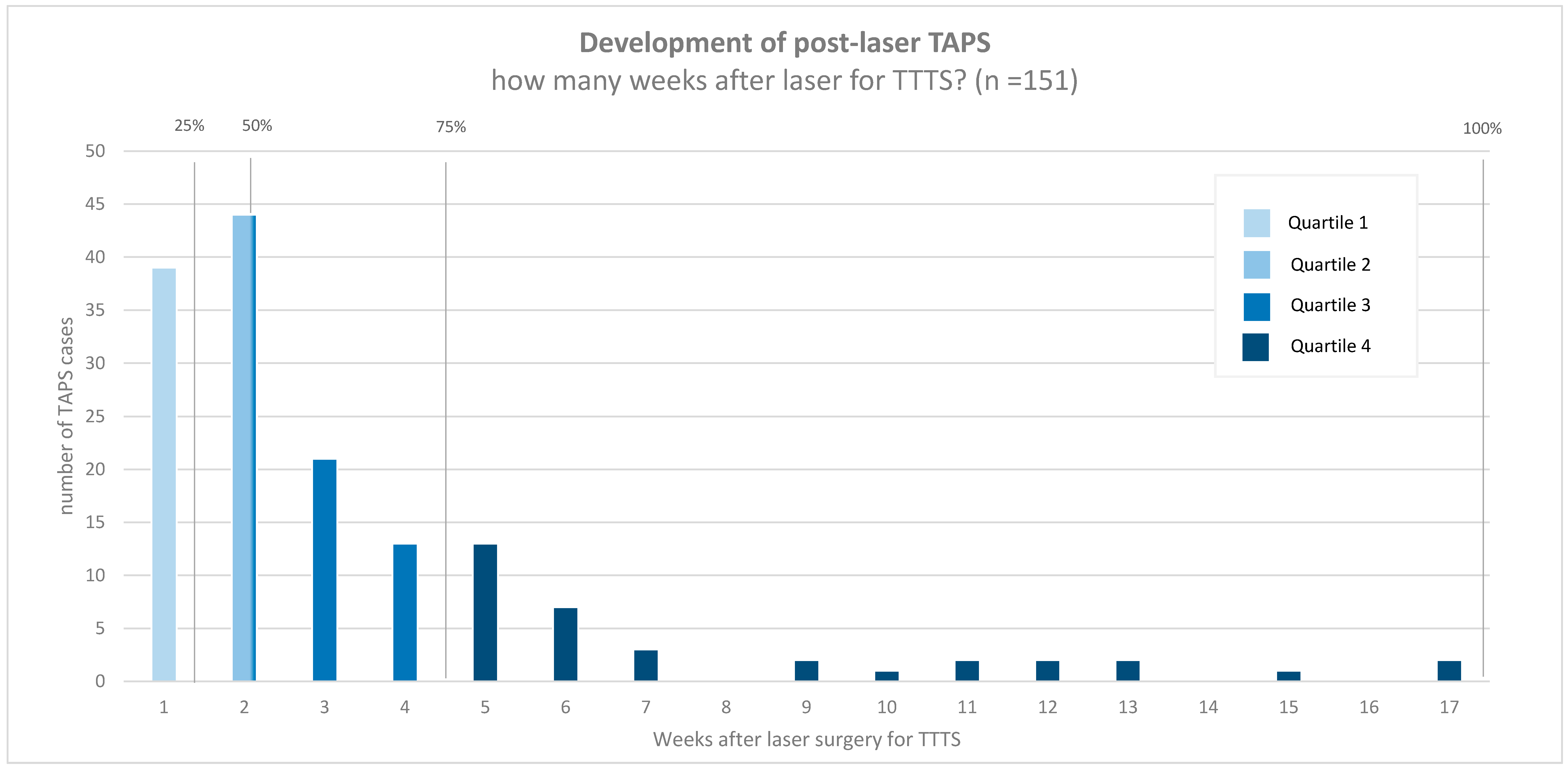
| Time between laser and post-laser TAPS (days) | 14 (7–28) |
| Persistence of TTTS-TAPS donor-recipient role § | 73/161 (45) |
| Laser for TTTS complete (surgeon’s opinion) ¶ | 126/156 (81) |
| Post-Laser TAPS (N = 164 Pregnancies, 328 Fetuses) | |
|---|---|
| GA at diagnosis | 23.1 (20.4–25.9) |
| TAPS stage at diagnosis | |
| 1 | 43/151 (28) |
| 2 | 69/151 (48) |
| 3 | 27/151 (17) |
| 4 | 12/151 (8) |
| Highest TAPS stage | |
| 1 | 22/151 (15) |
| 2 | 62/151(40) |
| 3 | 26/151 (16) |
| 4 | 22/151 (14) |
| 5 | 19/151 (15) |
| Presence of additional ultrasound markers † | |
| Starry-sky liver (recipient) | 56/141 (40) |
| Difference in placental echogenicity | 35/151 (23) |
| Antenatal management | |
| Expectant management | 62/151 (43) |
| Delivery | 9/151 (6) |
| IUT (± PET) | 44/151 (29) |
| Laser surgery | 24/151 (15) |
| Selective feticide | 11/151 (7) |
| Termination of pregnancy | 1/151 (1) |
| Female ‡ | 162/308 (53) |
| Cesarean § | 206/326 (63) |
| Injected Post-Laser TAPS Placentas (N = 74) | |
|---|---|
| Total number of anastomoses | 1 (1–2) |
| Number of AV anastomoses | 1 (0–1) |
| Number of VA anastomoses | 0 (0–1) |
| Number of AA anastomoses | 0 (0–0) |
| Number of VV anastomoses | 0 (0–0) |
| Presence of anastomoses | |
| Presence of AV/VA anastomoses | 58/74 (80) |
| Presence of AA anastomoses | 6/74 (8) |
| Presence of VV anastomoses | 5/74 (7) |
| Type of anastomoses per placenta | |
| No anastomoses | 10/74 (14) |
| AV (one direction) | 40/74 (54) |
| AVs (both directions) | 14/74 (19) |
| AV/VA and AA | 3/74 (4) |
| AV/VA and VV | 2/74 (3) |
| Only AA | 2/74 (3) |
| Only VV | 2/74 (3) |
| AV/VA, AA and VV | 1/74 (1) |
| All anastomoses diameter < 1 mm | 62/64 (97) |
| Post-Laser TAPS (N = 164 Pregnancies; 328 Fetuses) | TAPS Donors (N = 164 Fetuses) | TAPS Recipients (N = 164 Fetuses) † | p-Value | |
|---|---|---|---|---|
| GA at birth | 31.7 (28.6–33.7; 19.0–41.3) | |||
| Fetal demise † | 56/327 (17) | 43/164 (26) | 13/163 (8) | <0.001 |
| Spontaneous | 33/327 (10) | 25/164 (15) | 8/163 (5) | <0.001 |
| Intended | 23/327 (7) | 18/164 (11) | 5/163 (3) | 0.007 |
| Neonatal mortality | 27/271 (10) | 18/121 (15) | 9/150 (6) | 0.008 |
| Perinatal mortality (overall) † | 83/327 (25) | 61/164 (37) | 22/163 (14) | <0.001 |
| Perinatal mortality (spontaneous) † | 60/327 (18) | 43/164 (26) | 17/163 (10) | <0.001 |
| Severe neonatal morbidity ‡ | 105/263 (40) | 51/118 (43) | 54/145 (37) | 0.568 |
| Respiratory distress syndrome | 88/263(34) | 42/118 (36) | 46/145 (32) | 0.945 |
| Patent ductus arteriosus | 20/263 (8) | 11/118 (9) | 9/145 (6) | 0.278 |
| Necrotizing enterocolitis | 6/263 (2) | 4/118 (3) | 2/145 (1) | 0.275 |
| Retinopathy of prematurity | 9/263 (3) | 6/118 (5) | 3/145 (2) | 0.165 |
| Amniotic band syndrome | 3/263 (1) | 2/118 (2) | 1/145 (1) | 0.451 |
| Severe cerebral injury | 28/263 (11) | 13/118 (11) | 15/145 (10) | 0.916 |
| Birth weight (g) § | 1390 ± 567 | 1346 ± 525 | 1533 ± 588 | <0.001 |
| Severe growth restriction (bw < p3) § | 62/270 (23) | 31/121 (26) | 31/149 (21) | 0.267 |
| Mild growth restriction (bw < p10) § | 122/270 (45) | 60/121 (50) | 61/149 (41) | 0.061 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tollenaar, L.S.A.; Lopriore, E.; Faiola, S.; Lanna, M.; Stirnemann, J.; Ville, Y.; Lewi, L.; Devlieger, R.; Weingertner, A.S.; Favre, R.; et al. Post-Laser Twin Anemia Polycythemia Sequence: Diagnosis, Management, and Outcome in an International Cohort of 164 Cases. J. Clin. Med. 2020, 9, 1759. https://doi.org/10.3390/jcm9061759
Tollenaar LSA, Lopriore E, Faiola S, Lanna M, Stirnemann J, Ville Y, Lewi L, Devlieger R, Weingertner AS, Favre R, et al. Post-Laser Twin Anemia Polycythemia Sequence: Diagnosis, Management, and Outcome in an International Cohort of 164 Cases. Journal of Clinical Medicine. 2020; 9(6):1759. https://doi.org/10.3390/jcm9061759
Chicago/Turabian StyleTollenaar, Lisanne S.A., Enrico Lopriore, Stefano Faiola, Mariano Lanna, Julien Stirnemann, Yves Ville, Liesbeth Lewi, Roland Devlieger, Anne Sophie Weingertner, Romain Favre, and et al. 2020. "Post-Laser Twin Anemia Polycythemia Sequence: Diagnosis, Management, and Outcome in an International Cohort of 164 Cases" Journal of Clinical Medicine 9, no. 6: 1759. https://doi.org/10.3390/jcm9061759