Clinical Outcome of Edoxaban vs. Vitamin K Antagonists in Patients with Atrial Fibrillation and Diabetes Mellitus: Results from a Multicenter, Propensity-Matched, Real-World Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J.; Howard, V.J.; et al. Executive Summary: Heart Disease and Stroke Statistics—2015 Update: A report from the American Heart Association. Circulation 2015, 131, 434–441. [Google Scholar] [CrossRef]
- Pallisgaard, J.L.; Schjerning, A.-M.; Lindhardt, T.B.; Procida, K.; Hansen, M.L.; Torp-Pedersen, C.; Gislason, G. Risk of atrial fibrillation in diabetes mellitus: A nationwide cohort study. Eur. J. Prev. Cardiol. 2015, 23, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Echouffo-Tcheugui, J.B.; Shrader, P.; Thomas, L.; Gersh, B.J.; Kowey, P.R.; Mahaffey, K.W.; Singer, D.E.; Hylek, E.M.; Go, A.S.; Peterson, E.D.; et al. Care Patterns and Outcomes in Atrial Fibrillation Patients with and without Diabetes. J. Am. Coll. Cardiol. 2017, 70, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Esti-mates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [Green Version]
- Du, X.; Ninomiya, T.; De Galan, B.; Abadir, E.; Chalmers, J.; Pillai, A.; Woodward, M.; Cooper, M.; Harrap, S.B.; Hamet, P.; et al. Risks of cardiovascular events and effects of routine blood pressure lowering among patients with type 2 diabetes and atrial fibrillation: Results of the ADVANCE study. Eur. Hear. J. 2009, 30, 1128–1135. [Google Scholar] [CrossRef] [Green Version]
- Proietti, R.; Russo, V.; Wu, M.A.; Maggioni, A.P.; Marfella, R. Diabetes mellitus and atrial fibrillation: Evidence of a pathophysiological, clinical and epidemiological association beyond the thromboembolic risk. Giornale Italiano Cardiologia 2017, 18, 199–207. [Google Scholar]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castellà, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace 2016, 18, 1609–1678. [Google Scholar] [CrossRef]
- Plitt, A.; Ruff, C.T.; Goudev, A.; Morais, J.; Ostojic, M.C.; Grosso, M.A.; Lanz, H.J.; Park, J.-G.; Antman, E.M.; Braunwald, E.; et al. Efficacy and safety of edoxaban in patients with diabetes mellitus in the ENGAGE AF-TIMI 48 trial. Int. J. Cardiol. 2020, 304, 185–191. [Google Scholar] [CrossRef]
- Kaatz, S.; Ahmad, D.; Spyropoulos, A.C.; Schulman, S.; Anticoagulation, F.T.S.O.C.O. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2015, 13, 2119–2126. [Google Scholar] [CrossRef]
- Singer, D.E.; Chang, Y.; Fang, M.C.; Borowsky, L.H.; Pomernacki, N.K.; Udaltsova, N.; Go, A.S. The Net Clinical Benefit of Warfarin Anticoagulation in Atrial Fibrillation. Ann. Intern. Med. 2009, 151, 297–305. [Google Scholar] [CrossRef]
- Plitt, A.; McGuire, D.K.; Giugliano, R.P. Atrial Fibrillation, Type 2 Diabetes, and Non–Vitamin K Antagonist Oral Anticoagulants. JAMA Cardiol. 2017, 2, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Patti, G.; Di Gioia, G.; Cavallari, I.; Nenna, A. Safety and efficacy of nonvitamin K antagonist oral anticoagulants versus warfarin in diabetic patients with atrial fibrillation: A study-level meta-analysis of phase III randomized trials. Diabetes/Metab. Res. Rev. 2017, 33, e2876. [Google Scholar] [CrossRef] [PubMed]
- Varughese, G.I.; Patel, J.V.; Tomson, J.; Lip, G.Y. The prothrombotic risk of diabetes mellitus in atrial fibrillation and heart failure. J. Thromb. Haemost. 2005, 3, 2811–2813. [Google Scholar] [CrossRef]
- Benson, R.T.; Sacco, R.L. Stroke prevention: Hypertension, diabetes, tobacco, and lipids. Neurol. Clin. 2000, 18, 309–319. [Google Scholar] [CrossRef]
- Overvad, T.F.; Skjøth, F.; Lip, G.Y.; Lane, D.A.; Albertsen, I.E.; Rasmussen, L.H.; Larsen, T.B. Duration of Diabetes Mellitus and Risk of Thromboembolism and Bleeding in Atrial Fibrillation. Stroke 2015, 46, 2168–2174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, C.I.; Bunz, T.J.; Eriksson, D.; Sood, N.A.; Meinecke, A.-K. Effectiveness and safety of rivaroxaban vs. warfarin in people with non-valvular atrial fibrillation and diabetes: An administrative claims database analysis. Diabet. Med. 2018, 35, 1105–1110. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Hsu, P.-F.; Sung, S.-H.; Tu, S.-T.; Yu, B.-H.; Huang, C.-J.; Cheng, H.-M. Is There a Preferred Stroke Prevention Strategy for Diabetic Patients with Non-Valvular Atrial Fibrillation? Comparing Warfarin, Dabigatran and Rivaroxaban. Thromb. Haemost. 2018, 118, 072–081. [Google Scholar] [CrossRef]
- Russo, V.; Attena, E.; Mazzone, C.; Melillo, E.; Rago, A.; Galasso, G.; Riegler, L.; Parisi, V.; Rotunno, R.; Nigro, G.; et al. Real-life Performance of Edoxaban in Elderly Patients with Atrial Fibrillation: A Multicenter Propensity Score–Matched Cohort Study. Clin. Ther. 2019, 41, 1598–1604. [Google Scholar] [CrossRef]
- Patti, G.; Lucerna, M.; Cavallari, I.; Ricottini, E.; Renda, G.; Pecen, L.; Romeo, F.; Le Heuzey, J.-Y.; Zamorano, J.L.; Kirchhof, P.; et al. Insulin-Requiring Versus Noninsulin-Requiring Diabetes and Thromboembolic Risk in Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2017, 69, 409–419. [Google Scholar] [CrossRef]
- El Khawand, C.; Jamart, J.; Donckier, J.; Chatelain, B.; Lavenne, E.; Moriau, M.; Buysschaert, M. Hemostasis variables in type I diabetic patients without demonstrable vascular complications. Diabetes Care 1993, 16, 1137–1145. [Google Scholar] [CrossRef]
- Carmassi, F.; Morale, M.; Puccetti, R.; De Negri, F.; Monzani, F.; Navalesi, R.; Mariani, G. Coagulation and fibrinolytic system impairment in insulin dependent diabetes mellitus. Thromb. Res. 1992, 67, 643–654. [Google Scholar] [CrossRef]
- Kaur, R.; Kaur, M.; Singh, J. Endothelial dysfunction and platelet hyperactivity in type 2 diabetes mellitus: Molecular insights and therapeutic strategies. Cardiovasc. Diabetol. 2018, 17, 121. [Google Scholar] [CrossRef] [PubMed]
- Madonna, R.; De Caterina, R. Cellular and molecular mechanisms of vascular injury in diabetes—Part I: Pathways of vascular disease in diabetes. Vasc. Pharmacol. 2011, 54, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Fangel, M.V.; Nielsen, P.B.; Kristensen, J.K.; Larsen, T.B.; Overvad, T.F.; Lip, G.Y.; Jensen, M.B.B. Glycemic Status and Thromboembolic Risk in Patients with Atrial Fibrillation and Type 2 Diabetes Mellitus. Circ. Arrhythmia Electrophysiol. 2019, 12, e007030. [Google Scholar] [CrossRef] [PubMed]
- Shireman, T.I.; Howard, P.A.; Kresowik, T.; Ellerbeck, E. Combined Anticoagulant–Antiplatelet Use and Major Bleeding Events in Elderly Atrial Fibrillation Patients. Stroke 2004, 35, 2362–2367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Ruff, C.T.; Giugliano, R.P.; Murphy, S.A.; Nordio, F.; Patel, I.; Shi, M.; Mercuri, M.; Antman, E.M.; Braunwald, E. Concomitant Use of Single Antiplatelet Therapy with Edoxaban or Warfarin in Patients with Atrial Fibrillation: Analysis from the ENGAGE AF-TIMI48 Trial. J. Am. Hear. Assoc. 2016, 5. [Google Scholar] [CrossRef] [Green Version]



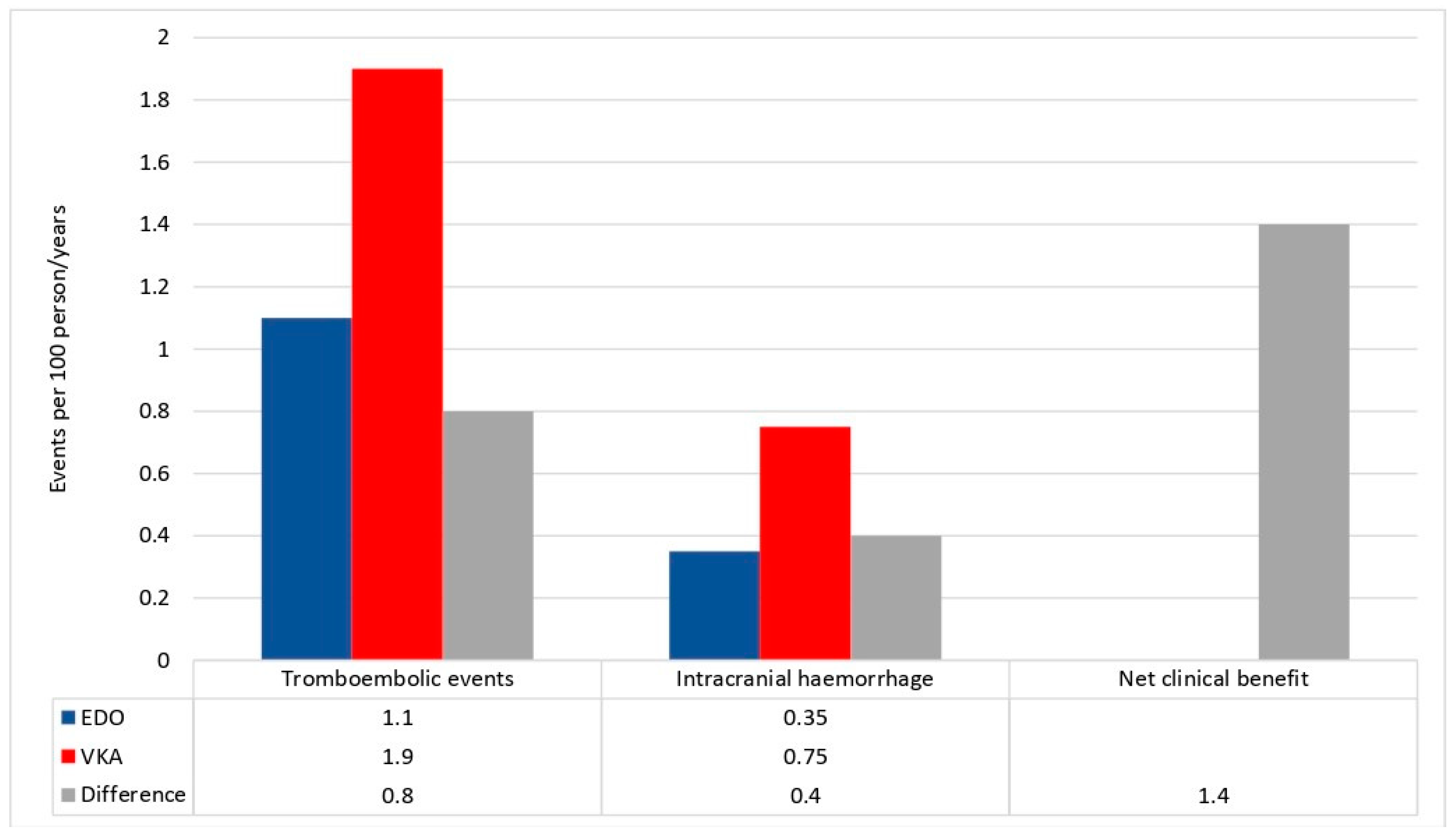{kind=link}
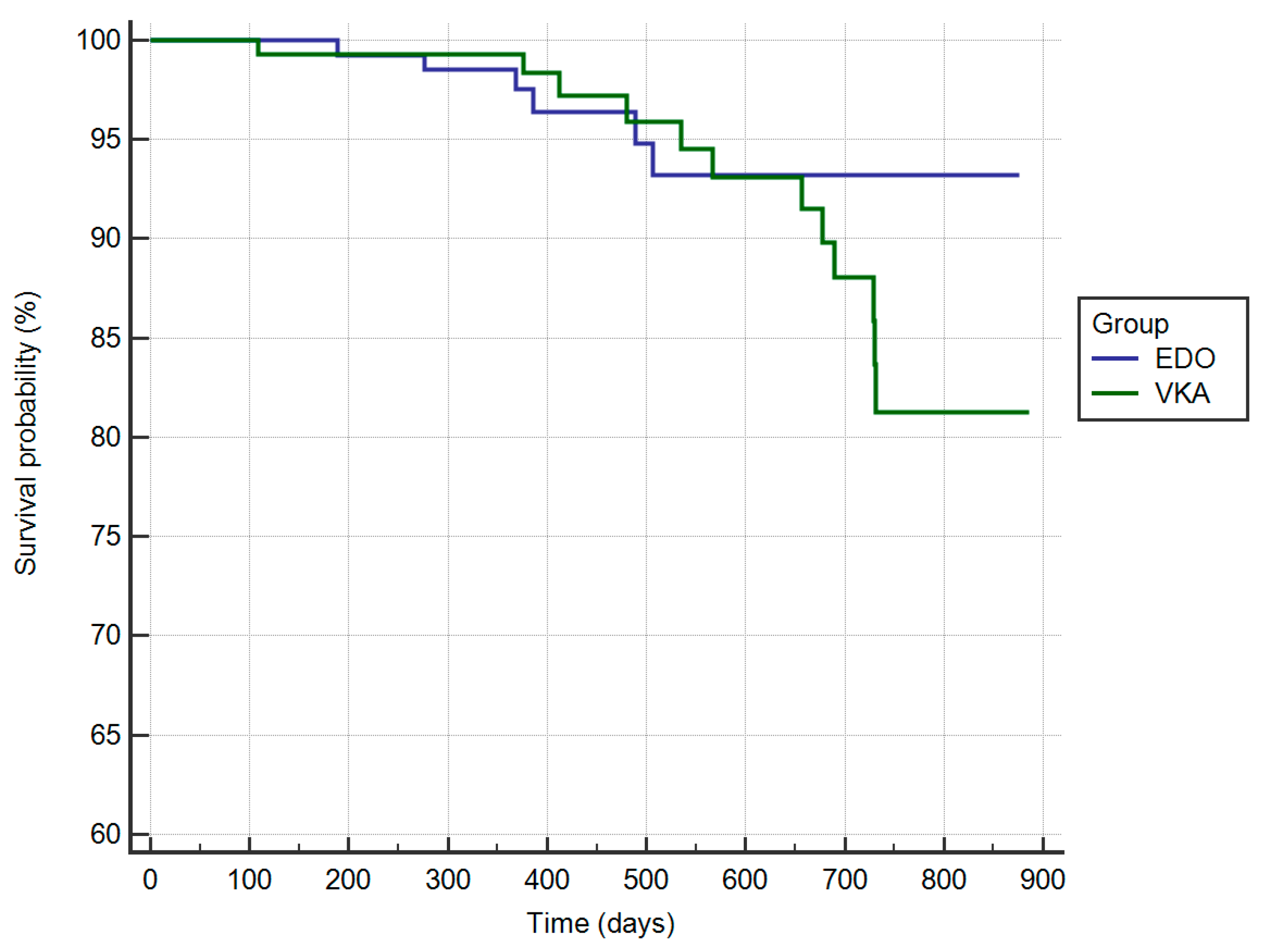{kind=link}
| Variable | Before Propensity Score Matching | After Propensity Score Matching | ||||
|---|---|---|---|---|---|---|
| EDO (n = 230) | VKA (n = 327) | p-Value | EDO (n = 135) | VKA (n = 135) | p-Value | |
| Age (years) | 69.1 ± 9.1 | 76.9 ± 1.4 | <0.001 | 69.2 ± 5.1 | 70.3 ± 5.0 | 0.72 |
| Female (n, %) | 105 (45.5) | 141 (43.1) | 0.59 | 56 (41.4) | 55 (40.7) | 0.71 |
| BMI (kg/m2) | 24.8 ± 4.5 | 28.8 ± 4.1 | 0.08 | 27.3 ± 3.3 | 27.6 ± 3.3 | 0.77 |
| Paroxysmal AF (n, %) | 57 (25) | 88 (27) | 0.78 | 34 (25) | 35 (26) | 0.78 |
| Persistent AF (n, %) | 80 (35) | 121 (37) | 0.89 | 46 (34) | 49 (36) | 0.81 |
| Permanent AF (n, %) | 92 (40) | 118 (36) | 0.82 | 55 (41) | 51 (38) | 0.81 |
| Hypertension (n, %) | 111 (48.5) | 197 (60.2) | 0.001 | 72 (53.1) | 75 (55.6) | 0.56 |
| Heart failure (n, %) | 39 (16.8) | 92 (28.2) | 0.001 | 28 (20.8) | 29 (21.4) | 0.7 |
| Prior stroke/TIA (n, %) | 64 (27.8) | 116 (35.4) | 0.001 | 39 (28.8) | 40 (29.4) | 0.7 |
| Prior major bleeding (n, %) | 10 (4.3) | 24 (7.5) | 0.06 | 5 (3.5) | 5 (3.5) | 0.7 |
| Prior MI (n, %) | 19 (8.3) | 43 (13.2) | 0.02 | 8 (5.7) | 9 (6.5) | 0.7 |
| CKD (n, %) | 36 (15.5) | 53 (16.1) | 0.57 | 21 (15.4) | 22 (16.1) | 0.57 |
| CHA2DS2VASc score | 4.2 ± 1.7 | 4.6 ± 1.6 | 0.57 | 4.3 ± 1.4 | 4.5 ± 1.5 | 0.56 |
| HAS-BLED score | 3.4 ± 1.4 | 3.6 ± 1.3 | 0.57 | 3.5 ± 1.1 | 3.6 ± 1.7 | 0.56 |
| LVEF (%) | 49.5 ± 6.4 | 40.3 ± 7.1 | 0.003 | 44.4 ± 5.2 | 42.3 ± 4.8 | 0.8 |
| Glycated hemoglobin (%) | 8.9 ± 1.1 | 9.6 ± 2.3 | 0.89 | 8.2 ± 1.5 | 8.9 ± 1.6 | 0.78 |
| Insulin Therapy (n, %) | 55 (24) | 114 (35) | 0.002 | 27 (20) | 27 (20) | 0.8 |
| Antiplatelets (n, %) | 44 (19) | 39 (12) | 0.05 | 15 (11) | 15 (11) | 0.8 |
| Oral hypoglycemic agents (n, %) | 182 (79) | 265 (81) | 0.57 | 108 (80) | 109 (81) | 0.9 |
| Lipid lowering drugs (n, %) | 182 (79) | 262 (80) | 0.57 | 128 (94.8) | 128 (94.8) | 0.9 |
| Edoxaban 60 mg (n, %) | 200 (87) | − | 117 (87) | |||
| Edoxaban 30 mg (n, %) | 30 (13) | − | 18 (13) | |||
| Acenocumarolo (n, %) | 42 (13) | 2 (1.5) | ||||
| Warfarin (n, %) | − | 284 (87) | 133 (98.5) | |||
| Therapeutic Dosage (n, %) | 216 (94) | 100 | ||||
| Underdosing (n, %) | 11 (5) | − | ||||
| Overdosing (n, %) | 2 (1) | − | ||||
| Predictors of Major Bleeding Events | ||
|---|---|---|
| Variable | HR (95% CI; Univariable) | HR (95% CI: Multivariable) |
| Age | 1.10 (0.87–1.12, p = 0.965) | − |
| Female sex | 0.99 (0.71–1.38, p = 0.969) | − |
| BMI | 1.00 (0.98–1.02, p = 0.973) | − |
| Hypertension | 0.69 (0.43–1.12, p = 0.132) | − |
| CAD | 0.70 (0.43–1.12, p = 0.134) | − |
| Heart failure | 1.47 (0.60–3.59, p = 0.396) | − |
| CKD | 0.89 (0.29–2.67, p = 0.832) | − |
| Prior Stroke/TIA | 1.05 (0.71–1.55, p = 0.796) | − |
| Past Bleeding | 1.08 (0.86–1.35, p = 0.515) | − |
| Glycated Hemoglobin | 1.24 (0.48–3.61, p = 0.396) | − |
| Oral Hypoglycemic Agents | 1.38 (1.10–1.78, p = 0.059) | NS |
| Antiplatelet Drug | 2.54 (1.53–4.22, p < 0.001) | 2.41 (1.43–4.07, p = 0.001) |
| Insulin Therapy | 1.76 (1.20–2.59, p = 0.004) | NS |
| Predictors of Thromboembolic Events | ||
|---|---|---|
| Variable | HR (95% CI; Univariable) | HR (95% CI; Multivariable) |
| Age | 1.23 (0.46–3.29, p = 0.020) | NS |
| Female sex | 1.14 (1.02–1.27, p = 0.687) | − |
| BMI | 0.86 (0.32–2.31, p = 0.764) | − |
| Hypertension | 0.94 (0.74–1.19, p = 0.599) | − |
| CAD | 1.26 (0.60–2.68, p = 0.540) | − |
| Heart failure | 1.35 (0.97–1.86, p = 0.071) | NS |
| CKD | 1.14 (0.83–1.56, p = 0.413) | − |
| Prior stroke/TIA | 1.28 (1.00–1.64, p = 0.061) | NS |
| Past bleeding | 1.14 (0.83–1.56, p = 0.413) | − |
| Glycated hemoglobin | 1.15 (1.04–1.27, p = 0.005) | 1.17 (1.06–1.29, p = 0.002) |
| Oral hypoglycemic agents | 1.28 (0.65–2.56, p = 0.440) | − |
| Antiplatelet drug (%) | 1.23 (0.46–3.29, p = 0.687) | − |
| Insulin therapy (%) | 1.65 (1.23–2.22, p = 0.003) | 1.76 (1.20–2.59, p = 0.004) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, V.; Attena, E.; Rago, A.; Melillo, E.; Di Micco, P.; Papa, A.A.; Napolitano, G.; D’Onofrio, A.; Golino, P.; Nigro, G. Clinical Outcome of Edoxaban vs. Vitamin K Antagonists in Patients with Atrial Fibrillation and Diabetes Mellitus: Results from a Multicenter, Propensity-Matched, Real-World Cohort Study. J. Clin. Med. 2020, 9, 1621. https://doi.org/10.3390/jcm9061621
Russo V, Attena E, Rago A, Melillo E, Di Micco P, Papa AA, Napolitano G, D’Onofrio A, Golino P, Nigro G. Clinical Outcome of Edoxaban vs. Vitamin K Antagonists in Patients with Atrial Fibrillation and Diabetes Mellitus: Results from a Multicenter, Propensity-Matched, Real-World Cohort Study. Journal of Clinical Medicine. 2020; 9(6):1621. https://doi.org/10.3390/jcm9061621
Chicago/Turabian StyleRusso, Vincenzo, Emilio Attena, Anna Rago, Enrico Melillo, Pierpaolo Di Micco, Andrea Antonio Papa, Giovanni Napolitano, Antonio D’Onofrio, Paolo Golino, and Gerardo Nigro. 2020. "Clinical Outcome of Edoxaban vs. Vitamin K Antagonists in Patients with Atrial Fibrillation and Diabetes Mellitus: Results from a Multicenter, Propensity-Matched, Real-World Cohort Study" Journal of Clinical Medicine 9, no. 6: 1621. https://doi.org/10.3390/jcm9061621