Comparative Safety of Bevacizumab, Ranibizumab, and Aflibercept for Treatment of Neovascular Age-Related Macular Degeneration (AMD): A Systematic Review and Network Meta-Analysis of Direct Comparative Studies

 , ,
, , 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
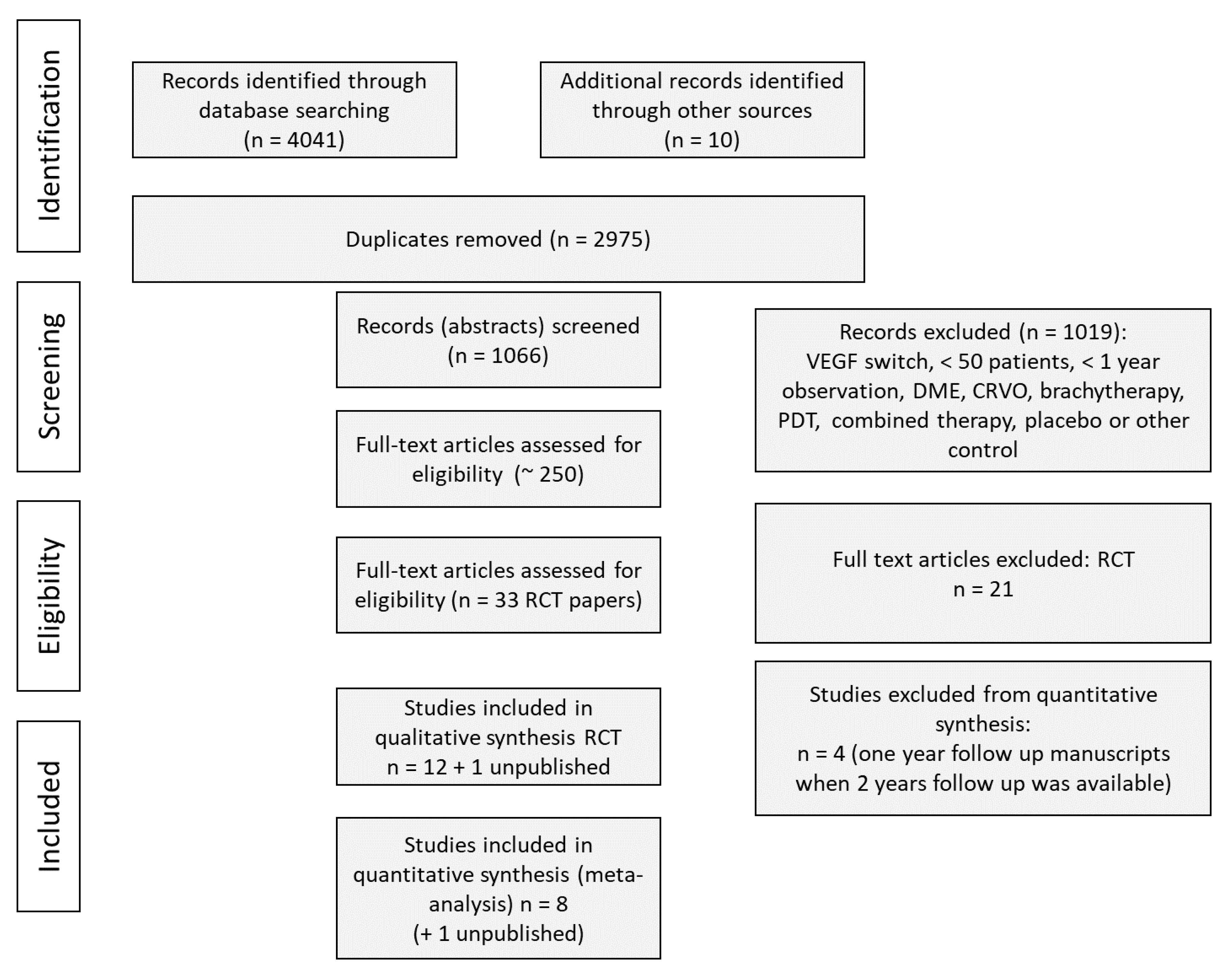
2.2. Selection of Studies
2.3. Inclusion and Exclusion Criteria
- (P) Study population: patients diagnosed with neovascular AMD
- (I) Interventions of interest: intravitreal BVZ, RBZ or AFB
- (C) Treatment comparisons: BVZ, RBZ and AFB
- (O) Outcomes of interest: any safety data reported (death, systemic and ocular serious adverse events)
- (T) Minimal follow-up period: 1 year
- (S) Studies were designed as RCTs. Studies published in English were eligible for inclusion in the review. Only studies that provided sufficient data of safety outcomes with at least 1-year follow-up and compared the safety of the following interventions: 1.25 mg BVZ or 0.5 mg RBZ monthly, as needed (pro re nata) or a treat-and-extend regimen, 2 mg AFB every 2 months or treat-and-extend regimen after 3 initial monthly doses (2q8), were included for network meta-analysis (NMA).
2.4. Data Extraction
2.5. Outcomes of Interest
2.6. Risk of Bias Assessment
2.7. Statistical Analysis
2.8. Sensitivity Analysis
3. Results
3.1. Characteristics of Included Studies and Quality Assessment
3.2. Risk of Bias Assessment
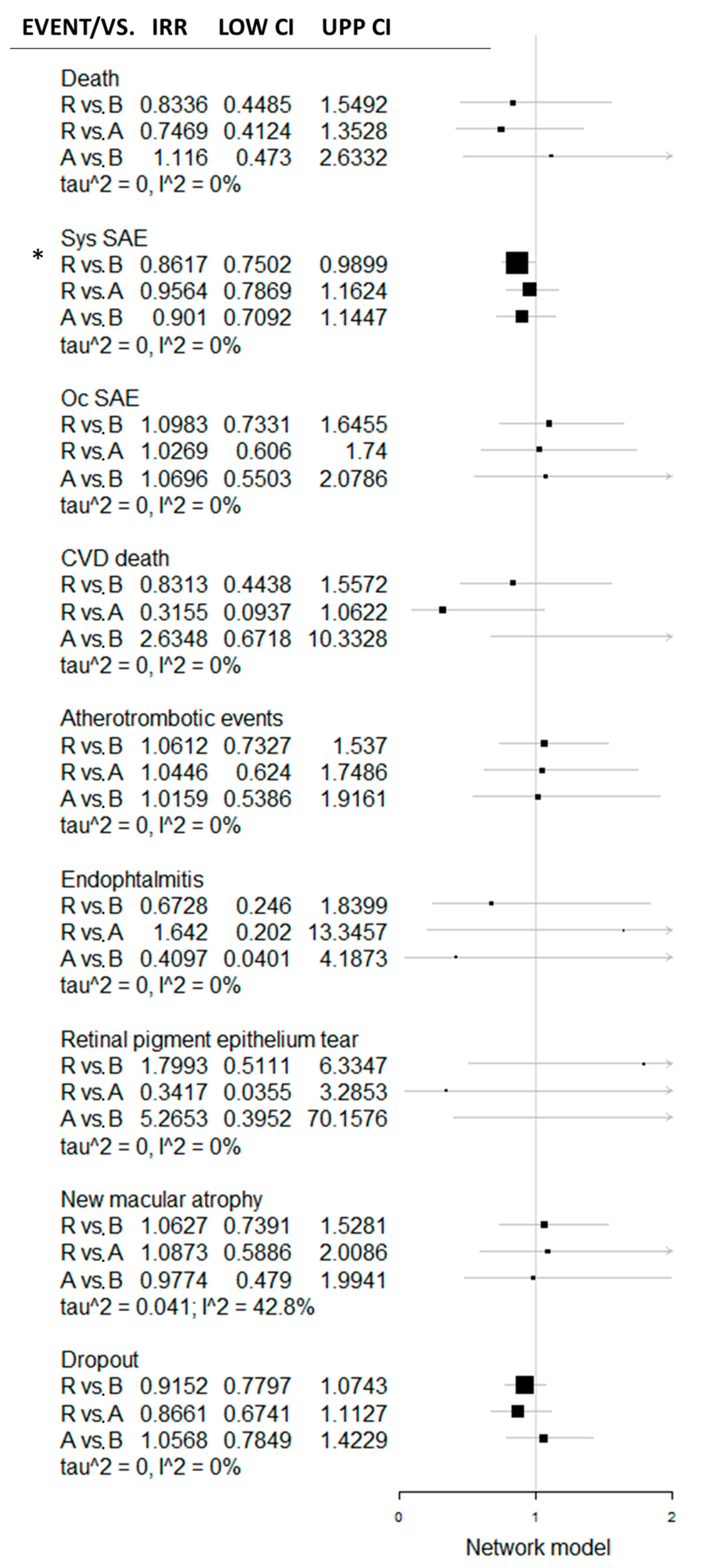
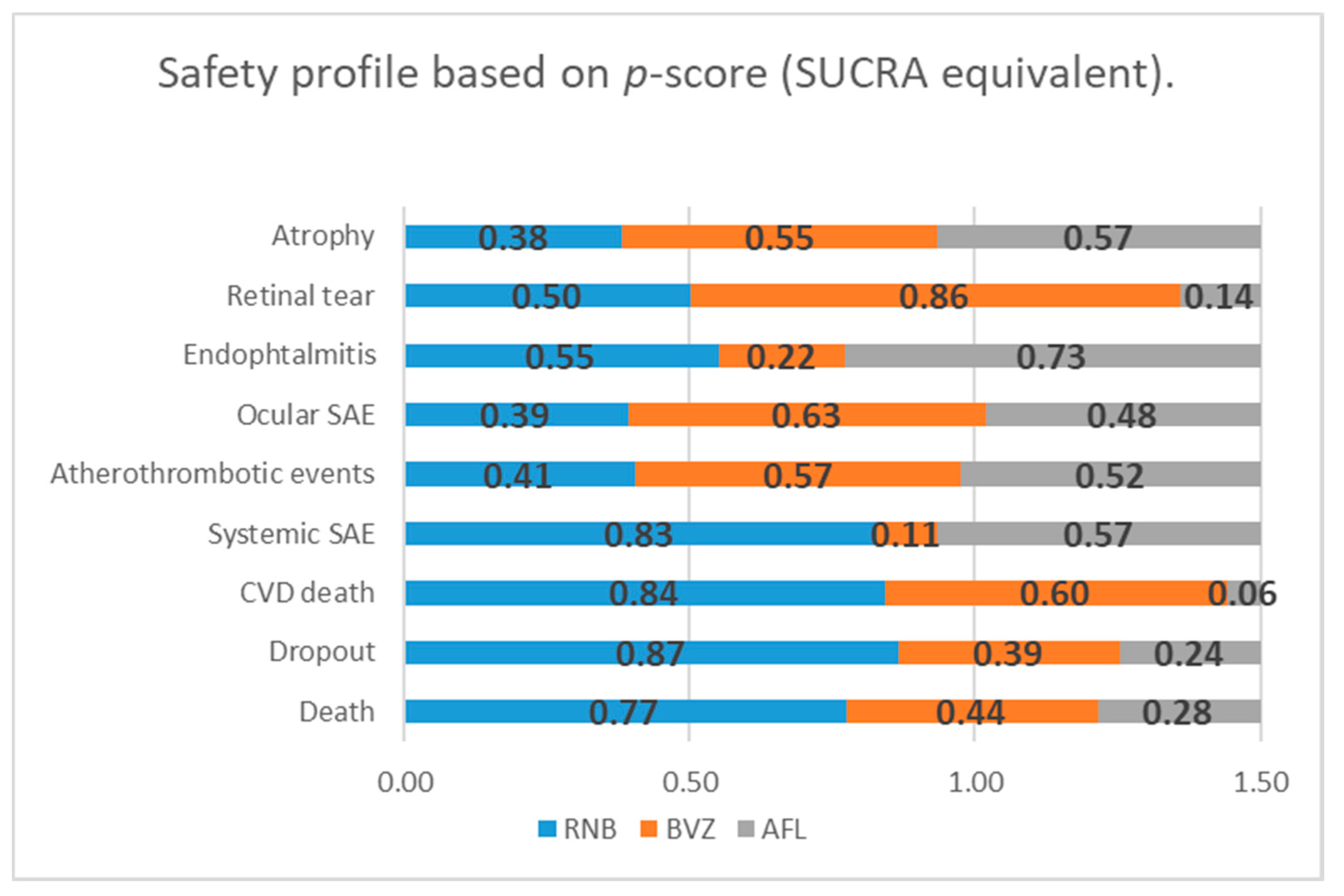
3.3. Safety Analysis
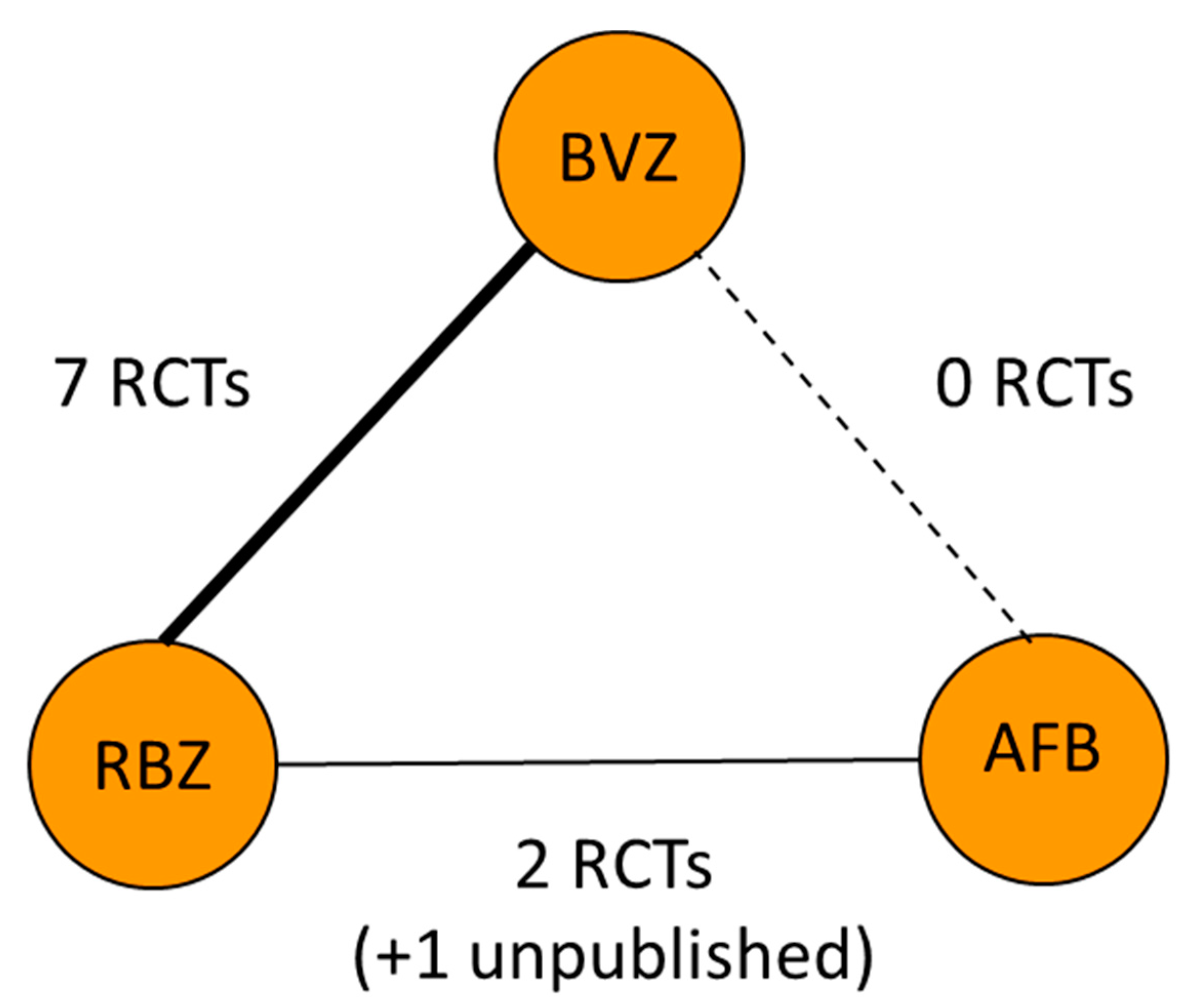
3.3.1. BVZ vs. RBZ
3.3.2. AFB vs. RBZ
3.3.3. AFB vs. BVZ
3.3.4. Synthetic Comparison of Three Options
4. Discussion
4.1. Limitations
4.2. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Chappelow, A.V.; Schachat, A.P. Neovascular age-related macular degeneration. In Retinal Pharmacotherapy, 1st, ed.; Nguyen, Q., Rodrigues, E., Farah, M., Mieler, W.F., Eds.; Saunders: Philadelphia, PA, USA, 2010; pp. 128–132. [Google Scholar]
- Wong, W.; Xinyi, S. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, 106–116. [Google Scholar] [CrossRef] [Green Version]
- Velez-Montoyaet, R.; Olson, J. Current knowledge and trends in age-related macular degeneration: Genetics, epidemiology, and prevention. Retina 2014, 34, 423–441. [Google Scholar] [CrossRef]
- Andrés-Guerrero, V.; Perucho-González, L. Current perspectives on the use of Anti-VEGF drugs as adjuvant therapy in Glaucoma. Adv. Ther. 2017, 34, 378–395. [Google Scholar] [CrossRef] [Green Version]
- Platania, C.B.; Di Paola, L.; Leggio, G.M.; Romano, G.L.; Filippo, D.; Salvatore, S.; Claudio, B. Molecular features of interaction between VEGFA and anti-angiogenic drugs used in retinal diseases: A computational approach. Front. Pharmacol. 2015, 6, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christoforidis, J.; Briley, K. Systemic biodistribution and intravitreal pharmacokinetic properties of bevacizumab, ranibizumab, and aflibercept in a nonhuman primate model. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5636–5645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Asten, F.; Michels, C. The cost-effectiveness of bevacizumab, ranibizumab and aflibercept for the treatment of age-related macular degeneration-A cost-effectiveness analysis from a societal perspective. PLoS ONE 2018, 13, e0197670. [Google Scholar] [CrossRef] [PubMed]
- Virgili, G.; Parravano, M. Anti-vascular endothelial growth factor for diabetic macular oedema: A network meta-analysis. Cochrane Database Syst. Rev. 2017, 22, CD007419. [Google Scholar] [CrossRef]
- Gemenetzi, M.; Lotery, A. Risk of geographic atrophy in age-related macular degeneration patients treated with intravitreal anti-VEGF agents. Eye 2016, 31, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ersoz, M.; Karacorlu, M. Retinal pigment epithelium tears: Classification, pathogenesis, predictors, and management. Surv. Ophthalmol. 2017, 62, 493–505. [Google Scholar] [CrossRef]
- Falavarjani, K.; Nguyen, Q. Adverse events and complications associated with intravitreal injection of anti-VEGF agents: A review of literature. Eye 2013, 27, 787–794. [Google Scholar] [CrossRef] [Green Version]
- Rücker, G.; Schwarzer, G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med. Res. Methodol. 2015, 15, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedrich, J.; Adhikari, N. Inclusion of zero total event trials in meta-analyses maintains analytic consistency and incorporates all available data. BMC Med. Res. Methodol. 2007, 7, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avery, R.; Castellarin, A. Systemic pharmacokinetics following intravitreal injections of ranibizumab, bevacizumab or aflibercept in patients with neovascular AMD. Br. J. Ophthalmol. 2014, 98, 1636–1641. [Google Scholar] [CrossRef] [PubMed]
- Avery, R.; Castellarin, A. Systemic pharmacokinetics and pharmacodynamics of intravitreal aflibercept, bevacizumab, and ranibizumab. Retina 2017, 37, 1847–1858. [Google Scholar] [CrossRef] [Green Version]
- Veroniki, A.A.; Straus, S.E. Is providing uncertainty intervals in treatment ranking helpful in a network meta-analysis? J. Clin. Epidemiol. 2018, 100, 122–129. [Google Scholar] [CrossRef]
- Zhang, X.; Guo, X. Comparison of bevacizumab and ranibizumab in age-related macular degeneration: A systematic review and meta-analysis. Int. J. Ophthalmol. 2014, 7, 355–364. [Google Scholar]
- Solomon, S.; Lindsley, K. Anti-vascular endothelial growth factor for neovascular age-related macular degeneration. Cochrane Database Syst. Rev. 2014, 8, CD005139. [Google Scholar] [CrossRef] [Green Version]
- Scott, L.; Chakravarthy, U. Gastrointestinal serious adverse events in patients treated with intraocular ranibizumab or bevacizumab for age-related choroidal neovascularisation, what do the recent trials tell us? Investig. Ophthalmol. Vis. Sci. 2014, 55, 1648. [Google Scholar]
- Moja, L.; Lucenteforte, E. Systemic safety of bevacizumab versus ranibizumab for neovascular age-related macular degeneration. Cochrane Database Syst. Rev. 2014, 15, CD011230. [Google Scholar]
- Thulliez, M.; Angoulvant, D. Cardiovascular events and bleeding risk associated with intravitreal antivascular endothelial growth factor monoclonal antibodies: Systematic review and meta-analysis. JAMA Ophthalmol. 2014, 132, 1317–1326. [Google Scholar] [CrossRef]
- Rodrigues, T.; Oliveira, M. Real-World results of aflibercept versus ranibizumab for the treatment of exudative AMD using a fixed regimen. BioMed Res. Int. 2018, 2018, 9276580. [Google Scholar]
- Doshi, R.; Leng, T. Reducing oral flora contamination of intravitreal injections with face mask or silence. Retina 2012, 32, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Baudin, F.; Benzenine, E. Association of acute endophthalmitis with intravitreal injections of corticosteroids or anti-vascular growth factor agents in a nationwide study in France. JAMA Ophthalmol. 2018, 136, 1352–1358. [Google Scholar] [CrossRef] [Green Version]
- Marticorena, J.; Romano, V. Sterile endophthalmitis after intravitreal injections. Mediat. Inflamm. 2012, 2012, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Forooghian, F.; Albiani, D. Comparison of endophthalmitis rates following intravitreal injection of compounded bevacizumab, ranibizumab, and aflibercept. Can. J. Ophthalmol. 2017, 52, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Chhabra, M. Tears of the retinal pigment epithelium—A review. Delhi. J. Ophthalmol. 2017, 27, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Sarraf, D.; Joseph, A. Retinal pigment epithelial tears in the era of intravitreal pharmacotherapy: Risk factors, pathogenesis, prognosis and treatment (an American Ophthalmological Society thesis). Trans. Am. Ophthalmol. Soc. 2014, 112, 142–159. [Google Scholar]
- Enslow, R.; Bhuvanagiri, S. Association of Anti-VEGF Injections with progression of geographic atrophy. Ophthalmol. Eye Dis. 2016, 8, 31–32. [Google Scholar] [CrossRef] [Green Version]
- Subramanian, M.; Abedi, G. Bevacizumab vs. ranibizumab for age-related macular degeneration: 1-year outcomes of a prospective, double-masked randomised clinical trial. Eye 2010, 24, 1708–1715. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bevacizumab (BVZ) | Ranibizumab (RBZ) | Aflibercept (AFB) | |
|---|---|---|---|
| Manufacturer | Avastin; Genetech, South San Francisco, CA, USA | Lucentis; Genetech, South San Francisco, CA, USA | Eylea; Regeneron Pharmaceuticals, Tarrytown, NY, USA |
| Type of molecule | Full-size recombinant humanized IgG1 kappa monoclonal antibody | Fab fragment of a recombinant humanized IgG1 kappa isotype murine monoclonal antibody | Fusion protein of the second Ig domain of human vascular endothelial growth factor receptor 1 (VEGFR-1) and the third Ig-binding domain of human VEGFR-2 with the constant fragment crystallizable portion of the human IgG1 |
| Molecular weight | 149 kDa | 48 kDa | 115 kDa |
| Picture |  |  |  |
| Comments | N-glycosylated in its Fc region | Not glycosylated | NA |
| Production | Mammalian cell lines CHO DP-12 | Escherichia coli cells, recombinant DNA technology | Hamster ovary cells |
| Receptor-ligand interaction | Against all isoforms of VEGF-A | Against all isoforms of VEGF-A | Binds to all isoforms of VEGF-A (higher affinity than BVZ and RBZ); also binding to VEGF-B and Placental Growth Factor (PIGF). |
| Authorization in the USA | FDA in 2005, colorectal and breast cancers, used in AMD off-label | FDA in 2006, AMD | FDA—2011, AMD |
| Reason for Exclusion | Number of Articles Excluded |
|---|---|
| All references identified | 4043 |
| Duplicates | 2975 |
| Unique references | 1068 |
| Excluded unique references | |
| Reviews | 22 |
| Brachytherapy | 5 |
| Combined anti-VEGF treatment | 8 |
| Central retinal vein occlusion (CRVO) | 15 |
| Diabetes macular edema | 61 |
| Less than one-year follow-up | 31 |
| Mixed diagnosis AMD and macular degeneration (MD) caused diabetic macular edema (DME)/ Polypoidal choroidal vasculopathy (PCV) | 7 |
| Photodynamic therapy(PDT) | 5 |
| Switch | 28 |
| Other reasons for exclusion (no direct comparison, secondary analysis, observational studies, etc.) | 747 |
| Not published as a full manuscript (no safety data available) | 13 |
| Included unique references | |
| RCT | 33 (12 unique studies) |
| Author Study | Treatment Groups | Regimen Doses | Following Months | Number of Patients: BVZ/RBZ or AFB/RBZ | Age, Years |
|---|---|---|---|---|---|
| CATT 1 (2011) | BVZ OR RBZ | 0.50 mg/in 0.05 mL RBZ or 1.25 mg/0.05 mL BVZ cont/discont | 12 m | 586/599 | 79.7/78.8 |
| CATT 2 | BVZ OR RBZ | 0.50 mg/in 0.05 mL RBZ or 1.25 mg/0.05 mL BVZ cont/discont | 24 m | 586/599 | 79.7/78.8 |
| IVAN 2012 | BVZ OR RBZ | 1.1.1.1 cont/discont regimen BRZ (0.5 mg) or BVZ (1.25 mg) | 12 m | 296/314 | 77.8/77.7 |
| IVAN 2013 | BVZ OR RBZ | 1.1.1.1 cont/discont regimen BRZ (0.5 mg) or BVZ (1.25 mg) | 24 m | 296/314 | 77.8/77.7 |
| GEFAL 2013 | BVZ OR RBZ | BVZ 1.25 mg or RBZ 0.50 mg in 0.05 mL of solution following treat-and-extend protocol | 12 m | 191/183 | 79.6/78.7 |
| BRAMD 2016 | BVZ OR RBZ | Monthly 1.25 mg BVZ or 0.5 mg RBZ | 12 m | 161/166 | 79/78 |
| LUCAS 2015 | BVZ OR RBZ | RBZ 0.5 mg or BVZ 1.25 mg following a treat-and-extend protocol | 24 m | 213/218 | 62/78 |
| MANTA 2013 | BVZ OR RBZ | RBZ 0.5 mg or BVZ 1.25 mg following a treat-and-extend protocol | 12 m | 154/163 | 76.7/77.6 |
| Biswas 2011 | BVZ OR RBZ | RBZ 0.5 mg or BVZ 1.25 mg monthly | 18 m | 50/54 | 64.4/63.5 |
| VIEW 1 | AFB OR RBZ | AFB 0.5 mg monthly (0.5q4), 2 mg monthly (2q4), 2 mg every 2 months after 3 initial monthly doses (2q8), or RBZ 0.5 mg monthly (Rq4) | 24 m | 911/304 | 78/78 |
| VIEW 2 | 24 m | 913/291 | 74/73 | ||
| RIVAL | AFB OR RBZ | AFB 2.0 mg OR 0.5 mg RBZ in a treat-and-extend regimen | 24 m | 139/142 | 76.6/78.7 |
| CATT 2 | IVAN2 | Gefal | BRAMD | LUCAS2 | MANTA | Biswas | VIEW12 | RIVAL2 | |
|---|---|---|---|---|---|---|---|---|---|
| patients dead | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| patients with ≥ 1 systemic SAE | Y | Y | Y | N | Y | Y | Y | Y | Y |
| patients dead from cardiovascular (CV) event | Y | Y | Y | N | Y | N | Y | Y | Y |
| patients with ≥ 1 venous thrombotic events | Y | Y | Y | N | Y | Y | Y | N | N/av |
| patients with ≥ 1 atherotrombotic events | Y | Y | Y | N | Y | Y | Y | Y | Y |
| patients with ≥1 ocular SAE | CATT1 only | Y | Y | N | N | Y | Y | Y | N/av |
| endophtalmitis | Y | N | Y | N | Y | Y | Y | Y | Y |
| pseudoendophtalmitis | Y | N | N | N | Y | Y | Y | N | N/av |
| patients with retinal pigment epithelium tear | CATT1 only | Y | N | N | Y | Y | Y | Y | N/av |
| new macular atrophy | Y | Y | N | N | N | N | N | Y | Y |
| dropout rate | Y | Y | Y | Y | Y | Y | Y | Y | Y |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plyukhova, A.A.; Budzinskaya, M.V.; Starostin, K.M.; Rejdak, R.; Bucolo, C.; Reibaldi, M.; Toro, M.D. Comparative Safety of Bevacizumab, Ranibizumab, and Aflibercept for Treatment of Neovascular Age-Related Macular Degeneration (AMD): A Systematic Review and Network Meta-Analysis of Direct Comparative Studies. J. Clin. Med. 2020, 9, 1522. https://doi.org/10.3390/jcm9051522
Plyukhova AA, Budzinskaya MV, Starostin KM, Rejdak R, Bucolo C, Reibaldi M, Toro MD. Comparative Safety of Bevacizumab, Ranibizumab, and Aflibercept for Treatment of Neovascular Age-Related Macular Degeneration (AMD): A Systematic Review and Network Meta-Analysis of Direct Comparative Studies. Journal of Clinical Medicine. 2020; 9(5):1522. https://doi.org/10.3390/jcm9051522
Chicago/Turabian StylePlyukhova, Anna A., Maria V. Budzinskaya, Kirill M. Starostin, Robert Rejdak, Claudio Bucolo, Michele Reibaldi, and Mario D. Toro. 2020. "Comparative Safety of Bevacizumab, Ranibizumab, and Aflibercept for Treatment of Neovascular Age-Related Macular Degeneration (AMD): A Systematic Review and Network Meta-Analysis of Direct Comparative Studies" Journal of Clinical Medicine 9, no. 5: 1522. https://doi.org/10.3390/jcm9051522