An Unsupervised Data-Driven Model to Classify Gait Patterns in Children with Cerebral Palsy

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Model Input
2.3. Data-Driven Model
2.4. Statistical Analysis
2.5. Relationships between AFO Types and Gait Pattern
3. Results
3.1. Data-Driven Model
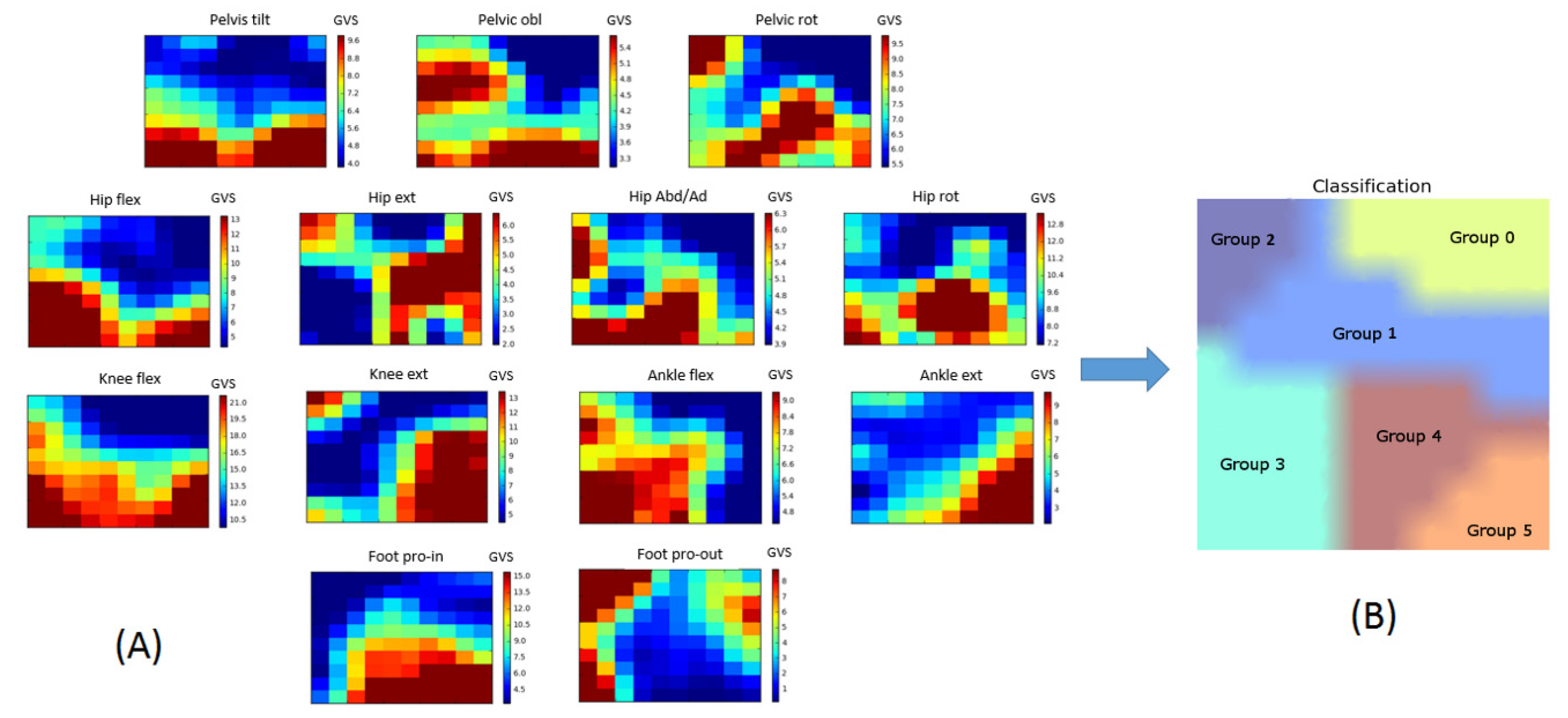
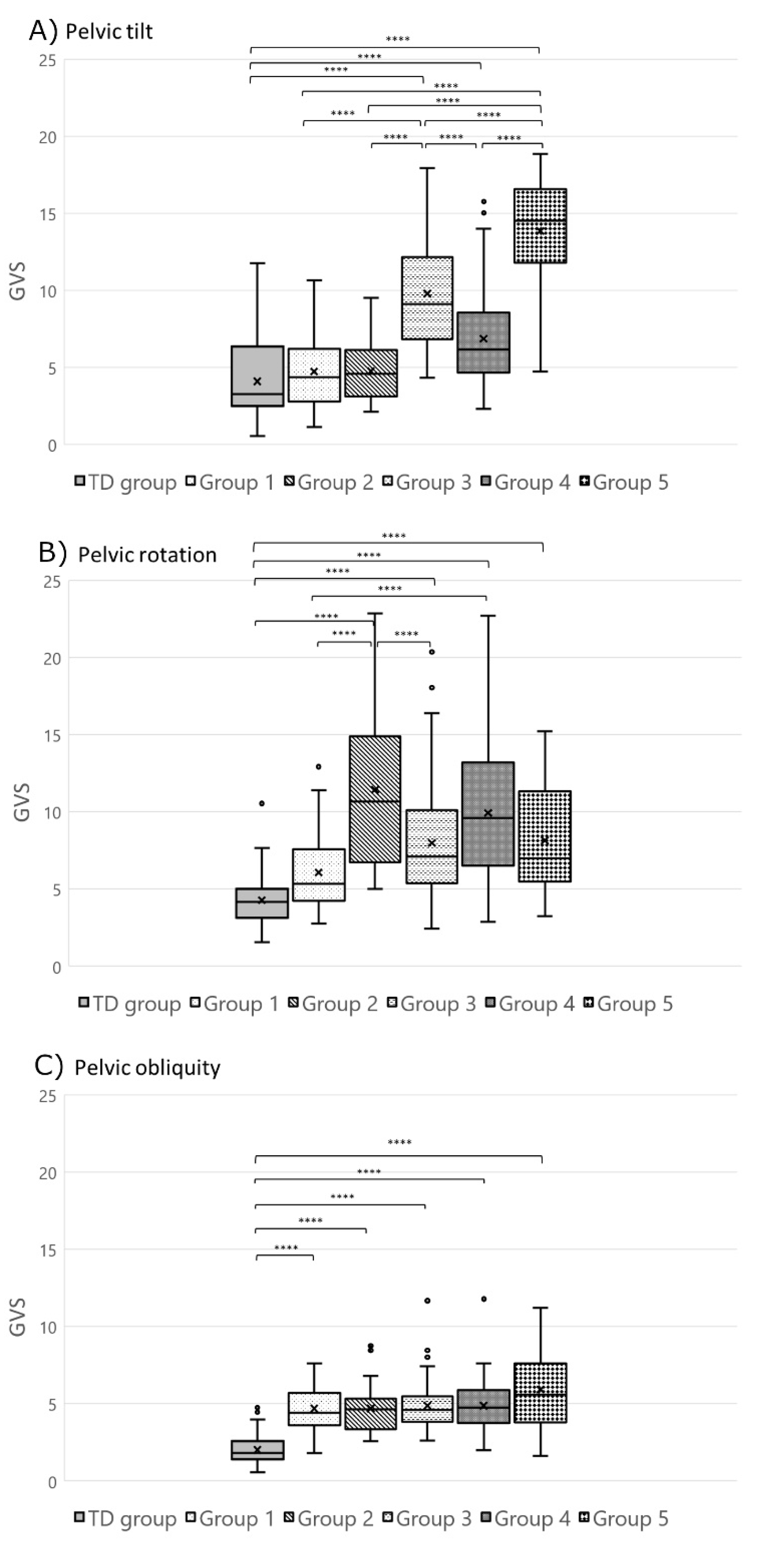
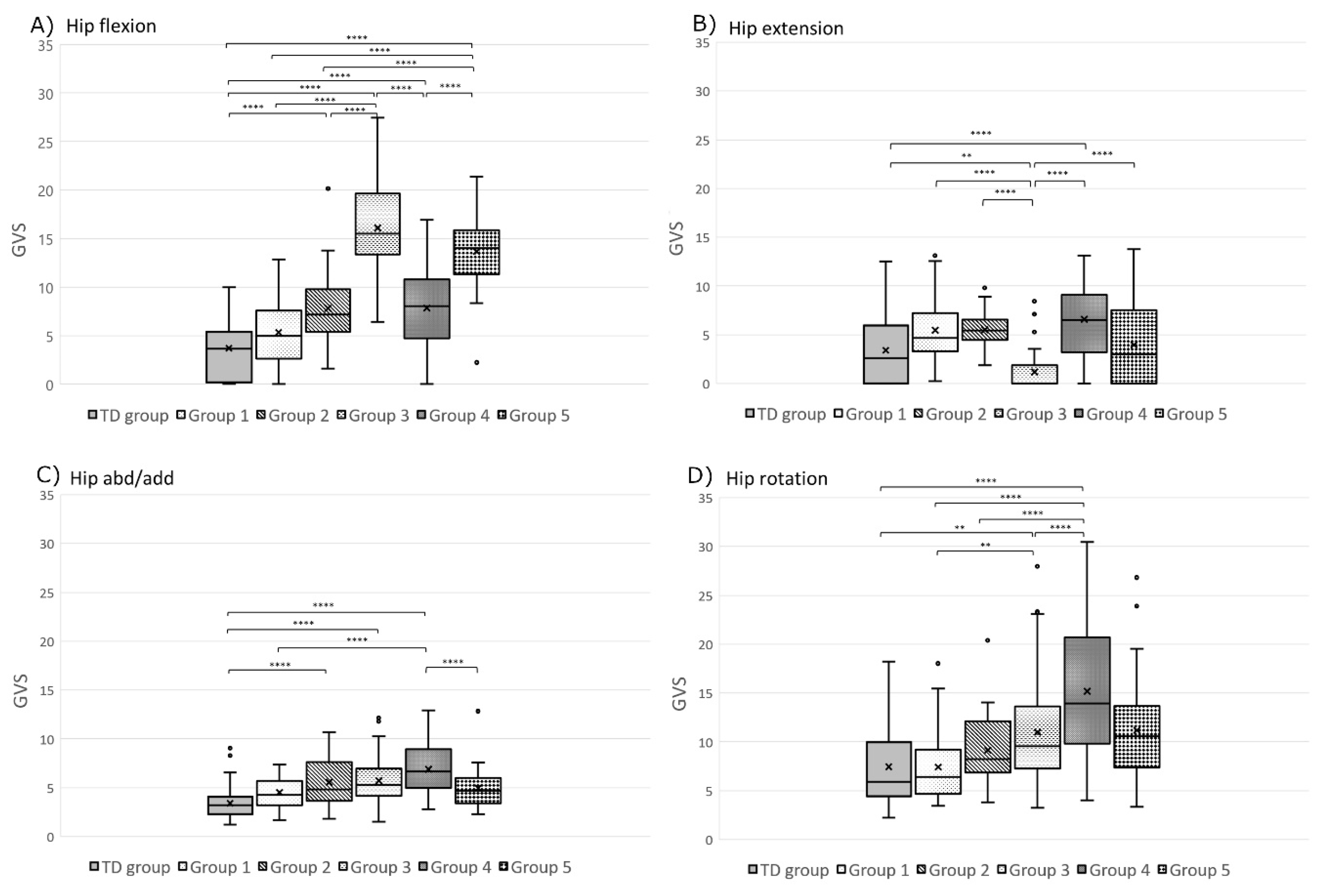
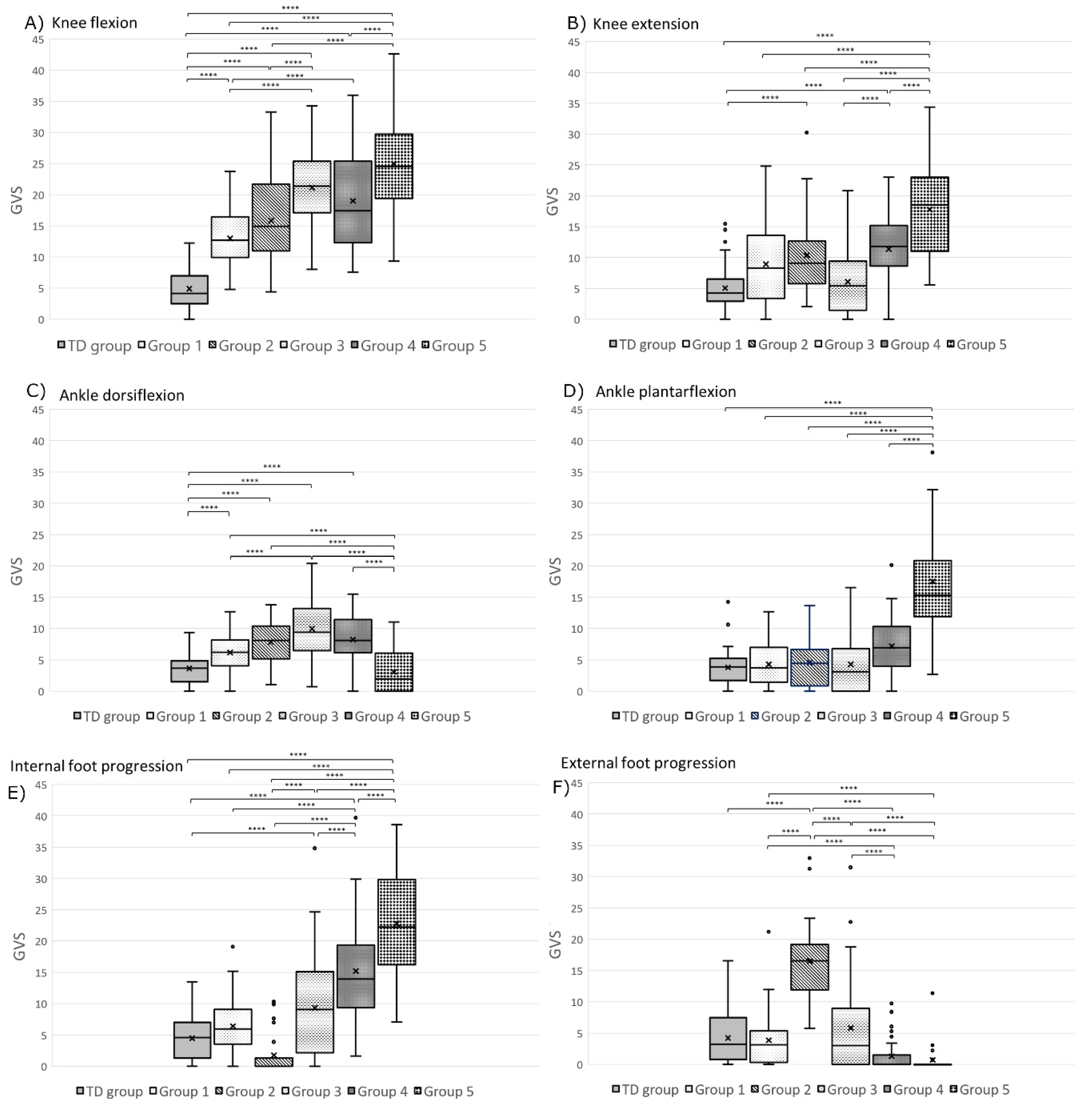
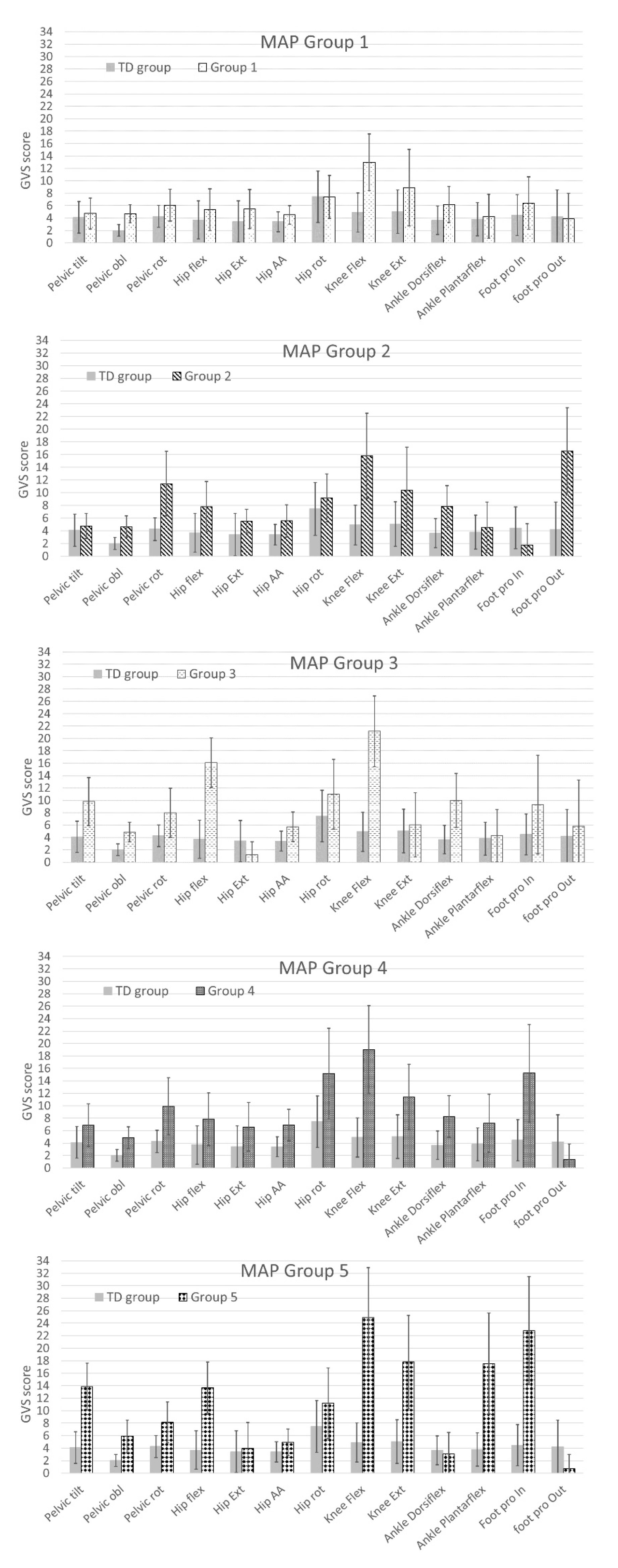
- Group 2: Limbs classified in Group 2 (n = 24) had a statistically significantly greater external foot progression angle GVS throughout the gait cycle compared to all the other groups (Figure 6). Group 2 limbs had greater GVSs than the TD children group for the following joint motions: pelvic rotation (p < 0.0001), pelvic obliquity (p < 0.0001), hip flexion (p < 0.0001), hip add/abd (p = 0.001), knee flexion (p < 0.0001), knee extension (p = 0.002), and ankle dorsiflexion (p < 0.0001) (Figure 4, Figure 5 and Figure 6).
- Group 3: Limbs in Group 3 (n = 56) had statistically significantly greater hip flexion GVSs than all the other groups (Figure 5). They also had a higher pelvic tilt (p < 0.0001), pelvic obliquity (p < 0.0001), pelvic rotation (p < 0.0001), hip extension (p = 0.006), hip add/abd (p < 0.0001), hip rotation (p = 0.008), knee flexion (p < 0.0001), ankle dorsiflexion (p < 0.0001), and internal foot progression (p = 0.002) than the limbs of TD children (Figure 4, Figure 5 and Figure 6).
- Group 4: Limbs in Group 4 (n = 39) displayed statistically significantly greater hip rotation GVSs than the other groups (Figure 5). Limbs in this group also had a greater GVS than TD children in all gait features (p < 0.0001) except for ankle plantar flexion (p = 0.009) and external foot progression (p = 0.131) (Figure 4, Figure 5 and Figure 6).
- Group 5: Limbs classified in Group 5 (n = 28) had statistically significantly greater pelvic tilt, knee extension, ankle plantar flexion, and internal foot progression GVSs than all the other groups (p < 0.0001) (Figure 4 and Figure 6). Group 5 also had greater pelvic obliquity and rotation (p < 0.0001) and hip and knee flexion (p < 0.0001) than TD children (Figure 4, Figure 5 and Figure 6).
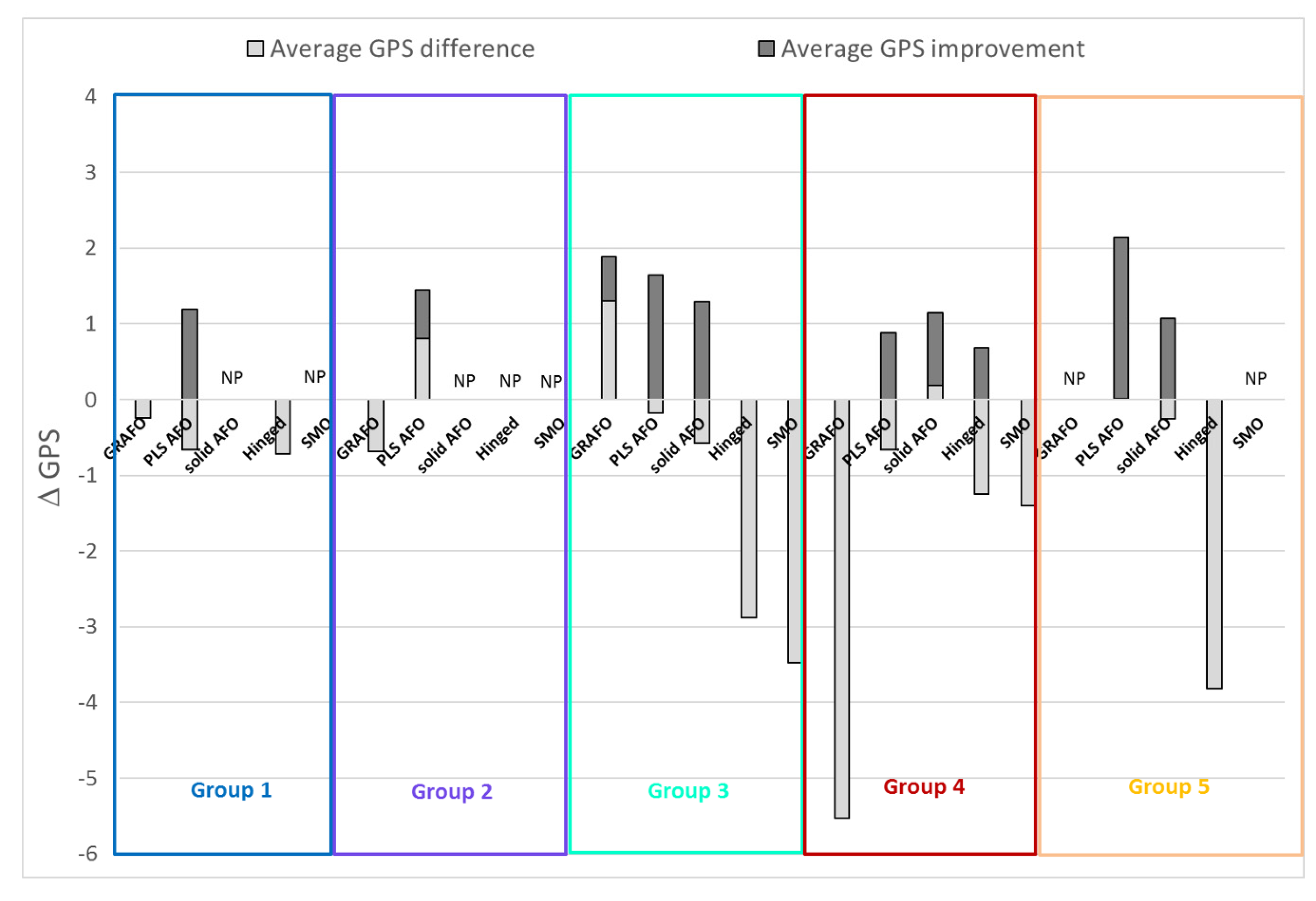
3.2. Relationships between Orthosis Prescription and Gait Pattern
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Morris, C.; Bowers, R.; Ross, K.; Stevens, P.; Phillips, D. Orthotic management of cerebral palsy: Recommendations from a consensus conference. NeuroRehabilitation 2011, 28, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridgewell, E.; Dobson, F.; Bach, T.; Baker, R. A systematic review to determine best practice reporting guidelines for AFO interventions in studies involving children with cerebral palsy. Prosthet. Orthot. Int. 2010, 34, 129–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bregman, D.J.J.; Rozumalski, A.; Koops, D.; de Groot, V.; Schwartz, M.; Harlaar, J. A new method for evaluating ankle foot orthosis characteristics: BRUCE. Gait Posture 2009, 30, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Graham, H.K.; Rosenbaum, P.; Paneth, N.; Dan, B.; Lin, J.-P.; Damiano, D.L.; Becher, J.G.; Gaebler-Spira, D.; Colver, A.; Reddihough, D.S.; et al. Cerebral palsy. Nat. Rev. Dis. Prim. 2016, 2, 15082. [Google Scholar] [CrossRef] [PubMed]
- Kerkum, Y.L.; Harlaar, J.; Buizer, A.I.; van den Noort, J.C.; Becher, J.G.; Brehm, M.-A. An individual approach for optimizing ankle-foot orthoses to improve mobility in children with spastic cerebral palsy walking with excessive knee flexion. Gait Posture 2016, 46, 104–111. [Google Scholar] [CrossRef]
- Brehm, M.; Harlaar, J.; Schwartz, M. Effect of ankle-foot orthoses on walking efficiency and gait in children with cerebral palsy. J. Rehabil. Med. 2008, 40, 529–534. [Google Scholar] [CrossRef] [Green Version]
- Gage, J.R. The Identification and Treatment of Gait Problems in Cerebral Palsy; Mac Keith Press: London, UK, 2009; ISBN 9781898683650. [Google Scholar]
- Baker, R.; McGinley, J.L.; Schwartz, M.H.; Beynon, S.; Rozumalski, A.; Graham, H.K.; Tirosh, O. The Gait Profile Score and Movement Analysis Profile. Gait Posture 2009, 30, 265–269. [Google Scholar] [CrossRef]
- Schutte, L.M.; Narayanan, U.; Stout, J.L.; Selber, P.; Gage, J.R.; Schwartz, M.H. An index for quantifying deviations from normal gait. Gait Posture 2000, 11, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, M.H.; Rozumalski, A. The gait deviation index: A new comprehensive index of gait pathology. Gait Posture 2008, 28, 351–357. [Google Scholar] [CrossRef]
- Ferber, R.; Osis, S.T.; Hicks, J.L.; Delp, S.L. Gait biomechanics in the era of data science. J. Biomech. 2016, 49, 3759–3761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinbolt, J.A.; Fox, M.D.; Schwartz, M.H.; Delp, S.L. Predicting outcomes of rectus femoris transfer surgery. Gait Posture 2009, 30, 100–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, J.L.; Delp, S.L.; Schwartz, M.H. Can biomechanical variables predict improvement in crouch gait? Gait Posture 2011, 34, 197–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ries, A.J.; Novacheck, T.F.; Schwartz, M.H. A data driven model for optimal orthosis selection in children with cerebral palsy. Gait Posture 2014, 40, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Collins, T.D.; Ghoussayni, S.N.; Ewins, D.J.; Kent, J.A. A six degrees-of-freedom marker set for gait analysis: Repeatability and comparison with a modified Helen Hayes set. Gait Posture 2009, 30, 173–180. [Google Scholar] [CrossRef] [PubMed]
- SOMPY: A Python Library for Self Organizing Map (SOM) 2014. Available online: https://github.com/sevamoo/SOMPY (accessed on 9 January 2017).
- Kohonen, T. Essentials of the self-organizing map. Neural Netw. 2013, 37, 52–65. [Google Scholar] [CrossRef]
- Jain, A.K.; Dubes, R.C. Algorithms for Clustering Data; Prentice Hall: Upper Saddle River, NJ, USA, 1988; ISBN 013022278X. [Google Scholar]
- Baker, R.; McGinley, J.L.; Schwartz, M.; Thomason, P.; Rodda, J.; Graham, H.K. The minimal clinically important difference for the Gait Profile Score. Gait Posture 2012, 35, 612–615. [Google Scholar] [CrossRef] [PubMed]
- Rodda, J.; Graham, H.K. Classification of gait patterns in spastic hemiplegia and spastic diplegia: A basis for a management algorithm. Eur. J. Neurol. 2001, 8, 98–108. [Google Scholar] [CrossRef]
- Gage, J.R. Gait Analysis in Cerebral Palsy; Mac Keith Press: London, UK, 1991. [Google Scholar]
- Wren, T.A.L.; Rethlefsen, S.; Kay, R.M. Prevalence of specific gait abnormalities in children with cerebral palsy: Influence of cerebral palsy subtype, age, and previous surgery. J. Pediatr. Orthop. 2005, 25, 79–83. [Google Scholar]
- Buckon, C.E.; Thomas, S.S.; Jakobson-Huston, S.; Moor, M.; Sussman, M.; Aiona, M. Comparison of three ankle–foot orthosis configurations for children with spastic diplegia. Dev. Med. Child Neurol. 2004, 46, 590–598. [Google Scholar] [CrossRef]
- Scalona, E.; Di Marco, R.; Castelli, E.; Desloovere, K.; Van Der Krogt, M.; Cappa, P.; Rossi, S. Inter-laboratory and inter-operator reproducibility in gait analysis measurements in pediatric subjects. Int. Biomech. 2019, 6, 19–33. [Google Scholar] [CrossRef] [Green Version]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Eddison, N.; Chockalingam, N. The effect of tuning ankle foot orthoses–footwear combination on the gait parameters of children with cerebral palsy. Prosthet. Orthot. Int. 2013, 37, 95–107. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prescription for Each Limb in Each Group | |||||||
|---|---|---|---|---|---|---|---|
| # of Llimbs | No Orthosis | GRAFO | PLS AFO | Solid/Rigid AFO | Hinged AFO | Others | Total |
| Group 1 | 23 | 1 | 23 | 0 | 2 | 0 | 49 |
| Group 2 | 8 | 2 | 14 | 0 | 0 | 0 | 24 |
| Group 3 | 13 | 5 | 25 | 8 | 1 | 4 | 56 |
| Group 4 | 11 | 1 | 17 | 6 | 3 | 1 | 39 |
| Group 5 | 2 | 0 | 18 | 7 | 1 | 0 | 28 |
| Total | 57 | 9 | 97 | 21 | 7 | 5 | 196 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choisne, J.; Fourrier, N.; Handsfield, G.; Signal, N.; Taylor, D.; Wilson, N.; Stott, S.; Besier, T.F. An Unsupervised Data-Driven Model to Classify Gait Patterns in Children with Cerebral Palsy. J. Clin. Med. 2020, 9, 1432. https://doi.org/10.3390/jcm9051432
Choisne J, Fourrier N, Handsfield G, Signal N, Taylor D, Wilson N, Stott S, Besier TF. An Unsupervised Data-Driven Model to Classify Gait Patterns in Children with Cerebral Palsy. Journal of Clinical Medicine. 2020; 9(5):1432. https://doi.org/10.3390/jcm9051432
Chicago/Turabian StyleChoisne, Julie, Nicolas Fourrier, Geoffrey Handsfield, Nada Signal, Denise Taylor, Nichola Wilson, Susan Stott, and Thor F. Besier. 2020. "An Unsupervised Data-Driven Model to Classify Gait Patterns in Children with Cerebral Palsy" Journal of Clinical Medicine 9, no. 5: 1432. https://doi.org/10.3390/jcm9051432