Listening in Noise Remains a Significant Challenge for Cochlear Implant Users: Evidence from Early Deafened and Those with Progressive Hearing Loss Compared to Peers with Normal Hearing


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Hebrew Version of the Matrix Sentence-In-Noise Test
2.3. Word Recognition in Quiet
2.4. Language Assessment
2.5. Cognitive Assessment
2.6. Apparatus
2.7. Study Design
2.8. Data Analysis
3. Results
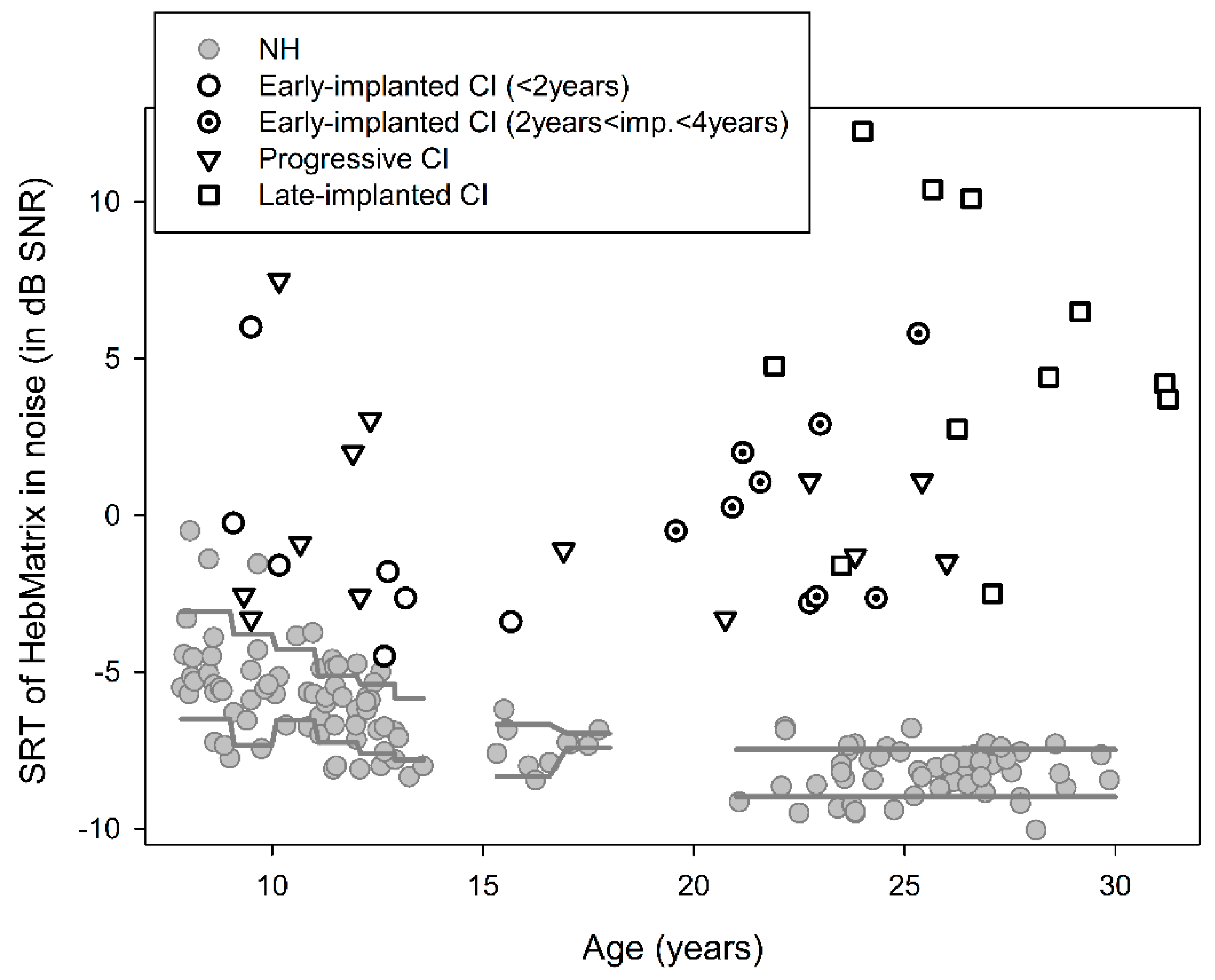
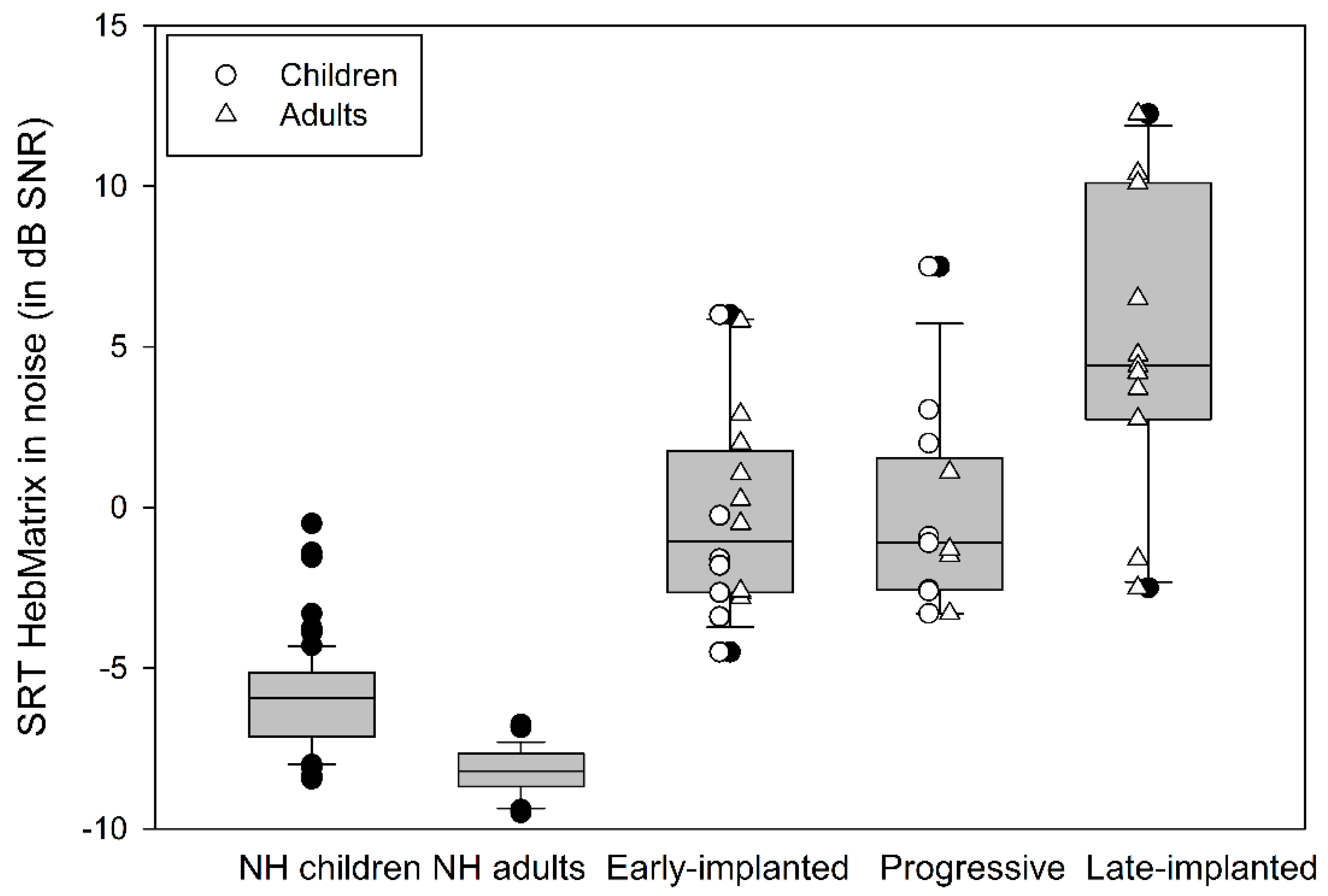
3.1. Sentence Recognition in Noise
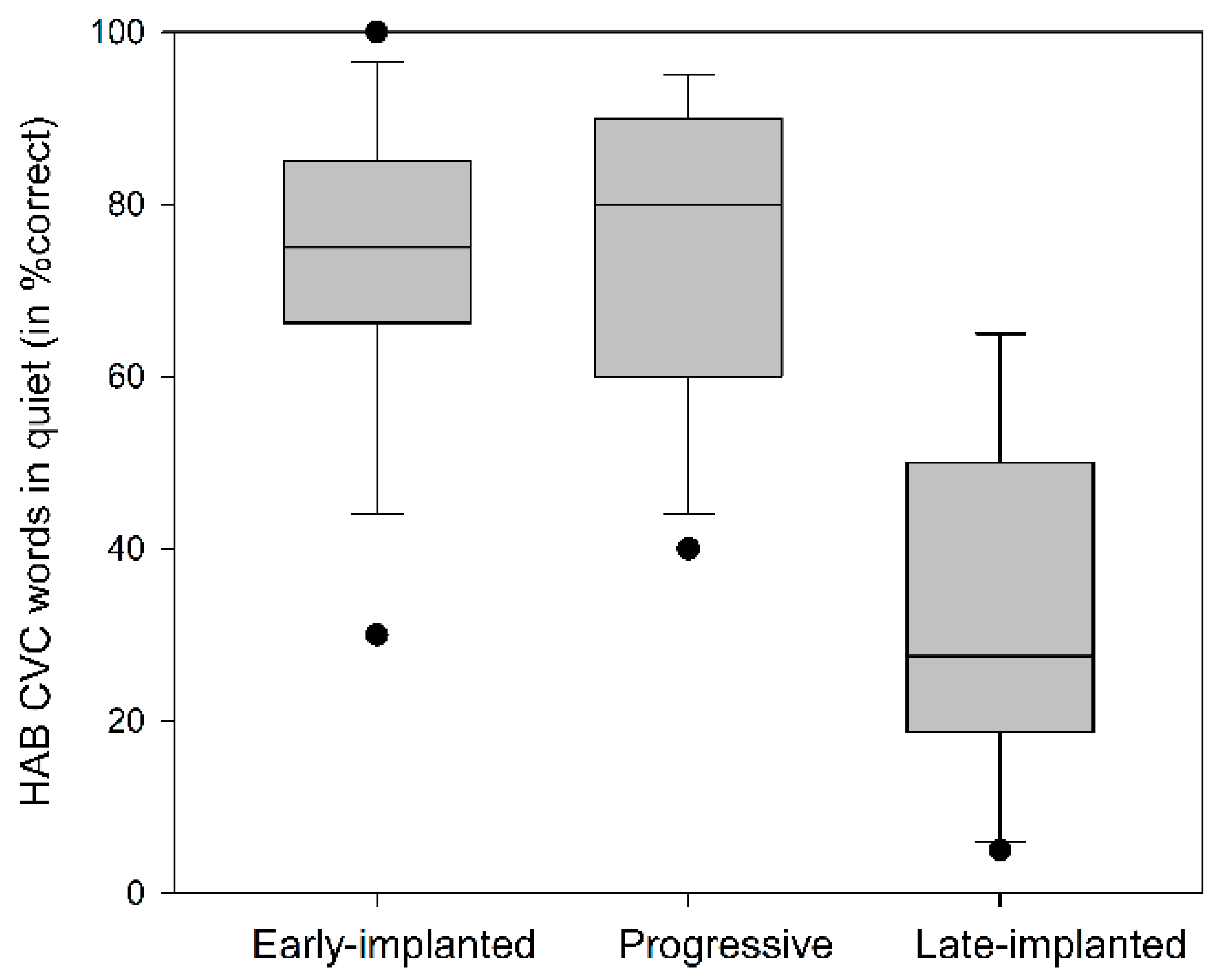
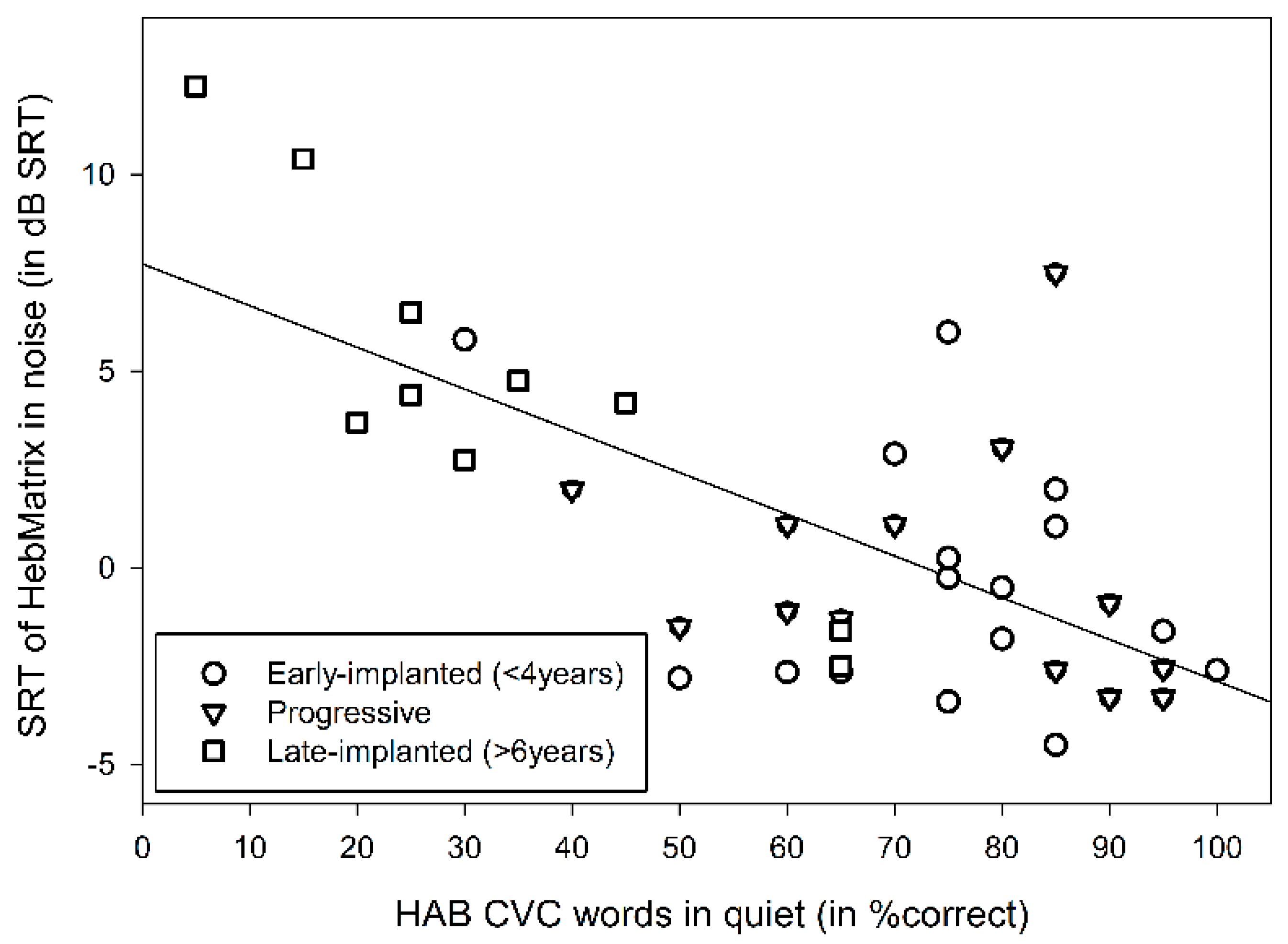
3.2. Word Recognition in Quiet
3.3. Linguistic and Cognitive Factors
4. Discussion
Limitations and Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Participants | Purpose | Method of Testing SIN | SIN Results |
|---|---|---|---|---|
| Bugannim et al., 2019 | NH & CI Young-adults | Assess the effect of auditory training on SIN perception | Hebrew Matrix test sentences in speech-shaped noise; adaptive SNR | CI: Mean SRTn of +1.3 ± 0.6 dB, range: −3.7 to +14 dB. NH: Mean SRTn of −8.1 ± 0.5 dB, range: −10.1 to −6.3 dB |
| Davidson et al., 2019 | CI Children | Identify an optimal level & duration of acoustic experience to facilitate language development | Lexical Neighborhood test (LNT) Words in four-talkers noise; fixed SNR of + 8 | CI: 63% correct identification |
| Goldsworthy & Markle 2019 | NH, HA, & CI Children | Assess the effect of different types of noise on SIN perception | Words in speech-spectrum noise, 2-talker babble, and instrumental music; adaptive SNR | CI: Mean SRTn of −5.7, −1.2, & −13.3 dB. NH: Mean SRTn of −9.3, −11.4 & −23.8, for the speech-spectrum noise, 2-talker babble, and instrumental music, respectively |
| Mishra & Boddupally, 2018 | NH & CI Children | Assess the effect of working memory training on SIN perception | Digit-triplets in speech shaped noise; adaptive SNR | CI: Mean SRTn of 15.52 dB, range: +9 to +21.01 dB NH: Mean SRTn of −8.81 dB, range: −11.50 to −6.50 |
| Ching et al., 2018 | CI Children | Assess factors that influence SIN perception | Words in a closed-set & BKB: open-set sentences test in babble noise; adaptive SNR | CI: Mean SRTn of 4.0–6.9 dB |
| Choi et al., 2017 | Bilateral & bimodal CI Children | Compare performance between bimodal & bilateral | Words in babble noise; fixed SNR of +5 | Bilateral CI: 52.7% ± 25.9% correct identification, Bimodal CI: 40.7% ± 28.7% correct identification |
| Cusumano et al., 2017 | Prelingually & postlingually deafened CI adults | Characterize the performance plateau after unilateral cochlear implantation | HINT or AzBio sentence tests; fixed SNR of +10 | Prelingual CI range: from 0% to 90% correct identification at 3 months, 1-year and 2-year post implantation testing |
| Eisenberg et al., 2016 | CI Children (CDaCI study) | Investigate associations between speech perception & spoken language | HINT-C sentences in speech shaped noise; fixed SNRs of +5 & +10 | CI: 52% of the sample had achieved >50% correct identification in the +10 and +5 SNR conditions at 3-year post activation testing |
| Friedmann et al., 2015 | CI Adolescents | Examine factors affecting outcomes for sequential bilateral CI | HINT sentence test; fixed SNR of + 10 | CI: 92.8% correct identification with both CIs |
| Van Wieringen & Wouters 2015 | CI Children | Assess Predictive factors for spoken language, and auditory & speech perception | CVC words in speech-weighted noise; adaptive SNR | CI: SRTn range from −6 dB to +8 dB |
| Caldwell & Nittrouer, 2013 | NH & CI Children | Examine phonological, language, and cognitive skills in CI children | Words in flat spectrum noise; fixed SNRs of −3, 0, & +3 | CI: 0% correct identification at −3 & 0 SNRs, and 13% at +3 SNR. NH: 22%, 27% and 50% correct identification at −3, 0, and +3 SNRs |
| Kim et al., 2013 | CI Children | Assess speech perception in children with a long interval between two implants | Monosyllabic words in speech noise; fixed SNR of +10 | CI: Approximately 82% & 85% correct identification for the 1st CI and both Cis respectively |
| Zeitler et al., 2012 | CI Adolescents | Assess the efficacy of implantation in prelingually deafened adolescents | HINT sentences; fixed SNR of +10 | No raw % correct data (showing only % change between assessments) |
| Gifford et al., 2011 | NH & CI Children | Assess speech perception with SmartSound strategies | HINT sentences in semi-diffuse restaurant noise; adaptive SNR | CI: Mean SRTn of 14.4 dB and 10.9 dB, depending on the coding strategy. NH: Mean SRTn of 0 dB |
| Davidson et al., 2011 | CI Adolescents | Assess speech perception & correlations to speech production & language tests | BKB sentences in babble noise; fixed SNR of +10 | CI Mean: 52.0% ± 26.3% correct identification |
| Shpak et al., 2009 | CI Children, adolescents and young-adults | Assess the benefits of late implantation in prelingually deafened individuals | CID test: sentences in speech-shaped noise; fixed SNR of +10 | CI Mean: 34% correct identification two years post implantation |
| Galvin et al., 2007 | CI Children | Evaluate the additional perceptual benefit from sequential bilateral implants | Spondee words discrimination in speech-shaped broadband noise; adaptive SNR | CI: Mean SRTn −12 dB, range: approximately −9 to +1.8 for the 1st CI, and −13 to −4 for both CIs |
| Wolfe et al., 2007 | CI Children | Evaluate speech recognition following sequential implantation | Spondee words in steady state speech-weighted noise; adaptive SNR | CI: Mean SRTn −5.75 dB for the 1st implanted ear, −2.17 dB for the 2nd and −11.75 dB for both CIs |
| Uziel et al., 2007 | CI Children | Assess speech perception, speech intelligibility, receptive language level & academic/occupational status | Meaningful sentences in noise; fixed SNR of +10 | CI Mean: 44.5% ± 28% correct identification, range: 0%–94% |
| Dettman et al., 2004 | CI Children | Assess speech perception & bilateral-bimodal benefits for children with significant residual hearing | BKB sentences in multi-talker babble; fixed SNR of +10 | CI Mean: 61.71% correct identification |
References
- O’Donoghue, G. Cochlear implants—Science, serendipity, and success. N. Engl. J. Med. 2013, 369, 1190–1193. [Google Scholar] [CrossRef] [PubMed]
- Perez, R.; Kishon-Rabin, L. Cochlear Implants–Pediatric. In Encyclopedia of Otolaryngology, Head and Neck Surgery; Kountakis, S.E., Ed.; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Bugannim, Y.; Roth, D.A.; Zechoval, D.; Kishon-Rabin, L. Training of Speech Perception in Noise in Pre-Lingual Hearing Impaired Adults with Cochlear Implants Compared with Normal Hearing Adults. Otol. Neurotol. 2019, 40, e316–e325. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, A.; Nittrouer, S. Speech perception in noise by children with cochlear implants. J. Speech Lang. Hear. Res. 2013, 56, 13–30. [Google Scholar] [CrossRef] [Green Version]
- Ching, T.Y.; Zhang, V.W.; Flynn, C.; Burns, L.; Button, L.; Hou, S.; McGhie, K.; Van Buynder, P. Factors influencing speech perception in noise for 5-year-old children using hearing aids or cochlear implants. Int. J. Audiol. 2018, 57, S70–S80. [Google Scholar] [CrossRef]
- Eisenberg, L.S.; Fisher, L.M.; Johnson, K.C.; Ganguly, D.H.; Grace, T.; Niparko, J.K.; Team, C.I. Sentence Recognition in Quiet and Noise by Pediatric Cochlear Implant Users: Relationships to Spoken Language. Otol. Neurotol. 2016, 37, e75–e81. [Google Scholar] [CrossRef] [Green Version]
- Hick, C.B.; Tharpe, A.M. Listening effort and fatigue in school-age children with and without hearing loss. J. Speech Lang. Hear. Res. 2002, 45, 573–584. [Google Scholar] [CrossRef]
- Mishra, S.K.; Boddupally, S.P. Auditory Cognitive Training for Pediatric Cochlear Implant Recipients. Ear Hear. 2018, 39, 48–59. [Google Scholar] [CrossRef]
- Wilson, B.S.; Dorman, M.F. Cochlear implants: A remarkable past and a brilliant future. Hear. Res. 2008, 242, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Gifford, R.H.; Shallop, J.K.; Peterson, A.M. Speech recognition materials and ceiling effects: Considerations for cochlear implant programs. Audiol. Neurotol. 2008, 13, 193–205. [Google Scholar] [CrossRef]
- Fu, Q.J.; Galvin, J.J. Maximizing cochlear implant patients’ performance with advanced speech training procedures. Hear. Res. 2008, 242, 198–208. [Google Scholar] [CrossRef] [Green Version]
- Kronenberger, W.G.; Colson, B.G.; Henning, S.C.; Pisoni, D.B. Executive functioning and speech-language skills following long-term use of cochlear implants. J. Deaf Stud. Deaf Educ. 2014, 19, 456–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, S.; Kraus, N. Sensory-cognitive interaction in the neural encoding of speech in noise: A review. J. Am. Acad. Audiol. 2010, 21, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Best, V.; Gallun, F.J.; Carlile, S.; Shinn-Cunningham, B.G. Binaural interference and auditory grouping. J. Acoust. Soc. Am. 2007, 121, 1070–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubinstein, J.T. How cochlear implants encode speech. Curr. Opin. Otolaryngol. Head Neck Surg. 2004, 12, 444–448. [Google Scholar] [CrossRef]
- Lorenzi, C.; Gilbert, G.; Carn, H.; Garnier, S.; Moore, B.C. Speech perception problems of the hearing impaired reflect inability to use temporal fine structure. Proc. Natl. Acad. Sci. USA 2006, 103, 18866–18869. [Google Scholar] [CrossRef] [Green Version]
- Drennan, W.R.; Rubinstein, J.T. Music perception in cochlear implant users and its relationship with psychophysical capabilities. J. Rehabil. Res. Dev. 2008, 45, 779–789. [Google Scholar] [CrossRef]
- Rönnberg, J.; Lunner, T.; Zekveld, A.; Sörqvist, P.; Danielsson, H.; Lyxell, B.; Dahlström, O.; Signoret, C.; Stenfelt, S.; Pichora-Fuller, M.K.; et al. The Ease of Language Understanding (ELU) model: Theoretical, empirical, and clinical advances. Front. Syst. Neurosci. 2013, 7, 31. [Google Scholar] [CrossRef] [Green Version]
- Stenfelt, S.; Rönnberg, J. The signal-cognition interface: Interactions between degraded auditory signals and cognitive processes. Scand. J. Psychol. 2009, 50, 385–393. [Google Scholar] [CrossRef]
- Boothroyd, A. Auditory development of the hearing child. Scand. Audiol. Suppl. 1997, 46, 9–16. [Google Scholar]
- Spehar, B.; Goebel, S.; Tye-Murray, N. Effects of Context Type on Lipreading and Listening Performance and Implications for Sentence Processing. J. Speech Lang. Hear. Res. 2015, 58, 1093–1102. [Google Scholar] [CrossRef] [Green Version]
- Kishon-Rabin, L.; Boothroyd, A. The Role of Hearing for Speech and Language Acquisition and Processing. In Handbook of Communication Disorders: Theoretical, Empirical, and Applied Linguistic Perspectivess; Ravid, D., Baron, A., Eds.; De Gruyter Mouton, Inc.: Berlin, Boston, 2018. [Google Scholar]
- AuBuchon, A.M.; Pisoni, D.B.; Kronenberger, W.G. Evaluating Pediatric Cochlear Implant Users’ Encoding, Storage, and Retrieval Strategies in Verbal Working Memory. J. Speech Lang. Hear. Res. 2019, 62, 1016–1032. [Google Scholar] [CrossRef] [PubMed]
- Cejas, I.; Mitchell, C.M.; Hoffman, M.; Quittner, A.L. CDaCI Investigative Team. Comparisons of IQ in Children with and without Cochlear Implants: Longitudinal Findings and Associations with Language. Ear Hear. 2018, 39, 1187–1198. [Google Scholar] [CrossRef] [PubMed]
- Geers, A.E.; Hayes, H. Reading, writing, and phonological processing skills of adolescents with 10 or more years of cochlear implant experience. Ear Hear. 2011, 32, 49S–59S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, C.; Goswami, U. Phonological awareness, vocabulary, and reading in deaf children with cochlear implants. J. Speech Lang. Hear. Res. 2010, 53, 237–261. [Google Scholar] [CrossRef]
- Chandramouli, S.H.; Kronenberger, W.G.; Pisoni, D.B. Verbal Learning and Memory in Early-Implanted, Prelingually Deaf Adolescent and Adult Cochlear Implant Users. J. Speech Lang. Hear. Res. 2019, 62, 1033–1050. [Google Scholar] [CrossRef]
- Niparko, J.K.; Tobey, E.A.; Thal, D.J.; Eisenberg, L.S.; Wang, N.Y.; Quittner, A.L.; Fink, N.E.; Team, C.I. Spoken language development in children following cochlear implantation. JAMA 2010, 303, 1498–1506. [Google Scholar] [CrossRef] [Green Version]
- Nittrouer, S.; Caldwell-Tarr, A.; Lowenstein, J.H. Working memory in children with cochlear implants: Problems are in storage, not processing. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1886–1898. [Google Scholar] [CrossRef] [Green Version]
- Pisoni, D.B.; Kronenberger, W.G.; Roman, A.S.; Geers, A.E. Measures of digit span and verbal rehearsal speed in deaf children after more than 10 years of cochlear implantation. Ear Hear. 2011, 32, 60S–74S. [Google Scholar] [CrossRef] [Green Version]
- AuBuchon, A.M.; Pisoni, D.B.; Kronenberger, W.G. Short-Term and Working Memory Impairments in Early-Implanted, Long-Term Cochlear Implant Users Are Independent of Audibility and Speech Production. Ear Hear. 2015, 36, 733–737. [Google Scholar] [CrossRef] [Green Version]
- Davidson, L.S.; Geers, A.E.; Blamey, P.J.; Tobey, E.A.; Brenner, C.A. Factors contributing to speech perception scores in long-term pediatric cochlear implant users. Ear Hear. 2011, 32, 19S–26S. [Google Scholar] [CrossRef] [Green Version]
- Geers, A.; Brenner, C.; Davidson, L. Factors associated with development of speech perception skills in children implanted by age five. Ear Hear. 2003, 24, 24S–35S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, J.; Thornton, A.R. Neural correlates of perceptual learning in the auditory brainstem: Efferent activity predicts and reflects improvement at a speech-in-noise discrimination task. J. Neurosci. 2008, 28, 4929–4937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, J.H.; Skoe, E.; Banai, K.; Kraus, N. Perception of speech in noise: Neural correlates. J. Cogn. Neurosci. 2011, 23, 2268–2279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akeroyd, M.A. Are individual differences in speech reception related to individual differences in cognitive ability? A survey of twenty experimental studies with normal and hearing-impaired adults. Int. J. Audiol. 2008, 47, S53–S71. [Google Scholar] [CrossRef]
- Davidson, L.S.; Geers, A.E.; Uchanski, R.M.; Firszt, J.B. Effects of Early Acoustic Hearing on Speech Perception and Language for Pediatric Cochlear Implant Recipients. J. Speech Lang. Hear. Res. 2019, 62, 3620–3637. [Google Scholar] [CrossRef]
- Geers, A.E. Speech, language, and reading skills after early cochlear implantation. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 634–638. [Google Scholar] [CrossRef] [Green Version]
- Lunner, T.; Rudner, M.; Rönnberg, J. Cognition and hearing aids. Scand. J. Psychol. 2009, 50, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Moberly, A.C.; Bates, C.; Harris, M.S.; Pisoni, D.B. The Enigma of Poor Performance by Adults with Cochlear Implants. Otol. Neurotol. 2016, 37, 1522–1528. [Google Scholar] [CrossRef]
- Rudner, M.; Foo, C.; Sundewall-Thorén, E.; Lunner, T.; Rönnberg, J. Phonological mismatch and explicit cognitive processing in a sample of 102 hearing-aid users. Int. J. Audiol. 2008, 47, S91–S98. [Google Scholar] [CrossRef]
- Svirsky, M.A.; Teoh, S.W.; Neuburger, H. Development of language and speech perception in congenitally, profoundly deaf children as a function of age at cochlear implantation. Audiol. Neurootol. 2004, 9, 224–233. [Google Scholar] [CrossRef]
- Manrique, M.; Cervera-Paz, F.J.; Huarte, A.; Molina, M. Prospective long-term auditory results of cochlear implantation in prelinguistically deafened children: The importance of early implantation. Acta Otolaryngol. Suppl. 2004, 55–63. [Google Scholar] [CrossRef] [PubMed]
- McConkey Robbins, A.; Koch, D.B.; Osberger, M.J.; Zimmerman-Phillips, S.; Kishon-Rabin, L. Effect of age at cochlear implantation on auditory skill development in infants and toddlers. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 570–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kral, A.; Kronenberger, W.G.; Pisoni, D.B.; O’Donoghue, G.M. Neurocognitive factors in sensory restoration of early deafness: A connectome model. Lancet Neurol. 2016, 15, 610–621. [Google Scholar] [CrossRef]
- Kral, A.; Dorman, M.F.; Wilson, B.S. Neuronal Development of Hearing and Language: Cochlear Implants and Critical Periods. Annu. Rev. Neurosci. 2019, 42, 47–65. [Google Scholar] [CrossRef]
- Kral, A.; Sharma, A. Developmental neuroplasticity after cochlear implantation. Trends Neurosci. 2012, 35, 111–122. [Google Scholar] [CrossRef] [Green Version]
- Kraaijenga, V.J.C.; Ramakers, G.G.J.; Smulders, Y.E.; van Zon, A.; Free, R.H.; Frijns, J.H.M.; Huinck, W.J.; Stokroos, R.J.; Grolman, W. No Difference in Behavioral and Self-Reported Outcomes for Simultaneous and Sequential Bilateral Cochlear Implantation: Evidence From a Multicenter Randomized Controlled Trial. Front. Neurosci. 2019, 13, 54. [Google Scholar] [CrossRef] [Green Version]
- Hoppe, U.; Hocke, T.; Digeser, F. Bimodal benefit for cochlear implant listeners with different grades of hearing loss in the opposite ear. Acta Otolaryngol. 2018, 138, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Hua, H.; Johansson, B.; Magnusson, L.; Lyxell, B.; Ellis, R.J. Speech Recognition and Cognitive Skills in Bimodal Cochlear Implant Users. J. Speech Lang. Hear. Res. 2017, 60, 2752–2763. [Google Scholar] [CrossRef]
- O’Neill, E.R.; Kreft, H.A.; Oxenham, A.J. Cognitive factors contribute to speech perception in cochlear-implant users and age-matched normal-hearing listeners under vocoded conditions. J. Acoust. Soc. Am. 2019, 146, 195. [Google Scholar] [CrossRef] [Green Version]
- Van Wieringen, A.; Wouters, J. What can we expect of normally-developing children implanted at a young age with respect to their auditory, linguistic and cognitive skills? Hear. Res. 2015, 322, 171–179. [Google Scholar] [CrossRef]
- Choi, J.E.; Moon, I.J.; Kim, E.Y.; Park, H.S.; Kim, B.K.; Chung, W.H.; Cho, Y.S.; Brown, C.J.; Hong, S.H. Sound Localization and Speech Perception in Noise of Pediatric Cochlear Implant Recipients: Bimodal Fitting Versus Bilateral Cochlear Implants. Ear Hear. 2017, 38, 426–440. [Google Scholar] [CrossRef]
- Friedmann, D.R.; Green, J.; Fang, Y.; Ensor, K.; Roland, J.T.; Waltzman, S.B. Sequential bilateral cochlear implantation in the adolescent population. Laryngoscope 2015, 125, 1952–1958. [Google Scholar] [CrossRef]
- Wolfe, J.; Baker, S.; Caraway, T.; Kasulis, H.; Mears, A.; Smith, J.; Swim, L.; Wood, M. 1-year postactivation results for sequentially implanted bilateral cochlear implant users. Otol. Neurotol. 2007, 28, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Goldsworthy, R.L.; Markle, K.L. Pediatric Hearing Loss and Speech Recognition in Quiet and in Different Types of Background Noise. J. Speech Lang. Hear. Res. 2019, 62, 758–767. [Google Scholar] [CrossRef] [PubMed]
- Cusumano, C.; Friedmann, D.R.; Fang, Y.; Wang, B.; Roland, J.T.; Waltzman, S.B. Performance Plateau in Prelingually and Postlingually Deafened Adult Cochlear Implant Recipients. Otol. Neurotol. 2017, 38, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Kim, L.S.; Jeong, S.W. Functional benefits of sequential bilateral cochlear implantation in children with long inter-stage interval between two implants. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 162–169. [Google Scholar] [CrossRef]
- Zeitler, D.M.; Anwar, A.; Green, J.E.; Babb, J.S.; Friedmann, D.R.; Roland, J.T.; Waltzman, S.B. Cochlear implantation in prelingually deafened adolescents. Arch. Pediatr. Adolesc. Med. 2012, 166, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Gifford, R.H.; Olund, A.P.; Dejong, M. Improving speech perception in noise for children with cochlear implants. J. Am. Acad. Audiol. 2011, 22, 623–632. [Google Scholar] [CrossRef]
- Shpak, T.; Koren, L.; Tzach, N.; Most, T.; Luntz, M. Perception of speech by prelingual pre-adolescent and adolescent cochlear implant users. Int. J. Audiol. 2009, 48, 775–783. [Google Scholar] [CrossRef]
- Galvin, K.L.; Mok, M.; Dowell, R.C. Perceptual benefit and functional outcomes for children using sequential bilateral cochlear implants. Ear Hear. 2007, 28, 470–482. [Google Scholar] [CrossRef]
- Uziel, A.S.; Sillon, M.; Vieu, A.; Artieres, F.; Piron, J.P.; Daures, J.P.; Mondain, M. Ten-year follow-up of a consecutive series of children with multichannel cochlear implants. Otol. Neurotol. 2007, 28, 615–628. [Google Scholar] [CrossRef] [PubMed]
- Dettman, S.J.; D’Costa, W.A.; Dowell, R.C.; Winton, E.J.; Hill, K.L.; Williams, S.S. Cochlear implants for children with significant residual hearing. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 612–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ching, T.Y.; van Wanrooy, E.; Dillon, H.; Carter, L. Spatial release from masking in normal-hearing children and children who use hearing aids. J. Acoust. Soc. Am. 2011, 129, 368–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollmeier, B.; Warzybok, A.; Hochmuth, S.; Zokoll, M.A.; Uslar, V.; Brand, T.; Wagener, K.C. The multilingual matrix test: Principles, applications, and comparison across languages: A review. Int. J. Audiol. 2015, 54, 3–16. [Google Scholar] [CrossRef]
- Hey, M.; Hocke, T.; Mauger, S.; Müller-Deile, J. A clinical assessment of cochlear implant recipient performance: Implications for individualized map settings in specific environments. Eur. Arch. Otorhinolaryngol. 2016, 273, 4011–4020. [Google Scholar] [CrossRef] [Green Version]
- Zaltz, Y.; Goldsworthy, R.L.; Kishon-Rabin, L.; Eisenberg, L.S. Voice Discrimination by Adults with Cochlear Implants: The Benefits of Early Implantation for Vocal-Tract Length Perception. J. Assoc. Res. Otolaryngol. 2018, 19, 193–209. [Google Scholar] [CrossRef]
- Brand, T.; Kollmeier, B. Efficient adaptive procedures for threshold and concurrent slope estimates for psychophysics and speech intelligibility tests. J. Acoust. Soc. Am. 2002, 111, 2801–2810. [Google Scholar] [CrossRef]
- Boothroyd, A. Statistical theory of the speech discrimination score. J. Acoust. Soc. Am. 1968, 43, 362–367. [Google Scholar] [CrossRef]
- Kishon-Rabin, L.; Patael, S.; Menahemi, M.; Amir, N. Are the perceptual effects of spectral smearing influenced by speaker gender? J. Basic Clin. Physiol. Pharmacol. 2004, 15, 41–55. [Google Scholar]
- Kavé, G. Phonemic fluency, semantic fluency, and difference scores: Normative data for adult Hebrew speakers. J. Clin. Exp. Neuropsychol. 2005, 27, 690–699. [Google Scholar] [CrossRef]
- Raven, J.C.; Court, J.H. Raven Manual, Section 1 Standard Progressive Matrices; Oxford Psychologist Press Ltd.: Oxford, UK, 1998. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children-III; The Psychological Corporation: San Antonio, TX, USA, 1991. [Google Scholar]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- Khan, S.; Edwards, L.; Langdon, D. The cognition and behaviour of children with cochlear implants, children with hearing aids and their hearing peers: A comparison. Audiol. Neurootol. 2005, 10, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Kos, M.I.; Deriaz, M.; Guyot, J.P.; Pelizzone, M. What can be expected from a late cochlear implantation? Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Santarelli, R.; De Filippi, R.; Genovese, E.; Arslan, E. Cochlear implantation outcome in prelingually deafened young adults. A speech perception study. Audiol. Neurootol. 2008, 13, 257–265. [Google Scholar] [CrossRef]
- Zeitler, D.M.; Kessler, M.A.; Terushkin, V.; Roland, T.J.; Svirsky, M.A.; Lalwani, A.K.; Waltzman, S.B. Speech perception benefits of sequential bilateral cochlear implantation in children and adults: A retrospective analysis. Otol. Neurotol. 2008, 29, 314–325. [Google Scholar] [CrossRef]
- DeThorne, L.S.; Schaefer, B.A. A guide to child nonverbal IQ measures. Am. J. Speech Lang. Pathol. 2004, 13, 275–290. [Google Scholar] [CrossRef]





| Subject ID | Gender | Etiology | Age at Identification (Years) | Age at Fitting HA (Years) | Age at Implantation (Years) | Age at Testing (Years) | Implant |
|---|---|---|---|---|---|---|---|
| CI1 | F | Suspected neonatal jaundice | Birth | 0.5 | 1.1 (L) 1.5 (R) | 10.17 | Cochlear C512 (R + L) |
| CI2 | F | Genetic | Birth | 0.25 | 1.11 (R) 4.11 (L) | 15.67 | Cochlear Freedom (R + L) |
| CI3 | F | Genetic | Birth | 0.25 | 1 (R) 2 (L) | 12.67 | Cochlear Freedom (R + L) |
| CI4 | F | Genetic | Birth | 0.33 | 1.5 (R) 2.4 (L) | 9.50 | Cochlear C512 (R + L) |
| CI5 | M | Genetic | Birth | 0.58 | 1 (R) 5 (L) | 13.17 | Cochlear Freedom (R) C512 (L) |
| CI6 | M | Unknown | Birth | 0.58 | 1 (R) 1.75 (L) | 9.08 | Cochlear C512 (R + L) |
| CI7 | M | Suspected CMV | Birth | 0.5 | 1.11 (L) | 12.75 | Cochlear C512 (L) |
| CI8 | F | Unknown | 0.25 | 0.25 | 2.8 15.7 | 20.9 | Cochlear Freedom (R + L) |
| CI9 | M | Genetic-connexin | 0.67 | 0.83 | 2.5 (L) | 24.3 | Cochlear Freedom (L) |
| CI10 | M | Genetic | 1.5 | 2 | 3 (L) | 21.2 | Cochlear Freedom (L) |
| CI11 | M | Genetic | 1.5 | 1.5 | 3.7 (R) 15 (L) | 21.6 | Cochlear Espirit (R) Freedom (L) |
| CI12 | F | Waardenburg syndrome | Birth | Unknown | 3 (L) | 25.3 | Cochlear Espirit (L) |
| CI13 | F | Genetic | 0.5 | 0.5 | 2.5 (L) | 19.6 | Cochlear Espirit (L) |
| CI14 | F | Waardenburg syndrome | Birth | 0.25 | 2.5 (L) 16 (R) | 22.8 | Cochlear Freedom (R) Nucleus 5 (L) |
| CI15 | M | Meningitis | 0.58 | 0.58 | 2.3 (R) 14 (L) | 22.9 | Cochlear Nucleus 22 (R) Nucleus 24 (L) |
| CI16 | M | Genetic | 0.83 | 1 | 3 (L) | 23 | Cochlear Nucleus (L) |
| CI17 | M | Genetic | Birth | 1.67 | 9 (R) 19 (L) | 29.2 | Cochlear Sprint (R) Freedom (L) |
| CI18 | M | Genetic | Birth | 1 | 6 (R) 13 (L) | 23.6 | Cochlear Sprint (R) Freedom (L) |
| CI19 | M | Unknown | Birth | 0.5 | 6 (L) | 21.9 | Cochlear Nucleus |
| CI20 | M | Unknown | Birth | 1 | 12.7 (R) | 28.4 | Cochlear Nucleus |
| CI21 | F | Unknown | Birth | 1 | 8.3 (R) | 24 | Advanced Bionics Naida |
| CI22 | M | Genetic-Connexin | Birth | 1 | 29.1 (L) | 31.2 | Advanced Bionics Naida |
| CI23 | M | Genetic-Connexin | Birth | 0.25 | 15.3 (R) 25.7 (L) | 27.1 | MedEL Opus (R + L) |
| CI24 | F | Unknown | Birth | 1 | 6.2 (L) | 26.3 | Cochlear Nucleus |
| CI25 | M | Unknown | Birth | 1 | 9 (L) 24.5 (R) | 25.7 | Cochlear Nucleus (R + L) |
| CI26 | M | Suspected hepatitis | Birth | 0.67 | 21.9 (L) | 26.6 | Cochlear Nucleus (L) |
| CI27 | M | Unknown | Birth | 1.5 | 31.33 (L) | 32.3 | MedEl Opus (L) |
| CI28 | F | Genetic-Connexin | Progressive | Unknown | 8.9 (R) | 9.33 | Cochlear C512 (R) |
| CI29 | F | Unknown | Progressive | 4 | 7.2 (R) 8.9 (L) | 10.17 | Cochlear C512 (R + L) |
| CI30 | M | Genetic | Progressive | 2 | 3.6 (R) 3.11 (L) | 9.5 | Cochlear C512 (R + L) |
| CI31 | F | Genetic | Progressive | 3 | 6.9 (L) | 10.67 | MedEl Rondo (L) |
| CI32 | F | Hematologic disease | Progressive | 3 | 3.8 (L) 4.7 (R) | 11.92 | Cochlear C512 (R + L) |
| CI33 | F | Unknown | Progressive | Unknown | 6.2 (R) 9.4 (L) | 12.08 | Cochlear Freedom (R) C512 (L) |
| CI34 | F | Genetic | Progressive | 5 | 15.5 (R) | 16.92 | Cochlear C512 (R) |
| CI35 | M | Genetic | Progressive | 3 | 6.1 (R) 10.1 (L) | 12.33 | Cochlear Freedom (R) C512 (L) |
| CI36 | M | Genetic | Progressive | 3.5 | 24.6 (L) | 26 | Advanced Bionics Naida (L) |
| CI37 | M | Genetic | Progressive | 3 | 19 (L) | 20.8 | Cochlear Freedom (L) |
| CI38 | F | Genetic-Connexin | Progressive | 0.58 | 13 (R) | 23.8 | Advanced Bionics Naida (R) |
| CI39 | F | Unknown | Progressive | 3 | 14.8 (L) | 22.8 | Cochlear Nucleus (L) |
| CI40 | F | Genetic | Progressive | 2 | 16 (R) 19.1 (L) | 25.4 | Advanced Bionics Neptune (R) Harmony (L) |
| Age | Raven (%) | TMT (Seconds) | Digit Range (Number) | Semantic Fluency (Number) | Phonemic Fluency (Number) | Receptive Vocabulary (%) | ||
|---|---|---|---|---|---|---|---|---|
| Progressive | Mean | 16.25 | 83 | 22.84 | 3.84 | 6.85 | 13.08 | 67.10 |
| SD | 6.5 | 12.77 | 10.51 | 1.21 | 2.92 | 3.98 | 18.51 | |
| n | 13 | 11 | 13 | 13 | 9 | 9 | 9 | |
| Early-Implanted | Mean | 17.75 | 82.63 | 22.71 | 4.35 | 6.48 | 12.92 | 71.14 |
| SD | 5.75 | 9.32 | 7 | 1.39 | 3.26 | 3.66 | 14.25 | |
| n | 16 | 15 | 16 | 14 | 9 | 9 | 9 | |
| Late-Implanted | Mean | 27.17 | 74.53 | 23.5 | 4.45 | 8.94 | 17.83 | 77.02 |
| SD | 3.75 | 16.3 | 10.87 | 1.21 | 3.32 | 4.57 | 19.22 | |
| n | 11 | 8 | 8 | 11 | 6 | 6 | 5 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaltz, Y.; Bugannim, Y.; Zechoval, D.; Kishon-Rabin, L.; Perez, R. Listening in Noise Remains a Significant Challenge for Cochlear Implant Users: Evidence from Early Deafened and Those with Progressive Hearing Loss Compared to Peers with Normal Hearing. J. Clin. Med. 2020, 9, 1381. https://doi.org/10.3390/jcm9051381
Zaltz Y, Bugannim Y, Zechoval D, Kishon-Rabin L, Perez R. Listening in Noise Remains a Significant Challenge for Cochlear Implant Users: Evidence from Early Deafened and Those with Progressive Hearing Loss Compared to Peers with Normal Hearing. Journal of Clinical Medicine. 2020; 9(5):1381. https://doi.org/10.3390/jcm9051381
Chicago/Turabian StyleZaltz, Yael, Yossi Bugannim, Doreen Zechoval, Liat Kishon-Rabin, and Ronen Perez. 2020. "Listening in Noise Remains a Significant Challenge for Cochlear Implant Users: Evidence from Early Deafened and Those with Progressive Hearing Loss Compared to Peers with Normal Hearing" Journal of Clinical Medicine 9, no. 5: 1381. https://doi.org/10.3390/jcm9051381