Middle Cerebral Artery Doppler Velocimetry for the Diagnosis of Twin Anemia Polycythemia Sequence: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Robyr, R.; Lewi, L.; Salomon, L.J.; Yamamoto, M.; Bernard, J.P.; Deprest, J.; Ville, Y. Prevalence and management of late fetal complications following successful selective laser coagulation of chorionic plate anastomoses in twin-to-twin transfusion syndrome. Am. J. Obstet. Gynecol. 2006, 194, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Yokouchi, T.; Murakoshi, T.; Mishima, T.; Yano, H.; Ohashi, M.; Suzuki, T.; Shinno, T.; Matsushita, M.; Nakayama, S.; Torii, Y. Incidence of spontaneous twin anemia-polycythemia sequence in monochorionic-diamniotic twin pregnancies: Single-center prospective study. J. Obstet. Gynaecol. Res. 2015, 41, 857–860. [Google Scholar] [CrossRef] [Green Version]
- Gucciardo, L.; Lewi, L.; Vaast, P.; Debska, M.; De Catte, L.; Van Meighem, T.; Doné, E.; Devlieger, R.; Deprest, J. Twin anemia polycythemia sequence from a prenatal perspective. Prenat. Diagn. 2010, 30, 438–442. [Google Scholar] [CrossRef]
- Lopriore, E.; Deprest, J.; Slaghekke, F.; Oepkes, D.; Middeldorp, J.M.; Vandenbussche, F.P.H.A.; Lewi, L. Placental characteristics in monochorionic twins with and without twin anemia-polycythemia sequence. Obstet. Gynecol. 2008, 112, 753–758. [Google Scholar] [CrossRef]
- Tavares de Sousa, M.; Fonseca, A.; Hecher, K. Role of fetal intertwin difference in middle cerebral artery peak systolic velocity in predicting neonatal twin anemia-polycythemia sequence. Ultrasound Obstet. Gynecol. 2019, 53, 794–797. [Google Scholar] [CrossRef]
- Lewi, L.; Jani, J.; Blickstein, I.; Huber, A.; Gucciardo, L.; Van Mieghem, T.; Doné, E.; Boes, A.S.; Hecher, K.; Gratacós, E.; et al. The outcome of monochorionic diamniotic twin gestations in the era of invasive fetal therapy: A prospective cohort study. Am. J. Obstet. Gynecol. 2008, 199, 514.e1–514.e8. [Google Scholar] [CrossRef]
- de Villiers, S.F.; Slaghekke, F.; Middeldorp, J.M.; Walther, F.J.; Oepkes, D.; Lopriore, E. Placental characteristics in monochorionic twins with spontaneous versus post-laser twin anemia-polycythemia sequence. Placenta 2013, 34, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Lopriore, E.; Middeldorp, J.M.; Oepkes, D.; Kanhai, H.H.; Walther, F.J.; Vandenbussche, F.P. Twin anemia-polycythemia sequence in two monochorionic twin pairs without oligo-polyhydramnios sequence. Placenta 2007, 28, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Veujoz, M.; Sananès, N.; Severac, F.; Meyer, N.; Weingertner, A.S.; Kohler, M.; Guerra, F.; Gaudineau, A.; Nisand, I.; Favre, R. Evaluation of prenatal and postnatal diagnostic criteria for twin anemia-polycythemia sequence. Prenat. Diagn. 2015, 35, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Tollenaar, L.S.A.; Lopriore, E.; Middeldorp, J.M.; Haak, M.C.; Klumper, F.J.; Oepkes, D; Slaghekke, F. Improved prediction of twin anemia-polycythemia sequence by delta middle cerebral artery peak systolic velocity: New antenatal classification system. Ultrasound Obstet. Gynecol. 2019, 53, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Slaghekke, F.; Favre, R.; Peeters, S.H.; Middeldorp, J.M.; Weingertner, A.S.; van Zwet, E.W.; Klumper, F.J.; Oepkes, D.; Lopriore, E. Laser surgery as a management option for twin anemia-polycythemia sequence. Ultrasound Obstet. Gynecol. 2014, 44, 304–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, A.; Gordijn, S.; Ganzevoort, W.; Thilganathan, B.; Johnson, A.; Baschat, A.; Hecher, K.; Reed, K.; Lewi, L.; Deprest, J.; et al. Consensus diagnostic criteria and monitoring of twin anemia polycythemia sequence: A Delphi procedure. Ultrasound Obstet. Gynecol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Khalil, A.; Rodgers, M.; Baschat, A.; Bhide, A.; Gratacós, E.; Hccker, K.; Kilby, M.D.; Lewi, L.; Nicolaides, K.H.; Oepkes, D.; et al. ISUOG Practice Guidelines: Role of ultrasound in twin pregnancy. Ultrasound Obstet. Gynecol. 2016, 47, 247–263. [Google Scholar] [CrossRef] [Green Version]
- Simpson, L.L. Twin-twin transfusion syndrome. Am. J. Obstet. Gynecol. 2013, 208, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Netherlands Trial. Register. Trial NL6879 (NTR7057). The TAPS Trial: Fetoscopic Laser Surgery for Twin Anemia Polycythemia. Sequence—A Multicenter Open-Label Randomized. Controlled Trial. Available online: https://www.trialregister.nl/trial/6879 (accessed on 3 June 2020).
- Nicholas, L.; Fischbein, R.; Aultman, J.; Ernst-Milner, S. Dispelling Myths about Antenatal TAPS: A Call for Action for Routine MCA-PSV Doppler Screening in the United States. J. Clin. Med. 2019, 8, 977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ACOG Practice Bulletin, No. 192: Management of Alloimmunization During Pregnancy. Obstet. Gynecol. 2018, 131, e82–e90. [CrossRef]
- Mari, G. Middle cerebral artery peak systolic velocity for the diagnosis of fetal anemia: The untold story. Ultrasound Obstet. Gynecol. 2005, 25, 323–330. [Google Scholar] [CrossRef]
- Fishel-Bartal, M.; Weisz, B.; Mazaki-Tovi, S.; Ashwal, E.; Chayen, B.; Lipitz, S.; Yinon, Y. Can middle cerebral artery peak systolic velocity predict polycythemia in monochorionic-diamniotic twins? Evidence from a prospective cohort study. Ultrasound Obstet. Gynecol. 2016, 48, 470–475. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2 Group QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Scheier, M.; Hernandez-Andrade, E.; Fonseca, E.B.; Nicolaides, K.H. Prediction of severe fetal anemia in red blood cell alloimmunization after previous intrauterine transfusions. Am. J. Obstet. Gynecol. 2006, 195, 1550–1556. [Google Scholar] [CrossRef] [PubMed]
- Visser, G.L.; Tollenaar, L.S.A.; Bekker, V.; Te Pas, A.B.; Lankester, A.C.; Oepkes, D.; Lopriore, E.; Verbeek, L. Leukocyte Counts and Other Hematological Values in Twin-Twin Transfusion Syndrome and Twin Anemia-Polycythemia Sequence. Fetal Diagn. Ther. 2020, 47, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Tollenaar, L.S.A.; Lopriore, E.; Slaghekke, F.; Oepkes, D.; Middeldorp, J.M.; Haak, M.C.; Klumper, F.J.C.M.; Tan, R.N.G.B.; Rijken, M.; Van Klink, J.M.M. High risk of long-term neurodevelopmental impairment in donor twins with spontaneous twin anemia-polycythemia sequence. Ultrasound Obstet. Gynecol. 2020, 55, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, Q.; Chu, S.; Shapiro, S.; Yao, H.; De Paepe, M.E. Discordant placental oxygenation and autophagy in twin anemia-polycythemia sequence (TAPS). Placenta 2020, 90, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.M.; Masoudian, P.; Fung-Kee-Fung, K.; El Demellawy, D. Intrauterine Interventions for the Treatment of Twin Anemia-Polycythemia Sequence: A Systematic Review. J. Obstet. Gynaecol. Can. 2019, 41, 981–991. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, L.D.; Fischbein, R.L.; Bhamidipalli, S.S. Twin anemia-polycythemia sequence and routine monitoring practices amongst maternal-fetal medicine specialists in the United States: An initial investigation. J. Perinat. Med. 2019, 47, 388–392. [Google Scholar] [CrossRef]
- Tollenaar, L.S.A.; Slaghekke, F.; van Klink, J.M.M.; Groene, S.G.; Middeldorp, J.M.; Haak, M.C.; Klumper, F.J.C.M.; Oepkes, D.; Lopriore, E. Twin-Twin Transfusion Syndrome with Anemia-Polycythemia: Prevalence, Characteristics, and Outcome. J. Clin. Med. 2019, 8, 1129. [Google Scholar] [CrossRef] [Green Version]
- Tollenaar, L.S.A.; Lopriore, E.; Middeldorp, J.M.; Haak, M.C.; Oepkes, D.; Slaghekke, F. Prevalence of placental dichotomy, fetal cardiomegaly and starry-sky liver in twin anemia polycythemia sequence. Ultrasound Obstet. Gynecol. 2019. [Google Scholar] [CrossRef]
- Bamberg, C.; Diemert, A.; Glosemeyer, P.; Hecher, K. Quantified discordant placental echogenicity in twin anemia-polycythemia sequence (TAPS) and middle cerebral artery peak systolic velocity. Ultrasound Obstet. Gynecol. 2018, 52, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Donepudi, R.; Akkermans, J.; Mann, L.; Klumper, F.J.; Middeldorp, J.M.; Lopriore, E.; Moise, K.J., Jr.; Bebbington, M.; Johnson, A.; Oepkes, D.; et al. Impact of cannula size on recurrent twin-twin transfusion syndrome and twin anemia-polycythemia sequence after fetoscopic laser surgery. Ultrasound Obstet. Gynecol. 2018, 52, 744–749. [Google Scholar] [CrossRef]
- McDonald, R.; Hodges, R.; Knight, M.; Teoh, M.; Edwards, A.; Neil, P.; Wallace, E.M.; DeKoninck, P. Optimal Interval between Ultrasound Scans for the Detection of Complications in Monochorionic Twins. Fetal Diagn. Ther. 2017, 41, 197–201. [Google Scholar] [CrossRef]
- Verbeek, L.; Slaghekke, F.; Sueters, M.; Middeldorp, J.M.; Klumper, F.J.; Haak, M.C.; Oepkes, D.; Lopriore, E. Hematological disorders at birth in complicated monochorionic twins. Expert Rev. Hematol. 2017, 10, 525–532. [Google Scholar] [CrossRef]
- De Paepe, M.E.; Gündoğan, F.; Mao, Q.; Chu, S.; Shapiro, S. Redness discordance in monochorionic twin placentas: Correlation with clinical and placental findings. Placenta 2017, 60, 54–60. [Google Scholar] [CrossRef]
- Sato, Y.; Ishii, K.; Yokouchi, T.; Murakoshi, T.; Kiyoshi, K.; Nakayama, S.; Yonetani, N.; Mitsuda, N. Incidences of Feto-Fetal Transfusion Syndrome and Perinatal Outcomes in Triplet Gestations with Monochorionic Placentation. Fetal Diagn. Ther. 2016, 40, 181–186. [Google Scholar] [CrossRef]
- Suzuki, S. Perinatal Outcomes of Monochorionic-Diamniotic Twin Pregnancies Uncomplicated at 28 Weeks of Gestation. Jpn. Clin. Med. 2016, 7, 15–17. [Google Scholar] [CrossRef] [Green Version]
- Lucewicz, A.; Fisher, K.; Henry, A.; Welsh, A.W. Review of the correlation between blood flow velocity and polycythemia in the fetus, neonate and adult: Appropriate diagnostic levels need to be determined for twin anemia-polycythemia sequence. Ultrasound Obstet. Gynecol. 2016, 47, 152–157. [Google Scholar] [CrossRef] [Green Version]
- Donepudi, R.; Papanna, R.; Snowise, S.; Johnson, A.; Bebbington, M.; Moise, K.J., Jr. Does anemia-polycythemia complicating twin-twin transfusion syndrome affect outcome after fetoscopic laser surgery? Ultrasound Obstet. Gynecol. 2016, 47, 340–344. [Google Scholar] [CrossRef] [Green Version]
- Stagnati, V.; Pagani, G.; Fichera, A.; Prefumo, F. Intertwin discrepancy in middle cerebral artery peak systolic velocity and third-trimester fetal growth restriction in monochorionic-diamniotic twin pregnancy. Ultrasound Obstet. Gynecol. 2016, 48, 66–71. [Google Scholar] [CrossRef]
- Ashwal, E.; Yinon, Y.; Fishel-Bartal, M.; Tsur, A.; Chayen, B.; Weisz, B.; Lipitz, S. Twin Anemia-Polycythemia Sequence: Perinatal Management and Outcome. Fetal Diagn. Ther. 2016, 40, 28–34. [Google Scholar] [CrossRef]
- Tollenaar, L.S.; Zhao, D.P.; Middeldorp, J.M.; Slaghekke, F.; Oepkes, D.; Lopriore, E. Color Difference in Placentas with Twin Anemia-Polycythemia Sequence: An Additional Diagnostic Criterion? Fetal Diagn. Ther. 2016, 40, 123–127. [Google Scholar] [CrossRef]
- Tollenaar, L.S.; Slaghekke, F.; Middeldorp, J.M.; Klumper, F.J.; Haak, M.C.; Oepkes, D.; Lopriore, E. Twin Anemia Polycythemia Sequence: Current Views on Pathogenesis, Diagnostic Criteria, Perinatal Management, and Outcome. Twin Res. Hum. Genet. 2016, 19, 222–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couck, I.; Lewi, L. The Placenta in Twin-to-Twin Transfusion Syndrome and Twin Anemia Polycythemia Sequence. Twin Res. Hum. Genet. 2016, 19, 184–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiersch, L.; Eitan, M.; Ashwal, E.; Weisz, B.; Chayen, B.; Lipitz, S.; Yinon, Y. Amniotic fluid discordance in monochorionic diamniotic twin pregnancies is associated with increased risk for twin anemia-polycythemia sequence. Prenat. Diagn. 2016, 36, 1099–1103. [Google Scholar] [CrossRef]
- Sananès, N.; Veujoz, M.; Severac, F.; Barthoulot, M.; Meyer, N.; Weingertner, A.S.; Kohler, M.; Guerra, F.; Gaudineau, A.; Nisand, I.; et al. Evaluation of the Utility of in utero Treatment of Twin Anemia-Polycythemia Sequence. Fetal Diagn. Ther. 2015, 38, 170–178. [Google Scholar] [CrossRef]
- Van Winden, K.R.; Quintero, R.A.; Kontopoulos, E.V.; Korst, L.M.; Llanes, A.; Chmait, R.H. Pre-Operative Twin Anemia/Polycythemia in the Setting of Twin-Twin Transfusion Syndrome (TTTS). Fetal Diagn. Ther. 2015, 37, 274–280. [Google Scholar] [CrossRef]
- Slaghekke, F.; Pasman, S.; Veujoz, M.; Middeldorp, J.M.; Lewi, L.; Devlieger, R.; Favre, R.; Lopriore, E.; Oepkes, D. Middle cerebral artery peak systolic velocity to predict fetal hemoglobin levels in twin anemia-polycythemia sequence. Ultrasound Obstet. Gynecol. 2015, 46, 432–436. [Google Scholar] [CrossRef] [Green Version]
- Sueters, M.; Oepkes, D. Diagnosis of twin-to-twin transfusion syndrome, selective fetal growth restriction, twin anaemia-polycythaemia sequence, and twin reversed arterial perfusion sequence. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 215–226. [Google Scholar] [CrossRef]
- Mabuchi, A.; Ishii, K.; Yamamoto, R.; Taguchi, T.; Murata, M.; Hayashi, S.; Mitsuda, N. Clinical characteristics of monochorionic twins with large hemoglobin level discordance at birth. Ultrasound Obstet. Gynecol. 2014, 44, 311–315. [Google Scholar] [CrossRef]
- Slaghekke, F.; van Klink, J.M.; Koopman, H.M.; Middeldorp, J.M.; Oepkes, D.; Lopriore, E. Neurodevelopmental outcome in twin anemia-polycythemia sequence after laser surgery for twin-twin transfusion syndrome. Ultrasound Obstet. Gynecol. 2014, 44, 316–321. [Google Scholar] [CrossRef]
- Baschat, A.A.; Oepkes, D. Twin anemia-polycythemia sequence in monochorionic twins: Implications for diagnosis and treatment. Am. J. Perinatol. 2014, 31 (Suppl. 1), S25–S30. [Google Scholar] [CrossRef]
- Rossi, A.C.; Prefumo, F. Perinatal outcomes of twin anemia-polycythemia sequence: A systematic review. J. Obstet. Gynaecol. Can. 2014, 36, 701–707. [Google Scholar] [CrossRef] [Green Version]
- Zhao, D.; Slaghekke, F.; Middeldorp, J.M.; Duan, T.; Oepkes, D.; Lopriore, E. Placental share and hemoglobin level in relation to birth weight in twin anemia-polycythemia sequence. Placenta 2014, 35, 1070–1074. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, L.; Slaghekke, F.; Hulzebos, C.V.; Oepkes, D.; Walther, F.J.; Lopriore, E. Hypoalbuminemia in donors with twin anemia-polycythemia sequence: A matched case-control study. Fetal Diagn. Ther. 2013, 33, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.P.; de Villiers, S.F.; Slaghekke, F.; Walther, F.J.; Middeldorp, J.M.; Oepkes, D.; Lopriore, E. Prevalence, size, number and localization of vascular anastomoses in monochorionic placentas. Placenta 2013, 34, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Favre, R.; Koch, A.; Weingertner, A.S.; Sananes, N.; Tu Trieu, N.; Kohler, M.; Guerra, F.; Nisand, I. Vascular pattern in monochorionic placentas with spontaneous TAPS and TTTS with residual anastomoses after laser: A case-control study. Prenat. Diagn. 2013, 33, 979–982. [Google Scholar] [CrossRef]
- Nakayama, S.; Ishii, K.; Kawaguchi, H.; Hayashi, S.; Hidaka, N.; Murakoshi, T.; Mitsuda, N. Perinatal outcome of monochorionic diamniotic twin pregnancies managed from early gestation at a single center. J. Obstet. Gynaecol. Res. 2012, 38, 692–697. [Google Scholar] [CrossRef] [PubMed]
- de Villiers, S.; Slaghekke, F.; Middeldorp, J.M.; Klumper, F.J.; Walther, F.J.; Oepkes, D.; Lopriore, E. Arterio-arterial vascular anastomoses in monochorionic twin placentas with and without twin anemia-polycythemia sequence. Placenta 2012, 33, 227–229. [Google Scholar] [CrossRef]
- Lopriore, E.; Slaghekke, F.; Middeldorp, J.M.; Klumper, F.J.; van Lith, J.M.; Walther, F.J.; Oepkes, D. Accurate and simple evaluation of vascular anastomoses in monochorionic placenta using colored dye. J. Vis. Exp. 2011, e3208. [Google Scholar] [CrossRef] [Green Version]
- Lopriore, E.; Slaghekke, F.; Oepkes, D.; Middeldorp, J.M.; Vandenbussche, F.P.; Walther, F.J. Hematological characteristics in neonates with twin anemia-polycythemia sequence (TAPS). Prenat. Diagn. 2010, 30, 251–255. [Google Scholar] [CrossRef]
- Slaghekke, F.; Kist, W.J.; Oepkes, D.; Pasman, S.A.; Middeldorp, J.M.; Klumper, F.J.; Walther, F.J.; Vandenbussche, F.P.H.A.; Lopriore, E. Twin anemia-polycythemia sequence: Diagnostic criteria, classification, perinatal management and outcome. Fetal Diagn. Ther. 2010, 27, 181–190. [Google Scholar] [CrossRef]
- Lopriore, E.; Slaghekke, F.; Oepkes, D.; Middeldorp, J.M.; Vandenbussche, F.P.; Walther, F.J. Clinical outcome in neonates with twin anemia-polycythemia sequence. Am. J. Obstet. Gynecol. 2010, 203, 54.e1–54.e5. [Google Scholar] [CrossRef]
- Habli, M.; Bombrys, A.; Lewis, D.; Lim, F.Y.; Polzin, W.; Maxwell, R.; Crombleholme, T. Incidence of complications in twin-twin transfusion syndrome after selective fetoscopic laser photocoagulation: A single-center experience. Am. J. Obstet. Gynecol. 2009, 201, 417.e1–417.e7. [Google Scholar] [CrossRef] [PubMed]
- Slaghekke, F.; Kist, W.J.; Oepkes, D.; Middeldorp, J.M.; Klumper, F.J.; Vandenbussche, F.P.H.A.; Lopriore, E. TAPS and TOPS: Two distinct forms of feto-fetal transfusion in monochorionic twins. Z. Geburtshilfe Neonatol. 2009, 213, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Lopriore, E.; Oepkes, D.; Middeldorp, J.M.; Vandenbussche, F.P. You only find what you are looking for. BJOG 2007, 114, 1306. [Google Scholar] [CrossRef] [PubMed]
- Lopriore, E.; Middeldorp, J.M.; Oepkes, D.; Klumper, F.J.; Walther, F.J.; Vandenbussche, F.P. Residual anastomoses after fetoscopic laser surgery in twin-to-twin transfusion syndrome: Frequency, associated risks and outcome. Placenta 2007, 28, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Mackie, F.L.; Morris, R.K.; Kilby, M.D. The prediction, diagnosis and management of complications in monochorionic twin pregnancies: The OMMIT (Optimal Management of Monochorionic Twins) study. BMC Pregnancy Childbirth 2017, 17, 153. [Google Scholar] [CrossRef]
- Farah, N.; Hogan, J.; Johnson, S.; Stuart, B.; Daly, S. Prospective risk of fetal death in uncomplicated monochorionic twins. Acta Obstet. Gynecol. Scand. 2012, 91, 382–385. [Google Scholar] [CrossRef]
- Barigye, O.; Pasquini, L.; Galea, P.; Chambers, H.; Chappell, L.; Fisk, N.M. High risk of unexpected late fetal death in monochorionic twins despite intensive ultrasound surveillance: A cohort study. PLoS Med. 2005, 2, e172. [Google Scholar] [CrossRef] [Green Version]
- Cheong-See, F.; Schuit, E.; Arroyo-Manzano, D.; Asma, K.; Barrett, J.; Joseph, K.S.; Asztalos, E.; Hack, K.; Lewi, L.; Lim, A.; et al. Prospective risk of stillbirth and neonatal complications in twin pregnancies: Systematic review and meta-analysis. BMJ 2016, 354, i4353. [Google Scholar] [CrossRef] [Green Version]
- Reitsma, J.B.; Rutjes, A.W.; Khan, K.S.; Coomarasamy, A.; Bossuyt, P.M. A review of solutions for diagnostic accuracy studies with an imperfect or missing reference standard. J. Clin. Epidemiol. 2009, 62, 797–806. [Google Scholar] [CrossRef] [Green Version]
- Parthenis, C.; Koleskas, D.; Spanoudaki, C.; Delivoria, V.; Souka, A. Upper limb vascular occlusion in the recipient of a monochorionic twin pair. J. Matern. Fetal Neonatal Med. 2015, 28, 922–923. [Google Scholar] [CrossRef] [PubMed]
- Tollenaar, L.S.A.; Slaghekke, F.; Lewi, L.; Ville, Y.; Lanna, M.; Weingertner, A.; Ryan, G.; Arévalo, S.; Khalil, A.; Brock, C.O.; et al. Treatment and outcome in 370 cases with spontaneous or post-laser twin anemia polycythemia sequence managed in 17 different fetal therapy centers. Ultrasound Obstet. Gynecol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Stranak, Z.; Korcek, P.; Hympanova, L.; Kyncl, M.; Krofta, L. Prenatally Acquired Multiple Limb Ischemia in a Very Low Birth Weight Monochorionic Twin. Fetal Diagn. Ther. 2017, 41, 237–238. [Google Scholar] [CrossRef] [PubMed]
- Brinsmead, S.K.; Walsh, C.A. TAPS-related fetal cerebellar disruption. J. Matern. Fetal Neonatal Med. 2017, 30, 2354–2355. [Google Scholar] [CrossRef] [PubMed]
- Lopriore, E.; Slaghekke, F.; Kersbergen, K.J.; de Vries, L.S.; Drogtrop, A.P.; Middeldorp, J.M.; Oepkes, D.; Benders, M.J. Severe cerebral injury in a recipient with twin anemia-polycythemia sequence. Ultrasound Obstet. Gynecol. 2013, 41, 702–706. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Document Number | Author | Pubmed ID | Year | Reason for Exclusion |
|---|---|---|---|---|
| 1 | Visser et al. | 31261154 | 2020 | Prenatal MCA-PSV not reported |
| 2 | Tollenaar et al. | 31432580 | 2020 | Postnatal Hb not reported |
| 3 | Mao et al. | 32056557 | 2020 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 4 | Tavares de Sousa et al. | 30207009 | 2019 | Included |
| 5 | Tollenaar et al. | 30125414 | 2019 | Included |
| 6 | Nicholas et al. | 30763267 | 2019 | Review article |
| 7 | Hill et al. | 31230662 | 2019 | Systematic review on treatments |
| 8 | Nicholas et al. | 31277521 | 2019 | Review article |
| 9 | Tollenaar et al. | 31366031 | 2019 | Postnatal Hb not reported |
| 10 | Khalil et al. | 31605505 | 2019 | Review article |
| 11 | Tollenaar et al. | 31856326 | 2019 | Postnatal Hb not reported |
| 12 | Bamberg et al. | 28557152 | 2018 | Postnatal Hb not reported |
| 13 | Donepudi et al. | 28925589 | 2018 | Postnatal Hb not reported |
| 14 | McDonald et al. | 27561094 | 2017 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 15 | Verbeek et al. | 28460542 | 2017 | Prenatal MCA-PSV not reported |
| 16 | De Paepe et al. | 29208240 | 2017 | Prenatal MCA-PSV not reported |
| 17 | Fishel-Bartal et al. | 26663574 | 2016 | Included |
| 18 | Sato et al. | 26760043 | 2016 | Study on triplets with monochorionic placentation |
| 19 | Suzuki et al. | 27257402 | 2016 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 20 | Lucewicz et al. | 25580896 | 2016 | Review article |
| 21 | Donepudi et al. | 26033705 | 2016 | Postnatal Hb not reported |
| 22 | Stagnati et al. | 26173065 | 2016 | Postnatal Hb not reported |
| 23 | Ashwal et al. | 26580546 | 2016 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 24 | Tollenaar et al. | 26788848 | 2016 | Prenatal MCA-PSV not reported |
| 25 | Tollenaar et al. | 27068715 | 2016 | Review article |
| 26 | Couck et al. | 27098457 | 2016 | Review article |
| 27 | Hiersch et al. | 27734505 | 2016 | Both parameters reported, however cannot determine true/false negatives (i.e., Hb levels when MCA-PSV were negative). Specificity, sensitivity, ROC not reported. |
| 28 | Sananes et al. | 25790745 | 2015 | Prenatal MCA-PSV not reported |
| 29 | Veujoz et al. | 25484182 | 2015 | Included |
| 30 | Yokouchi et al. | 25510181 | 2015 | Prenatal MCA-PSV not reported |
| 31 | Van Winden et al. | 25721425 | 2015 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 32 | Slaghekke et al. | 26094734 | 2015 | Included |
| 33 | Sueters et al. | 24433823 | 2014 | Review article |
| 34 | Mabuchi et al. | 24585685 | 2014 | Prenatal MCA-PSV not reported |
| 35 | Slaghekke et al. | 24706478 | 2014 | Prenatal MCA-PSV not reported |
| 36 | Slaghekke et al. | 24753027 | 2014 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 37 | Baschat et al. | 24858317 | 2014 | Review article |
| 38 | Rossi et al. | 25222165 | 2014 | Systematic review of outcomes |
| 39 | Zhao et al. | 25449031 | 2014 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 40 | de Villiers et al. | 23481221 | 2013 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 41 | Verbeek et al. | 23485951 | 2013 | Prenatal MCA-PSV not reported |
| 42 | Zhao et al. | 23639577 | 2013 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 43 | Favre et al. | 23744723 | 2013 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 44 | Nakayama et al. | 22413750 | 2012 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 45 | de Villiers et al. | 22257747 | 2012 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 46 | Lopriore et al. | 21912373 | 2011 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 47 | Lopriore et al. | 20087909 | 2010 | Prenatal MCA-PSV not reported |
| 48 | Slaghekke et al. | 20339296 | 2010 | Review article |
| 49 | Lopriore et al. | 20417489 | 2010 | Prenatal MCA-PSV not reported |
| 50 | Habli et al. | 19788973 | 2009 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 51 | Slaghekke et al. | 20099211 | 2009 | Review article |
| 52 | Lopriore et al. | 18827116 | 2008 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 53 | Lopriore et al. | 17877693 | 2007 | Letter to editor |
| 54 | Robyr et al. | 16522415 | 2006 | Unclear if Hb was measured on cases with normal MCA |
| Studies from the secondary search of bibliographies | ||||
| 1 | Lopriore et al. | 16644009 | 2006 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 2 | Lewi et al. | 18533114 | 2008 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
| 3 | Mackie et al. | 28549467 | 2017 | Neither prenatal MCA-PSV nor postnatal Hb were reported |
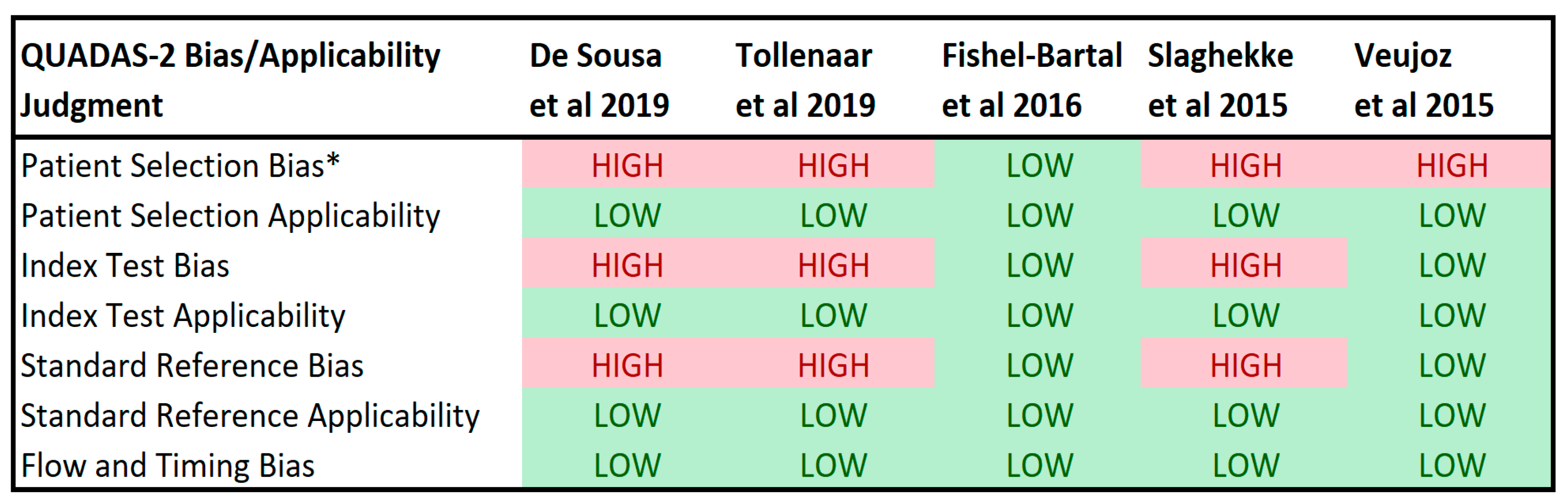
| QUADAS II Signaling Questions | De Sousa 2019 | Tollenaar 2019 | Fishel-Bartal 2016 | Slaghekke 2015 | Veujoz 2015 |
|---|---|---|---|---|---|
| Domain 1: Patient Selection Risk of Bias | |||||
| Was a consecutive or random sample of patients enrolled? | No * | Yes | Yes | No ƚ | No ƚ |
| Was a case-control design avoided? | Yes | Yes | Yes | No ƚ | No ƚ |
| Did the study avoid inappropriate exclusions? | Yes | No ǂ | Yes | Yes | Yes |
| Domain 2: Index Test Bias Risk of Bias | |||||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | Yes | Yes | Yes | Yes |
| If a threshold was used, was it prespecified? | Unclear | Unclear | Unclear | Yes | Yes |
| Was a clearly defined schedule described for timing of initial and follow-up application of the index test? | No § | No § | Yes | No § | Yes |
| Domain 3: Reference Test Risk of Bias | |||||
| Is the reference standard likely to correctly classify the target condition? | Yes | Yes | Yes | Yes | Yes |
| Were the reference standard results interpreted without knowledge of the results or the index test? | Unclear | Unclear | Unclear | Unclear | Unclear |
| Were reference test values from repeat intrauturine transfusions or reference test values following birth in neonates who had a previous intrauterine transfusion used to calculate sensitivity/specificity? | No | Yes ¶ | No | Yes # | No |
| Domain 4: Flow and Timing Risk of Bias | |||||
| Was there an appropriate interval between the test(s) and reference standard? | Yes (at birth) | Yes (≤1 wk) | Yes (≤1 wk) | Yes (<48 h) | Yes (at birth) |
| Did all patients receive the reference standard? | Yes | Yes | Yes | Yes | Unclear |
| Did patients receive the same reference standard? | Yes | Yes | Yes | Yes | Yes |
| Were all patients included in the analysis? | Yes | Yes | No (69/162, 43%) | Yes | No (9/20, 45%) |
| Characteristic | De Sousa 2019 | Tollenaar 2019 | Fishel-Bartal 2016 | Slaghekke 2015 | Veujoz 2015 |
|---|---|---|---|---|---|
| Study Design | Retrospective | Retrospective | Prospective | Retrospective | Prospective |
| Number of women | 154 | 80 | 69 | 43 | 433 |
| Number and Type of TAPS | 15 (14 s + 1 pl) | 35 * | 9 (7 s + 2 pl) | 43 (12 s + 31 pl) | 20 (10 s + 10 pl) |
| Incidence of TAPS | 9.7% | 35.3% | 13.0% | N/A | 4.6% |
| GA at delivery all twins (wks) | 35 (26–39) wks | 35 (33–36) controls only | 33.6 (24.6–38.3) | -- | -- |
| GA at diagnosis (wks) | 34.8 (26–39) | <1 wk before delivery | <1 wk before delivery | 25 (19–30) Antenatal diagnosis 26.5 (19–32) Postnatal diagnosis | 24.8 +/− 5.9 |
| GA at delivery for TAPS cases (wks) | 29 + 4 to 37 + 0 | 32 (29–34) | -- | 25 (19–30) Antenatal diagnosis 26.5 (19–32) Postnatal diagnosis | 32.1 +/− 1.9 |
| TAPS Stage at diagnosis | Not reported | Not reported | Not reported | Not reported | Stage I-47.0% Stage II-29.4% Stage III-17.7% Stage IV-5.9% Stage V-0.0% |
| Treatment of TAPS | Not reported | IUT-6 IUT + PET-4 | IUT-2 | Not reported | IUT-2 FLS-7 |
| Overall Survival following TAPS diagnosis | Not reported | 55/58 (94.8%) | Not reported | 69/82 (84.1%) | 15/20 (75.0%) |
| Cesarean Delivery | 72.1% | Not reported | 50.7% | 78.9% | Not reported |
| Characteristic | De Sousa 2019 | Tollenaar 2019 | Fishel-Bartal 2016 | Slaghekke 2015 | Veujoz 2015 |
|---|---|---|---|---|---|
| Interval between MCA-PSV and Hb measurement | 2 (0–7) days | <1 week | <1 week | -- | <48 h |
| Antenatal finding for diagnosis of TAPS | ΔMCA-PSV > 0.373 MOM (cutoff determined by ROC analysis) | (1) MCA-PSV < 1.0 MOM (recipient), MCA-PSV > 1.5 MOM(donor) (2) ΔMCA-PSV > 0.5 MOM | (1) MCA-PSV < 1.0 MOM (recipient), MCA-PSV > 1.5 MOM (donor) (2) ΔMCA-PSV by ROC analysis. (ROC cutoff not reported) | MCA-PSV < 1.0 MOMs (recipient), MCA-PSV > 1.5 MOMs (donor) | MCA-PSV < 1.0 MOMs (recipient), MCA-PSV > 1.5 MOMs (donor) |
| Postnatal finding for diagnosis of TAPS | Hb difference > 90% (7.25 Hb) | Hb difference > 8 g/dL and Reticulocyte Ratio > 1.7 or anastomoses < 1mm | Anemia: Hct < 45% Polycythemia: Hct > 65% | Anemia: Hct > 5 SD below mean Polycythemia: Hct > 5 SD above mean | Hb difference > 8 g/dL and Reticulocyte Ratio > 1.7 or anastomoses < 1mm |
| AUC (95% CI) | 0.976 (0.935–0.993) | Not reported | 1) Anemia: 0.687 (0.547–0.827) Polycythemia: 0.617 (0.505–0.728) 2) TAPS 0.871 (0.757–0.985) | Not Reported | Not Reported |
| Sensitivity (95% CI) | 93.3% (68.1–99.8) | 1) 46% (30–62) 2) 83% (67–92) | Not reported | Anemia: 94% (85–98) Polycythemia: 97% (87–99) | 71% |
| Specificity (95% CI) | 95.7% (90.8–98.4) | 1) 100% (29–100) 2) 100% (92–100) | Not reported | Anemia: 74% (62–83) Polycythemia: 96% (89–99) | 50% |
| PPV (95% CI) | 70.0% (45.7–88.1) | 1) 100% (81–100) 2) 100% (88–100) | Not reported | Anemia: 76% (65–85) Polycythemia: 93% (93–100) | 88% |
| NPV (95% CI) | 99.3% (95.9–100) | 1) 70% (58–80) 2) 88% (77–94) | Not reported | Anemia: 94% (83–98) Polycythemia: 99% (93–100) | 33% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brock, C.O.; Bergh, E.P.; Moise, K.J., Jr; Johnson, A.; Hernandez-Andrade, E.; Lai, D.; Papanna, R. Middle Cerebral Artery Doppler Velocimetry for the Diagnosis of Twin Anemia Polycythemia Sequence: A Systematic Review. J. Clin. Med. 2020, 9, 1735. https://doi.org/10.3390/jcm9061735
Brock CO, Bergh EP, Moise KJ Jr, Johnson A, Hernandez-Andrade E, Lai D, Papanna R. Middle Cerebral Artery Doppler Velocimetry for the Diagnosis of Twin Anemia Polycythemia Sequence: A Systematic Review. Journal of Clinical Medicine. 2020; 9(6):1735. https://doi.org/10.3390/jcm9061735
Chicago/Turabian StyleBrock, Clifton O., Eric P. Bergh, Kenneth J. Moise, Jr, Anthony Johnson, Edgar Hernandez-Andrade, Dejian Lai, and Ramesha Papanna. 2020. "Middle Cerebral Artery Doppler Velocimetry for the Diagnosis of Twin Anemia Polycythemia Sequence: A Systematic Review" Journal of Clinical Medicine 9, no. 6: 1735. https://doi.org/10.3390/jcm9061735